
Abstract
Purpose:
To describe the outcome of patients with poorly differentiated thyroid cancer (PDTC) presenting with gross extrathyroidal extension (ETE).
Materials and Methods:
After obtaining Institutional Review Board approval, we performed a retrospective review of a consecutive series of thyroid cancer patients treated by primary surgical resection with or without adjuvant therapy at Memorial Sloan-Kettering Cancer Center from 1986 to 2009. Out of 91 PDTC patients, 27 (30%) had gross ETE (T4a), and they formed the basis of our study. Of 27 patients, 52% were women. The median age was 70 years (range 27–87 years). Ten patients (37%) presented with distant metastases; four to bone, three to lung, and three to both bone and lung. All patients had extended total thyroidectomy, except two who had subtotal thyroidectomy. Twenty patients (74%) had central compartment neck dissection and 11 also had lateral neck dissection. Four patients had pN0, six (30%) pN1a, and 10 (50%) pN1b neck disease. Twenty-one patients (77%) had adjuvant therapy: 15 (55%) radioactive iodine (RAI) only, three (11%) postoperative external beam radiation (EBRT) only, and three (11%) had both RAI and EBRT. Overall survival (OS), disease-specific survival (DSS), local recurrence–free survival (LRFS), and regional recurrence–free survival (RRFS) were calculated by the Kaplan Meier method.
Results:
The median follow-up time was 57 months (range 1–197 months). The 5 year OS and DSS were 47% and 49%, respectively. This poor outcome was due to distant metastatic disease; 10 patients had distant metastases at presentation and a further six developed distant metastases during follow-up. Locoregional control was good with 5-year LRFS and RRFS of 70% and 62%, respectively. Overall, eight patients (30%) had recurrences: two had distant alone, two regional, two regional and distant, one local and distant, and one had local, regional, and distant recurrence.
Conclusion:
Aggressive surgery in patients with PDTC showing gross ETE resulted in satisfactory locoregional control. Due to the small proportion of patients who received EBRT (22%), it is not possible to analyze its benefit on locoregional control. Of significance is the observation that the majority of patients (60%) who presented with or subsequently developed distant metastases eventually died of distant disease. New systemic therapies to target distant metastatic disease are required for improvements in outcome.
Introduction
PDTC tends to present with higher rates of gross extrathyroidal extension (ETE) than differentiated thyroid carcinoma (DTC) (4). In DTC, the presence of gross ETE is the most important tumor characteristic determining outcome along with patient age. Complete surgical removal of all gross disease is the key to a favorable outcome in DTC, and up to 100% 15-year survival rates have been reported (5). In PDTC, however, there is a lack of reports in the literature on the management and outcome of patients with gross ETE. The role of aggressive surgical resection has not been as clearly defined in PDTC as in DTC. The objective of our study was therefore to define the role of aggressive surgical resection on locoregional control and survival in patients with PDTC with gross ETE. We also wanted to study the patterns of treatment failure and report long-term outcome in these patients.
