
Abstract
Background:
Orbital fibroblast proliferation and hyaluronic acid (HA) release are responsible for some of the clinical features of Graves' ophthalmopathy (GO). Thus, inhibition of these processes may be a possible therapeutic approach to this syndrome. Enalapril, a widely used antihypertensive drug, was found to have some inhibitory actions on fibroblast proliferation in cheloid scars in vivo, based on which we investigated its effects in primary cultures of orbital fibroblasts from GO patients and control subjects.
Methods:
Primary cultures of GO and control fibroblasts were treated with enalapril or with a control compound (lisinopril). Cell proliferation assays, lactate dehydrogenase release assays (as a measure of cell necrosis), apoptosis assays, and measurement of HA in the cell media were performed.
Results:
Enalapril significantly reduced cell proliferation in both GO and control fibroblasts. Because enalapril did not affect cell necrosis and apoptosis, we concluded that its effects on proliferation reflected an inhibition of cell growth and/or a delay in cell cycle. Enalapril significantly reduced HA concentrations in the media from both GO and control fibroblasts.
Conclusions:
Enalapril has antiproliferative and HA suppressing actions in both GO and control fibroblasts. Clinical studies are needed to investigate whether enalapril has any effects in vivo in patients with GO.
Introduction
High doses of glucocorticoids (GC), either alone or in association with orbital irradiation, is the most common therapeutic approach in patients with moderate-severe and active forms of GO (2 –6). In contrast, patients with mild and inactive GO are generally given only local, supportive measures, because these forms of GO are scarcely responsive to GC and because of the risks that high doses of GC carry (7 –9). Nevertheless, patients with mild GO still suffer from the syndrome, because of their symptoms, and also because of the changes in their physical appearance, which influence their quality of life profoundly (2 –5). Thus, efforts in the last few years have been aimed at identifying drugs that may be helpful to patients with mild forms of GO, possibly being devoid of the side effects that GC carry. On the clinical side, in a recent study, selenium was found to be relatively effective (10). On the laboratory side, quercetin was found to reduce proliferation and HA release in cultured orbital fibroblasts from GO patients, but also from subjects without GO (11).
Here we investigated the effects of the angiotensin-converting enzyme (ACE) inhibitor enalapril in primary cultures of orbital fibroblasts. Our study is based on the previous observations of a possible healing effect of enalapril in cheloid scars, in subjects who were given the drug for high blood pressure (12), and also of an inhibitory effect of enalapril on the transforming growth factor (TGF)-β (13), a cytokine involved in HA synthesis in fibroblasts (14).
Materials and Methods
Primary cultures of fibroblasts
Orbital adipose tissue samples were collected from five GO patients who underwent orbital decompression. Normal orbital tissue samples were collected from five patients who underwent eye surgery for unrelated reasons. Informed consent was obtained from all patients according to institutional guidelines.
To prepare primary cultures of fibroblasts, tissue samples were minced, dispersed in Medium 199 (Sigma, St. Louis, MO) containing 20% fetal bovine serum (Invitrogen Corporation, Carlsbad, CA), penicillin (Sigma), and gentamycin (Sigma). Cells were kept in cell culture dishes in cell incubators at 37°C for 2 weeks. Then, cells were expanded up to 12–15 passages and kept in Medium 199 containing 10% fetal bovine serum and antibiotics until use.
Preparation of cell extracts
Cells were washed with PBS and incubated on ice for one hour in lysis buffer (1% Triton X-100, 1% deoxycholate in H2O). Samples were spun for 10 minutes at 10,000 g, pellets were discarded, and supernatants were collected. Protein concentrations were measured with the Bradford method.
