
Abstract
Background:
Historically, systemic therapy for radioactive iodine (RAI)–refractory thyroid cancer has been understudied. Available drugs have modest efficacy. Romidepsin is a histone deacetylase inhibitor with potent antitumor effects both in vitro and in vivo. In thyroid cancer cell lines, romidepsin increases expression of both thyroglobulin and the sodium iodide symporter messenger RNAs, suggesting the possibility of improved iodine concentrating ability of RAI-resistant tumors.
Methods:
This was a single-institution Simon 2-stage phase II clinical study. Eligible patients had progressive, RAI-refractory, recurrent/metastatic, nonmedullary, nonanaplastic thyroid cancer. Response Evaluation Criteria in Solid Tumors (RECIST) 1.0 measurable disease and adequate organ/marrow function were required. Romidepsin 13 mg/m2 was administered intravenously on days 1, 8, and 15, in cycles of 28 days. The primary endpoint was the response rate by RECIST; change in RAI avidity was a secondary endpoint. The study closed after the first stage due to the lack of response.
Results:
Twenty patients were enrolled: female, 50%; median age, 64 years; histology, 8 papillary/1 follicular/11 Hürthle. Grade 4–5 adverse events (AEs) possibly related to the drug: grade 5, 1 sudden death; grade 4, 1 pulmonary embolus. Twelve of 20 subjects had a reported adverse event. No RECIST major responses have been seen. Response per protocol: stable disease, 13; disease progression, 7. Restoration of RAI avidity was documented in two patients. Median overall survival and time on study was 33.2 (1–71+) and 1.7 (0.46–12) months, respectively.
Conclusions:
We observed preliminary signs of in vivo reversal of RAI resistance after treatment with romidepsin. However, no major responses were observed and accrual was poor after the grade 5 AE.
Introduction
Unfortunately, current approaches to the treatment of progressive RAI-refractory thyroid cancer are limited. Doxorubicin is the only FDA-approved treatment in this setting. More recently, there has been significant promising research evaluating the benefit of various tyrosine kinase inhibitors in this setting (4 –8). However, there is no clear evidence that either doxorubicin or other systemic agents significantly improve survival compared to supportive care and local measures only (e.g., palliative radiation therapy or surgery).
Histone deacetylase (HDAC) inhibitors have been shown to repress growth of anaplastic thyroid cancer cells through the induction of apoptosis and phase-specific arrest (9,10). In the laboratory, HDAC inhibitors have been shown to increase RAI uptake in poorly differentiated and anaplastic thyroid cancer cell lines (11,12). HDAC inhibitors have also been shown to enhance the effects of cytotoxic chemotherapy (doxorubicin) in anaplastic cell lines (13).
Romidepsin (NSC 630176, FR901228; Depsipeptide) is a unique bicyclic peptide, originally isolated from Chromobacterium violaceum, that was shown to be an HDAC inhibitor in 1998 (14). Two phase I studies have been performed in patients with advanced solid tumors to determine its maximum tolerated dose (MTD). When romidepsin was given as a 4-hour infusion on days 1 and 5 of a 21-day cycle (15), the MTD was 17.8 mg/m2 due to dose-limiting asthenia and fatigue. The MTD for an alternative phase I schedule of romidepsin, given on days 1, 8, and 15 of a 28-day cycle, was 13.3 mg/m2, with asthenia and fatigue again representing the dose-limiting toxicities (16). Preclinical data with romidepsin have shown dedifferentiation in thyroid cancer cell lines, including an increased expression of sodium iodide symporter (NIS) RNA (12) in addition to growth inhibition and apoptosis (17).
Based on this preclinical work, a phase II study with romidepsin for the treatment of RAI-refractory nonmedullary thyroid cancer was undertaken at Memorial Sloan-Kettering Cancer Center (MSKCC). The primary objective of the study was to evaluate the response rate and safety of romidepsin in this setting. The main secondary objective was to assess the effects of romidepsin on NIS through the use of RAI scans.
