
Abstract
Background:
Recent studies have described an encapsulated and an infiltrative form of follicular variant of papillary thyroid carcinoma (FVPTC). While encapsulated tumors have been reported to have virtually no metastatic potential or recurrence risk if angioinvasion and capsular penetration are absent, infiltrative tumors have been found to have a significant metastatic potential and a risk of recurrence. In our experience, a substantial number of FVPTCs are neither fully encapsulated nor infiltrative, but instead are partially-encapsulated (PE) or well-circumscribed (WC). Thus, the aim of this study was to investigate the metastatic potential and recurrence risk of PE/WC FVPTCs in comparison with that of encapsulated and infiltrative tumors.
Methods:
We studied 77 FVPTCs resected between 2000 and 2002 and characterized the tumors as encapsulated, PE/WC, or infiltrative. Histologic assessment was then correlated with lymph node status and clinical outcome.
Results:
In our cohort, 27 (35%) tumors were encapsulated, 35 (45%) were PE/WC, and 15 (19%) were infiltrative. Lymph node status was similar between PE/WC and encapsulated tumors, but was significantly different between encapsulated and infiltrative groups (p<0.001), and PE/WC and infiltrative groups (p<0.001). Lymph node metastases were absent in all 15 cases of encapsulated tumors and all 9 cases of PE/WC tumors with sampled lymph nodes, but were present in 7 of 9 (78%) cases of infiltrative tumors with sampled lymph nodes. For patients with available clinical follow-up (66 cases, 86%), the median follow-up time was 111 months. No patients with encapsulated tumors recurred, one (3%) patient with a PE/WC tumor had recurrent/residual disease, and two (15%) patients with infiltrative tumors had recurrent/residual disease. The one patient with a PE/WC tumor who had recurrent/residual disease had a tumor bed recurrence 7 years after initial resection. Significantly, this was the only patient in the PE/WC group that had a positive resection margin.
Conclusions:
Our results demonstrate that PE/WC FVPTCs have a very low metastatic potential/recurrence risk, indicating that they should be distinguished from more aggressive infiltrative FVPTCs.
Introduction
Recent studies have described an encapsulated and an infiltrative form of FVPTC (18 –20). In a study comparing the biologic behavior of encapsulated and infiltrative FVPTCs, encapsulated tumors lacking vascular invasion or capsular penetration (i.e., noninvasive encapsulated FVPTCs) were found to have virtually no metastatic potential or recurrence risk (18). In contrast, infiltrative tumors were found to have a significant metastatic potential and a risk of recurrence. Based on the results of these studies, the authors advocated conservative treatment, that is, lobectomy only, for patients with noninvasive encapsulated FVPTC. Moreover, a subsequent study that confirmed the prognostic difference between encapsulated and infiltrative FVPTCs also demonstrated that they have different molecular profiles (19). Overall, FVPTC has been shown to harbor molecular alterations that are more similar to those seen in follicular adenomas/carcinomas than those associated with classical type PTC (21 –25); however, it appears that FVPTC is a molecularly heterogeneous group. Rivera et al. found that BRAF mutations were absent in all encapsulated FVPTCs, but present in 26% of infiltrative tumors. RAS mutations, on the other hand, were identified in 36% of encapsulated FVPTCs, but found in only 10% of infiltrative tumors (19). Thus, the molecular alterations seen in encapsulated FVPTCs appear to be more similar to follicular adenomas/carcinomas, while infiltrative tumors harbor mutations that are more similar to those seen in classical-type PTC.
Histologically, encapsulated FVPTCs possess a fibrous tumor capsule, while infiltrative tumors are characterized by absent or incomplete tumor encapsulation with tongues of tumor infiltrating into non-neoplastic thyroid parenchyma. In our experience, a significant number of FVPTC are neither encapsulated nor infiltrative, but are instead partially-encapsulated (PE)/well-circumscribed (WC). To our knowledge, no study has evaluated the biologic behavior of these tumors. Thus, the aim of this study was to investigate the metastatic potential and recurrence risk of PE/WC FVPTCs in comparison with that of encapsulated and infiltrative tumors. With this aim, we performed a retrospective study histologically evaluating the growth pattern of 77 FVPTCs resected at Brigham and Women's Hospital and correlating the findings with clinical outcome.
