
Abstract
Background:
Graves' orbitopathy (GO) is thought to be related to one or more autoantigens present in the thyroid and in orbital tissues. Although this may not imply a quantitative relation between thyroid antigens and degree of GO, which in turn is a risk factor for a more pronounced GO, we postulated that the severity of GO may parallel the amount of thyroid tissue, namely, the size of the thyroid gland. This hypothesis is also based on the observation that patients with Graves' disease presenting with large goiters tend to have more severe hyperthyroidism. Thus, we evaluated retrospectively whether there is a correlation between the degree of GO at its first observation and, among other parameters, the thyroid volume.
Methods:
Eighty-six consecutive patients with untreated GO lasting for no longer than 24 months underwent an endocrinological and an ophthalmological evaluation, the latter including: exophthalmometry, eyelid width, clinical activity score (CAS), diplopia, and visual acuity. The overall degree of GO was ranked using the NOSPECS score as well as a modification of the NOSPECS score. The following parameters were considered for correlations: time since GO appearance, time since detection of hyperthyroidism, FT3, anti-thyrotropin receptor antibodies, thyroid volume, and cigarette-years.
Results:
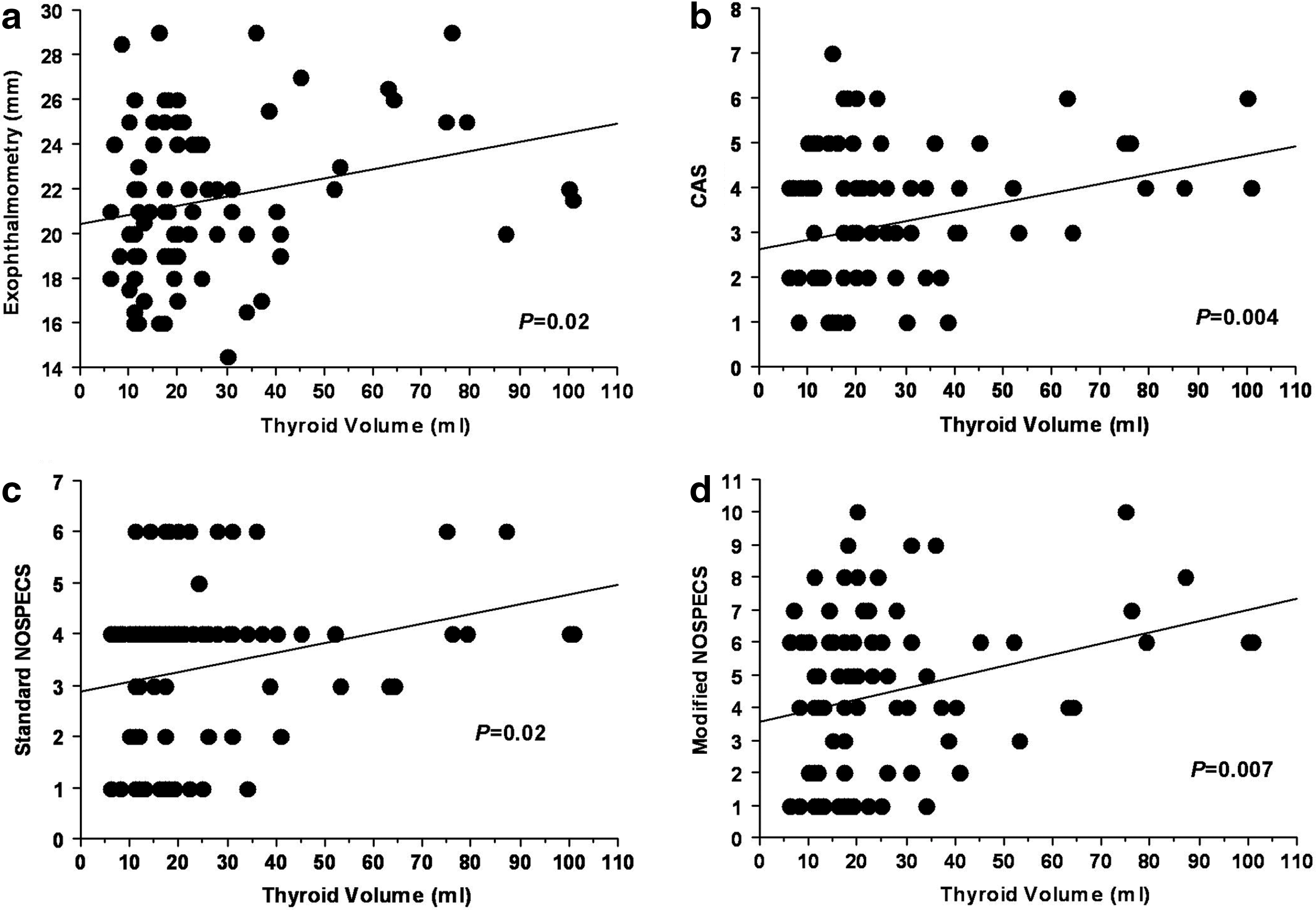
Thyroid volume, but not the other parameters, correlated significantly by simple regression with exophthalmometry (p=0.02) and CAS (p=0.02). The standard NOSPECS score correlated with FT3 (p=0.05), thyroid volume (p=0.02), and cigarette-years (p=0.03), by simple, but not by multiple regression analysis. The modified NOSPECS score correlated with thyroid volume (p=0.007) and cigarette-years (p=0.04) by simple regression, and with thyroid volume also by multiple regression analysis (p=0.05).
