
Abstract
Background:
Excessive iodine exposure is associated with thyroid dysfunction and thyroid autoimmunity. Most surgical hand-scrub solutions contain large amounts of iodine, and transcutaneous and mucosal absorption of iodine from these antiseptic solutions has been demonstrated. In this study we determined the effect of hand scrubbing with iodine-containing surgical hand-scrub solutions on urinary iodine concentrations (UICs) in operating room staff.
Methods:
The study included 117 surgeons and surgical nurses from two different hospitals who often used surgical hand-scrub solutions as the iodine exposure group and 92 age-matched hospital staff from nonsurgical units of the same hospitals as the controls. In the iodine exposure group, 39 subjects (from hospital 1) used iodine-containing hand scrub solutions intermittently, and the remaining 78 in the surgical staff (from hospital 2) used only iodine-containing hand-scrub solutions. Morning spot urine specimens were collected from all participants for the analysis of UIC.
Results:
The operating room staff had significantly higher UICs compared to the control group (142 μg/L [12–822 μg/L] vs. 89 μg/L [10–429 μg/L], p<0.001). UICs from 39% of the subjects from hospital 2 were found to reach levels higher than 300 μg/L.
Conclusion:
Scrubbing with iodine-containing solutions might lead to iodine excess among surgical staff. Further studies investigating the effects of hand scrubbing with iodine-containing products on thyroid function and on thyroid antibodies of the operating room staff are needed to determine the consequences of this high iodine exposure.
Introduction
One of the most important uses of iodine is as a disinfectant in skin soaps. Notably some surgical hand-scrub solutions, which are considered to be safe antiseptics, contain large amounts of iodine and are commonly used as broad-spectrum topical disinfectants (4). Transcutaneous absorption of remarkable amounts of iodine from these antiseptic solutions has been demonstrated in patients with burn wounds. This has also been noted in infants, possibly related to their thin and therefore more permeable skin (5,6). In animal experiments, transcutaneous absorption of povidone-iodine, a type of iodine-rich antiseptic solution, from healthy skin has also been reported (7). Additionally, exposure to povidone-iodine via the skin or umbilical cord of preterm infants can lead to elevated plasma iodine levels, and consequently increased urine iodine levels and thyroid dysfunction (8,9). In contrast, similar studies conducted in North America have not shown any thyroid dysfunction despite elevated iodine levels in the urine of preterm infants indicating high exposure (10,11). With regard to transcutaneous iodine absorption in healthy adults, only a few cases or limited studies have been performed (12 –14). The skin of healthy adults should be less permeable that that of neonates or preterm infants. Among healthy adults, some of the occupations that involve iodine exposure are those in operating rooms for which hand scrubbing is done with iodine-containing solutions. As of yet, there has been no study of the effect of hand scrubbing with such solutions on the urinary iodine concentrations (UICs) of surgeons and other operating room staff. In the present cross-sectional double-center study, we determined the effects of hand scrubbing with iodine-containing antiseptics on the UIC of operating room staff. The study was performed in a region of mild to moderate iodine deficiency.
Materials and Methods
The study involved 117 operating room staff from two different tertiary care hospitals (mean age 35±8.6 years, 37 women and 80 men) who used iodine-containing surgical hand antiseptics (iodine exposure group) and 92 age-matched hospital staff (mean age 33±9.5, 33 women and 84 men) from nonsurgical units who did not have any exposure to iodine-containing hand-scrub solutions. The volume of operations in hospital 1 and hospital 2 was similar, with an average number of operations under general anesthesia of about 25,000 cases/year. In the iodine exposure group, 39 subjects (from hospital 1) used iodine-containing hand-scrub solutions intermittently (they used hand scrubs with or without iodine randomly) and the remaining 78 surgical staff (from hospital 2) used only iodine-containing hand-scrub solutions (povidone-iodine products). In the iodine exposure group, the subjects scrubbed up to the elbow joint for at least for 5 minutes to standardize the iodine effect. All of the participants had actively participated in operations for at least the previous 2 weeks. Subjects with a history of iodine exposure, including having had any involvement with interventions using iodine-containing contrast agents or a history of thyroidal diseases, were excluded from the study. Morning spot urine specimens were collected from all participants for the analysis of UIC on Fridays. Informed consent was obtained from each subject in the study. Urine samples were kept at 4°C in deionized tubes and analyzed within 30 days after the collection. UICs were determined using the method recommended by the World Health Organization–International Council for the Control of Iodine Deficiency Disorders (WHO-ICCIDD); specifically, the calorimetric ceric ion arsenous acid wet ash method based on the Sandell–Kolthoff reaction, using Fisher® reagents (Spectrum Chemicals and Laboratory Products, Gardena, CA) and a spectronic 20 (Thermo Scientific Instruments Group, Madison, WI) and Genesis autoanalyzer (McKinley Scientific, Sparta, NJ) (15) in our iodine laboratory controlled by the Ensuring the Quality of Urinary Iodine Procedures (EQUIP) program of the Centers for Disease Control and Prevention.