Materials and Methods
Following Institutional Review Board approval, a database search was made of the term PDTC for patients treated by primary surgical resection with or without adjuvant therapy at Memorial Sloan-Kettering Cancer Center (MSKCC) from 1986 to 2009. This produced 72 PDTC patients. Archived histopathology slides were available for 69 patients and were reviewed by two independent pathologists that subspecialized in thyroid malignancy (R.A.G. and D.L.C.) and were blinded to clinical data and outcome. The diagnosis of PDTC (MSKCC) was based on histologic and/or immunohistochemical evidence of follicular cell differentiation and presence of tumor necrosis and/or ≥5 mitoses per 10 high-power fields (×400) (3). Concordance rate between the two reviewing pathologists was 78% and for the rest a consensus diagnosis was reached. Of 69 PDTC cases, 57 were classified as PDTC by the MSKCC criteria, seven as DTC, three as anaplastic cancer, and two as metastatic cancer to the thyroid (lung and adenoid cystic carcinoma). In addition, the pathology of all DTC patients from 1986 to 2009 that died of the disease was also reviewed. This identified 36 further patients with PDTC (MSKCC). The total number of PDTC (MSKCC) patients was 93. Two patients were subsequently excluded: one with inoperable disease, and one with unknown primary site and PDTC in metastatic lymph nodes only. Therefore, the final number of PDTC (MSKCC) patients included in the analysis was 91. Of these, 27 patients (30%) had gross ETE with invasion of adjacent structures (T4a) at presentation based on operative and clinical reports. Staging was classified according to the AJCC Cancer Staging Manual 7th edition (6). These 27 patients form the basis of our analysis. Patient charts were reviewed, and patient characteristics, clinical presentation, treatment, tumor pathological features, recurrences, and survival were recorded. Recurrence was defined as any local, regional, or distant recurrence that was either biopsy-proven or a new radiologic finding identified on computed tomography, magnetic resonance imaging, positron emission tomography (PET) scanning, or by new radioactive iodine (RAI) uptake found at a distant site or in the neck with adequate thyrotropin stimulation. Patients were considered to have died of the disease if it was confirmed by a death certificate or a hospital summary. Overall survival (OS), disease-specific survival (DSS), local recurrence–free survival (LRFS), and regional recurrence–free survival (RRFS) were calculated by the Kaplan Meier method and univariate comparisons between groups were done using the logrank test. Statistical analysis was carried out using commercially available software (JMP version 5.0; SAS Institute Inc., Cary, NC). Given the small sample size, multivariate analysis of outcomes was not possible. All percentages were rounded to the nearest integer.
Results
Patient and tumor characteristics are shown in Table 1. Of 27 patients, 14 (52%) were women. The median age was 70 years (range 27–87). The majority of patients (96%) were 45 years of age and older. Only four patients (15%) had a history of radiation exposure. Fourteen (52%) had a primary tumor that was larger than 4 cm. Twenty patients (74%) underwent neck dissection: all patients had a central compartment neck dissection and 11 patients also had a lateral neck dissection. Four (20%) patients had pN0 and 16 (80%) were pN+: 10 (50%) pN1b and six (30%) pN1a. The surgical margins were reported to be positive on pathology examination in 24 patients (89%). Ten patients (37%) had distant metastases at presentation: four with bone, three with lung, and three with both lung and bone metastases.
M1, distant metastasis at presentation.
Treatment details are shown in Table 2. All patients had an extended total thyroidectomy, except for two who had a subtotal thyroidectomy: in one patient the contralateral lobe was atrophic and was left in situ to be treated with postoperative radioiodine (RAI), and in another patient a small portion of the contralateral normal-appearing lobe was left in situ at the discretion of the operating surgeon. Structures that were most commonly invaded by the primary tumor were upper respiratory tract (67% of patients: five with larynx, five with trachea, and eight with both larynx and trachea involvement), recurrent laryngeal nerve (63%), esophagus (56%), and major veins (11%). Of 27 patients, 19 had more than one structure invaded. Recurrent laryngeal nerve resection, submucosal esophagectomy (excision of the muscular wall of esophagus) and shaving the tumor off the upper airway cartilage with or without cricothyroid muscle resection were the most common types of extended procedures. Gross residual disease was left in five (19%) patients according to the operating surgeon's note. Adjuvant therapy was given in 21 patients (77%): 15 (55%) had RAI alone, three (11%) had postoperative external beam radiation (EBRT) alone, and three (11%) had both RAI and EBRT.
RAI, radioiodine; EBRT, postoperative radiotherapy.
Of five patients with gross residual disease, two patients had only RAI (one had a locoregional recurrence), one had only EBRT (no locoregional recurrence), one had both RAI and EBRT (no locoregional recurrence), and one had no adjuvant therapy after refusing EBRT (the patient had a locoregional recurrence).