Materials and Methods
Eligibility criteria
Patients were required to have a histology- or cytology-confirmed diagnosis of nonmedullary thyroid carcinoma (papillary, follicular, or Hürthle cell), reviewed at MSKCC. In addition, patients were required to have measureable disease fulfilling Response Evaluation Criteria in Solid Tumors (RECIST) 1.0 criteria (18). The cancer needed to be progressive as defined by one of the following criteria: (i) presence of new or progressive lesions; (ii) new lesions on bone or fluorodeoxyglucose-positron emission tomography (FDG-PET) scan; or (iii) rising thyroglobulin documented by three consecutive rises. The cancer must have been RAI-refractory as defined by absent or insufficient (defined as “faint” or “minimal,” based on the independent assessment by two observers from either endocrinology or nuclear medicine) RAI uptake as documented by a whole-body RAI scan <6 months before initiation of therapy on protocol. Biologic/targeted agents or radiotherapy were not allowed within the 4 weeks before starting romidepsin. Prior cytotoxic chemotherapy was not allowed except if administered as a radiation sensitizer >3 months before initiation of romidepsin. Adequate renal function (serum creatinine within normal institutional limits or urine creatinine clearance ≥60 mL/min) and hepatic function (total bilirubin within normal institutional limits, serum glutamic oxaloacetic and pyruvic transaminase [SGOT and SGPT, respectively] <2.5×upper limit of normal upper limits), and Eastern Cooperative Oncology Group (ECOG) performance status <2 were required. Patients with a history of brain metastases were excluded. Pregnant or lactating females were excluded; a negative pregnancy test was required of all females with child-bearing potential. The protocol was approved by the National Cancer Institute (NCI) and MSKCC Institutional Review Board. All participating patients were required to provide written informed consent.
For the first 13 patients, exclusion criteria included a history of serious ventricular arrhythmia or QTc >500 ms. In addition, patients were excluded if there was cardiac hypertrophy, clinical evidence of conduction disturbances or NY class III or IV congestive heart disease, poorly controlled angina, uncontrolled dysrhythmias, or history of myocardial infarction within 12 months of study entry.
After the first 13 patients, there was an unexplained sudden death of a study patient. The study was then amended and patients were excluded also if the screening EKG showed QTc >480 ms or ST segment depression ≥2 mm. In addition, subjects were excluded if there was a history of sustained ventricular tachycardia, ventricular fibrillation, Tirade de Pointes, or cardiac arrest unless currently addressed with an automatic implantable cardioverter defibrillator; any cardiac arrhythmia requiring anti-arrhythmic medication other than a beta blocker or calcium channel blocker, or patients in whom digitalis cannot be discontinued; hypertension (i.e., blood pressure ≥160/95); Mobitz II second degree block in patients who do not have a pacemaker (patients with first degree or Mobitz I second degree block, bradyarrhythmias, or sick sinus syndrome requiring Holter monitoring and evaluation by cardiology), and patients with any other cardiac disease could be excluded at the discretion of the Principal Investigator following consultation with cardiology. Furthermore, it was required that an echocardiogram be done at screening and subjects were excluded if it showed left ventricular ejection fraction <50%, left ventricular hypertrophy as defined by end-diastolic wall thickness of >12 mm in both the left ventricular posterior wall as well as septum, or restrictive cardiomyopathy.
Trial design
The primary objectives of the study were to determine the antitumor activity of romidepsin per RECIST (either by major response or clinical benefit) in RAI-refractory nonmedullary thyroid cancer along with safety/tolerability of the dosing regimen. Clinical benefit was defined as stable disease for 6 months. A secondary objective was to assess the effects of romidepsin on NIS expression in vivo (i.e., changes in RAI uptake). Other secondary objectives included (i) evaluation of post-treatment changes in serum thyroglobulin; (ii) correlate changes in post-treatment FDG-PET scans with whole-body RAI scans; and (iii) on a preliminary basis, evaluate changes in the expression of NIS on pre- and post-treatment biopsy specimens. Unfortunately, the latter objective could not be analyzed since only one patient had a post-treatment biopsy (which was not either of the patients that had RAI reversal on a scan).
