
Abstract
Background:
In some patients, papillary thyroid carcinoma (PTC) lymph-node metastases are noted to be black (dark) in color at the time of surgical removal. The goal of this project was to determine histological, genetic, and clinical features that are associated with regional black PTC metastasis.
Methods:
Fifteen patients with black PTC metastases (black-PTC) were compared to a control cohort of 15 patients with nonblack PTC metastasis (nonblack PTC). Each sample was evaluated for the histological characteristics, BRAF V600E mutational status, and associated patient clinical data.
Results:
The degree of cystic degeneration (80% vs. 27%, p=0.004), percent hemosiderin deposition (20% vs. 6%, p=0.001), and presence of classical variant (100% vs. 67%, p=0.018) were significantly greater in black PTC than nonblack PTC (α=0.05). Other results were not significantly different.
Conclusion:
This study demonstrates that black compared to nonblack metastases have a greater degree of cystic degeneration and hemosiderin deposition leading to discoloration, and a trend toward an increased incidence in BRAF V600E mutations. This study is the first of its kind to describe the clinical, pathological, and genetic features associated with black PTC lymph-node metastasis.
Introduction
Materials and Methods
Fifteen patients were identified with black PTC metastases at surgery (black-PTC cohort). Figure 1 demonstrates the typical intraoperative findings during the surgical procedure of patients within this cohort. Figure 2 illustrates the specimen as it is received for gross evaluation. A control cohort was established with 15 consecutive patients having PTC metastasis that were not identified as black at surgery (nonblack PTC cohort). The accuracy of diagnoses of PTC on all cases was confirmed. Each case was evaluated for percent involvement of lymph nodes by the metastatic PTC, presence of associated microcalcifications, presence and extent of