Materials and Methods
Pathology and medical record review
A search of the pathology database at Brigham and Women's Hospital was performed for lobectomy and thyroidectomy specimens with PTC measuring >1 cm diagnosed between 2000 and 2002. The slides for each case were reviewed, and FVPTCs were identified. For a tumor to be diagnosed as FVPTC, the tumor was required to have an entirely or almost entirely follicular architecture (i.e., ≤1% papillary architecture) along with cytologic features of PTC. Cases were excluded if the patient had a second thyroid carcinoma measuring >1 cm or had more than two additional microcarcinomas. Cases with an anaplastic or a poorly differentiated component were excluded (with a poorly differentiated component defined according to the criteria described in the Turin proposal) (26). After these inclusion and exclusion criteria had been met, we analyzed a total of 77 cases of FVPTC. Data extracted from original pathology reports included the following: type of specimen (lobectomy, thyroidectomy), size of tumor (cm), presence of extrathyroidal extension, margin status (positive/negative), presence of lymph node metastases, number of lymph nodes involved by tumor, and presence of extranodal extension. All available H&E slides of tumor for each case were reviewed (mean 6, range 1–23) by two pathologists (M.V. and J.A.B.) who were blinded to the clinical outcome.
Each tumor was classified as encapsulated, infiltrative, or PE/WC (Fig. 1). Tumors with a complete fibrous capsule delineating the tumor from the benign thyroid parenchyma were categorized as encapsulated tumors. For a tumor to be considered encapsulated, a fibrous capsule was required to be evident around the entire tumor. If the tumor had a partial capsule, but had areas at the periphery with tumor directly adjacent to benign thyroid parenchyma with no intervening capsule, these tumors were classified as PE/WC (as long as this tumor edge was well-circumscribed). Encapsulated tumors with either lymphovascular invasion (present within the capsule or beyond) or complete capsular penetration were categorized as encapsulated tumors with invasion (with the presence of capsular penetration, lymphovascular invasion, and number of foci of lymphovascular invasion recorded for each case). Infiltrative tumors were defined as