
Abstract
Background:
The American Thyroid Association guidelines recommend the routine use of radioactive iodine for remnant ablation (RRA) in all T3 or greater primary tumors, and selective use in patients with intrathyroidal disease >1 cm, or evidence of nodal metastases. The guidelines recognize that there is conflicting and inadequate data to make firm recommendations for most patients. The aim of this study was to analyze our institutional experience of the use of RRA in the management of papillary thyroid cancer, with a particular focus on outcomes for those patients selected not to receive RRA.
Methods:
We retrospectively reviewed 1129 consecutive patients who underwent total thyroidectomy at the Memorial Sloan-Kettering Cancer Center between 1986 and 2005. Of these, 490 were pT1–2 N0, 193 pT1–2 N1, and 444 pT3–4. Details on recurrence and disease-specific survival were recorded by the Kaplan–Meier method and compared using the log-rank test.
Results:
The five-year disease-specific survival and recurrence-free survival in the pT1/T2 N0, pT1–2 N1, and pT3–4 were 100% and 92%, 100% and 92%, and 98% and 87% respectively. Low-risk patients who were managed without RRA (who tended to have limited primary disease, pT1–2, and low-volume metastatic disease in the neck, pT1–2 N1—fewer than five nodes, all <1 cm greatest dimension) had five-year recurrence-free survival of >97%. In the group with advanced local tumors (pT3–4), those patients who did not receive RRA (who tended to have pT3 N0 disease) had five-year recurrence-free survival of >90%.
Conclusion:
Following appropriate surgical management, the majority of patients with low-risk local disease and even some patients with more advanced-stage (pT3) tumors or regional metastases have low rates of recurrence and high rates of survival when managed without RRA.
Introduction
At the Memorial Sloan-Kettering Cancer Center (MSKCC), we have used a risk-group stratification policy to select patients who are at higher risk of cause-specific death. Such risk stratification aims to select appropriate treatment for each individual case. Within our institution, we have applied this approach to select patients appropriate for both conservative surgery in the form of lobectomy in low-risk patients, and aggressive resections including neck dissection and laryngopharyngeral resections where appropriate in high-risk cases. In addition to surgical resection, we have also used risk-group stratification to identify which patients may benefit from additional therapies, such as RAI, external beam radiation therapy, or systemic therapy. Although papillary microcarcinomas in young patients are widely accepted as being low risk, and therefore are not routinely offered RAI, we extend the category of low-risk tumors to those that are <4 cm and remain confined to the gland. We also consider low-volume neck disease (fewer than five positive nodes, all <1 cm greatest dimension) as being at low risk of death, and therefore a select subset of such patients are also managed without routine RRA.
The objective of our study was to examine and compare our results on survival and recurrence rates in patients who were selected not to receive RRA, by examining a contemporary data set of patients with PTC managed by total thyroidectomy at MSKCC between 1986 and 2005.We also report on the overall efficacy of RRA on recurrence and survival in all patients and also on specific subgroups, namely patients with pT1–2 N0 disease, patients with pT1–2 N+ disease, and those with locally advanced (pT3–4) disease separately.
Materials and Methods
Following approval by the Institutional Review Board, 1129 consecutive patients who had total thyroidectomy for PTC (using the 2009 AJCC staging manual) between 1986 and 2005 were identified from our institutional database of 1810 patients treated for WDTC at MSKCC. Patients with all T stages (T1a–4) were considered for this study. Although low-risk patients with limited local disease are offered thyroid lobectomy in the absence of high-risk features or nodular disease in the contralateral lobe, around half of the patients in this cohort had limited local disease (pT1–2). Patients who underwent initial treatment elsewhere prior to referral, those who were considered unresectable at the time of referral or surgery, those treated with less than total thyroidectomy, and those presenting with evidence of distant metastasis at presentation or on postoperative RAI scan (within six months) were excluded. As not all patients underwent postoperative RAI scanning, it is possible that some patients treated without RRA may have harbored occult metastases following surgery. If discovered within six months, such patients were coded as M1. If they presented later than six months, they were coded as recurrence. (Only three patients treated without RRA suffered distant metastases at 7, 27, and 50 months, and this factor is therefore unlikely to bias the results.)