Cell proliferation assays
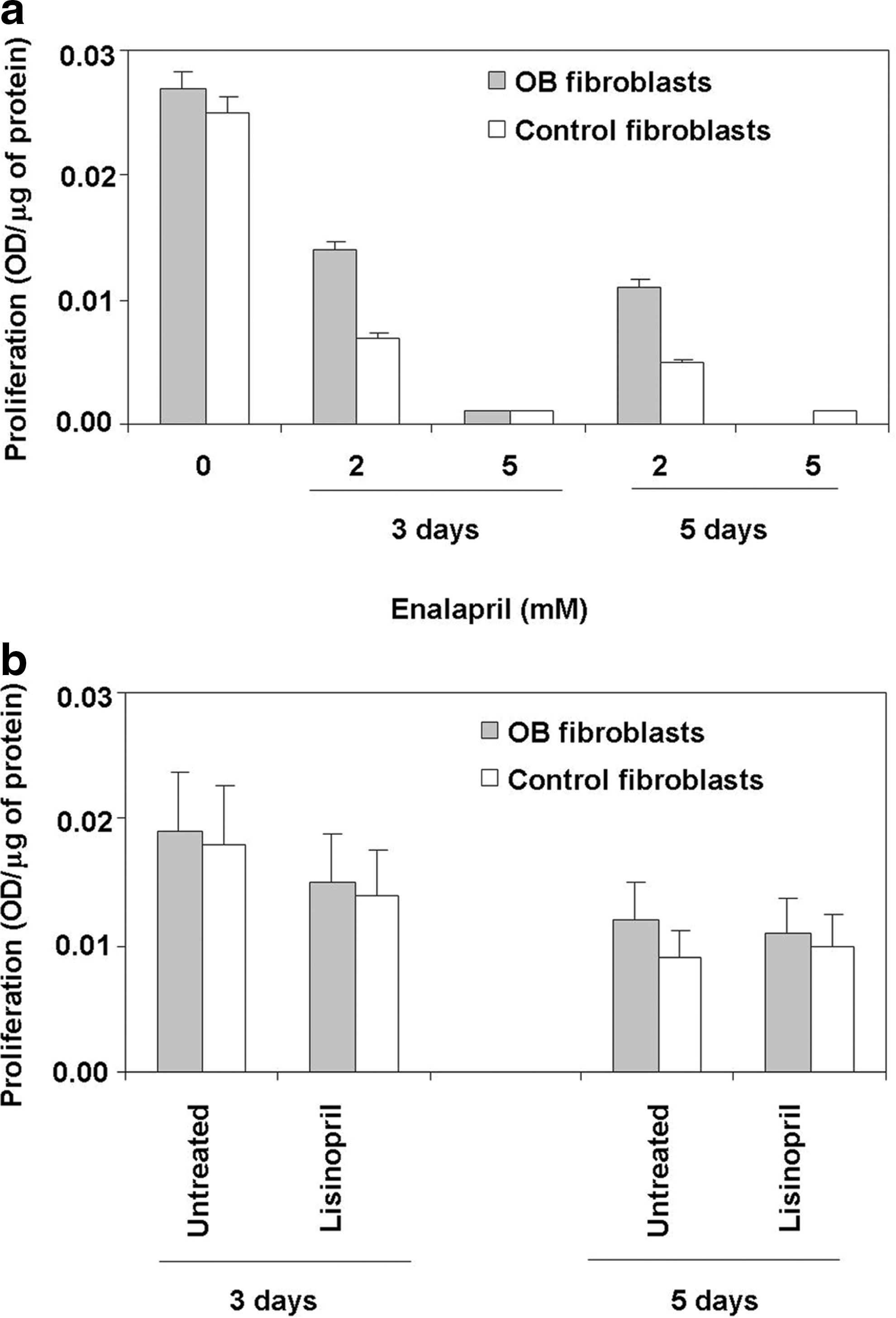
Cell proliferation was measured using a commercial colorimetric immunoassay (Roche Diagnostic GmbH, Penzberg, Germany), according to the manufacturer's instructions. This assay is based on the determination of BrdU incorporation during DNA synthesis. The assay was performed in cells treated for 3 or 5 days in a medium without compounds, or in a medium containing either one of the following compounds: (i) enalapril (Sigma) 2 or 5 mM, and (ii) lisinopril (Sigma) 5 mM.
Lactate dehydrogenase release assays
Cell toxicity (necrosis) was determined using a commercial kit (Promega Corporation, Madison, WI), according to the manufacturer's instructions. The assay is based on a colorimetric, quantitative measurement of lactate dehydrogenase (LDH), a stable cytosolic enzyme released upon cell lysis. Cells were treated for 3 or 5 days with enalapril 2–5 mM, or lisinopril 5 mM for 5 days, or were untreated for the same period of time.
Apoptosis assays
Apoptosis was tested using a commercial method (Biocolor Ltd., Newtownabbey, Northern Ireland), according to the manufacturer's instructions. The assay is based on a dye selectively taken up by cells undergoing apoptosis. Cells were treated for 5 days with enalapril or lisinopril 5 mM, or were untreated for the same period of time.
HA production assays
HA was measured in cell media using a commercial, colorimetric ELISA (Echelon Sciences, Salt Lake City, UT), according to the manufacturer's instructions. Cells were treated for 5 days with enalapril or lisinopril 5 mM, or were untreated for the same period of time.