This was a single-institution (MSKCC) Simon 2-stage phase II clinical study. Romidepsin was administered on an outpatient basis at a dose of 13 mg/m2 as a 4-hour infusion on days 1, 8, and 15 of each 28-day cycle. A 5HT3 antagonist and dexamethasone 12 mg was given before each infusion and an antiemetic (e.g., metoclopramide) was administered after the completion of therapy as indicated.
Criteria for removal of the study included disease progression, unacceptable adverse event(s) or delay due to toxicity of greater than 4 weeks, or clinically significant reversal of RAI resistance as documented by serial RAI scans.
Study assessments
Baseline radiographic studies (noncontrast CT scan and/or MRI) and a PET scan were required before starting therapy. Radiographic studies were repeated every two cycles. The PET scan was repeated after the second and sixth cycle of therapy. An RAI scan was repeated after cycle 2 of therapy. Repeat RAI scans were done after patients received Thyrotropin alfa 0.9 mg intramuscularly daily on 2 consecutive days, starting 2 days before RAI administration. Serum thyroglobulin levels were measured every two cycles.
For safety, patients were monitored before each infusion with an electrocardiogram (ECG), complete blood counts, and serum electrolytes, creatinine, blood urea nitrogen (BUN), glucose, liver function tests, and magnesium. The same laboratory studies were done weekly. Patients were evaluated by a physician on days 1 and 15, and other times as needed. Adverse event reporting was done on the day of each treatment using the NCI Common Terminology Criteria for Adverse Events version 3.0. ECGs were performed before each infusion, 1 hour after each infusion, and between 24 and 72 hours after administration of romidepsin. In addition, safety parameters were reviewed at least twice a year by an outside Safety Monitoring Board. One dose reduction was allowed.
After a grade 5 event, when the study was reopened, all patients were required to have an ECG before the start of treatment.
Statistical analyses
Response rates were defined per RECIST 1.0 (18). The study's primary objective was a major response within 8 weeks of treatment initiation or clinical benefit (stable disease for at least 6 months). An optimal Simon 2-stage design was used for undesirable and promising major response rates of 5% and 20%. Setting the type I error rate at 5% and type II at 10%, it was required that 21 patients be treated initially and if there were 2 or more major responses (or, in lieu of this, 9 or more subjects showed clinical benefit), an additional 20 patients would be added. Per protocol, all patients who met the eligibility criteria (unless they received no medication) must be included in the main analysis of the response rate, with the definition of disease progression (failure to respond to therapy) to include subjects defined as progressive disease, early death from progressive disease, early death from malignant disease, early death from toxicity, early death from other cause, and unknown (i.e., not assessable or insufficient data).
To analyze the PET scan response, the SUVmax values of 5 lesions (SUVmax-sum) were added together and the percent differences were compared between the baseline FDG-PET scan and the FDG-PET scan after the second cycle. Comparison of this outcome to best response by RECIST was done using Pearson correlation.
Results
Patient characteristics
Subjects were accrued between November 16, 2004, and September 20, 2007. The last treatment was given December 26, 2007. A total of 20 subjects were accrued to the study. Thirteen patients were accrued between November 16, 2004, and April 25, 2005. However, after the grade 5 toxicity event, the study was temporarily suspended to both accrual and treatment. After the study reopened, accrual was poor and only seven patients entered the study between May 8, 2006, and September 20, 2007. The study was closed after the first 20 patients since it would have been impossible to reach the objective of the first stage to expand the study to a second stage. The median age of the patients was 64 years (range 30–78). Fifty percent were female.
Histology included: papillary, 8; follicular, 1; and Hürthle cell carcinomas, 11. Median Karnofsky Performance Status was 90% (range 80%–100%).