Data collected included patient demographics and surgical details, including the presence of gross extra-thyroid extension. Histopathological details recorded included tumor histology, primary tumor size, presence of extra-thyroid extension and presence of metastatic lymph nodes. Postoperative treatment detail recorded was the use of RAI.
Based on clinical and histopathological features, cases were classified into low-, intermediate-, and high-risk groups for death based on the MSKCC previously published risk stratification system (Table 1) (11,12). Patients under the age of 45 years who present with papillary carcinomas <4 cm confined to the thyroid gland (intraglandular), without evidence of distant metastatic disease, are at very low risk of death, whereas patients over the age of 45 years, with extrathyroid extension (ETE), aggressive histopathology, and disease >4 cm in dimension or distant metastatic disease are at higher risk. Young patients with, or older patients without, aggressive histopathological features form an intermediate risk group (13).
MSKCC, Memorial Sloan-Kettering Cancer Center; ETE, extrathyroid extension.
The recent American Thyroid Association (ATA) guidelines provided a method of stratification based on risk of recurrence rather than death, which was also applied to this group (Table 2) (8). Patients with fully excised disease without ETE, aggressive histopathology, vascular invasion, or regional or distant metastases are at low risk of recurrence. Patients with macroscopic ETE, distant metastases, or incomplete tumor resection are at high risk of recurrence. All other patients represent an intermediate risk group for recurrence.
Only low risk if all are true.
Intermediate or high risk if any are true.
RAI, radioactive iodine.
In the cohort of patients from 1986 to 2005, preoperative ultrasound was not routinely used for preoperative assessment of the central and lateral compartment lymph nodes. The assessment of the lateral neck nodes was based on preoperative clinical examination, and if enlarged, ultrasound carried out. Assessment of the central compartment for all patients was intraoperative by palpation of the central compartment lymph nodes at the time of thyroidectomy. If no palpable nodes were present in the central compartment, then no elective central compartment neck dissection was done. If nodes were palpable, then a central compartment neck dissection was carried out. Due to this approach to the neck, we have coded our results as N0 when no positive nodes were excised and N1 when positive nodal disease was reported on histology. Not all patients had formal neck dissections in either the N0 or N1 group, and those who had fewer than six nodes excised (pNx) without evidence of positive disease were described as N0. Postoperative thyroid stimulating hormone (TSH) suppression is practiced for all patients, aiming for a level of between 0.1 and 0.5 μU/mL.
Our institutional approach to selecting patients for RRA has evolved during the time period studied. All high-risk patients are considered for RRA, whereas low-risk patients are generally selected for management without RRA. Intermediate risk patients are offered RRA dependent on patient and tumor factors. In the mid-1980s, the use of RAI increased nationally as well as within our institution. More recently, our disease management team has become increasingly selective with the intermediate-risk group, limiting the use of RRA in older patients who have limited local disease, and in those young patients with low-volume neck disease. Despite this general institutional approach, clinicians and patients vary in their assessment of risk and benefit, and an individualized treatment approach is employed in all cases, which introduces heterogeneity when analyzed retrospectively.
Prior to 1999, all RAI ablations and retreatments were done using traditional thyroid hormone withdrawal for four to six weeks. Since 1999, the vast majority of RAI ablations and treatments have been done using recombinant human TSH simulation. While our current recommendations call for lower RAI-administered activities, for the majority of the time period of the study, RAI ablation–administered activities were usually in the range of 100 mCi for remnant ablation, 150 mCi if pathological lymph-node metastases were present, and 175–200 mCi if distant metastases were present at diagnosis. Just as with the selection of patients for RAI remnant ablation, decisions regarding retreatment with RAI were complex, multifactorial, and varied among the treating physicians at our institution.