Data presentation and statistics
Data are presented as median±interquartile range obtained in three experiments. The cumulative difference at various time intervals and/or at various enalapril concentrations was analyzed by the Friedmann test. p-values were not adjusted for multiple testing.
To overcome possible differences in cell numbers between wells, results from all experiments were normalized for the amount of proteins in cell extracts. In this regard, the amount of proteins per well was not affected by both enalapril and lisinopril. Thus, the protein content per well was 30.8±4.9 μg in untreated fibroblasts, 31.5±3.3 μg in fibroblasts treated with enalapril 5 mM for 5 days, and 27.9±4.3 μg in fibroblasts treated with lisinopril 5 mM for 5 days, with no statistical differences. These findings were confirmed even when the analysis was restricted to GO or control fibroblasts and in experiments performed at lower concentrations of enalapril or lisinopril or for a shorter period of time (3 days).
Results
Enalapril inhibits orbital fibroblasts proliferation
Fibroblasts were treated with enalapril 2 or 5 mM, for 3 or 5 days. The concentrations of enalapril were well below the cytotoxic dose, which was found to be >5 mM on cell viability counts at 72 hours (not shown). Proliferation of orbital fibroblasts was reduced in both GO and control fibroblasts, both at 3 and 5 days (Fig. 1a). The decrease in proliferation was statistically significant in both groups (p=0.0008 in GO fibroblasts and p=0.0010 in control fibroblasts). The effect of enalapril was specific, as lisinopril, another ACE-inhibitor, had negligible effects (Fig. 1b).
Enalapril does not affect cell toxicity in orbital fibroblasts
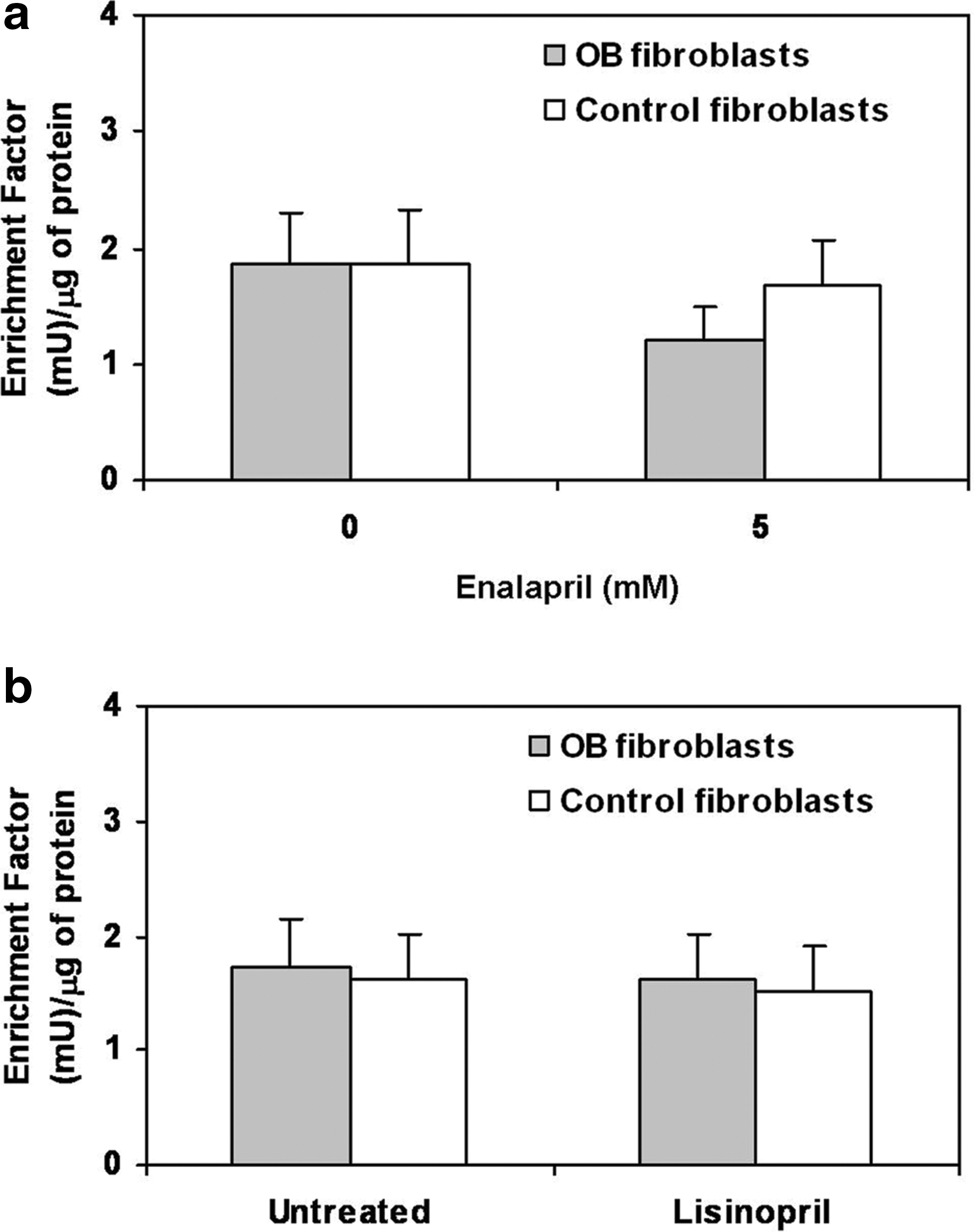
To understand the mechanisms responsible for inhibition of cell proliferation, we determined LDH release from cells, as a measure of cell toxicity (necrosis) (15). Fibroblasts were treated for 3 or 5 days with 5 mM enalapril. As shown in Figure 2a, enalapril did not cause any significant increase in cell toxicity in either of the fibroblast groups, and also lisinopril had no effect (Fig. 2b).

