
Abstract
Background:
There is variation in the use of radioactive iodine (RAI) as treatment for well-differentiated thyroid cancer. The factors involved in physician decision-making for RAI remain unknown.
Methods:
We surveyed physicians involved in postsurgical management of patients with thyroid cancer from 251 hospitals. Respondents were asked to rate the factors important in influencing whether a thyroid cancer patient receives RAI. Multivariable analyses controlling for physician age, gender, specialty, case volume, and whether they personally administer RAI, were performed to determine correlates of importance placed on patients' and physicians' worry about death from cancer and differences between low– versus higher–case-volume physicians.
Results:
The survey response rate was 63% (534/853). Extent of disease, adequacy of surgical resection, patients' willingness to receive RAI, and patients' age were the factors physicians were most likely to report as quite or very important in influencing recommendations for RAI to patients with thyroid cancer. Interestingly, both physicians' and patients' worry about death from thyroid cancer were also important in determining RAI use. Physicians with less thyroid cancer cases per year were more likely than higher-volume physicians to report patients' (p<0.001) and physicians' worry about death (p=0.016) as quite or very important in decision-making. Other factors more likely to be of greater importance in determining RAI use for physicians with lower thyroid cancer patient volume versus higher include the accepted standard at the affiliated hospital (p=0.020), beliefs about RAI expressed by colleagues comanaging patients (p=0.003), and patient distance from the nearest facility administering RAI (p=0.012).
Conclusion:
In addition to the extent of disease and adequacy of surgical resection, physicians place importance on physician and patient worry about death from thyroid cancer when deciding whether to treat a patient with RAI. The factors important to physician decision-making differ based on physician thyroid-cancer case-volume, with worry about death being more influential for low–case-volume physicians. As the mortality from thyroid cancer is low, the importance placed on death in decision making may be unwarranted.
Introduction
The use of radioactive iodine (RAI) for remnant ablation following surgical resection for well-differentiated thyroid cancer has increased (7,8), but there is still controversy regarding the effectiveness of postoperative RAI use for reducing mortality and disease-specific survival in the majority of thyroid cancer patients (9 –12). Recently, a study found that postoperative RAI used for well-differentiated thyroid cancers does not impact survival of patients designated as low risk after thyroidectomy (13). The increasing use of RAI in thyroid cancer has health implications, as the risk–benefit ratio for RAI use may not be favorable in low-risk patients. Reported adverse effects include eye/nasolacrimal, salivary, pulmonary, gastrointestinal, hematopoietic, and gonadal dysfunction, as well as development of second primary malignancies (8,14 –16). Moreover, escalating healthcare costs from unnecessary RAI use in these patients will be unjustifiable. Although our previous work has demonstrated a relationship between surgeon preference for more intensive management and greater subsequent RAI use (17), and between the specialty of the primary decision-maker and RAI use (18), the factors that contribute to physician decision-making for RAI use post-thyroid surgery remain unknown.
In an effort to identify the factors that influence whether a physician recommends that a thyroid cancer patient receive RAI after thyroid surgery, we surveyed nonsurgical physicians involved in thyroid cancer management.
Methods
Data source and study population
As previously described by Haymart et al. (17,18), surgeons from randomly sampled hospitals affiliated with the National Cancer Database were surveyed. The 560 surgeon respondents were then asked to “please list the names, specialties, and hospital affiliations of the physicians who provide care to your thyroid cancer patients or administer RAI when needed.” The 903 physicians identified by the surgeons were the subjects of this second survey study.
The modified Dillman survey method (19) was used to enhance survey response rates. This protocol consists of (i) an initial mailing of an introductory letter, the survey instrument, a postage-paid return envelope, and a small gift, (ii) a postcard reminder 3 weeks later, and (iii) a second survey with a postage-paid return envelope to all nonresponders after another 2 weeks.
Data from the survey were de-identified and the double entry method was used to ensure <1% error. The study was granted exemption by the University of Michigan Institutional Review Board.
