
Abstract
Background:
Well-differentiated follicular thyroid carcinomas (FTCs) usually act indolently, while aggressively acting tumors are difficult to detect early enough. Estrogen receptors (ERs) have prognostic significance in many cancers. Thyroid diseases, including neoplasms, are associated with the female sex. The prognostic significance of ERs in FTCs has not been reported previously.
Methods:
We studied the role of ERα and ERβ in 83 cases of follicular thyroid adenoma (FTA) and 43 FTC cases, including seven cases of poorly differentiated FTC, obtained from the Department of Surgery, Helsinki University Central Hospital between 1990 and 2009. Patient follow-up was conducted until March 2011. Expression of ERα, ERβ, and MIB-1/Ki-67 was investigated by immunohistochemistry and correlated with clinicopathological characteristics, including survival.
Results:
Two major observations were apparent. First, ERβ expression was significantly higher in FTA than in FTC, and it was a stronger differential diagnostic marker than MIB-1/Ki-67. Second, low ERβ expression correlated with poor survival in FTC. All cancer-specific deaths due to FTC were among low ERβ-score patients.
Conclusion:
ERβ is a differential marker for malignancy and could thus be used as a preoperative tool. FTC patients with a low ERβ score need more thorough follow-up and may benefit from more aggressive treatment.
Introduction
FTC is approximately four times more common in women than in men. Hormones, especially estrogens, are thought to have an influence on this female preponderance. The effects of estrogens are mainly mediated through nuclear estrogen receptor (ER) subtypes α and β (6). ERs are members of the superfamily of nuclear receptors able to transduce extracellular signals into transcriptional responses, and they are similar in architecture to other steroid hormone receptors. Steroid hormone receptors differ from other nuclear receptors in the nature of their ligands, in their relation to a range of heat-shock proteins, and in their binding to estrogen response elements (EREs) in the promoter regions of target genes (6,7). The ERα and ERβ genes are located on different chromosomes, their proteins have different cellular distributions, they regulate different genes, they elicit different transcriptional responses, and they can oppose each other's action (7,8). Numerous human tissues express both ER subtypes, including breast (9), ovary (10), prostate (11), lung (12), colon (13), and pancreas (8). Varying expression has also been shown in the thyroid tissue for both ERα and ERβ (14 –17).
ER expression in cancer tissues has a prognostic value. High ERα expression is associated with a better survival and a better response to antiestrogen therapy in breast cancer (18) and a better survival in ovarian cancer (19), but with a poorer survival in lung cancer (12). Low ERβ expression and poor survival occur in breast cancer (9), ovarian cancer (20), and lung cancer (21). To our knowledge, the prognostic value of ERs in FTC has not been reported. Here, we evaluated the immunohistochemical expression of ERα and ERβ in a large series of different follicular thyroid neoplasms.
Materials and Methods
Patient material
Tissue specimens were collected from 125 patients, who underwent thyroid surgery for follicular neoplasms at the Department of Surgery, Helsinki University Central Hospital (HUCH) between 1990 and 2009. The patients were identified from the database of the Department of Pathology, HUCH. Clinical data were obtained from patient records of the Department of Surgery and the Department of Oncology, HUCH, with survival data from the Population Register and cause of death from patient records and from Statistics Finland for the follow-up time until March 2011. The study was approved by the Surgical Ethics Committee and the National Supervisory Authority for Welfare and Health, Helsinki, Finland (Valvira).
The tumors were reclassified according to the World Health Organization (WHO) classification of tumors of endocrine organs (1). Immunohistochemical thyroglobulin staining was performed to ensure the viability of tissue specimens as well as to confirm the diagnosis. A tumor was considered oxyphilic if at least 75% of its cells were oxyphilic. Highly cellular tumors with evidence of increased proliferation activity as well as nuclear atypia, but lacking invasion, were classified as atypical adenomas. Invasive growth was required for the diagnosis of FTC. Poorly differentiated FTC (PDFTC) cases were separated from cases with well-differentiated FTC (WDFTC), the former showing thyroglobulin-positive tumor cells with high proliferative activity.