Outcomes data included local, regional, and distant recurrence as well as details of death. Local and regional recurrences were determined by clinical examination supplemented with imaging and fine-needle aspiration if recurrence was suspected. During the 1980s and 1990s, serum thyroglobulin (Tg) was not routinely used to detect recurrence. Similarly, annual ultrasound was not uniformly used as a tool for detection of recurrent disease during the majority of the study period. Both the use of Tg monitoring and serial ultrasound have become standard practice within our institution in recent years and now influence the further investigation of patients within this cohort.
The presence of local or regional recurrence following treatment was based on cytological or histopathological confirmation of structurally identifiable disease. Local recurrence was defined as recurrent disease located in the operated thyroid bed confirmed by cytological sampling or histological analysis following further surgery. Regional recurrence was defined as recurrent disease found in the cervical lymph nodes, confirmed again by cytological sampling or histopathology following subsequent surgical resection. Distant recurrence was determined by imaging studies, including radioiodine uptake scans, computed tomography (CT) scans, positron emission tomography scans, or cytological and histopathological evidence where available. Not all patients in the cohort had serial measurement of Tg. For this reason, we did not consider isolated Tg changes as recurrence. However, in current practice, patients with previously undetectable Tg (<0.2) who develop detectable levels are investigated with ultrasound, fine-needle aspiration of suspicious nodes or nodules, and CT scanning of the neck and chest in an attempt to identify evidence of structural disease.
Disease-specific outcomes were calculated using the date of last follow-up with the treating surgeon or endocrinologist at MSKCC. Details of death were determined from death certificates and hospital records where available. All patients who had evidence of active structural disease at the time of last follow-up and died during follow-up were considered to have died of disease. The median follow-up for the entire patient cohort was 63 months (range 1–282 months). Outcomes data were therefore calculated at five years. The completeness index (ratio of expected patient follow-up to observed patient follow-up) was 0.83 and 0.60 at 5 and 10 years respectively. Statistical analysis was carried out using JMP statistical package (SAS Institute Inc., Cary, NC) and IBM SPSS Statistics (IBM Corp., Chicago, IL). Variables were compared within groups using Pearson's chi-squared test. Survival outcomes were analyzed using the Kaplan–Meier method. Univariate analysis was carried out by the log-rank test, and multivariate analysis by the Cox proportional hazards method. A p-value of <0.05 was considered significant.
Results
Entire group
The median follow-up of this patient cohort was 63 months (range 1–282 months). The median age was 46 years (range 11–91 years) with a male-to-female ratio of 1:2.8. All patients were managed with total thyroidectomy (no patients with subtotal or near total thyroidectomy) and had no evidence of macroscopic residual disease following surgery or distant metastases. A total of 689 patients underwent no neck dissection (61%), 94 patients (8%) had central neck dissection, and 346 patients (31%) had central and lateral neck dissections. Of the 440 patients who underwent neck dissection, 355 (81%) had evidence of nodal metastases on histopathology. There were 691 patients (61%) who received postoperative RRA. Patient, tumor, and treatment details are shown in Table 3. Stratified by the administration of RRA, those receiving RRA were more likely to be male, to have more advanced pT and N stage disease, and to be in the high-risk MSKCC and ATA groups.
RRA, RAI remnant ablation; ATA, American Thyroid Association.
During follow-up, 18 patients (2%) died of disease and 84 (7%) developed recurrence: 4 patients recurred locally (<0.1%), 61 recurred regionally (5%), and 38 had distant recurrence (0.3%). There were 20 patients considered to have active disease at the time of last follow-up. Of these, 10 had isolated distant metastases, 1 isolated regional, and 1 isolated local recurrence. Of the remaining 8 patients, 7 had regional and distant disease and 1 had local, regional, and distant disease. The five-year disease-specific survival (DSS) and recurrence-free survival (RFS) rates were 99% and 92% respectively. For DSS, univariate analysis showed age >45 years, male sex, pT stage, and N-positive disease (N1b worse than N1a) to be predictors of worse outcome (Table 4). The administration of RRA did not predict DSS (five-year DSS RRA 99% vs. no RRA 100%, p=0.821). Due to the limited number of events (18 deaths), multivariate analysis of DSS could only be carried out with two variables; incorporating age and pT stage confirmed age >45 years and pT to be independent predictors of cause-specific mortality. Patients over the age of 45 years were 8.9 times more likely to die of disease. Patients with pT4 disease were 5.5 times more likely to die compared with pT1 patients. N stage was not predictive of outcome in either a multivariate model including pT and N stage, or N stage and age >45 years.