Statistical analysis
All parameters are shown as the median and the interquartile ranges (IQRs). Differences among three groups for urinary iodine concentrations were evaluated by Kruskal–Wallis variance analysis. When the p-value from the Kruskal–Wallis test statistics was significant, a multiple comparison test was used to determine the groups that differed from each other. A p<0.05 was considered as statistically significant. Analyses were carried out using the SPSS software version 15.0 (SPSS, Chicago, IL).
Results
Demographic data and UIC levels of the study subjects are summarized in Figure 1 and Table 1. The median values of UIC of operating room staff from hospital 1 (126 μg/L [IQR 98–155]) and hospital 2 (166 μg/L [IQR 128–410]) were significantly higher compared to the control group (89 μg/L [IQR 42–139], p<0.017 and p<0.001, respectively; Table 1). When subjects from both hospitals were analyzed together, the median UIC (142 μg/L [IQR 114–347]) was significantly higher compared to the control group (p<0.001). The median values of UIC of operating room staff from hospital 2 had significantly higher levels compared with hospital 1 (166 μg/L [IQR 128–410] vs. 126 μg/L [IQR 98–155], p<0.001) as well.
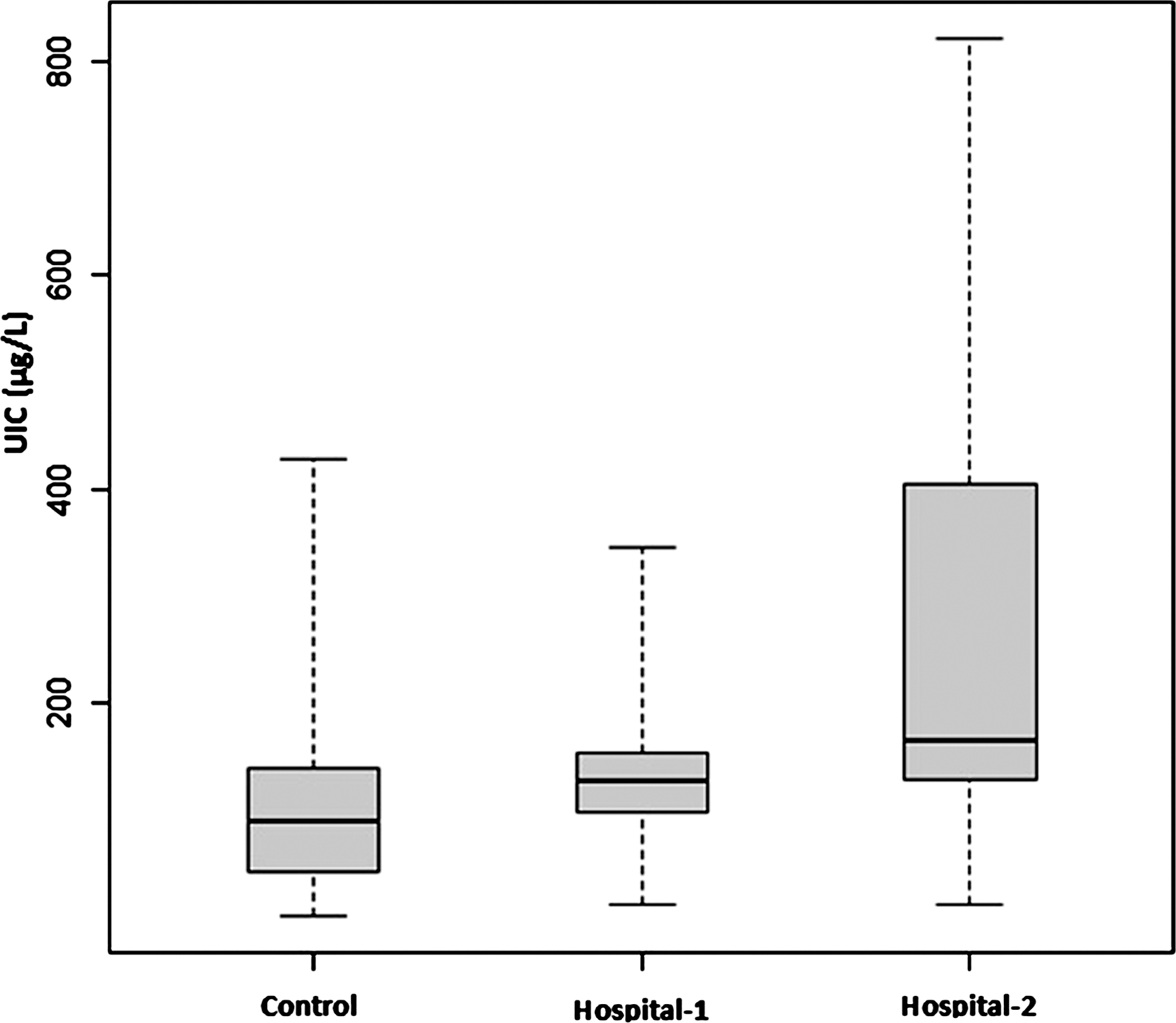
The median values of urinary iodine concentrations (UICs) of operating room staff from hospital 1 and hospital 2 had significantly higher levels compared to the control group (see Table 1).