Of 19 patients who had only microscopic positive margins, 12 patients had only RAI (five had a locoregional recurrence), two had only EBRT (one had a locoregional recurrence), and two had both RAI and EBRT (no locoregional recurrence). No adjuvant therapy was recommended in two patients (one of them had a locoregional recurrence), and for one the status of adjuvant therapy was not known (the patient had locoregional recurrence). Using Fishers exact test, no statistically significant association was found between EBRT and locoregional recurrence. Systemic therapy (sorafenib followed by doxorubicin) was given to 1 out of 16 patients with distant disease for palliation of RAI-refractory progressive disease. Of 27 patients, 19 patients underwent RAI scanning: 11 had RAI uptake outside the thyroid bed, seven did not have RAI uptake outside the thyroid bed, and for one patient data were not available. Out of 10 patients with distant metastasis at presentation (M1), seven (70%) had RAI-avid M1 disease, one (10%) had non–RAI-avid M1 disease, and two patients did not undergo RAI scanning. M1 PET-positivity was revealed in two patients, while it was negative in three and not done in five (50%) patients with M1 disease.
With a median follow-up of 57 months (range 1–197 months), the 5-year OS and DSS were 47% and 49%, respectively (Fig. 1). Overall, eight patients (30%) had recurrences: two (7%) distant alone, two (7%) regional alone, two (7%) regional and distant, one (4%) local and distant, and one (4%) local, regional, and distant. Ten (37%) patients had persistent distant metastatic disease since initial presentation. The 5-year LRFS was 70% and 5-year RRFS survival was 62%. The 5 year loco-regional recurrence–free survival was 56% (Fig. 2). Of five patients who had gross residual disease, two patients had no locoregional control (one had adjuvant RAI and one patient had no adjuvant treatment) and three patients had locoregional control (one had adjuvant RAI, one EBRT, and one RAI/EBRT). Of 19 patients with only microscopic residual disease (positive margins), eight had no locoregional control (five had adjuvant RAI, one had EBRT, one no adjuvant treatment, and for one data on adjuvant treatment were not available). Of 14 patients (52%) who died of thyroid cancer, 11 patients died of distant disease and three patients died of uncontrollable locoregional disease with distant metastatic disease also being present. The low survival was therefore attributable to distant metastatic disease in the majority of patients, rather than locoregional recurrence.