Measures
Before administration to targeted physicians, the survey instrument was piloted in a multidisciplinary group of providers at the University of Michigan. The survey instrument was created and reviewed by a multidisciplinary group of providers, consisting of health services researchers involved in survey methodology and providers from the fields of endocrinology, surgery, and nuclear medicine. The instrument was then piloted in a cohort of endocrinologists and nuclear medicine physicians in Ann Arbor, Michigan. After piloting, minor revisions were made before survey administration.
Subsequently, the survey was administered. A 5-point Likert scale was used for the 17 survey items addressing factors involved in RAI decision making, with the following options: 1=not at all important, 2=a little important, 3=somewhat important, 4=quite important, and 5=very important. Respondents were asked to rate the following factors' importance in influencing whether a thyroid cancer patient receives RAI: extent of disease, adequacy of surgical resection, patient age, the accepted standard of care at the affiliate hospital, the beliefs about RAI treatment expressed by colleagues comanaging the patient, patient level of flexibility at work, patient willingness to receive RAI, patient interest in conceiving a child, presence of young children in the patient's home, patient distance from nearest facility that administers RAI, patient ability to tolerate thyroid hormone withdrawal before RAI, patient anxiety about their diagnosis and prognosis, patient worry about complications from RAI, patient worry about death from thyroid cancer, physician worry about litigation, physician worry about complications from RAI, and physician worry about patient death from thyroid cancer.
Statistical analysis
The 5-point Likert scale used to rate the factors influencing use of RAI for thyroid cancer was dichotomized to very and quite important versus not at all, a little, and somewhat important. Descriptive statistics were generated.
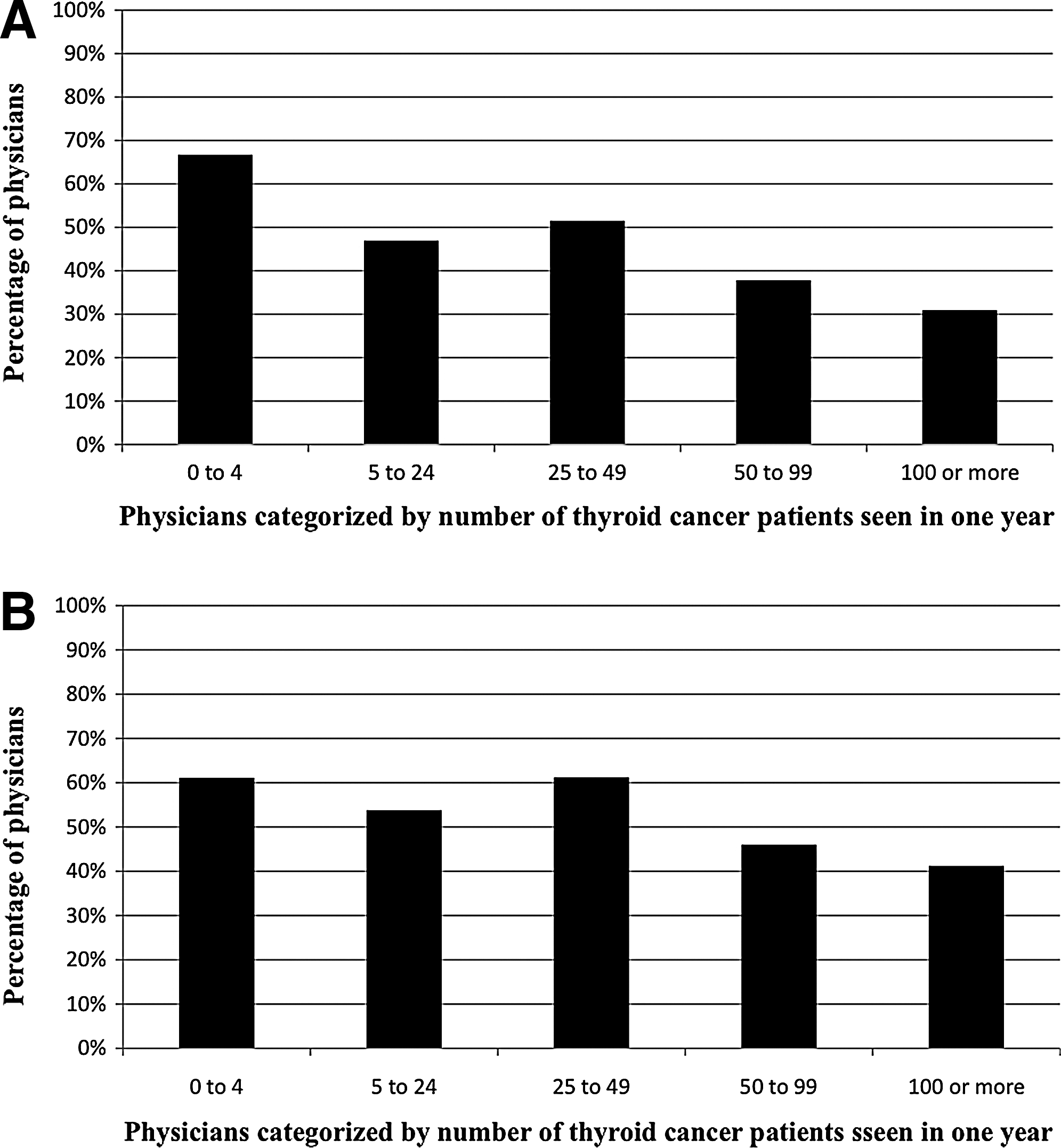