Conclusions:
Thyroid volume correlates with the severity of GO at its first observation, especially with exophthalmometry and CAS. The finding is in line with a possible pathogenetic role of antigens shared by the thyroid and orbital tissues. Nevertheless, other mechanisms may explain this observation, including an overall more reactive immune system in patients with a large goiter, resulting in more severe thyroid and eye disease, regardless of the nature of the autoantigen, or whether it is shared by the thyroid and the orbit.
Introduction
The possibility that GO is actually related to one or more autoantigens present in the thyroid gland and in orbital tissues does not necessarily imply a quantitative relation between thyroid antigens and the degree of GO. However, also based on the knowledge that Graves' patients with a large goiter tend to have more severe hyperthyroidism, and that the latter is a risk factor for a more pronounced GO (10,11), we postulated that the severity of GO may parallel the volume of the thyroid tissue. Thus, here we evaluated retrospectively whether there is a correlation between the degree of GO at its first observation and, among other parameters, the thyroid volume measured by ultrasound.
Patients and Methods
Patients
We evaluated retrospectively 86 consecutive GO patients (31 males, 55 females; age 48.0±13.6 years, range 17–91 years) who came to our observation between 2008 and 2011. Inclusion criteria were (i) appearance of GO signs or symptoms for no longer than 24 months; (ii) no previous treatment for GO with the exception of local measures (eye lubricants); (iii) no treatment for Graves' hyperthyroidism except for anti-thyroid drugs.
GO evaluation
All patients underwent a GO assessment, which included: (i) exophthalmometry, performed using an Inami exophthalmometer; (ii) measurement of eyelid width; (iii) evaluation of the clinical activity score (CAS) according to Mourits (12); (iv) assessment of ocular motility and diplopia; (v) assessment of the corneal status; (vi) examination of the fundus oculi; (vii) measurement of visual acuity. All measurements were performed according to the recommendations of the European Group on Graves' Orbitopathy (EUGOGO) (13). The ophthalmologist was always blinded to the patient treatment and clinical features unrelated to the eyes, and because this was a retrospective study, the ophthalmologist could not be biased.
Serum assays and clinical evaluation
Serum FT3 (Lysophase; Abbott Labs, Abbott Park, IL), thyrotropin (TSH; Delfia Wallac, Gaithersburg, MD), and anti-TSH receptor antibodies (TRAb; Brahms, Berlin, Germany) were measured in all patients. Thyroid ultrasound was performed in all patients by the same examinator, who, because this was a retrospective study, could not be biased. Thyroid volume was calculated using the ellipsoid formula, as reported previously (14).
End-points
The primary end-point of the study was the evaluation of possible correlations between the GO features (exophthalmometry, eyelid width, CAS, diplopia, and visual acuity) and the following variables: (i) thyroid volume; (ii) time from the first appearance of eye symptoms; iii) time from the diagnosis of Graves' hyperthyroidism; (iv) serum FT3; (v) serum TRAb; (vi) smoking habits.
The secondary end-point was the evaluation of possible correlations between the overall degree of GO and the variables reported above. The overall degree of GO was ranked using the NOSPECS score (15 –17), as well as a modification of the same score. The NOSPECS score includes six classes of GO severity. As reported in Table 1, we assigned 1–6 points to each class. Thus, patients in class I were given one point, patients in class II were given two points, and so on. In the modified NOSPECS score, because classes II–VI include two or more subclasses, we added one additional point if a given patient had the highest degree of his/her class of assignment. Furthermore, we added one additional point for each of the classes below his/her class of assignment for which the criteria were fulfilled.