DSS, disease-specific survival; 5y, 5-year survival rate; 10y, 10-year survival rate; p U, p-value by univariate analysis; HR, hazard ratio; CI, 95% confidence interval; p M, p-value by multivariate analysis; NS, not significant.
For RFS, univariate analysis showed male sex, advanced pT stage, N-positive disease, and the administration of RRA to predict recurrence. Patients who had RRA had a worse five-year RFS than those who did not (90% vs. 97%, p<0.001) as predicted by the higher rate of intermediate and high-risk cases in this group by ATA stratification guidelines. On multivariate analysis incorporating age, sex, pT stage, N stage, and administration of RAI, only pT3, pT4, and N-positive disease were found to be independent predictors of outcome. Patients with pT3 disease had a twofold increased risk of recurrence, and patients with pT4 disease a 4.5-fold increased risk of recurrence compared to pT1 patients. Patients with N1 disease had a 3.4-fold increased risk of recurrence compared to patients without excised evidence of nodal metastases.
More detailed univariate analysis of local, regional, and distant recurrence-free survival (LRFS, RRFS, and DRFS respectively) showed age, sex, pT stage, and N stage to be important predictors of outcome (again N1b performed worse than N1a; Table 5). RRFS and DRFS were worse for patients who had RRA (94% vs. 99%, p<0.001, and 95% vs. 99%, p=0.001 respectively). There were too few events to carry out multivariate analysis of LRFS. However, multivariate analysis of RRFS and DRFS showed that pT4 and N-positive disease were independent predictors of recurrence (Table 5). Patients with pT4 disease had a 3.4-fold increased risk of regional recurrence and a 2.4-fold increased risk of distant recurrence compared to pT1 patients. Patients with N1 disease had a 3.1-fold increased risk of regional recurrence and a 3.8-fold increased risk of distant recurrence compared to N0 patients.
LRFS, local recurrence-free survival; RRFS, regional recurrence-free survival; DRFS, distant recurrence-free survival.
Recurrence in patients with T1 or T2 N0 disease
Within the cohort, 490 patients had disease localized to the thyroid at presentation. Of these, 282 patients (58%) had nodal tissue excised (N0; node sampling or formal neck dissection), the remaining 208 (42%) had no nodes excised (Nx). Of the 282 patients who had nodal tissue excised, 55 had formal central compartment neck dissections, 4 had lateral neck dissections, and the remaining patients had delphian, perithyroidal, or paratracheal node biopsies. All patients were N0 on pathological review. RRA was performed on 178 patients (36%). Patient, tumor, and treatment details are shown in Table 6. All patients were either low or intermediate risk patients using the MSKCC and ATA classifications. In agreement with our selection criteria for RRA, the patients in the group who had RRA were more likely to be male and more likely to have T2 than T1 disease.
There were no local recurrences in this subgroup, and therefore no factors predictive of LRFS were identified. There were only four regional recurrences (4/490, 1%) and two distant recurrences (2/490, 2%) during follow-up. The five-year DSS was 100% and RFS was 92% in this subgroup.
Stratifying by RRA, the five-year RRFS and DRFS for patients that did not have RRA were 98% and 100% respectively. The five-year RRFS and DRFS for patients that had RRA were 100% and 99% respectively. These differences were not statistically significant. Therefore, based on our selection criteria for RRA, patients who did not have RRA had an excellent outcome. These results support the MSKCC risk-group stratification and patient selection for RRA.