Based on the survey, the provider case-volume was categorized in intervals of 0–4, 5–24, 25–49, 50–99, and 100 or more patients with thyroid cancer seen in 1 year. Multivariable logistic regression analysis controlling for gender, age, specialization, provider case volume, and whether providers personally administer RAI, was performed to determine correlates of importance placed on patient's and physician's worry about death. Additional multivariable logistic regression analyses controlling for gender, age, specialization, and whether providers administer RAI, were performed evaluating differences between low versus higher case volume physicians.
All statistical tests were performed using SAS 9.2 (SAS Institute, Inc., Cary, NC). Two-sided tests were used with p<0.05 considered as statistically significant.
Results
Seventeen of 903 surveyed physicians were found to be ineligible for the survey because they were unreachable due to incorrect mailing address and 33 were ineligible because they were deceased, ill, retired, or not treating thyroid cancer patients. Of the 853 response-eligible physicians, 534 (63%) completed the survey; these respondents represent 251 of the sampled hospitals.
Table 1 shows the respondent characteristics. The majority of the respondents were white and male (79% and 74%, respectively), and the mean age was 52 years. Respondents had an average of 20 years in practice; 67% were endocrinologists, 15% nuclear medicine providers, 10% other, 5% oncologists, and 2% radiologists. From the category other, 71% answered radiation oncology as their specialization. In regard to practice setting, 57% were in private practice, 23% in an academic tertiary care center, 15% in a community-based academic affiliate, and 5% in other settings. Of the respondents, 62% answered that they do not routinely administer RAI in their practice.
RAI, radioactive iodine.
Figure 1 shows that the extent of disease (94%), adequacy of surgical resection (87%), patients' willingness to receive RAI (64%), and patients' age (62%) were reported to be important factors influencing recommendations regarding RAI use for patients with thyroid cancer. Both physicians' (53%) and patients' (45%) worry about death from thyroid cancer were also important in determining RAI use. Physicians with less thyroid cancer cases per year were more likely to report physicians' and patients' worry about death as quite or very important in decision making. The median values for the 17 factors that influence RAI use are listed in Table 2.