tumors either entirely lacking or partially lacking a tumor capsule with tongues of tumor infiltrating into the benign thyroid parenchyma. PE/WC tumors entirely or partially lacked a tumor capsule. However, unlike infiltrative tumors, PE/WC tumors also lacked infiltration of tumor into adjacent thyroid parenchyma. Instead, these tumors had a well-circumscribed edge. Cases with any indication of an infiltrative edge were classified as infiltrative. All cases, regardless of growth pattern, had nuclear features of PTC, as depicted in Figure 1C, F, and I.
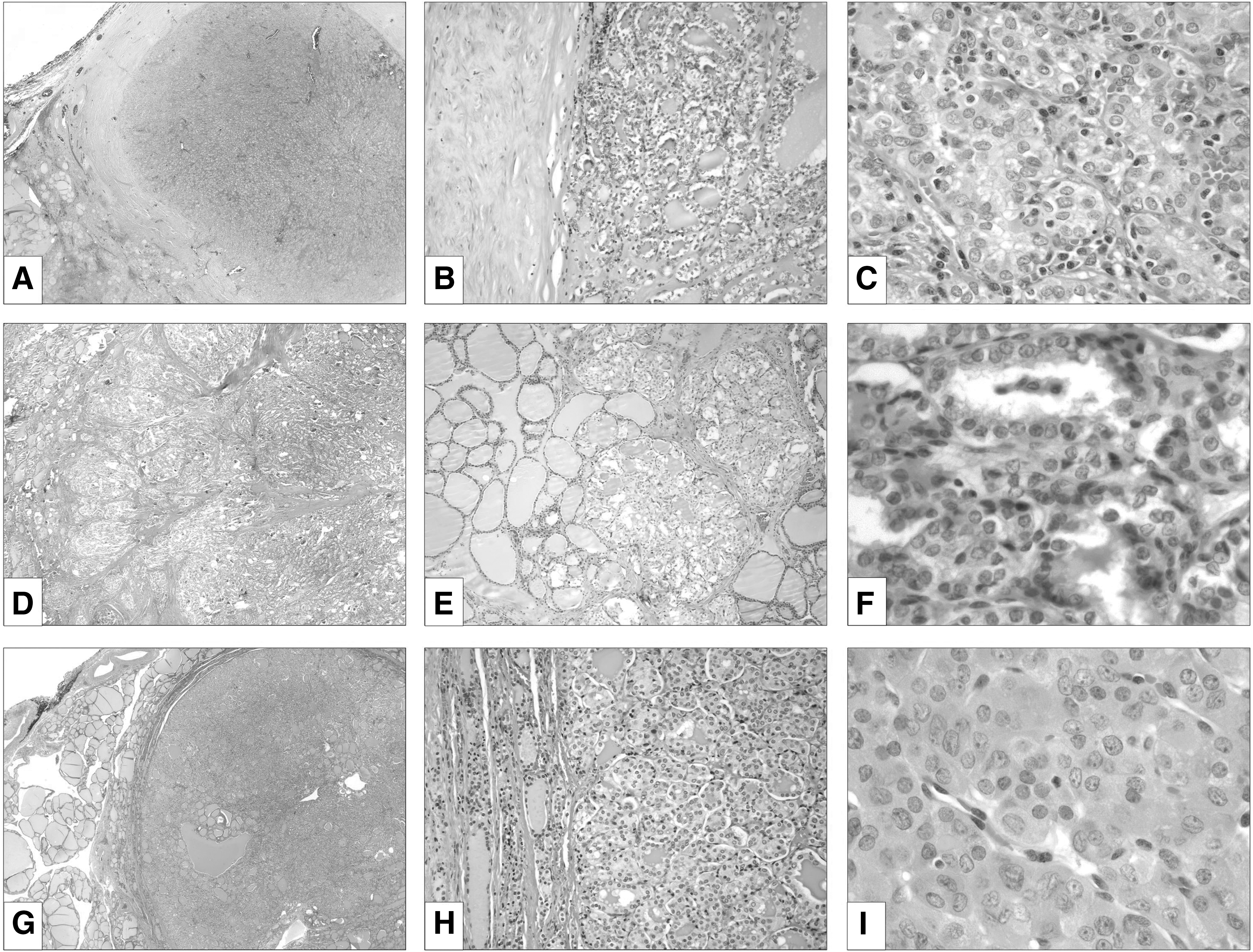
Examples of follicular variant of papillary thyroid carcinoma (FVPTC) according to growth pattern.
Demographic data were extracted from the electronic medical record, and included: age at diagnosis, sex, treatment with RAI, time to recurrence, type of recurrence (tumor bed, lymph node metastasis, and distant metastasis), additional surgery, and total time of clinical follow-up (months).
Statistical analysis
Correlations were examined using ANOVA or Fisher's exact test, as appropriate. p-Values <0.05 were considered significant. Statistical analysis was performed in STATA 11.0 (Stata Corp., College Station, TX).
Results
Clinical characteristics
The clinical characteristics and treatment strategies of the patients included in this study are summarized in Table 1.
There was no significant difference between encapsulated, infiltrative, or PE/WC groups for any clinical characteristic (p>0.05) by ANOVA or Fisher's exact test as appropriate.
Encapsulated tumors with invasion had either complete capsular penetration by tumor and/or lymphovascular invasion.
FVPTC, follicular variant of papillary thyroid carcinoma; PE, partially-encapsulated; WC, well-circumscribed.
Of the 77 patients included in the study, there were 66 (86%) women and 11 (14%) men. The mean age at time of thyroidectomy was 50 years (range 21–89 years). Fifty-six (73%) patients underwent initial total thyroidectomy, 14 (18%) patients underwent an initial lobectomy followed by a completion thyroidectomy, and 7 (9%) underwent only lobectomy. Thirty-two (42%) patients received RAI treatment (including one patient who underwent only a lobectomy). There was no significant difference in patient clinical characteristics or treatment strategies by tumor group.