Toxicity
There was one grade 4 event (pulmonary embolus) and one grade 5 event (sudden death) that were thought to be possibly related to treatment. The cause of the sudden death remains unknown. The patient died 2 days after receiving his third dose of romidepsin (cycle 1, day 17). This subject had experienced no other grade 2 or greater toxicity. Two other subjects died during the study; however, both deaths were felt to be related to progression of disease.
Grade 3 nonhematological events that were thought to be at least possibly related to drug were fatigue, 1; dysphagia, 1; dyspnea, 1; and prolonged QTc interval on ECG, 1. Table 1 summarizes all of the toxicity data related to romidepsin.
WBC, whole blood count; SGPT, serum glutamic pyruvic transaminase; SGOT, serum glutamic oxaloacetic transaminase.
Clinical activity
By the criteria set in the protocol, there were 0 patients with a major response, 13 (65%) with stable disease, and 7 (35%) with disease progression. Of those with stable disease on study, only two remained on study without progression for at least 6 months. Only two patients had at least 10% shrinkage by RECIST criteria of their tumor as their maximum response. The breakdown of cause for disease progression was: progressive disease, 5; sudden death, 1; and withdrawal of consent before completing two cycles, 1. The reasons for coming off study by response are listed in Table 2.
RAI, radioactive iodine.