The tissue material consisted of 43 FTC and 82 FTA cases (Fig. 1). The consecutive FTC material included 36 cases of WDFTC and 7 of PDFTC. WDFTC cases were further classified into 9 cases of minimally invasive (focal capsular and/or vascular invasion) and 27 of widely invasive FTC. The FTA material included 9 atypical adenomas, 29 oxyphilic adenomas, and 44 consecutive typical FTA. Clinicopathological features, such as sex, age at diagnosis, oxyphilia, necrosis, proliferation index, capsular invasion and vascular invasion, nodal invasion, tumor-node-metastasis classification (TNM), tumor stage, extrathyroidal invasion, as well as primary and secondary metastasis were recorded.

A flow chart introducing the study's tumor material. The gray area inside boxes represents the proportion of oxyphilic tumors.
Each carcinoma patient received a 30–120 mCi radioactive iodine (RAI) ablation dose within ∼4–6 weeks after thyroidectomy. Advanced disease required additional RAI treatment, radiation, surgery, or chemotherapy. The mean follow-up time for all FTC patients was 9.2 years (range 0.1–20.5 years), for WDFTC patients 10.1 years (range 0.1–20.5 years), and for PDFTC patients 4.6 years (range 0.6–9.4 years).
Tissue microarray
For tissue microarray (TMA) construction, formalin-fixed paraffin-embedded hematoxylin–eosin slides were re-evaluated and representative areas were selected. From corresponding tissue blocks, tumor punctures were taken from two representative areas from the border and one from the central area of the tumor. From these areas, cores were obtained and inserted into a recipient paraffin block with a total of 56 cores, using a tissue microarrayer (Beecher Instruments, Silver Spring, MD; MTABooster® Version 1.01 for Beecher Manual Arrayer, Alphelys, Plaisir, France). Three sections from different levels were cut from each TMA block to obtain nine spots per tissue sample for immunohistochemical analysis.
Immunohistochemistry
The TMA samples were used for immunohistochemistry, as described previously (22). For MIB-1 evaluation, whole-tissue slides were used. Immunostaining was performed in an Autostainer 480 (LabVision, Fremont, CA), using the Dako REAL EnVision Detection System, Peroxidase/DAB+, Rabbit/Mouse (DakoCytomation, Glostrup, Denmark). The primary antibodies were monoclonal ERα (1:50, clone ER-6F11; Novocastra Laboratories Ltd. [Newcastle upon Tyne, United Kingdom]), polyclonal ERβ (1:100, clone H-150, sc-8974; Santa Cruz Biotechnology, Inc., Santa Cruz, CA), monoclonal MIB-1 (1:150; DakoCytomation,), and polyclonal thyroglobulin (1:2000, DakoCytomation) antibodies. Mammary tissue was used as a positive control and a slide without a primary antibody as a negative control. Immunohistochemical stainings of ERα and ERβ were nuclear and were scored by the percentage of positive nuclei with a 5% accuracy. The scoring pattern is shown in Figure 2. MIB-1 staining was scored with an evaluation scale of 0%–2%, 2%–5%, 5%–10%, and >10% positive nuclei. The stainings were scored independently by two researchers (J.H. and A.H.). In case of a disagreement, a consensus score was determined.