Compared to the control group.
F, female; M, male; UIC, urinary iodine concentration; SD, standard deviation; IQR, interquartile range; HSG, hand-scrubbing group.
UIC levels from 39% (30/78) of the subjects, involving eight cardiothoracic surgeons, seven nurses, five general surgeons, four urologists, two gynecologists, two neurosurgeons, and two orthopedic surgeons in the iodine exposure group from hospital 2, were found to be >300 μg/L. One of the neurosurgeon's from hospital 1 had a UIC >300 μg/L.
Discussion
In this cross-sectional double-center study, we demonstrated for the first time that the operating room staff can have significantly higher levels of UIC compared with the staff from nonsurgical units. In nearly 40% of the staff using solely the iodine-containing scrub solutions, UICs were >300 μg/L. According to WHO-ICCIDD, a median urinary iodine level >300 μg/L indicates excessive iodine intake for a surveyed population and can be associated with adverse health consequences. However, the upper limit for iodine intake is not well defined on an individual basis (16).
Povidone-iodine is widely used as a topical antiseptic for mucosa, skin, and surgical procedures. Topical preparations of povidone-iodine contain 8% to 12% iodine (17). Elevated serum or urine iodine levels have been reported in patients with skin burns (5,18), neonates (19), infants (6), and patients with pressure wounds (20 –22), who were treated with povidone-iodine. It was previously accepted that adult skin is much less permeable and therefore, transcutaneous absorption of iodine might be ignored. However, Tomoda et al. (13) demonstrated in iodine-sufficient regions that the UIC of postsurgical patients, whose skin was prepared only once using povidone-iodine, was markedly increased compared to the preoperative UIC. It has also been shown that acute exposure to povidone-iodine preoperatively in infants from endemic iodine-deficient regions and to nonionic contrasts in some procedures such as radiography can cause thyroid dysfunction (6,23). In the present study, the median UIC of the control group was 89 μg/L, a value that is below an optimal UIC (>100 μg/L). Moreover, we demonstrated in a recent study that the median UIC of the Turkish population was 107 μg/L after iodine prophylaxis; however 50% of the population still experienced various degrees of iodine deficiency (severe iodine deficiency in 7.2% of the population, moderate in 20.6%, and mild in 19.3%) (24).
The major aim of this study was to assess UIC in seldom, repetitive, and continuous users of iodine-containing antiseptics. We found that repetitive povidone-iodine use among the operating-room staff may cause excessive iodine exposure by transcutaneous absorption. A similar study was conducted with a limited number of nonsurgical ward nurses, who had to use povidone-iodine products for hand washing and gargling several times a day in Japan (14). Although it was demonstrated that the serum levels of iodine did not significantly increase in the group using povidone-iodine, the mean serum-free thyroxine levels were slightly, but significantly, higher compared to the controls. However, this study included only a small group of nurses, and the mucosal or cutaneous exposure time to the povidone-iodine products were probably shorter compared to operating room staff. The operating room staff might also be exposed to more gaseous forms of iodine because of the large number of people using hand scrubs within the same time-frame and in the same scrubbing sinks, in addition to the topical, preoperatively applied povidone-iodine on patients in the operating rooms. Interestingly, besides the repetitive use of povidone-iodine, residual effects of iodine-based disinfectants have also been demonstrated after the solution is removed by rinsing the skin with water. These effects were mostly due to the retention of the agents in the skin surface (25).
Although the individual participants were questioned whether they had any thyroid disorders, a limitation of the study is that thyroid function tests were not done.
A recent study suggested that on an individual basis, more than 10 urine samples are needed to evaluate iodine excretion correctly (26). Another study reported that a transient increase in urinary iodine levels was followed by a return to basal values on the third or fifth day after a single topical application of povidone-iodine (13). In the present study, as other limiting factors, UIC measurements of the study subjects were not repeated and urine creatinine levels were not measured. Nevertheless, the urine specimens were collected only on Fridays in order to detect the change of UIC, and this method was consistent with findings of the latter study (13).
In conclusion, it was demonstrated for the first time in this study that operating room staff using iodine-containing surgical hand antiseptics are exposed to significantly higher levels of iodine compared to the staff from nonsurgical units. Furthermore, approximately 40% of all operating room staff, especially those using iodine-containing solutions continuously, were exposed to iodine levels that exceeded the recommended daily intake. Further studies investigating the effects of hand scrubbing with iodine-containing products on thyroid function and thyroid antibodies in the operating room staff are needed to clarify the issue.
Footnotes
Author Disclosure Statement
The authors declare that no competing financial interests exist.