Recurrence in patients with T1 or T2 N1 disease
A total of 193 patients had pT1 or pT2 tumors and positive cervical nodal metastases (N1). As expected, the majority of these patients had RRA, as they were considered by the treating clinician to be at higher risk for both recurrence and/or death. Of the 193 patients, 142 were selected to receive RRA (74%) and 51 did not receive RRA (26%). The case records of the 51 patients who did not have RRA were examined thoroughly in an attempt to identify a reason for not giving RRA. Patient, tumor, and treatment details are shown in Table 7. These patients tended to be young and have low-risk tumors using the MSKCC classification; 41 (79%) patients were below 45 years of age, and 40 (77%) patients were categorized as low-risk, with the remaining 12 patients categorized as at intermediate risk of death. Seven patients were seen in conjunction with an endocrinologist, and these were more likely to receive RAI ablation than patients followed by surgeons alone. A flowchart stratifying patients by thyroglobulin level, size of the largest metastatic focus in lymph node, and number of positive lymph nodes is shown in Figure 1. Of 51 patients, 5 had a postoperative Tg <1, 9 had Tg >1, and 27 patients had no postoperative Tg recorded. Of the 46 patients who did not have an undetectable Tg, 14 had the largest metastatic lymph node focus <1 cm, in 18 patients the size of the largest node was not reported, and in the remaining 15 patients the node was >1 cm in maximum dimension. Of the 33 patients who did not have a largest metastastic node <1 cm recorded, 22 had five or fewer positive lymph nodes. This left 8 patients with more than five positive nodes and a metastatic focus >1 cm. No clear reason could be identified as to why these patients did not have RRA. The number of positive nodes was unrecorded for the remaining two patients.
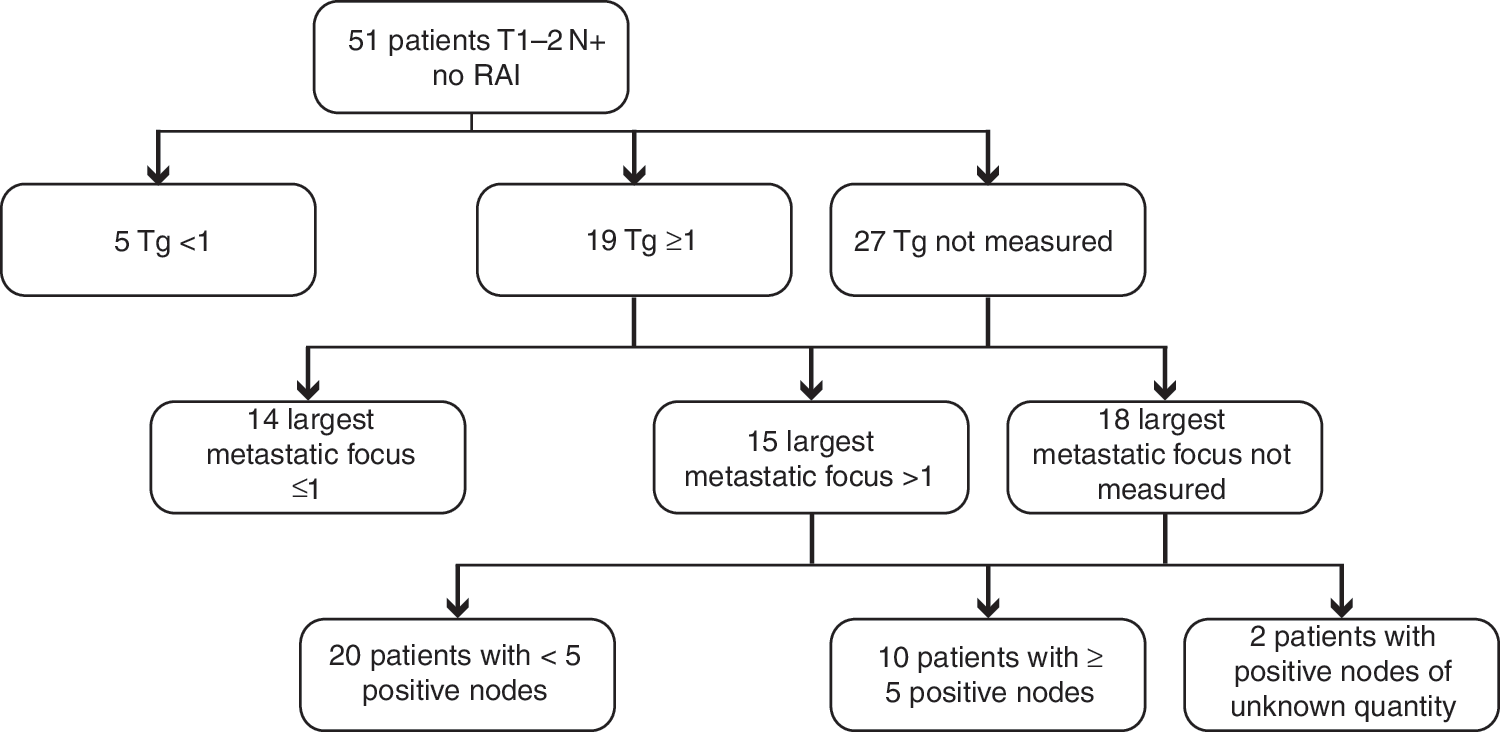
Analysis of T1–2 N1 patients who did not receive radioactive iodine, stratified by thyroglobulin level, size of largest node, and number of nodes excised.
For patients with T1–2 N1 disease, the five-year DSS and RFS were 100% and 92% respectively. There was only one local recurrence, and therefore no factors predictive of LRFS were identifiable. Table 8 shows predictors for RRFS and DRFS for this group. Of 15 regional recurrences, 13 were in the group who received RAI, with only two in the group that did not receive RAI. The five-year RRFS in patients who had RRA was 93%, compared with 100% for those who did not (p=0.263). For distant recurrence, all five distant recurrences occurred in patients who had RRA, giving a five-year DRFS of 93% versus 100% (p=0.274).