Of the 13 subjects with stable disease, 1 had progression of disease (POD) after six cycles of treatment, 4 eventually withdrew due to toxicity, 3 patients decided to withdraw due to lack of RAI uptake on the whole-body iodine scan, and 3 withdrew consent during the suspension of the study. The final two subjects were removed from the study due to apparent RAI reversal. Of the subjects who had stable disease, five received more than two cycles of romidepsin. Three of these five received at least six cycles of romidepsin. The longest any patient received treatment was for 12 cycles. The median time on treatment was 1.7 months (range 0.46–12 months).
In this study, the median overall survival was 33.2 months (range 1–71 months). Sixteen subjects have died. The median overall survival was 43.1 months (range 8–71 months) within the group of 13 patients who had stable disease compared to 3.7 months (range 1–64 months) in the group of 7 patients who had disease progression (p=0.08 by Log-rank Test). Of the subjects who had stable disease, 4 out of the 13 were still alive at last follow-up, while all of the patients who had progressive disease had died (Fig. 1).
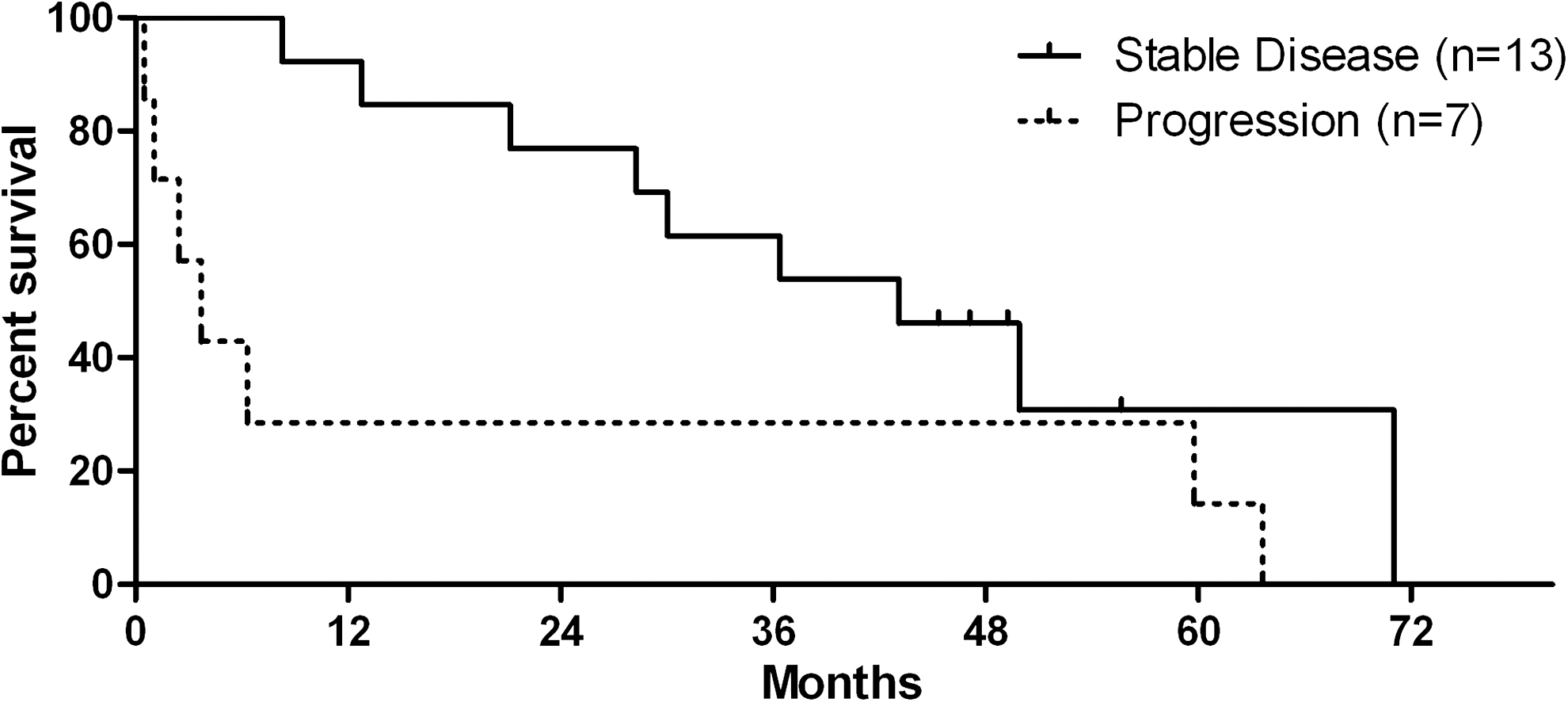
Overall survival comparing group with stable disease (n=10) and group with disease progression (n=10).
Due to the short time on the study for the majority of patients, changes in serum thyroglobulin are only reported for the patients who received treatment for at least 1 month (total of 13 subjects). One subject was excluded due to the presence of antithyroglobulin antibodies making the thyroglobulin levels uninterpretable. Of the remaining 12 subjects, after 8 weeks, 8 had a rise in their serum thyroglobulin (range of 8%–270%). All eight of these patients were on treatment for less than 2 months. Of the remaining four subjects, the decline in thyroglobulin ranged from 0% to 31% at 8 weeks. All four of these patients were on study for greater than 2 months.