Histopathologic features
The histopathologic characteristics of the thyroidectomy specimens evaluated in this study are summarized in Table 2 according to the growth pattern of FVPTC.
Encapsulated tumors with invasion had either complete capsular penetration by tumor and/or lymphovascular invasion.
p-Values are comparing encapsulated (total), infiltrative, and PE/WC groups.
In our cohort, 27 (35%) tumors were encapsulated, 15 (19%) were infiltrative, and 35 (45%) were PE/WC. Of the 27 encapsulated tumors, 13 (48%) were classified as invasive due to the presence of capsular penetration, lymphovascular invasion, or both capsular penetration and lymphovascular invasion. Eight showed capsular penetration alone, and 5 cases had lymphovascular invasion (with or without capsular penetration). All five cases with lymphovascular invasion showed <4 foci of invasion. No PE/WC tumors had lymphovascular invasion. The mean tumor size for the entire cohort was 2.4 cm (range 1.0–8.0 cm). The tumor size was not significantly different between tumor groups. For encapsulated tumors, the mean size was 2.9 cm (range 1.0–8.0 cm); for infiltrative tumors, it was 2.1 cm (range 1.0–5.4 cm); and for PE/WC tumor, it was 2.2 cm (range 1.1–6.3 cm). Overall, 8 (10%) tumors were multifocal (with no more than two additional foci of microcarcinoma based on our exclusion criteria). The low rate of multifocality in this study is likely the result of our exclusion criteria. The rates of multifocality were not significantly different between groups. Extrathyroidal extension was present in 5 (6%) cases in our cohort. The number of cases with extrathyroidal extension was similar between encapsulated and PE/WC groups, but the number of infiltrative tumors with extrathyroidal extension was significantly greater than the number of encapsulated and PE/WC tumors with extrathyroidal extension (p<0.01). Extrathyroidal extension was present in association with only 1 (4%) encapsulated tumor that demonstrated capsular invasion, 4 (27%) infiltrative tumors, and no PE/WC tumors. In total, 7 (9%) cases had positive resection margins, including 3 (11%) cases in the encapsulated group, 3 (20%) cases in the infiltrative group, and 1 (3%) case in the PE/WC group. There was no difference in margin status between tumor groups.
Lymph node status and tumor recurrences
Lymph node status and tumor recurrences in the study patients are summarized in Table 3 according to the growth pattern of FVPTC.
Encapsulated tumors with invasion had either complete capsular penetration by tumor and/or lymphovascular invasion.
p-values are comparing encapsulated (total), infiltrative, and PE/WC groups.
Lymph nodes were sampled in 33 patients (15 encapsulated, 9 infiltrative, and 9 PE/WC).
Clinical follow-up was available in 66 (86%) cases (23 encapsulated, 13 infiltrative, and 30 PE/WC).
Thirty-three (43%) patients had lymph nodes taken at the time of the initial surgery. The percentage of cases with sampled lymph nodes was significantly different between groups (p=0.02). Lymph nodes were sampled in 15 (56%) of 27 encapsulated tumors, 9 (60%) of 15 infiltrative tumors, and 9 (26%) of 35 PE/WC tumors.
Lymph node metastases were present in 7 (9%) cases in the entire cohort, and 7 (21%) of 33 cases with sampled lymph nodes. While the rate of lymph node metastases was the same for encapsulated and PE/WC tumors, a statistically significant difference in LN status was present between encapsulated and infiltrative groups (p<0.001) and between PE/WC and infiltrative groups (p<0.001). Lymph node metastases were absent in all 15 cases of encapsulated tumors and all 9 cases of PE/WC tumors with sampled nodes, but were present in 7 of 9 (78%) cases of infiltrative tumors with sampled nodes. The average number of positive lymph nodes in the infiltrative group was 3 (range 1–11), the average size of the largest lymph node metastasis was 0.7 cm (range 0.05–1.8 cm), and 2 (29%) cases with lymph node metastases demonstrated extranodal extension.