The ATA system for classifying recurrence in patients proved to be an effective predictor of both regional and distant recurrence in this group of patients, whereas the MSKCC system, designed to predict mortality, was not (Table 8).
Recurrence in patients with T3 or T4 disease
There were 444 patients who presented with locally advanced disease (pT3 or pT4). The median follow-up in this group was 64 months (range 1–282 months). Patient, tumor, and treatment details are shown in Table 9. Of the 444 patients, 276 also had N1 disease (62%). As expected, the vast majority of patients (371, 84%) received adjuvant RAI. The patients who had RRA were more likely to have had N1 disease. However, a select group of 73 patients did not have RRA. Those who did not have RRA were more likely to be N0 and have T3 disease (local disease >4 cm or the presence of microscopic ETE).
The five-year DSS and RFS rates were 98% and 87% respectively. Three patients recurred locally, all of whom had RRA (Table 10). Of 42 patients who had regional recurrence, 41 (98%) had RRA. There were 31 patients who had distant recurrence, of whom 28 (90%) had RRA. Of the 73 patients who did not have RRA, there were no local recurrences, only one regional recurrence and three distant recurrences. This indicated that the selection criteria used for these 73 patients was adequate.
The five-year RRFS of those who had RRA was 91% versus 98% for those who did not (p=0.019). Although on univariate analysis male sex, pT4 disease, and N-positive disease predicted outcome, RRA did not (Table 10). On multivariate analysis, pT4 disease remained an independent predictor of outcome. Patients with pT4 disease were 2.3 times more likely to have regional recurrence compared with those with pT3 disease.
The five-year DRFS within this group was 93%. Both the presence of T4 and N1 disease were predictive of outcome on univariate and multivariate analyses. Patients with pT4 disease were 2.3 times more likely to have distant recurrence compared to patients with pT3 disease. Patients with N1 disease were 3.7 times more likely to have distant recurrence compared to patients with N0 disease. Again, the RRA did not predict outcome, with a 93% five-year DRFS both in groups receiving and in those not having RRA (Table 10). The ATA system for classifying patients again proved to be an effective predictor of both regional and distant recurrence in this group of patients, whereas the MSKCC system was not (Table 8).