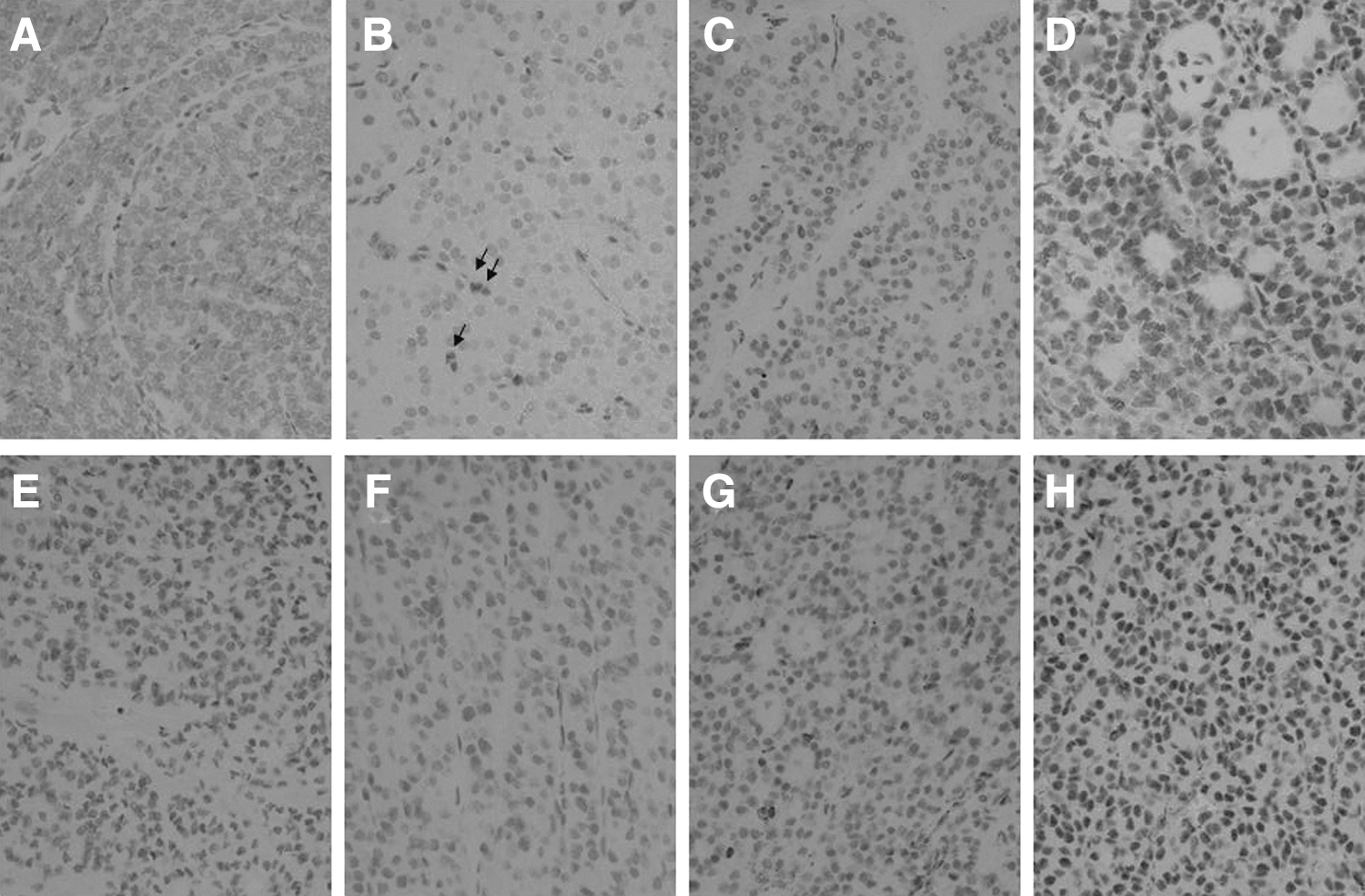
Scoring of estrogen receptor β (ERβ) in follicular thyroid carcinomas
Statistical methods
The correlation between the immunohistochemical expression of ERα or ERβ and clinicopathological features was assessed with a χ2 test or with Fisher's exact test when applicable. The Kaplan–Meier method with log-rank test was used to estimate the survival of patients and the prognostic value of ERβ expression. Patients alive at the end of the follow-up period and patients who died from unrelated causes were considered as censored cases. A p-value ≤0.05 was regarded as statistically significant. Receiver–operating characteristic (ROC) curve analysis was used to compare the diagnostic value of ERβ and MIB-1 to calculate the area under the curve (AUC) value. The logistic regression model was used to evaluate whether ERβ and MIB-1 provided independent diagnostic information and whether their combination would improve accuracy. Statistical analyses were performed with SPSS 17.0 software (IBM–SPSS, Armonk, NY).