extracapsular extension, presence and extent of cystic degeneration, and the histologic architecture of the tumor. Special stains were performed by the clinical laboratories at Penn State Hershey Medical Center using standard procedures for melanin (Fontana–Masson silver method), hemosiderin (Gomori's iron stain), CD31 (clone JC70), and Ki-67 (clone MIB-1). CD31 was used to calculate a mean vessel density of the tumor and of its adjacent lymph node by taking the mean of the number of CD31+ vessels present in four different 400× fields. BRAF V600E mutational status was determined by a polymerase chain reaction (PCR) method using archived formalin fixed paraffin embedded tissue. Patient data, including demographic characteristics and results of imaging studies, were collected from the clinical medical record. Comparisons between proportions were performed by the Fisher Exact and Barnard's exact test, which is a more powerful alternative in 2×2 tables and applicable when either the row or column marginals of the table are fixed, as was the case in this study (8,9). Only Barnard p-values are displayed. Comparisons between continuous variables were performed by a nonparametric Wilcoxon exact rank sum test. SAS v9.3 was used to conduct the Fisher Exact tests and Wilcoxon tests, and a R statistics system routine was used for the Barnard's test (10).
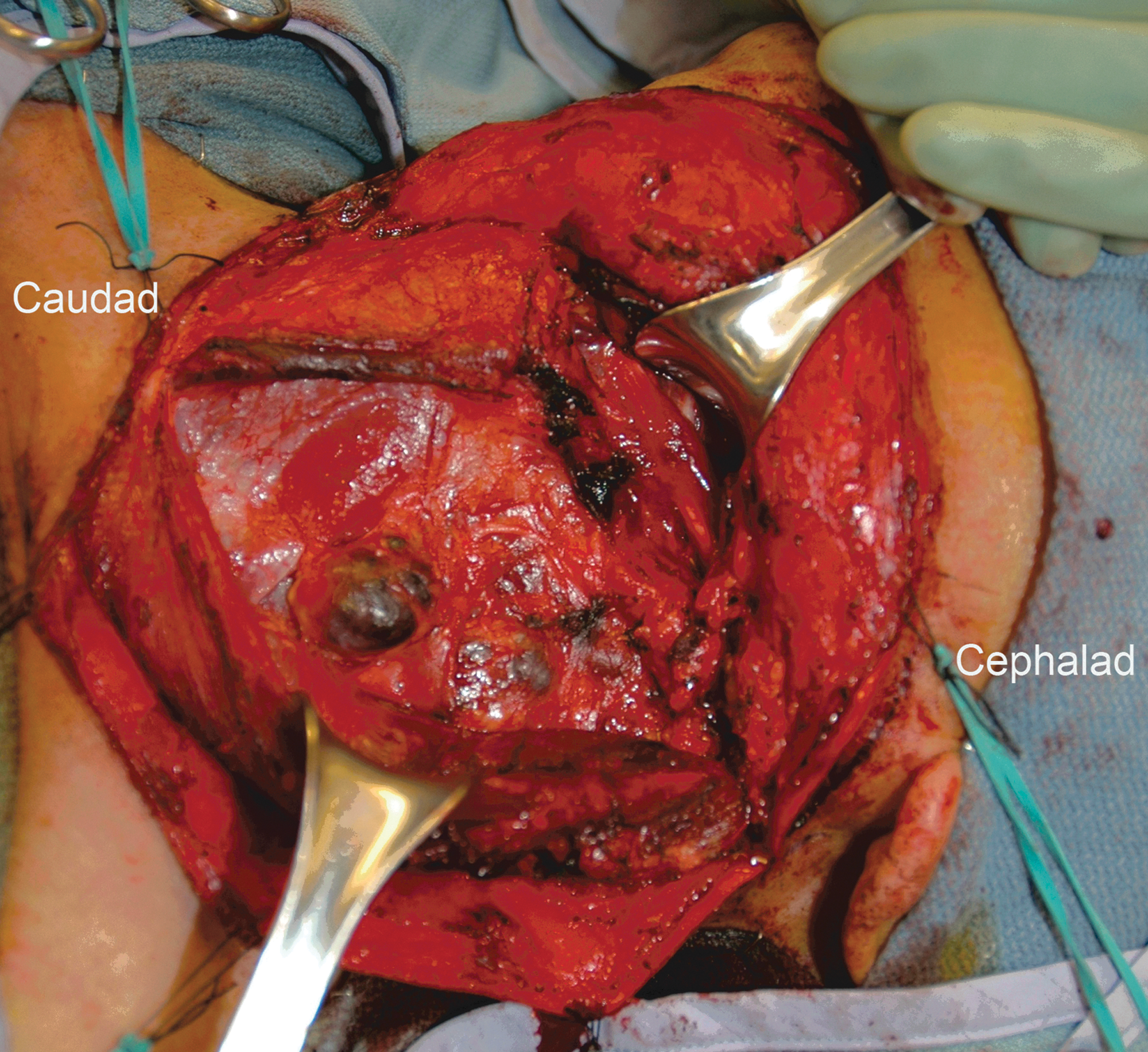
Characteristic appearance of black papillary thyroid carcinoma (PTC) lymph-node metastasis within the lateral neck at the time of neck dissection. Color images available online at
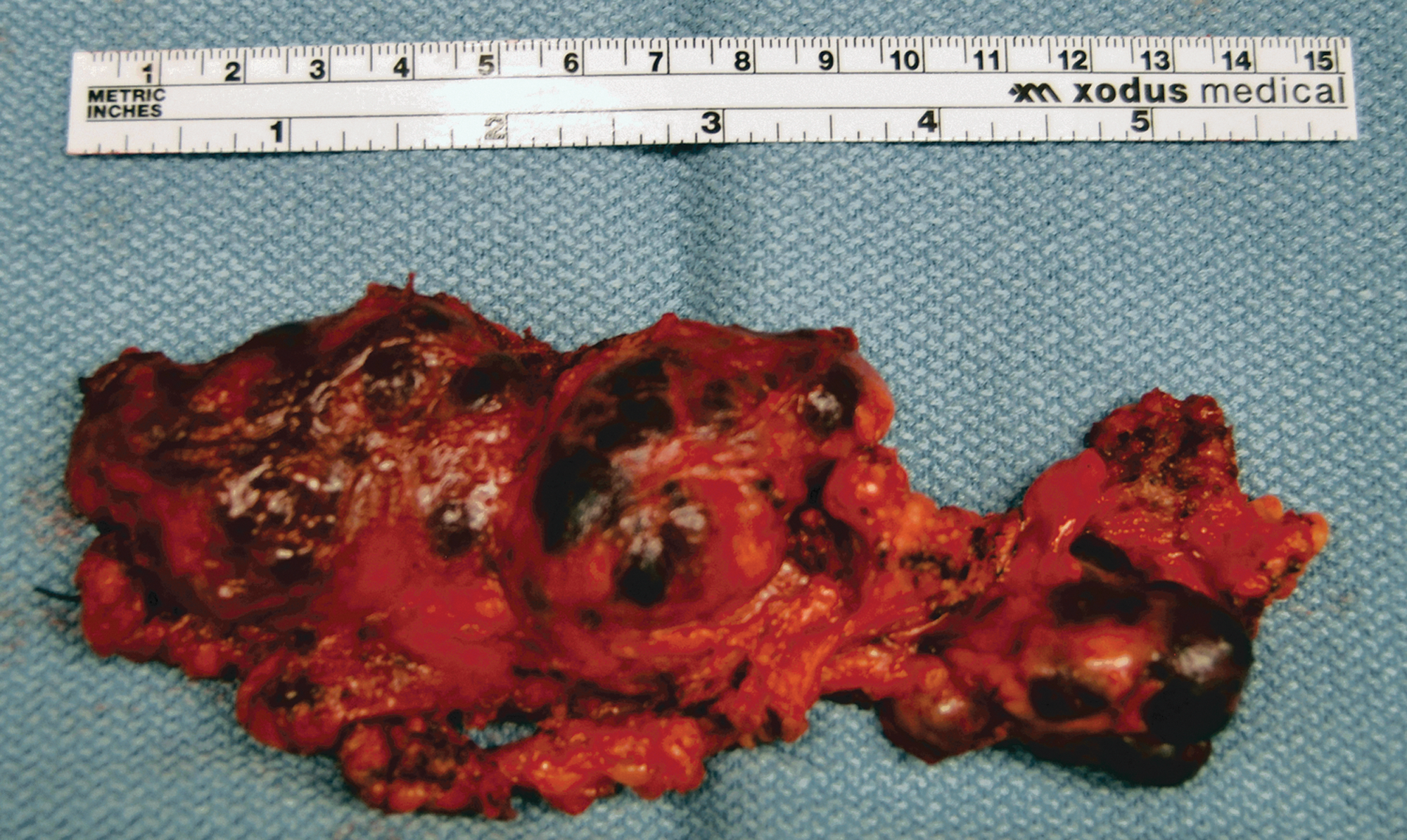
Black PTC metastasis in levels II–IV lymph-node dissection specimen after resection. Color images available online at
Results