Discussion
The prognosis for patients diagnosed with WDTC is usually excellent (6,11,14 –17). Patterns of treatment have evolved over the last 25 years, with increasing use of RAI to ablate postoperative remnant thyroid tissue (5,6). Despite this, the evidence supporting its use is conflicting (18), particularly in those patients stratified as a low-risk group for death (12,16,17,19,20). Many groups have examined the role of RAI in the treatment of WDTC. Some have demonstrated improved survival in patients receiving postoperative RAI (21 –23), particularly in high-risk groups (14,17,20,24 –26). In more recent studies, other groups have found no significant differences in overall survival outcomes (6,17,27 –29). In terms of recurrence rates following treatment, again there is disagreement between studies, with some identifying improved rates (14,23,24,26) whilst others have not (6,29). Our study focuses on patients with PTC treated with a standardized surgical approach, involving extracapsular thyroidectomy and therapeutic neck dissection to remove proven or suspicious cervical lymph-node metastases. We do not practice or recommend subtotal or near total thyroidectomy when total thyroidectomy is indicated. We do not carry out elective central or lateral neck dissection, as it has not been proven to improve survival. Although we use adjuvant RAI to ablate any remnant of thyroid tissue in cases considered at higher risk of mortality (12), we are selective in the use of RRA for low- and even intermediate-risk cases. The objective of our study was to analyze our experience of the selective use of RRA in the management of WDTC.
We recognize that PTC presents to the clinician over a spectrum, ranging from patients with early-stage disease, which carries an excellent prognosis, to those with advanced locoregional disease in whom one can expect a worse outcome. To support the selective use of RAI in our patient cohort, we analyzed three subgroups: pT1–2 N0, pT1–2 N1, and pT3–4. In patients presenting with disease limited to the thyroid gland (pT1–2 N0), 64% (312 of 490) of our patients did not receive adjuvant RAI, with no detrimental impact on either DSS or RFS. This is in keeping with the findings of other groups in these low-risk patients (20). It is worth remembering that we do not practice routine elective neck dissections, and it is therefore likely that many patients in this group considered to have disease confined to the thyroid in fact had occult nodal metastases of questionable clinical significance. In similar patients who had evidence of regional metastases (pT1–2 N1), we chose to treat the majority of patients with RRA (74%, 142 of 193 patients). However, 51 patients were carefully selected not to have RRA. Of these patients, only seven saw an endocrinologist. Therefore, the selection of these patients was determined by surgeons with extensive experience in thyroid cancer management. These patients were mainly young, under the age of 45 years, with low-risk tumors. Analyzing these patients in more detail, five had a postoperative Tg <1 ng/mL. Of the remaining 46 patients, 22 had five or fewer lymph-node metastases. Data reported by Leboulleux et al. (30), Ito et al. (31), and by Sugatani et al. (32) have reported that the risk of recurrence in patients with fewer than five positive nodes is 3–8%, and therefore this could explain the low risk of recurrence in our patients. In addition, the size of the metastatic lymph node foci has also been reported to be predictive of recurrence (33), with the risk of regional recurrence being higher (32%) if the metastatic foci are larger than 1 cm. In our cohort of patients, 14 of the 51 had metastatic foci <1 cm. This left eight patients who had more than five positive nodes or metastatic foci >1 cm. We could not identify any reason for these patients not receiving RAI. However, there was no detrimental impact on either five-year DSS or RFS. Our survival and recurrence figures therefore indicate that, with careful selection, some patients with N1 disease can be treated safely without adjuvant RRA. At our institution, a highly selected group of young patients with pT1–2 tumors, fewer than five positive nodes, and with microscopic deposits of cancer may be managed with observation without RRA and with careful monitoring of thyroglobulin levels and regular ultrasound.
In higher risk patients with locally advanced (pT3 or pT4) disease, as expected, the majority of patients (84%, 371 of 444) were treated with RRA. Careful selection of some patients, principally those with T3 disease and N0 necks, allowed some patients not to have RRA. There was no detrimental impact on five-year DSS or RFS, thus supporting our selection process for RRA in this cohort of patients.