Results
ERα expression in thyroid neoplasms
ERα expression was mainly negative in both adenomas (89%, 73/82) and carcinomas (93%, 40/43; Table 1). Further evaluation of carcinoma subgroups showed negative ERα expression in 100% of PDFTC (7/7), 92% of WDFTC (33/36), 93% of oxyphilic FTC (14/15), 93% of nonoxyphilic FTC (26/28), 89% of minimally invasive FTC (8/9), and 94% of widely invasive FTC (32/34). Negative expression patterns were also seen in FTA subgroups: 91% of typical FTA (40/44), 83% of oxyphilic FTA (24/29), and 89% of atypical FTA (8/9) were negative for ERα.
Boldface indicates a proportion ≥50%. One widely invasive WDFTC failed to stain with ERβ due to difficulties in the TMA procedure.
FTC, follicular thyroid carcinomas; PDFTC, poorly differentiated FTC; WDFTC, well-differentiated FTC; FTA, follicular thyroid adenomas; ER, estrogen receptor; TMA, tissue microarray.
ERβ expression in thyroid neoplasms
One widely invasive FTC failed to stain with ERβ due to difficulties with the TMA procedure; this diminished the tumor number used in the statistical analysis concerning ERβ to 42. ERβ was expressed abundantly in both adenoma and carcinoma tissues, since 90% of FTC (38/42) and 99% (81/82) of FTA were positive (Table 1 and Fig. 2). ERβ expression was significantly higher in FTA than in FTC (p<0.001), an association that existed between each subgroup of FTA and FTC (Fig. 3). A preferable differential cutoff value level was 10% (p<0.001, rχ=26.923) between FTC and FTA, with a specificity of 90% and sensitivity of 51%. ROC curve analysis with this cutoff value showed that ERβ was a better differential diagnostic marker between FTC and FTA than MIB-1 (AUC=0.757 vs. AUC=0.677) in our material (Fig. 4). A logistic regression equation showed that ERβ expression was more sensitive than MIB-1 (Table 2). We