Enalapril does not induce apoptosis in orbital fibroblasts
We then investigated whether enalapril has any effects on apoptosis. As shown in Figure 3a and b, neither enalapril nor lisinopril affected apoptosis in both GO and control fibroblasts.
Apoptosis measurement after treatment with enalapril
Enalapril reduces HA release
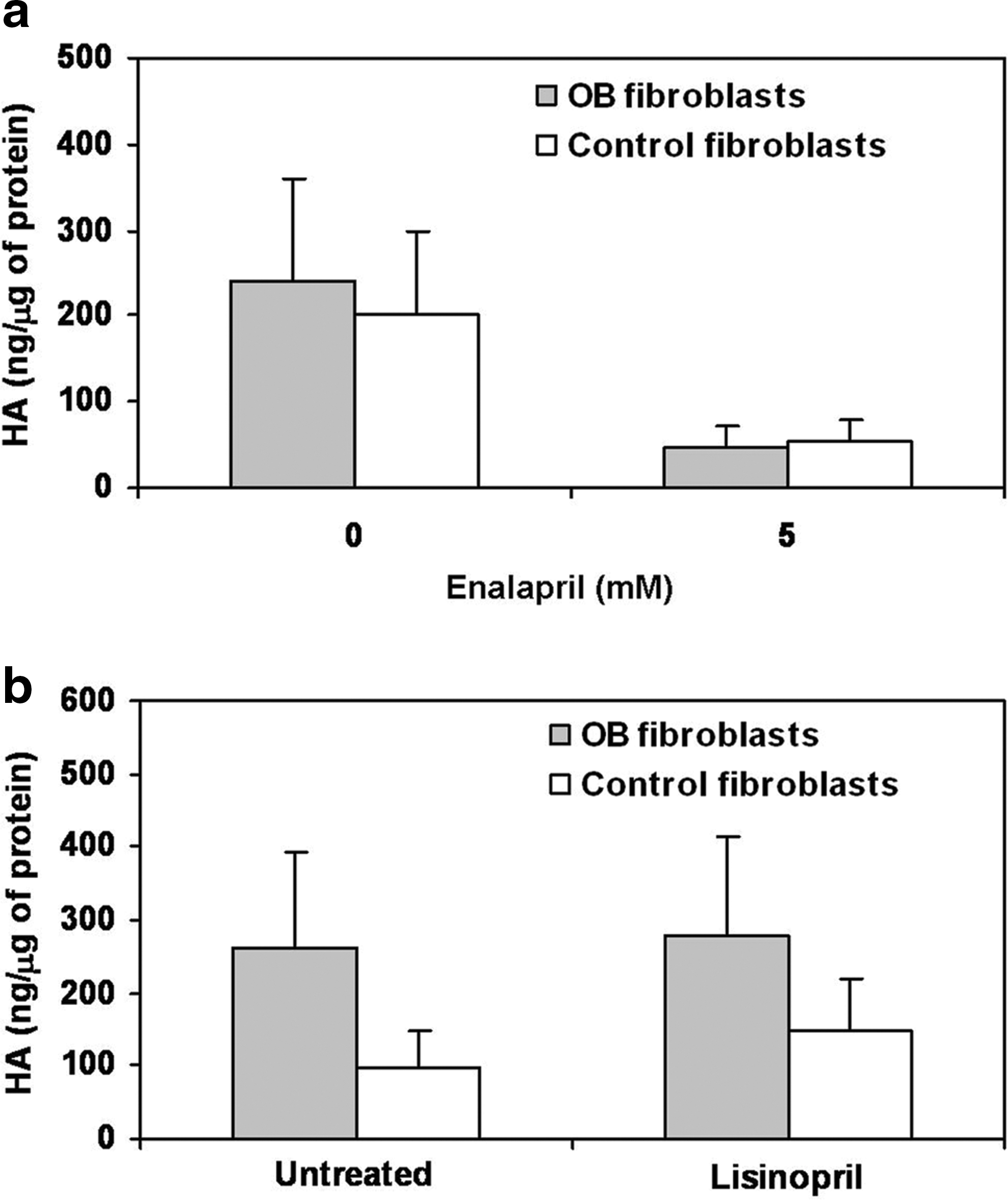
To evaluate the effects of enalapril on HA release, we measured HA in the cell media following treatment of orbital fibroblasts with 5 mM enalapril for 5 days. As shown in Figure 4a, HA concentrations were reduced upon enalapril treatment in both groups, in a statistically significant manner (p=0.0431 in both GO and control fibroblasts). Lisinopril treatment had negligible effects (Fig. 4b).
Discussion
In the present study, we provide evidence for an inhibitory effect of enalapril on orbital fibroblast proliferation and HA production. The possibility of an inhibitory effect was considered because of previous studies suggesting that enalapril may have some inhibitory actions on fibroblast growth and HA synthesis (12 –14). Enalapril belongs to the family of ACE-inhibitor drugs and is commonly used in patients with high blood pressure (16). In addition to their effects on blood pressure, ACE-inhibitors are known to reduce the left ventricular collagen content and attenuate collagen remodeling in the postinfarctual period (16). Furthermore, they have been shown to exert a pulmonary antifibrotic effect (16). These apparent inhibitory effects on the extracellular matrix may involve an action of ACE-inhibitors on GAG production by fibroblasts. Thus, enalapril has been shown to have an inhibitory action on TGF-β, a cytokine involved in HA synthesis (13,14). Finally, recently Iannello et al. reported two cases of patients given enalapril for high blood pressure, in whom they observed healing of cheloid scars, suggesting a possible inhibitory effect of enalapril in fibroblast proliferation (12).