RAI avidity
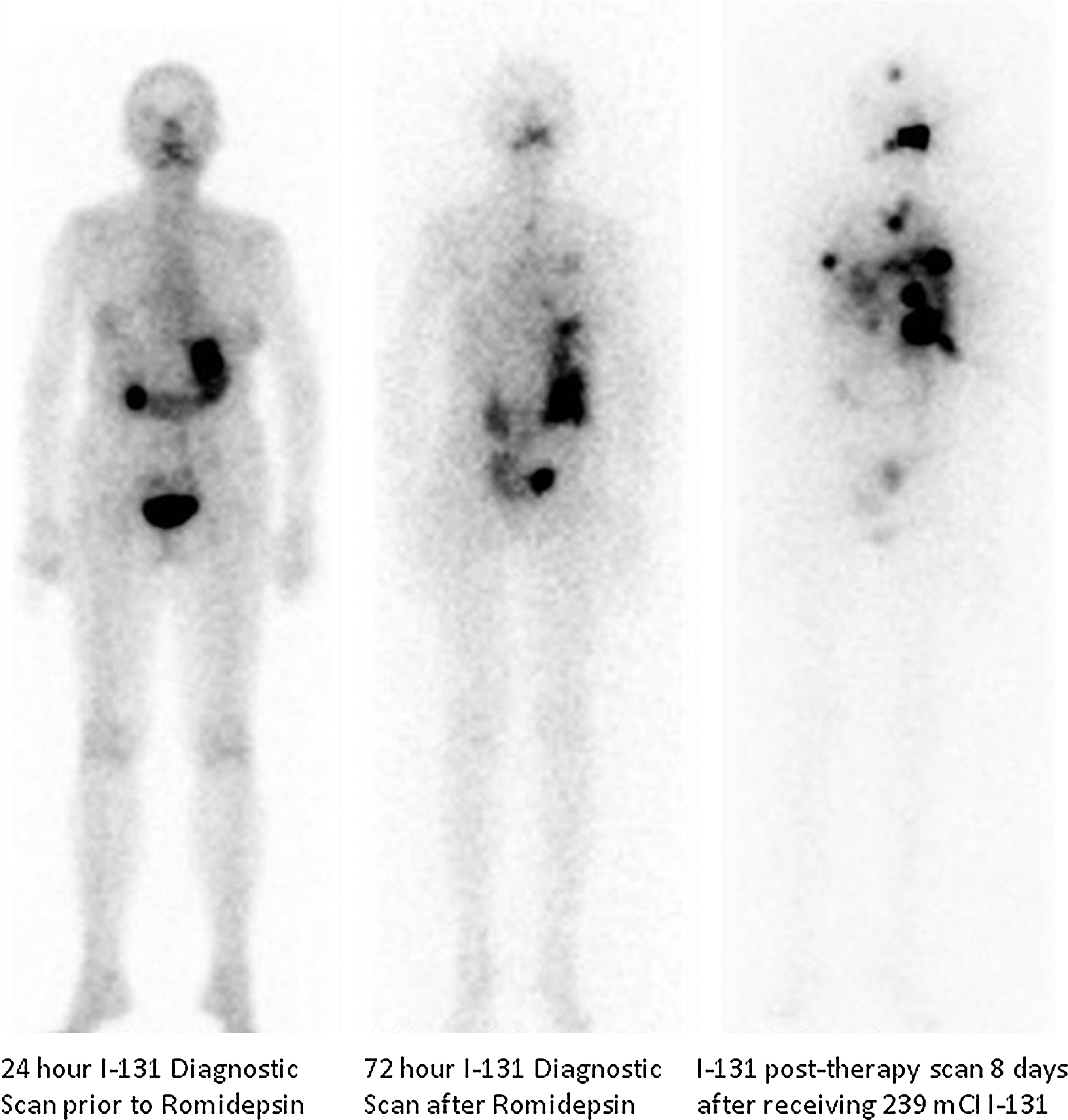
Repeat RAI scans were done in 16 of the 20 patients on the clinical study. There were two reversals. One reversal occurred after the patient was on romidepsin for 12 cycles. The other had a reversal after two cycles. Both were retreated with RAI. See Figures 2 and 3 for example.

Reversal of radioactive iodine (RAI) avidity in patient 1.
Reversal of RAI avidity in patient 2.
Patient 1 (Hürthle cell carcinoma) had a negative RAI scan about 1 month before the start of treatment and again after two cycles. He had a repeat RAI scan around his 12th cycle, which showed RAI uptake localizing to a nodule in the right lung. He was treated with 250 mCi of RAI. Unfortunately, serial serum thyroglobulin measurements were uninterpretable because of the presence of antithyroglobulin antibodies. A CT done 3 months after treatment with RAI did show a decrease in the size of the lung nodule; however, other metastases were growing and the patient restarted systemic therapy.
Patient 2 (papillary carcinoma) had a negative RAI scan 5–6 months before starting the clinical trial. After two cycles of treatment, the RAI scan showed multiple foci of abnormal increased iodine tracer uptake in the neck, left lung, and left pleura, all of which were new. The patient received 240 mCi of RAI. Her serum thyroglobulin before treatment was 1050 ng/mL. Three months later, it had declined down to 410 ng/mL. Unfortunately, a CT scan at that time showed progression of the disease in all nodules.