calculated the probability of cancer index with the combination of ERβ and MIB-1 expression levels in the logistic regression model. In using this probability index as a diagnostic test, no significant improvement in accuracy was obtained when compared with either ERβ or MIB-1 alone in an ROC analysis (data not shown). With a cutoff value of 5%, a level conducted from carcinoma-specific mortality as each death of disease case (n=8) had an ERβ expression ≤5%, the specificity of ERβ as a diagnostic marker was 92%, while the sensitivity diminished to 42% (p<0.001, rχ=19.900). No significant difference appeared in ERβ expression between the carcinoma subgroups (WDFTCs, PDFTCs, widely or minimally invasive subgroups).
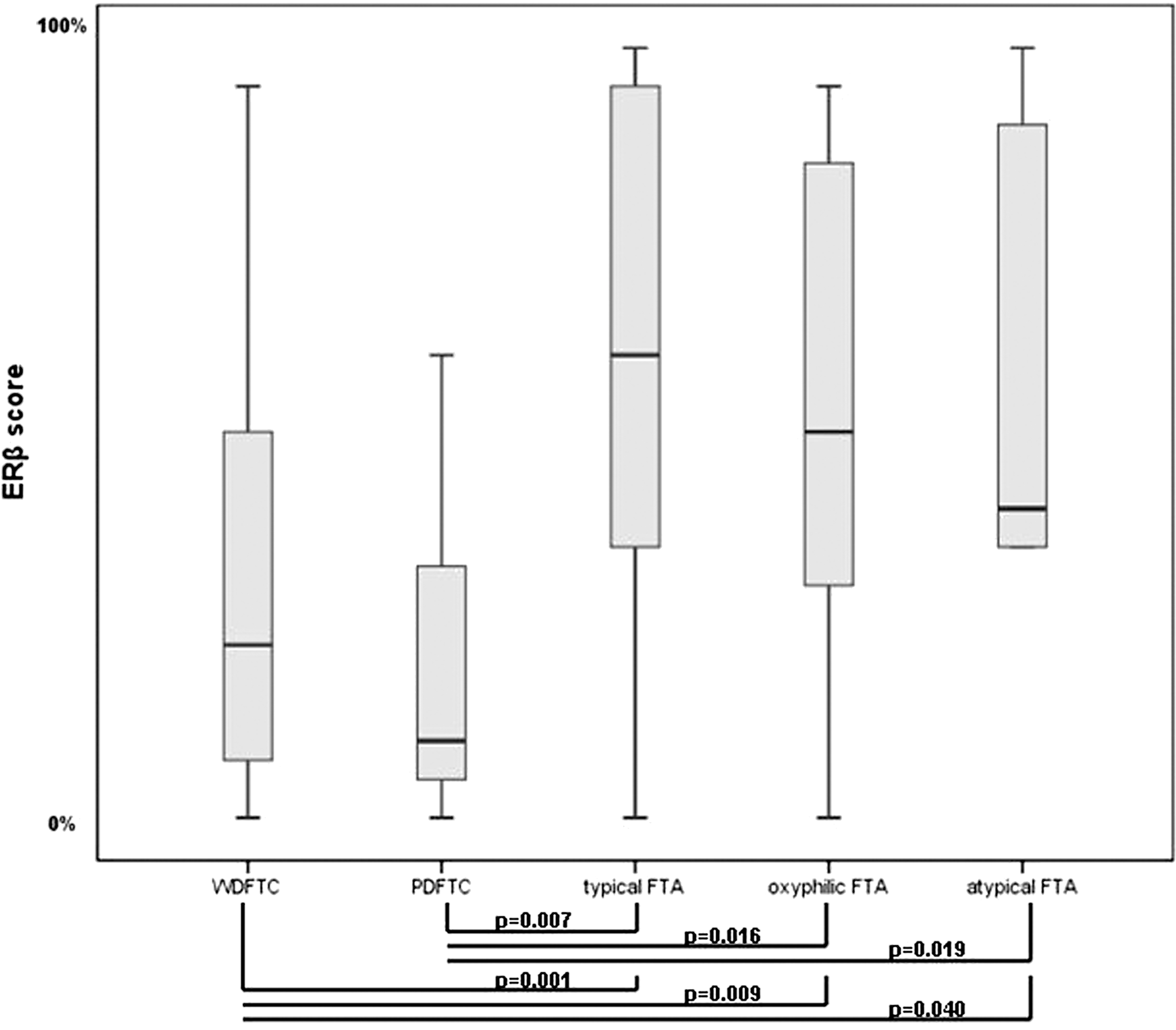
ERβ expression in follicular thyroid neoplasms in a box-plot figure. Whiskers represent extreme values; edges of boxes, the quartiles; and bold line, the median value. p-Values from chi-square or Fisher's exact tests between tumor groups are shown at the lower part of the figure.
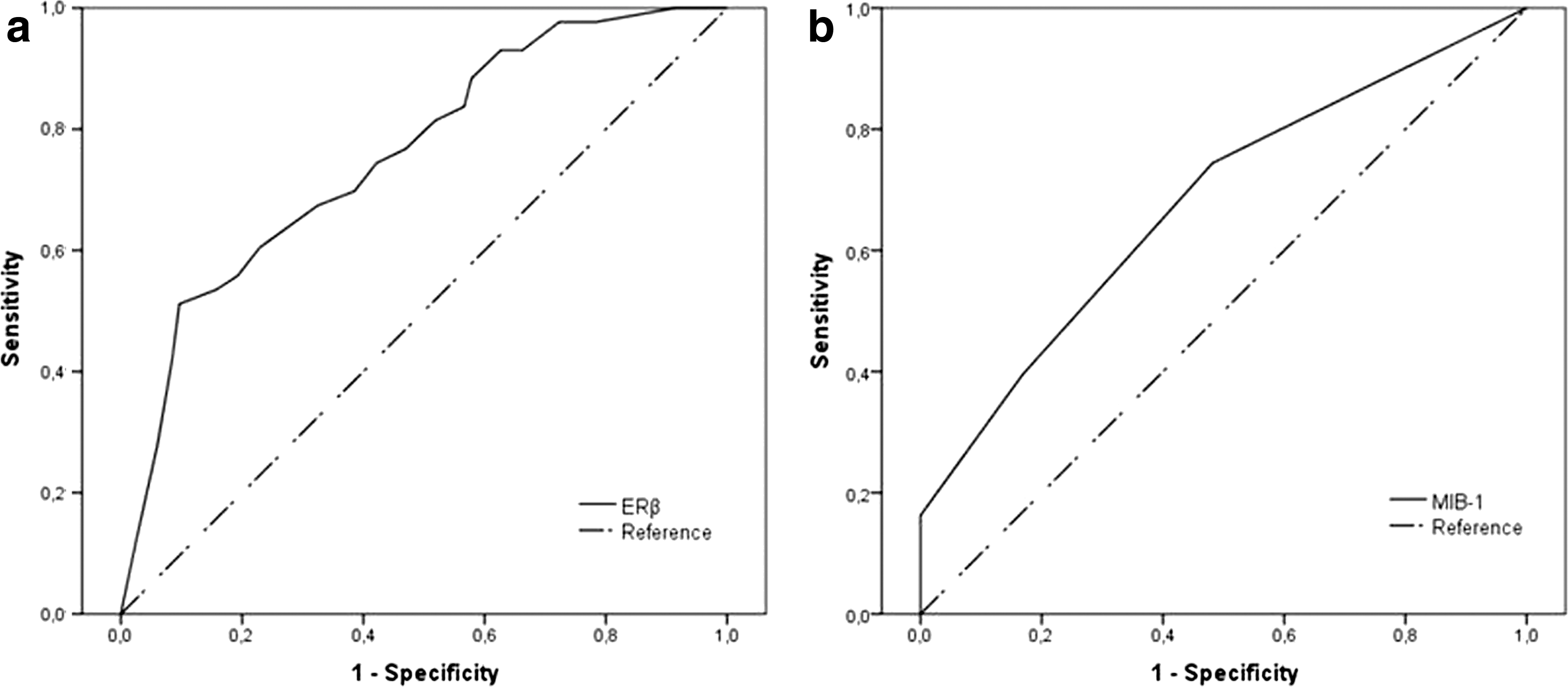
Comparison of the diagnostic value of
Model employed a 5% unit increase in a continuous scale. Categorical scale: [1] 0%–2%, [2] 2%–5%, [3] 5%–10%, [4] >10%) as independent diagnostic variables based on 43 follicular thyroid carcinoma patients and 83 follicular thyroid adenoma patients.
Source: DeLellis and Williams, 2004 (1).
SE, standard error; OR, odds ratio; CI, 95% confidence interval.
ERβ and clinicopathological characteristics of FTC
Low ERβ expression of ≤5% correlated with poor prognosis throughout the whole group of FTC patients (log rank p=0.003). The WDFTC were correlated with outcome as well (p=0.034), and the correlation was even stronger with only the widely invasive type of FTC included (p=0.006), since no cancer-related deaths were