In the present study, we investigated the effects of enalapril in primary cultures of orbital fibroblasts taken from patients with GO or from control subjects; namely, patients who had undergone orbital surgery for reasons unrelated to GO. Enalapril markedly reduced cell proliferation in both cell groups, but it did not influence cell toxicity or apoptosis. Therefore, we concluded that its effects on proliferation reflect an inhibition of cell growth and/or a delay in cell cycle. Nevertheless, further studies are required to investigate, in detail, the molecular and cellular mechanisms involved in the action of enalapril in orbital fibroblasts. In addition to its effects on cell proliferation, enalapril markedly reduced HA release by orbital fibroblast, which, as discussed below, is quite relevant in view of the role of HA in GO (1).
As mentioned above, orbital fibroblast proliferation and increased GAG secretion are among the major mechanisms responsible for the pathological changes of orbital tissues in GO (1). Inhibition of these processes may be a reasonable therapeutic approach to GO, especially in the early stage of the syndrome, when these processes occur mostly (1 –6). Our findings raise the possibility that enalapril may be tested in patients with GO. The fact that its actions in vitro were exerted in both GO and control fibroblast should not be a limitation for a possible clinical use of enalapril, considering that, in any case, enalapril is largely employed in the clinical practice for high blood pressure, and if it had an effect on fibroblast proliferation in subjects without GO, this would be clinically irrelevant, as it has never been reported among the side effects of this drug (16). On the other hand, orbital fibroblast proliferation and HA production are known to be much greater in GO patients than in patients without GO, because of which enalapril may have a detectable effect in GO, as it seems to do in cheloid scars (12). Further studies are needed to investigate this issue.
Footnotes
Acknowledgment
This study was supported by a Grant from MIUR (Ministero dell'Istruzione, dell'Università e della Ricerca Scientifica) (2004068078 to MM).
Disclosure Statement
All authors declare that they do not have any commercial association that might create a conflict of interest in connection with this manuscript.