One additional point was added if the patient had the highest degree in his/her class of assignment. One additional point was added to patient scores for each of the class/classes below their class of assignment, when the inclusion criteria were fulfilled.
CAS, clinical activity score.
Data presentation and statistical analyses
Descriptive data are presented as mean±SD or median (IQR), when appropriate. When appropriate, the following tests were performed: (i) simple regression analysis; (ii) multiple regression analysis (only within parameters that were significant by simple regression analysis). p-Values ≤0.05 were considered significant.
Results
Overall features of patients
At the time of our observation, 57 patients were euthyroid under anti-thyroid drugs (54 methimazole and 3 propylthiouracil), 4 were untreated and hyperthyroid, 27 were hyperthyroid in spite of anti-thyroid drugs (26 methimazole and 1 propylthiouracil, either taken at insufficient dosage or started since a too short period of time), and 2 were hypothyroid due to methimazole over dosage. Details on thyroid, GO features, and smoking habits are reported in Table 2.
FT3, serum-free T3; TRAb, serum anti-TSH receptor antibodies; IQR, interquartile range; GO, Graves' orbitopathy.
Variables correlated with the individual GO features
As shown in Table 3 and in Figure 1a, exophthalmometry correlated significantly with thyroid volume. In contrast, none of the other variables correlated with exophthalmometry. Eyelid width did not correlate with any of the variables under examination, whereas CAS correlated significantly with thyroid volume (Table 3, Fig. 1b), but not with the other variables. Neither diplopia nor visual acuity showed any correlation with the variables under examination (Table 3).
Correlation between thyroid volume and
Exophthalmometry, eyelid width, and visual acuity refer to the most affected eye. Significant p-values are presented in boldface.
Because GO is known to be affected by hyperthyroidism (10,11), we investigated whether there was a correlation between thyroid volume and GO only in patients who had been presumably euthyroid for at least 3 months. Within the 57 patients who were euthyroid at our observation, hyperthyroidism had been diagnosed and treated since more than 3 months in 52 of them. Presumably, the vast majority of these 52 patients had been euthyroid over the last 3 months. Thus, the thyroid hormone and TSH assays performed over the 3 months preceding our observation were normal in 43 patients, and in the remaining 9 patients who did not have a recent thyroid hormone and TSH assays, the anti-thyroid drug dosage had not been changed over the last 3 months. Limited to these 52 euthyroid patients, exophthalmometry correlated significantly with thyroid volume (p=0.03), whereas CAS did not (p=0.07). However, eyelid width, which, as reported above, did not correlate with thyroid volume when all patients were considered, showed a significant correlation with thyroid volume (p=0.03). Diplopia and visual acuity did not show any significant correlation with thyroid volume.
Variables correlated with the overall GO degree
To assess the overall degree of GO, we used the NOSPECS score (15 –17), as well as a modification of the NOSPECS score, as reported in Table 1. The standard NOSPECS scores correlated significantly with FT3 and cigarette-years (Table 4), as well as with thyroid volume (Table 4, Fig. 1c), by simple, but not by multiple regression analysis. Interestingly, the correlation with FT3 was inverse (not shown). The modified NOSPECS score correlated significantly with cigarette-years (Table 4) and thyroid volume (Table 4, Fig. 1d) by simple regression analysis, but by multiple regression analysis, the correlation remained only for thyroid volume (Table 4). The correlation between the standard and the modified NOSPECS score with thyroid volume was confirmed when the analysis was restricted to the 52 patients who had been presumably euthyroid over the 3 months preceding our observation (standard NOSPECS p=0.03; modified NOSPECS p=0.006).
Significant p-values are presented in boldface.
Discussion
In the present study, we show a significant correlation between thyroid volume and severity of GO at its first observation. As reported above, thyroid volume was found to correlate significantly with exophthalmometry and CAS. In addition, thyroid volume correlated significantly with the NOSPECS score by simple regression analysis, and with a modification of the NOSPECS score both by simple and multiple regression analysis. Along with the European Group on the Graves' Orbitopathy severity scale and with the VISA classification, the Werner's NOSPECS is used to determine the overall degree of GO (12,13,15 –17). Obviously, the score carries several limitations, because of which it has been largely criticized and, in part, dismissed (13,15). Nevertheless, we decided to use the NOSPECS score to confirm the findings we obtained using the individual GO features. To overcome one of the limitations of the NOSPECS score, namely, the fact that patients assigned to a given class are ranked in the same manner regardless of whether they fulfill the features also for the classes below their class of assignment, we developed arbitrarily a modification of the NOSPECS score. Because of the limitations of the NOSPECS score and because the modified NOSPECS score remains to be validated, our conclusions can be at the moment based mostly on the correlations of thyroid volume with exophthalmometry and CAS, whereas the correlation with both the standard and the modified NOSPECS score can be considered only as a mean to somehow confirm those findings.