For patients with clinical follow-up available (66 cases, 86%), the mean and median follow-up times were 100 and 111 months, respectively, with no significant difference in follow-up time between groups. There was no significant difference in recurrences between the tumor groups. No patients with encapsulated tumors recurred, 1 (3%) patient with a PE/WC tumor, and 2 (15%) patients with infiltrative tumors recurred. The one patient with a PE/WC tumor who had recurrent/residual disease was a 42 year-old woman who underwent a lobectomy (with a subsequent completion thyroidectomy) that showed a 2.0 cm PE/WC FVPTC with no additional foci of tumor in the lobectomy or completion specimen. She did not receive RAI at the time of her initial resection. Seven years after the initial resection, the patient underwent a RAI scan after an ultrasound showed a new cystic lesion (previous ultrasound had shown no residual thyroid tissue). The scan showed a 2–3 cm midline focus of markedly increased RAI activity located within the lower thyroid bed. Based on these findings, the patient received RAI treatment. This PE/WC tumor was histologically indistinguishable from the other tumors in the PE/WC group; however, it was the only tumor in the group that had a positive resection margin. Of the two patients with infiltrative tumors that had recurrent/residual disease, one had a local recurrence 6 months after total thyroidectomy and RAI therapy (this patient had a positive margin on initial thyroidectomy), and the other had a local recurrence and pulmonary metastases 2 months after total thyroidectomy.
Discussion
While FVPTC is an indolent tumor, further risk stratification of patients diagnosed with FVPTC is important both to identify those who might benefit from more aggressive management and to spare others from overtreatment. Recent studies have described an encapsulated form of FVPTC with virtually no metastatic potential or recurrence risk if angioinvasion and capsular penetration are absent (i.e., noninvasive), and an infiltrative form of FVPTC with significant metastatic potential and a risk of recurrence (18 –20). However, a substantial number of cases of FVPTC are neither encapsulated nor infiltrative, but are instead best characterized as partially-encapsulated or well-circumscribed. The behavior of these PE/WC tumors has not been established. Thus, the aim of this study was to investigate the metastatic potential and recurrence risk of PE/WC FVPTCs in comparison with that of encapsulated and infiltrative tumors.
Of the 77 FVPTCs in our study, 27 (35%) tumors were encapsulated, 35 (45%) were PE/WC, and 15 (19%) were infiltrative. The rate of lymph node metastases in our cohort was 9%. This rate of lymph node metastases is similar to that reported in the literature for FVPTC and lower than that for classical-type PTC (18,22,27). The lymph node status was the same between PE/WC and encapsulated tumors, but significantly different between encapsulated and infiltrative groups (p<0.001), and PE/WC and infiltrative groups (p<0.001). Lymph node metastases were absent in all 15 cases of encapsulated tumors and all 9 cases of PE/WC tumors with sampled lymph nodes, but were present in 7 of 9 (78%) cases of infiltrative tumors with sampled lymph nodes. A lack of lymph node metastases in association with noninvasive encapsulated FVPTC and a significant rate of lymph node metastases in association with infiltrative tumors is consistent with results from previous studies (18,20). While it is somewhat surprising that none of the encapsulated FVPTCs with lymphovascular invasion in our cohort (five tumors) had lymph node metastases, the lymphovascular invasion in these cases was focal (<4 foci). In the study by Liu et al., the only encapsulated tumors with lymph node metastases had ≥4 foci of lymphovascular invasion. Nonetheless, it is clear that any tumor with even focal lymphovascular invasion should be considered as having metastatic potential, as distant metastases have been reported in association with encapsulated FVPTC with even focal lymphovascular invasion (28). The finding that lymph node metastases were found in association with six of the infiltrative tumors without recorded lymphovascular invasion suggests that although lymphovascular invasion is present, it is not always evident in the examined histologic sections. It is also important to note that only noninvasive encapsulated PTCs with a follicular growth pattern appear to lack metastatic potential. In a study evaluating encapsulated PTCs, 27% of noninvasive encapsulated PTCs with a classical morphology had associated lymph node metastases (20). Thus, the results of our study corroborate the previously reported findings and indicate that PE/WC tumors have a low metastatic potential. One caveat in the interpretation of our lymph node findings is that the rate of lymph node sampling was significantly different between groups. Approximately the same percentage of patients with encapsulated and infiltrative tumors had sampled lymph nodes (56% and 60%, respectively); however, fewer patients with PE/WC tumors had sampled nodes (29%). The reason for this difference in lymph node sampling is unclear. While it does mean that the results for lymph node status could be subject to bias, the fact that no lymph node recurrences were identified in PE/WC tumors suggests that these tumors did not have associated lymph node metastases which were not sampled.