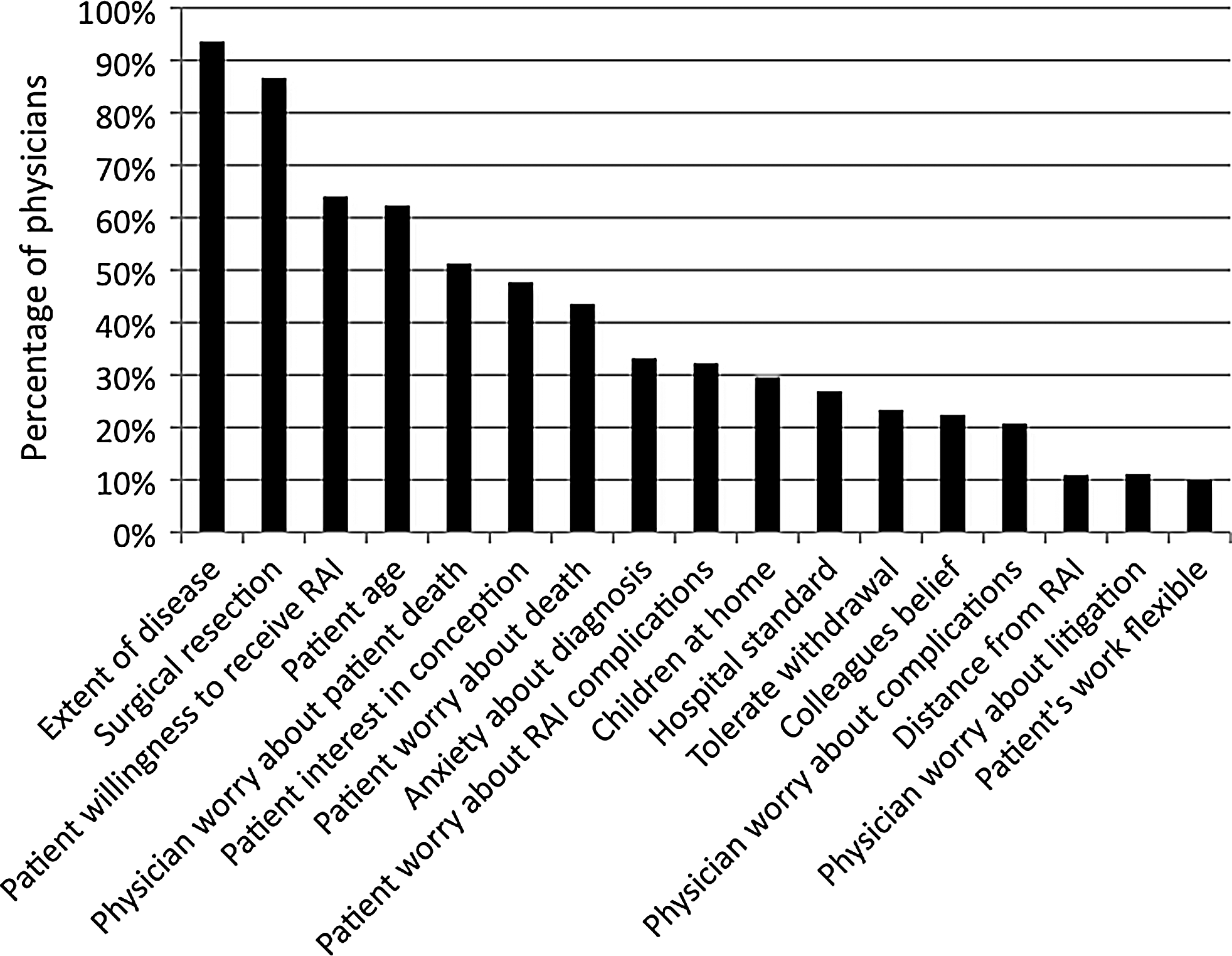
Factors physicians report as quite or very important in influencing whether a patient receives radioactive iodine (RAI) therapy for treatment of thyroid cancer.
The range for all 17 items was 1–5.
In analyzing responses from providers surveyed by region, we found that there was variability in the degree to which providers rated the importance of hospital standards in their decision making regarding RAI use. The physicians surveyed from the East South Central region placed the least importance, while the physicians surveyed from the Mid-Atlantic region placed the most importance on hospital standards (p-value<0.001). None of the other sixteen survey items differed by region.
After controlling for physician gender, age, specialization, and whether the provider personally administers RAI, lower volume physicians were statistically more likely to place importance on patients' worry (p<0.001) (Fig. 2A and Table 3) and physicians' worry about death (p=0.016) compared to high-volume physicians (Fig. 2B and Table 4). Other factors more likely to be rated as quite or very important to physicians with lower thyroid cancer patient volume include accepted standards at affiliated hospital (p=0.020), beliefs about RAI expressed by colleagues comanaging patients (p=0.003), and patient distance from the nearest facility administering RAI (p=0.012).