seen in the minimally invasive patient group. No progression of disease was seen during the follow-up in the minimally invasive carcinoma group. In widely invasive WDFTC, the correlation was barely achieved (p=0.050). In PDFTC, there was no correlation between ERβ and prognosis (p=0.167), although each death from a disease case had a score of 5% or below (Fig. 5a–e). All patients who died of disease had an advanced stage at the time of diagnosis, T4 tumor in five of eight patients (63%), and stage IV disease in seven of eight patients (88%) (Table 3).

Kaplan–Meier survival curves correlated to ERβ expression with a cutoff value of 5% in
Diff., differentiation; invas, invasiveness; wid, widely invasive; prim, primary; sec, secondary; met, metastasis; RAI, radioactive iodine; treat, treatment; rad, radiation; chemo, chemotherapy; adr, adriamycin; gem, gemcitabin; surg, surgery; metast., metastatis to.
Nine surviving carcinoma patients had scores ≤5%, and all were WDFTC, with two having a minimally invasive and seven a widely invasive histological type. None had primary metastases at the time of diagnosis, while two of nine (22%) exhibited stage IV disease at the time of diagnosis. One patient had a recurrence at the end of follow-up (Table 4).
Min, minimally invasive; free, free of disease; on-going, on-going disease; other, other cause of death.
Twenty-five carcinoma patients alive or having died from unrelated causes had scores of >5%, including 3 PDFTC and 22 WDFTC. Seven of the WDFTC were minimally invasive and 15 widely invasive. In all, 2 out of 25 (8%) exhibited stage IV disease at the time of diagnosis. All three PDFTC patients had a recurrence at the end of follow-up. The remaining cases were WDFTC, 20 of which were without recurrence or metastases. The last two patients died from nonrelated causes.