In our cohort, there were very few patients who had recurrent/residual disease despite having a relatively long clinical follow-up (median follow-up time 111 months). No patients with encapsulated tumors recurred, 1 (3%) patient with a PE/WC tumor had recurrent/residual disease, and 2 (15%) patients with infiltrative tumors had recurrent/residual disease. There was no significant difference in RAI treatment between the groups that would lead to differences in the recurrence rates between groups. The one patient with a PE/WC tumor who had recurrent/residual disease had a tumor bed recurrence 7 years after initial resection. Significantly, this was the only patient in this group that had a positive resection margin. Of the two patients with infiltrative tumors who had recurrent/residual disease, one patient had a local recurrence in the setting of a positive resection margin, while the other patient had a lung metastasis. Again, our results for encapsulated and infiltrative tumors are similar to those reported in the literature, showing virtually no recurrence potential for noninvasive encapsulated FVPTC, and a small, but real recurrence risk for infiltrative FVPTC. Based on the results of the studies by Liu et al. and Rivera et al., the authors advocated conservative treatment, that is, lobectomy only, for patients with noninvasive encapsulated FVPTC. Their recommendation was, in part, based on the fact that approximately half of the patients in their study underwent lobectomy alone. In our study, 7% of patients with encapsulated tumors and 14% with PE/WC tumors underwent lobectomy alone.
When studying FVPTC, it is important to acknowledge that it is a tumor with problems in diagnostic reproducibility. A tumor that some pathologists might consider an encapsulated FVPTC may be interpreted by others as a follicular adenoma due to differences in threshold for what is considered a sufficient amount of nuclear features to render a diagnosis of FVPTC. Even expert thyroid pathologists render divergent diagnoses for these tumors (29). One variable that contributes to divergent diagnoses is whether nuclear features are required to be seen throughout the entire tumor. At our institution, while we require more than focal nuclear changes, we do not require these changes to be overtly present throughout the entire tumor. In many encapsulated and PE/WC tumors, the nuclear changes are more pronounced at the periphery. In contrast, infiltrative tumors tend to have more uniform nuclear features. Observer variation in FVPTC is problematic, as different diagnostic opinions can result in different clinical management. Reporting the growth pattern of FVPTCs may ameliorate this problem. For example, for encapsulated FVPTCs, lobectomy alone could be recommended which is the same management that would be prompted by a diagnosis of follicular adenoma. Thus, evaluating the growth pattern of FVPTCs may diminish the clinical significance of divergent pathologic interpretations.
Based on the results of this study, we would advise reporting FVPTC as encapsulated, PE/WC, and infiltrative, so that encapsulated and PE/WC tumors are distinguished from more aggressive infiltrative FVPTC. The results of this study clearly warrant future studies with larger cohorts to confirm the results. If the results of this study are confirmed, it would seem reasonable to advocate conservative management, that is, lobectomy only, for patients with either noninvasive encapsulated or PE/WC FVPTCs. Finally, it would be interesting to evaluate the molecular alterations of PE/WC FVPTCs. Rivera et al. demonstrated that BRAF mutations were absent in all encapsulated FVPTCs, but present in 26% of infiltrative tumors, while RAS mutations were identified in 36% of encapsulated FVPTCs, but found in only 10% of infiltrative tumors (19). If the molecular profile of PE/WC FVPTC is similar to that of encapsulated tumors, this would provide further evidence that these two groups are biologically similar. A study is currently underway to investigate the molecular alterations found in PE/WC FVPTC.
Footnotes
Acknowledgment
This work was supported by the Eleanor and Miles Shore Fellowship for Scholars in Medicine, Harvard Medical School.
Disclosure Statement
The authors declare that no competing financial interests exist.