A possible limitation of our findings is that the patients were heterogeneous in terms of thyroid function, which, especially hyperthyroidism, is known to affect the degree of GO (10,11). To overcome this limitation, we restricted our analysis to patients who had been presumably euthyroid in the 3 months preceding our observation and found that thyroid volume still correlated with exophthalmometry as well as with the standard and the modified NOSPECS score. In addition, thyroid volume correlated with eyelid width. With all due limitations related to the uncertainty that all of these patients were actually euthyroid over the last 3 months (see Results), our findings seem to confirm a correlation between thyroid volume and GO regardless of thyroid function.
A second possible limitation of our study is that the vast majority of patients underwent thyroid ultrasound under anti-thyroid medications, which can affect the size of the thyroid gland (18). Thus, our findings require confirmation in GO patients with untreated Graves' hyperthyroidism, for which further studies are needed.
As reported above, the extent of the correlation between thyroid volume and GO, either considering the individual GO features or the overall GO degree, was relatively variable. Nevertheless, all findings seem to point to the fact that this correlation is real, including the analysis restricted to euthyroid patients. We considered the possibility that the correlation between thyroid volume and the degree of GO reflected a mere anatomical variable. Thus, we investigated whether there was a correlation between patient height and thyroid volume, or between height and either the individual GO features or the standard and modified NOSPECS score. However, we could not find any significant correlation (not shown), which presumably excludes this possibility.
The only other parameter that correlated significantly with the standard and the modified NOSPECS scores in addition to thyroid volume was smoking, namely cigarette-years, which is in keeping with the knowledge that smoking is associated with an increased frequency of GO in Graves' patients, with a more severe degree of GO, and with a worse outcome of GO following treatments (1,19 –22). Interestingly, there was an inverse correlation between the standard NOSPECS score and serum FT3, which, however, was not confirmed when we used the modified NOSPECS score. Nevertheless, this finding is in keeping with the knowledge that hypothyroidism can be associated or it may determine a progression of GO (1,19 –22).
No correlation was observed between the individual GO features or the degree of GO and the time since GO first appearance or since the first detection of hyperthyroidism. To our surprise, no correlation was found between GO features or degree and serum TRAb. Thus, TRAb levels were previously reported to be correlated with the severity and activity of GO (23), and the TSH receptor is generally considered as the main autoantigen of GO (1,2). The most likely explanation for this apparent discrepancy is that the majority of patients were under anti-thyroid drugs. Thus, correction of hyperthyroidism with anti-thyroid drugs is known to be associated with a reduction of TRAb levels (24). On the other hand, although the TSH receptor is the most plausible candidate autoantigen at this point, other autoantigens may be involved (1,2), which may eventually contribute the lack of correlation between TRAb levels and degree of GO in our patients.
Despite all these limitations, the finding of a correlation between thyroid volume and severity of GO is in line with the hypothesis that the pathogenesis of GO could be related to autoimmunity against autoantigens common to the thyroid gland and orbital tissues (1 –3). Nevertheless, other mechanisms may explain our observations. First, the presence of more severe forms of GO in patients with a large goiter may simply reflect an overall more reactive immune system, regardless of the nature of the autoantigen or whether the autoantigen is actually present in both the thyroid gland and in orbital tissues. Second, patients with a large goiter tend to have a more severe degree of hyperthyroidism and there is a certain tendency toward more severe GO in patients with uncontrolled hyperthyroidism (10,11). Thus, the more severe GO observed in patients with a large goiter may simply be due to the more severe hyperthyroidism. Further studies are needed to investigate and clarify the mechanisms underlying our observations. In any case, whatever the mechanisms responsible for the correlation between GO and thyroid volume are, it has to be kept in mind that severe GO can still occur in patients with a small goiter or with a normal thyroid, and also, although rarely, in patients who underwent thyroidectomy (21). Thus, thyroid ultrasound should not be necessarily performed as a mean to predict GO severity in all patients, although it can still be useful, especially for planning thyroid treatment.
Footnotes
Acknowledgment
This research was supported by a grant from MIUR (Ministero dell'Istruzione, dell'Università e della Ricerca Scientifica; 2004068078 to M.M.).
Disclosure Statement
All authors declare that they do not have any commercial association which might create a conflict of interest in connection with this manuscript.