Referring to Table 1, within the black-node PTC metastasis cohort, the average age was 51 (standard deviation [SD]=17.5) as compared to an average age of 44 (SD=16.4) within the nonblack node PTC metastasis cohort (p>0.05). The male-to-female ratio was 9:6 versus 7:8 (p=0.32). In the black node cohort, 9:15 had recurrent presentation compared to 7:15 in the nonblack node cohort (p=0.585). Node size was 1.93 (SD=1.62) versus 1.63 (SD=0.77), p=0.789. No significant difference in demographics was detected between groups, providing no evidence of bias attributable to differing case mix.
Data are reported as number/total or mean (standard deviation) of 15 subjects in each cohort.
Referring to Table 2, in the black-nodes cohort, 6:14 patients had T3 disease compared to 5:14 in the nonblack-node cohort (p=0.822). The primary PTC was multifocal in 11:14 of black nodes compared to 6:13 of nonblack nodes (p=0.115), with regional metastasis identified in 15:15 black nodes compared to 13:14 nonblack nodes (p=0.497). In the black nodes, 11:15 of the lymph nodes were present within the central compartment of the neck compared to 12:15 nonblack nodes (p=0.783). Bilateral metastasis occurred in 7:15 of black nodes compared to 3:15 nonblack nodes (p=0.142). Radio iodine uptake was noted in 7:15 black nodes versus 7:14 nonblack nodes (p=0.956). Fluorodeoxyglucose-avidity was noted in all patients for whom testing was performed.
Data are reported as number/total or mean (standard deviation) of 15 subjects in each cohort.
PTC, papillary thyroid carcinoma; FDG, fluorodeoxyglucose.
The predominant morphologic variant of PTC identified was classical PTC (15:15 cases) within black nodes versus 10:15 in nonblack nodes (p=0.018). The remainder of nonblack cases demonstrated a follicular variant of PTC. Patient rates with cystic degeneration present in the metastatic tumor within the black cohort was 12:15 as compared to 4:15 in the nonblack cohort (p=0.004; Fig. 3A, B). There was no significant difference in the presence of extracapsular extension (black nodes 2:15, nonblack nodes 2:15, p=1.00) or presence of calcifications (black nodes 9:15, nonblack nodes 11:15, p=0.526).