Disease-specific survival in poorly differentiated thyroid cancer (PDTC) with extrathyroidal extension (ETE). Median survival time: 57 months.
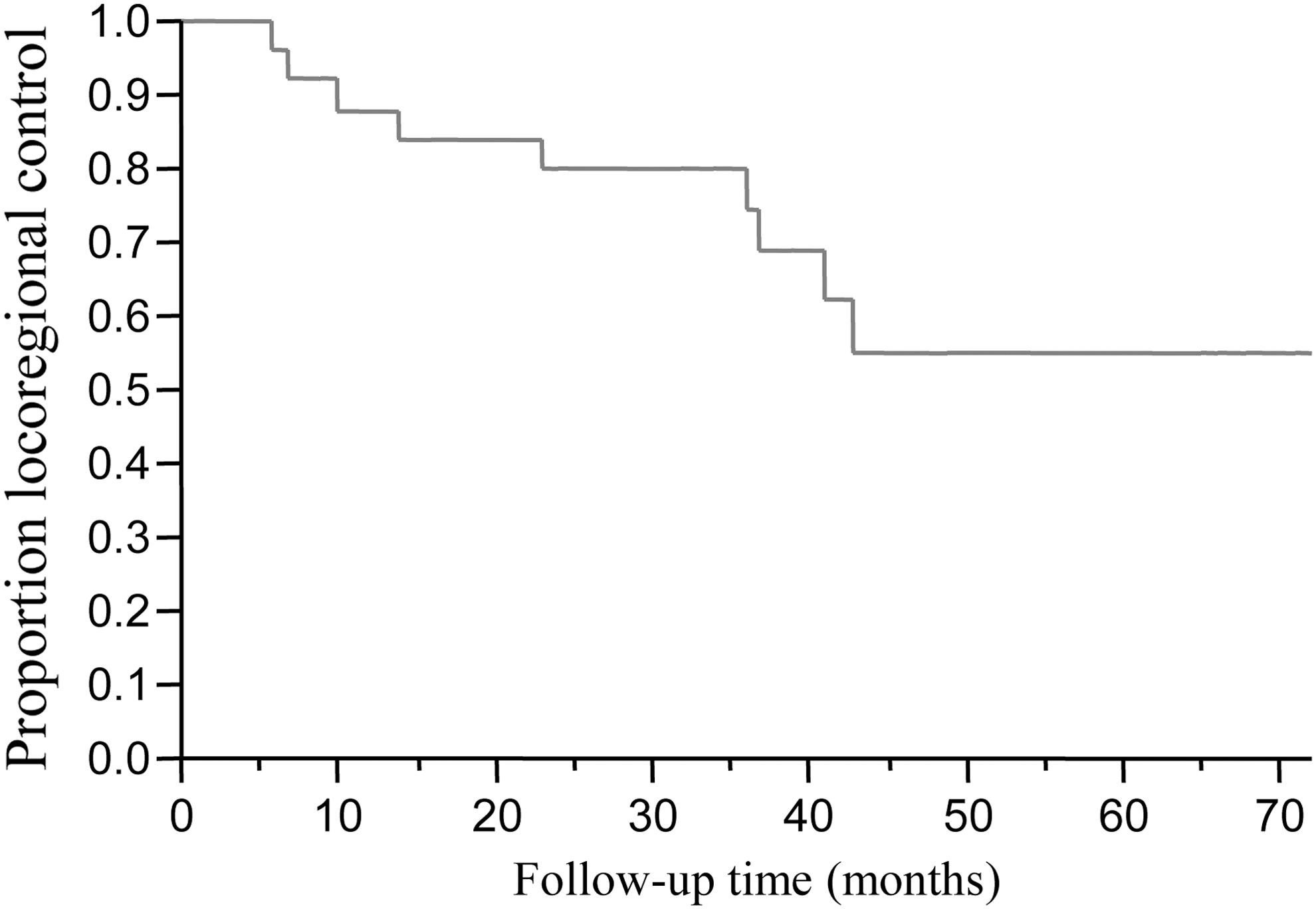
Loco-regional control in PDTC with ETE. 5 year loco-regional control: 56%.
Discussion
PDTC has recently been recognized as a separate entity in the WHO Classification of Endocrine Tumors in 2004 (1) and the Turin proposal (2) based on architecture and high-grade features. It has also been reported that high-grade features such as mitoses, necrosis, nuclear pleomorphism, and invasiveness are of diagnostic and prognostic significance (7,8) and that a more homogenous group of PDTC tumors may be defined if the diagnosis is based on mitosis and necrosis rather than on growth pattern (3). PDTC has an intermediate aggressive behavior in the progression spectrum from DTC to AC. It has a tendency to present with higher rates of local invasion than DTC (4). Although there are literature reports on the outcome of patients with DTC with gross ETE (9,10), clinical studies on PDTC are limited due to its rarity and the heterogeneity of criteria for the diagnosis of PDTC. In DTC, management consists of an aggressive surgical approach in which the goal of surgery is to achieve removal of all gross disease. Indeed high survival rates can be achieved if this aggressive surgical approach is adopted (5). Our policy in the management of patients with PDTC and gross ETE is similar to that of DTC. The goal is to achieve removal of all gross disease in order to control the central compartment of the neck, minimize the risk of locoregional recurrence and hence prevent life-threatening airway obstruction or hemorrhage. However, the efficacy of this type of surgical approach in PDTC has not been reported before. The objective of our study was therefore to assess the efficacy of this approach of gross total surgical resection in the management of PDTC with gross ETE.