There was no correlation between ERβ expression and clinicopathological characteristics of FTC, including age at the time of diagnosis, sex, tumor stage, TNM classification, metastasis site, tumor size, or proliferation index (Table 5). Moreover, there was no correlation with neck recurrences, primary or secondary metastases, invasiveness, oxyphilia, necrosis, vascular or capsular invasion, differentiation grade, or serum thyroglobulin level tested before the first RAI treatment. Correlations occurred between ERβ expression (WDFTCs p=0.017 and PDFTCs p=0.029) and death from disease.
One widely invasive WDFTC failed to stain with ERβ due to difficulties in the TMA procedure.
Discussion
Here we report scant ERα and abundant ERβ expression in follicular thyroid neoplasms, including PDFTC. ERβ expression was significantly higher in FTA than in FTC. Loss of ERβ expression was a prognostic factor in FTC, with no correlation with other clinicopathological variables.
The association between ERs and thyroid cancer is a much-discussed topic. Both ERα and ERβ are seen in neoplastic as well as non-neoplastic thyroid tissues. Contradicting results concerning ERα expression in thyroid tissues have been reported. ERα expression in thyroid carcinomas has been found to be higher or lower compared to non-neoplastic thyroid tissue (14 –16). Our study showed only scant ERα expression in follicular thyroid neoplasms, which does not suggest a role of ERα in follicular thyroid carcinogenesis. Egawa et al. (14) showed a higher ERβ expression in follicular carcinoma than in follicular adenoma tissues. This result was not supported by several other studies (15 –17). We, however, detected abundant ERβ expression, especially in adenomas compared with carcinomas.
Our results suggest that ERβ may be a helpful marker in differentiating FTA from FTC, because the ROC curve analysis showed a specificity of 90%, with a cutoff value of 10%. The sensitivity of ERβ, on the other hand, remained at an inadequate level of 51%, and thus ERβ alone is not suitable for the differential diagnosis between FTA and FTC. As such, ERβ expression cannot replace the histological carcinoma criteria of capsular or vascular invasion at the histological examination. Numerous studies on attempts to find a differential marker between FTA and FTC have been published, such as galectin-3, thyroid peroxidase (23), dipeptidyl peptidase 4 (DPP IV) (24), HBME-1, and cytokeratin-19 (25), but only MIB-1 is routinely used in diagnostics classifying carcinomas (26). We previously showed that MIB-1 expression is significantly higher in FTC than in FTA (22). The present study shows an even better differential diagnostic value with ERβ than with MIB-1, according to a logistic regression analysis, although combining these markers resulted in no improvement in diagnostic accuracy. Still, since ERβ identified those fatal carcinomas that had a low MIB-1 index, ERβ may be further exploited for diagnostic purposes. On the other hand, there was no significant difference between carcinoma subgroups, undoubtedly due to the small number of patients in these groups, although the median ERβ value was clearly higher for WDFTC than for PDFTC.
Previously, prognostic immunohistochemical markers for thyroid carcinomas of follicular cell origin have been suggested, such as thyroid peroxidase and galectin-3 (23), cyclooxygenase 2 (27), and p27KIP1 and Ki67/MIB-1 (28). To our knowledge, this is the first report on ERβ as a prognostic marker in FTC. Each patient who died of disease had a tumor with low ERβ expression, and the strongest prognostic significance was observed with a cutoff value of 5%. An interesting observation was that each death case with a low ERβ tumor score presented with advanced disease status at the time of diagnosis. Our results are in line with a recent study by Magri et al. showing a correlation between low ERβ expression and an aggressive feature, vascular invasiveness, in small T1 of the TNM staging system of well-differentiated thyroid carcinomas, including 87 PTC and 4 FTC (29). Thomas and Gustafsson (7) discussed the declining level of both ERα and ERβ expression in several cancers as the disease progressed, postulating the possible role of the ERβ1 isoform in maintaining the cell's differentiated and epithelial phenotype. This possible connection between the declining level of ERβ and disease progression in FTC needs further verification.