Comparison of histological features of black versus nonblack PTC metastasis. Black-PTC metastasis
Hemosiderin deposition was observed in 15:15 of black nodes and 10:15 of nonblack nodes (p=0.526) and, on average, involved a greater percentage of the nodes in black cases (20%) than in nonblack cases (6%, p=0.001; Fig. 3C, D). Melanin deposition was virtually absent in all nodes in both cohorts. CD31 was used to assess mean vessel density within the tumor and adjacent lymph node. No significant difference in mean vessel density was noted within the tumor (black nodes 36.3%, nonblack nodes 16.3%, p=0.153). There was no significant difference in Ki-67 proliferative activity (black nodes 3%, nonblack nodes 4%, p>0.05). The BRAF V600E mutation was identified in 13:15 of black nodes and 9:15 of nonblack nodes (p=0.119).
Discussion
This study is the first of its kind to describe the clinical, pathological, and genetic features of PTC lymph node metastases with a black (dark) appearance at surgery. Cystic degeneration is a common pathologic finding in tumors, and occurs in up to 40% of patients with PTC metastases (6,11,12). It is sometimes accompanied by varying degrees of hemorrhage with the blood and hemosiderin pigment producing dark, brown, purple, or black discoloration of the fluid and tissues. Our findings demonstrated that the clinically identified black nodes have a greater degree of cystic degeneration, which is accompanied by a greater hemosiderin deposition than present in their nonblack counterparts. Blood and hemosiderin pigmentation are well known as a cause of dark, purple, or black discoloration of tissues. Other known causes such as melanin and minocycline therapy were excluded in our cases by their absence in the tumor and associated tissues on examination using the appropriate identifying stains.
Although cystic degeneration is a common finding in PTC lymph node metastases, it is possible that patients with cystic degeneration and hemorrhage causing black PTC metastasis represent a distinct subpopulation. In our study, there is a trend toward an increased BRAF V600E positivity rate in the black-PTC cohort. In sporadic PTC, activating BRAF mutations are identified in up to 70% of PTC (13,14) and are thought to lead to dysregulation of the RAF/MEK/MAPK pathway, in turn promoting dedifferentiation, proliferation, and protection against apoptosis in involved tumors. The presence of a BRAF mutation can be associated with increased clinically aggressive disease including decreased disease-specific survival, extrathyroidal extension, and tumor size (14 –16).
From the results of our study, we hypothesize that black PTC metastases may represent a subpopulation of thyroid tumors in which cystic degeneration and hemorrhage are a result of tumor overgrowth and/or disruption of its blood supply. It is possible, however, that this black discoloration is the inevitable end point of all lymph-node metastasis of PTC and that the nonblack group has not yet reached this growth end point. The pathologic findings in the black lymph-node group may be mediated by BRAF mutations through multiple downstream pathways. Several studies have shown increased expression of vascular endothelial growth factor (VEGF) in BRAF positive PTC (17,18).
A recent ultrasound study indicated that cystic architecture and hypoechogenicity predict BRAF positivity (19). Other ultrasound studies of metastatic lymph nodes have demonstrated avascular areas, tortuous vessels, and abnormal distributions of vessels with increased flow at the periphery of the node, often in association with loss of the normal echogenic hilum. As tumor deposits increase in a node, hyperechogeneity and vascular flow increases (20). Using these ultrasound studies as a guide, we attempted to characterize vascular patterns examining CD31 immunohistochemical stains, but analysis of the data did not identify a significant difference in mean vessel density between black-PTC and nonblack PTC cohorts. It is possible that VEGF induced angiogenesis within a tumor is unstable and prone to disruption, and once the blood supply is lost, tumor ischemia and necrosis led to the greater degree of cystic degeneration and hemorrhage causing the gross discoloration.
Langer et al. (20) state that, on ultrasound, the most specific feature of metastatic PTC is the tendency of these nodes to undergo cystic degeneration. Affected nodes may contain a small solitary cystic area, multiple scattered cystic areas, or may undergo near complete degeneration of the parenchyma with only a fluid-filled cyst remaining. We suspect that the black discoloration is part and parcel of the phenomenon of cystic degeneration.
This manuscript provides the first systematic description of the phenomenon of black (dark) PTC lymph-node metastases. Further studies are needed to understand why the morphological phenomenon occurs. Our data raise the possibility that BRAF V600E mutations may be implicated in the phenomenon and, if subsequent studies would sufficiently support our hypothesis, may provide the surgeon with a first indication of more aggressive disease that may require more extensive treatment such as a therapeutic lymph-node dissection at the time of discovery.
Footnotes
Acknowledgments
We acknowledge the assistance of the Community Science and Health Outcomes Core (CSHO) from the Penn State Hershey Cancer Institute in the preparation of this manuscript.
Author Disclosure Statement
The authors have no grant support or other financial interests to disclose.