PDTC (MSKCC) was relatively rare among our thyroid carcinoma patients (91 patients over a period of 24 years), and this is in agreement with the relatively rare incidence reported in the literature (11). Our data show higher rates of gross ETE at presentation in PDTC (30%) than is reported for DTC, 4% (12) to 11% (13), and this supports the finding that PDTC presents with higher rates of local invasion than DTC.
The most common central compartment structures invaded in our PDTC (MSKCC) patients were similar to those reported for DTC with gross ETE. Upper respiratory tract invasion occurred in 67% of our cohort compared with 49% (9) and 82% (14) in reports on DTC. However, there was a higher frequency of recurrent laryngeal nerve involvement with 63% of our patients compared with 47% (9) and 32.6% (15) reported for DTC. In addition, there was significantly higher esophageal invasion, with 56% of our patients having invasion compared with 21% (9) and 8.6% (15) in DTC. The tendency of PDTC in our MSKCC cohort to invade more posteriorly located structures (esophagus, trachea or larynx, and recurrent nerve) compared with DTC can be explained by the more aggressive local behavior of PDTC but also by the fact that over half of patients presented with a primary tumor larger than 4 cm in size.
The majority of our patients had extended thyroidectomy with resection of involved structures. Two patients underwent subtotal thyroidectomy, in one case to preserve a functioning contralateral recurrent laryngeal nerve due to sacrifice of the ipsilateral nerve during tumor removal, and in the second case a small portion of the contralateral lobe was left at the discretion of the operating surgeon. Removal of extrathyroid disease included organ preservation in the majority of cases: either by shaving the tumor off the trachea, larynx, or both (73% of patients with laryngotracheal invasion) or by submucosal esophagectomy (93% of patients with esophageal invasion). Partial thickness esophagectomy preserving mucosal continuity is oncologically safe in the absence of direct invasion of the mucosa because locally invading thyroid cancer is usually confined to the muscularis layer without extension into the submucosa and mucosa (16). This high rate of surgical gross disease clearance in 74% of our patients is higher than the 56% previously reported by other investigators for locally invasive DTC (9).
However, it should be noted that all 27 patients were considered operable, and patients with T4b tumors (unresectable disease) were excluded from our analysis. In the study on papillary thyroid cancer with local invasion reported by McCaffrey et al. (9), 30% of the patients had invasion of the jugular vein, carotid artery, or prevertebral fascia, with the latter two designating T4b unresectable disease. Therefore a comparison of our clearance rate with reported rates in the literature has to be interpreted with caution.
Although we had a high rate of gross disease removal, the margins of surgical resection were reported histologically close or positive in 89% of our patients. Due to the large number of patients with positive margins, the majority of our patients (77%) received postoperative adjuvant therapy (RAI, EBRT, or both). The decision for adjuvant treatment was determined by the treating physician and an individual risk estimation of the extent of gross or microscopic residual disease. However, it was also based on patient compliance, particularly in the case of EBRT. In our analysis, we did not find a statistically significant association between EBRT and locoregional recurrence. However, the patient numbers were small and therefore no conclusions can be drawn with regards to the benefits of EBRT. In general, due to the reduced morbidity associated with radiotherapy given by intensity-modulated radiation therapy, EBRT is now currently recommended more frequently and is better tolerated.
Based on the aggressive surgical approach, the 5-year locoregional control in our patients was satisfactory at 56%. The 5-year local and regional control rates (70% and 62%, respectively) were inferior to local (92%) and regional (72%) control rates reported for DTC patients with ETE (17). Despite locoregional recurrence in our patients, the reason for death was usually distant metastatic disease rather than uncontrolled central compartment disease. Only three patients died as a result of airway involvement from locoregional recurrence.