PET scans
Only 12 of the 20 patients on the study had PET scans after the second cycle. Changes in the PET scans (see Materials and Methods for definition) ranged from −50% to +37%. Nine patients had decreases in the SUVmax (three patients with >25% decrease). There was no significant correlation between the PET scan response and response by RECIST criteria. Of the two patients with RAI reversal, patient 1 had a decrease in SUVmax-sum of 24% and patient 2 had an increase in SUVmax-sum of 8%.
Discussion
The primary objective of this study was to evaluate the response rate in RAI-refractory thyroid cancer with the use of romidepsin. No major responses were seen in this group. However, the study was complicated by an unexpected sudden death. Due to the death, the study was suspended for a short time (about 6 months) during which five patients came off study before completing two cycles of treatment. Furthermore, this event led to a significant slowing of accrual.
The cause of death in the one subject is still unclear. The subject had completed one cycle (three treatments) of romidepsin with no significant reported toxicity. No autopsy was performed. For safety reasons, it was decided to temporarily suspend the study (i.e., all active subjects stopped treatment and no patients were accrued to study) while this was being investigated, and all patients who were on the study were informed of the incident. During the period, while the study was being suspended, two patients decided to withdraw from the study.
While there were no responses seen, only 3 of the 20 patients (15%) actually had progression of their disease while receiving active treatment. Three subjects completed six or more cycles. Of these patients, one stopped after 6 cycles due to a prolonged QTc interval on ECG, one withdrew consent after 6 cycles, and one came off study after 12 cycles due to RAI reversal. A phase I study by Piekarz et al. (19) did not show any responses in the nine patients they treated with romidepsin. However, six of the nine patients with thyroid cancer did have stable disease for a median of 33 weeks. Woyach et al. (20) evaluated the HDAC inhibitor vorinostat in a phase II study for subjects with RAI-refractory thyroid cancer. They also noted no responses in the 16 patients with differentiated thyroid cancer. They noted stable disease in nine patients with a median duration of 24 weeks.
RAI reversal was a secondary hypothesis of this study. The phase I study by Piekarz et al. (19) using a different dosing schedule for romidepsin did not show RAI reversal in 4 patients who had follow-up diagnostic RAI scans. In the study by Woyach et al. (20), one out of three subjects had RAI reversal of their tumor with the use of vorinostat. Preclinical data have suggested that romidepsin can increase NIS expression and uptake of iodine in thyroid cancer cell lines (11,12). Sixteen of the 20 participants in the study had an RAI scan during treatment. Of these 16 subjects, 2 had RAI reversal. After RAI reversal, both subjects withdrew from the protocol and were treated with RAI. However, despite receiving RAI treatment, neither patient had a long-term benefit from the treatment.
Conclusions
No responses, only stable disease, were seen with romidepsin in the treatment of RAI-refractory thyroid cancer, which is consistent with other studies evaluating single-agent HDAC inhibitors. Preclinical data using HDAC inhibitors with cytotoxic chemotherapy in thyroid cancer cell lines suggest a potential role as a chemotherapy sensitizer that could still be considered in future clinical studies (13,21). The true efficacy of romidepsin against RAI-refractory thyroid cancer is difficult to determine in this study due to the effect of an unexpected sudden death, which led to the temporary suspension of the study during which 25% of the subjects were removed from the study. However, confirmation of preclinical data that romidepsin could sensitize refractory thyroid cancer to RAI was obtained in this study, although a significant clinical benefit due to this sensitization was not found. We would not recommend further investigation of romidepsin as a single agent in RAI-refractory thyroid cancer.
Footnotes
Acknowledgment
This study was funded by Grant N01 CM 62206.
Disclosure Statement
No conflict of interest exists for any of the authors.