Discussion
The results of this study improve our knowledge of the factors that influence whether a physician recommends RAI for a patient with well-differentiated thyroid cancer. Extent of disease, adequacy of surgical resection, patients' willingness to receive RAI, and patients' age were the most important factors influencing recommendations regarding RAI use for patients with thyroid cancer. Interestingly, patients' and physicians' worry about death also played an important role in decision making. Compared to higher volume physicians, physicians with less thyroid cancer cases each year were more likely to prioritize patients' worry and physicians' worry about death, accepted standards at affiliated hospital, beliefs about RAI expressed by colleagues comanaging patients, and patient distance from the nearest facility administering RAI.
Previous work has shown a significant rise in the proportion of patients with well-differentiated thyroid cancer treated with RAI after surgery, as well as a wide hospital-level variation in RAI use in these patients (7). It is now known that both the specialty of the primary decision maker (18) and the thyroid surgeon's tendency for more aggressive management are associated with greater RAI use in patients with low-risk disease (17). However, the clinical and nonclinical factors influencing physician decision making in RAI use have not been previously studied. As the most recent clinical guidelines leave the use of RAI to provider discretion in a large proportion of patients (20), understanding the clinical and nonclinical factors that providers use in their decision-making process is critical to understanding the rise in RAI use. This knowledge will ultimately encourage tailoring of treatment to disease severity. Our study has shown that significant importance is placed on both physicians' and patients' worry about death. This is remarkable considering that there is unclear survival benefit to RAI use in the majority of thyroid cancer patients as most patients have an excellent prognosis regardless of intervention (10,20 –22). A recent study by Schvartz et al., with follow-up of 10.3 years, failed to prove any survival benefit of RAI after surgery in a large cohort of low-risk, well-differentiated thyroid cancer patients (13). Moreover, the benefits of RAI use in these patients may not always exceed the risks (8,14,15).
Several studies have investigated the importance of worry about death from cancer when considering treatment, especially among breast and ovarian cancer patients (23,24). However, these primarily focus on patients with advanced cancer. Our study's results are novel, in that, worry about death appears to influence treatment in a cancer with a generally favorable prognosis.
The strengths of this study include an innovative research question, a large sample size of providers and hospitals, and a high response rate among providers. However, this study has limitations. First, survey studies in general carry a risk for nonresponse bias. Second, it is not known whether the provider report to the survey questions is consistent with provider treatment behavior. Third, although the survey included a comprehensive set of factors that may influence physician decision making, there may be other factors that we did not inquire about. Finally, although this study focuses solely on the physician, the patient is also involved in the decision-making process.
Despite its limitations, this study sheds light onto some of the factors involved in provider decision making in regard to RAI use in patients with well-differentiated thyroid cancer. Surprisingly, importance is placed on worry about death by both patients and providers. As the mortality from well-differentiated thyroid cancer is low, the importance placed on death in decision making may be unwarranted. Fear may be driving the rise in RAI use, suggesting a role for better provider education and further research into the risk–benefit of low-risk thyroid cancer treatments.
Footnotes
Acknowledgments
The authors thank Brittany Gay, Barbara Salem, Ashley Gay, and Kathryn Schuessler for their work in data collection and processing. We also acknowledge the endorsement from the American Thyroid Association and the collaboration with the American College of Surgeons Commission on Cancer. Dr. Papaleontiou is supported by the NIH Institutional National Research Service Award (T32). This study was funded by K07CA154595-02 to Dr. Haymart from the National Institutes of Health, the University of Michigan Comprehensive Cancer Center Idea Award, the Cancer Surveillance and Outcomes Research Team (CanSORT) Pilot of Feasibility Fund, and the Elizabeth Caroline Crosby Fund.
Disclosure Statement
There are no commercial associations or conflicts of interest to be disclosed by any of the authors of this manuscript.