Like all retrospective studies, these data have limitations. There is obvious physician and patient-related selection bias in the decision to use RAI. However, our patients were all managed within a single tertiary referral cancer center with a fairly uniform approach to surgery, histopathological reporting, postoperative treatment, and follow-up. This cannot be said for studies based mainly on the records of national databases. Despite this, our approach to the use of RRA evolved during the time period studied, which limits the conclusions we can draw from our results. Those patients managed with RRA tended to be at higher risk of recurrence, being older with more aggressive tumors. For that reason, direct comparison of groups stratified by use of RRA is not reported. It should also be emphasized that all patients in this cohort were treated with extracapsular total thyroidectomy. Subtotal thyroidectomy is rarely carried out in our institution. Our excellent outcomes may therefore be a direct result of this complete and methodical technique of thyroidectomy. It should be emphasized that such results may not occur in outside centers that are not centers of excellence, in cases where thyroid cancer is diagnosed incidentally after surgery for benign goiter, or in countries where iodine deficiency is endemic. Our results should therefore be interpreted with caution, as they only apply to centers with a similar surgical approach to our own. Follow-up protocols during the time period studied were based upon clinical examination, without the routine use of thyroglobulin or annual ultrasound. Therefore, most recurrences were palpable structural disease rather than sonographically identified small volume, or “biochemical” recurrence. Our data support our selection criteria for RRA. In particular, our data illustrate that for intraglandular T1–2 N0 disease, survival and recurrence are similar in the RRA and no RRA groups, suggesting RRA is not required in the majority of cases. For similar patients with N1 disease, RRA is generally advocated. However, even in this group, there is a highly select group of young patients with low-volume neck disease who can be treated safely without RRA. For advanced stage T3 or T4 disease, a select group of T3 N0 patients can be safely managed without RRA. Our data analysis shows the accuracy of the MSKCC risk stratification system for analyzing death and also the accuracy of the ATA risk stratification system for analyzing recurrence.
Following surgical therapy, a decision must be made between the surgeon, endocrinologist, nuclear medicine physician, and patient whether to recommend RRA. Current international guidelines recommend consideration of RRA for all tumors that are >1 cm or that are associated with extrathyroid extension or that have spread beyond the thyroid (8 –10). Given the known rates of occult nodal metastasis to the central (34) and lateral neck (35), clinicians may therefore consider the use of RRA in almost all patients they encounter. Our data show that select patients can be identified that can be safely managed without adjuvant RRA. We believe that this selection is important, as the side effects of RAI are increasingly recognized. A number of groups have shown that iodine uptake outside thyroid tissue results in significant salivary and lacrimal dysfunction (36 –39). A recent report on the effect of RAI following total thyroidectomy suggested increased rates of dysphagia in patients who received RAI (39). These late side effects have been reported to have a negative impact on quality-of-life scores for patients who receive high levels of RAI activity (40). Perhaps more important is the reported increased risk of second primary malignancies developing in patients treated with high levels of RAI activity, with groups reporting increased rates of salivary and hematological malignancies following RAI therapy (5,41). It is also important to realize that the use of RRA has not been conclusively proven to reduce mortality or recurrence related to PTC in the absence of distant metastases. These patients are likely to do well following appropriate surgical management, and RRA should be considered only for the patients most likely to benefit. This study was not designed to assess the efficacy of RAI, which we believe may be beneficial in properly selected patients who present with PTC. The results of this study should not lead clinicians to reject the use of RRA in lower-risk patients. However, a balance between risk and benefit must be made on an individual patient basis. We report that select patients can be managed safely without postoperative RRA, resulting in excellent outcomes.
In conclusion, following complete tumor resection, with total thyroidectomy, the majority of patients with low-risk local disease and even some patients with more advanced stage (pT3) tumors or regional metastases have low rates of recurrence and high rates of survival when managed without RRA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.