Estrogen, essential for various physiological functions, for example, normal mammary gland growth and development, induces cell proliferation and has mitogenic effects on breast, endometrial, and ovarial tissues (30). In thyroid cancer cells, estrogen induces cell proliferation and enhances adhesion, migration, and invasion, mainly through ERα (31 –34). ERβ, on the other hand, is thought to play a protective role in carcinogenesis. Since it has an inhibitory effect against the mitogenic effects of estrogens, it is thought to act as an antiproliferative and apoptosis-promoting receptor, and consequently after downregulating ERβ, a significant increase in cell proliferation is seen (8,16,30,33,34). ERβ is thought to protect against hyperproliferation caused by α-induction (32,35). Therefore, an increase in ERα and a decrease in ERβ may be a critical step in estrogen-dependent tumor differentiation and progression as suggested by our results observed in FTC. In line with this, a significant prognostic association was reported between low ERβ expression and poor survival of patients with breast cancer (9), ovarian cancer (20), and lung cancer (21). Our results showing that loss of ERβ predicted a poor outcome agree with these conclusions. Comparably, a malignant transformation from FTA to FTC is a debated process (36,37) and, referring to the aforementioned tumor progression, a reduction in ERβ expression was seen in our carcinoma material when compared with adenomas.
The clinical outcome of WDFTC patients, especially the widely invasive type, presents a prognostic dilemma. The minimally invasive type is nearly always an indolently acting tumor group, while PDFTC can behave aggressively. In our study, ERβ was a promising tool for the prediction of the clinical behavior of widely invasive WDFTC.
Poorly differentiated thyroid carcinoma is a new diagnostic entity, introduced in 2004 (38). This subtype acts in an intermediate manner between well-differentiated and anaplastic thyroid carcinomas (39). Poor differentiation on histology is a well-known indicator of poor prognosis, with a 5-year survival of 50% (38). Our material included seven PDFTC cases, including four patients who died of disease and exhibited a low ERβ expression and three patients still alive with on-going disease who exhibited a score of over 5%. Still, there was no correlation between survival and ERβ expression in PDFTC, possibly because of the low number of cases.
Our material contained 17 patients with low ERβ scores, 8 of whom died of disease and 9 who were still alive with only 1 having active disease at the end of a follow-up. Bearing in mind the convincing evidence of the prognostic influence of low ERβ in many cancers, the fact that eight patients recovered without recurrences may be due to the thyroid carcinoma's indolent biology, sensitivity to therapy or even disease dormancy (40). Our follow-up period is still limited and further recurrences may emerge in the future. If ERβ were used in clinical practice, it seems questionable whether aggressive treatment of patients could be justified, since nearly half of those with low ERβ scores would recover with less aggressive treatment. On the other hand, some patients with high scores had aggressive disease, thus needing treatment accordingly.
Our study is, to the best of our knowledge, the first report on the association between ERβ tumor expression and prognosis in FTC. The study has limitations, including the TMA procedure used, which is sensitive to biases, since only a small proportion of the tumor area is evaluated in the histological specimen. Additionally, the total number of carcinoma-related deaths is small, as is the number of PDFTC cases; thus, clinical implications based on such low numbers should be further studied and assessed critically. Still, it is important to find a prognostic marker for the identification of those patients whose disease is potentially fatal.
In conclusion, ERβ may have clinical utility in differentiating FTA from FTC and in assessing the prognosis of FTC patients, thus identifying those patients who need more aggressive treatment.
Footnotes
Acknowledgments
We thank Päivi Peltokangas, Tuire Koski, and Eija Heiliö of the University of Helsinki/HUSLAB, and Elina Aspiala of Helsinki University Central Hospital, for excellent technical assistance. We thank the Helsinki University Language Center for text editing. Funding for this study was provided by Sigrid Juselius Foundation, Finska Läkaresällskapet, Medicinska understödsföreningen Liv och Hälsa, and the Finnish Cancer Foundation.
Disclosure Statement
All authors declare that there is no conflict of interest that could be perceived as prejudicing the impartiality of the research reported.