The M1 rates in our cohort (37%) were similar to M1 rates reported by other investigators in PDTC where the majority of patients presented with gross ETE (T4) (18). However, the incidence of subsequent distant metastases was lower in our cohort, 22% vs. 50% (18). In contrast, our M1 rates were higher than those reported for DTC with ETE, 37% vs. 9% (19), as were the rates of subsequent distant metastases, 22% vs. 6% (12). This indicates that distant metastatic disease is more frequent for patients with PDTC compared with DTC (4). The majority of our patients who presented with M1 disease (7 of 10, 70%) had RAI-avid disease. This is comparable to 67% RAI-avid M1 disease in DTC (20). However, it should be noted that DTC is often a much more RAI-avid disease than PDTC, and is identified both on the diagnostic and posttherapy scans. In contrast, PDTC usually shows uptake only after a large therapeutic dose. PDTC is therefore technically RAI avid but probably below the therapeutic threshold. Although patients with RAI-avid metastases have better prognosis in DTC (21), and RAI avidity of M1 disease has a significant impact on DSS (22), it was not possible to assess the significance of RAI avidity and outcome in PDTC due to the small number of patients.
Five-year OS rates for other reports of PDTC with ETE are similar to our cohort, 47% vs. 55% (23). In contrast, survival rates reported for DTC with gross ETE are higher than in our cohort of patients with PDTC (MSKCC), 5-year OS of 79% (9) and 10-year DSS of 90.6% (10). This is due to the more aggressive biology of PDTC, with a higher incidence of distant metastatic disease compared with DTC. The cause of death in the majority of our patients was distant metastatic disease rather than uncontrolled locoregional disease. Of 14 patients (52%) who died, 11 patients died of distant disease alone, and three died of locoregional disease with distant disease also being present. In recent reports on PDTC, almost all deaths from PDTC (with 63% of patients having ETE) were caused by distant disease (50% due to distant disease, and 50% due to both local and distant disease) (18). In concordance with these results, distant disease was the only significant predictor for survival on multivariate analysis in PDTC (24).
Despite this high incidence of distant metastases, gross disease clearance in the thyroid and central compartment is still justified in these patients because it prevents death by local invasion of central compartment structures and asphyxiation. By lowering the rate of locoregional failure as a cause of death, treatment of distant disease becomes the main issue in thyroid cancer patients. Since PDTC, as it is currently defined, is a new entity, there are no standard treatments available for treating distant metastatic disease. Metastatic lesions in PDTC often do not respond to RAI due to the loss of differentiation. Metastasectomy is also rarely done in the case of PDTC. Therefore, the development of new molecular targeted therapies for PDTC is important. Most clinical trials in thyroid cancer have focused on multitargeted kinase inhibitors, which often simultaneously inhibit angiogenic targets as well as targets in the MAPK pathway (25). Furthermore, there is a potential for antiangiogenic agents to increase the efficacy of conventional therapies (chemotherapy, radiotherapy, or RAI treatment) (26). Results from clinical trials on modulators of growth, apoptosis, or other novel targets are currently pending. However, no novel treatment has yet shown improved survival for thyroid cancer patients (25). Therefore, further studies are necessary to develop targeted therapy that would result in complete response and minimal toxicity in progressive metastatic thyroid cancer, which is in most cases poorly differentiated and nonresponsive to traditional therapy.
In conclusion, we report that up to 30% of patients with PDTC (MSKCC) present with locally advanced disease with gross ETE. In these patients, up to 37% already present with distant metastases and overall over 50% will develop distant metastases. Despite this, aggressive surgical resection removing all gross locoregional disease supplemented with adjuvant therapy can produce excellent control of the disease in the neck. As a consequence, survival rates (OS and DSS) of our patients are still acceptable (47% and 49%, respectively) although poorer than those reported for DTC with gross ETE. Our study shows that while satisfactory locoregional control is achieved, the main cause of disease related death in PDTC with ETE is distant disease. Therefore, further development of novel therapies to optimally target progressive metastatic disease unresponsive to traditional modes of treatment is necessary to improve survival outcomes in this group of patients.
Footnotes
Disclosure Statement
Authors have nothing to disclose.