
Abstract
Background:
The presence of microcalcification is highly suggestive of malignancy; however, the association of macrocalcification with cancer remains unclear and controversial. The purpose of this study was to evaluate the diagnostic yield and accuracy of ultrasound (US)-guided fine-needle aspiration (FNA) of thyroid nodules with macrocalcifications and to investigate the association between macrocalcification subtype and malignancy risk.
Methods:
We retrospectively reviewed sonographic findings and pathologic results of thyroid nodules with macrocalcification in patients who underwent US-guided FNA in our hospital from January 2009 through December 2010. Inclusion criteria were as follows: (i) malignant or benign nodules confirmed on histologic examination of surgical specimens after US-guided FNA and (ii) nodules not histologically confirmed that were subjected to FNA at least twice and follow-up US examinations for 2 years. Thyroid nodules with macrocalcification were classified into four groups: smooth total (eggshell) calcification, smooth partial calcification, irregular calcification, and nodular calcification. The diagnostic yield of FNA for thyroid nodules with macrocalcification was determined by cytology. Sensitivity, specificity, and diagnostic accuracy of preoperative FNA cytology were calculated and compared with those of histologic examination of surgical specimens.
Results:
There were 188 nodules with macrocalcification in 167 patients; of these, 95 were benign, 80 were malignant, and 13 were nondiagnostic. The diagnostic yield of FNA for thyroid nodules with macrocalcification was 93.08%. Sensitivity, specificity, positive predictive value, and negative predictive value were 98.51%, 90.91%, 95.65%, and 96.77%, respectively. The false-positive value and false-negative value were 9.09% and 1.49%, respectively. The diagnostic accuracy was 96%. There was no statistically significant difference in the association between macrocalcification subtype and malignancy risk (p>0.05).
Conclusions:
Macrocalcification associated with thyroid nodules is not a reliable criterion for malignancy. FNA of thyroid nodules with macrocalcification had a high diagnostic yield and a reliable accuracy. Consistency between cytology and histology was almost perfect. Therefore, FNA is a good screening method for malignancy of thyroid nodules with macrocalcification.
Introduction
Fine-needle aspiration (FNA) is the most accurate, cost-effective, and simplest screening test for diagnosis of thyroid nodules. The routine use of FNA has reduced the rate of unnecessary surgery for thyroid nodules and has doubled the percentage of cancers detected in surgically resected material (14,15). However, FNA has been reported to have a false-negative rate of 11%–25% and unsatisfactory or nondiagnostic results of 5%–30% (5,16,17). Furthermore, the role of FNA in thyroid lesions with macrocalcifications is controversial (18) because calcified lesions are a common cause of nondiagnostic sampling.
The purpose of this study was to evaluate the diagnostic yield and accuracy of ultrasound (US)-guided FNA of thyroid nodules with macrocalcifications and to investigate the association between macrocalcification subtype and malignancy.
Materials and Methods
This study was approved by the Institutional Review Board and, being retrospective, informed consent was not required.
We retrospectively evaluated US findings of 1637 patients who underwent FNA of a thyroid nodule between January 2009 and December 2010. Macrocalcifications were present in 167 patients with 188 nodules (Fig. 1).
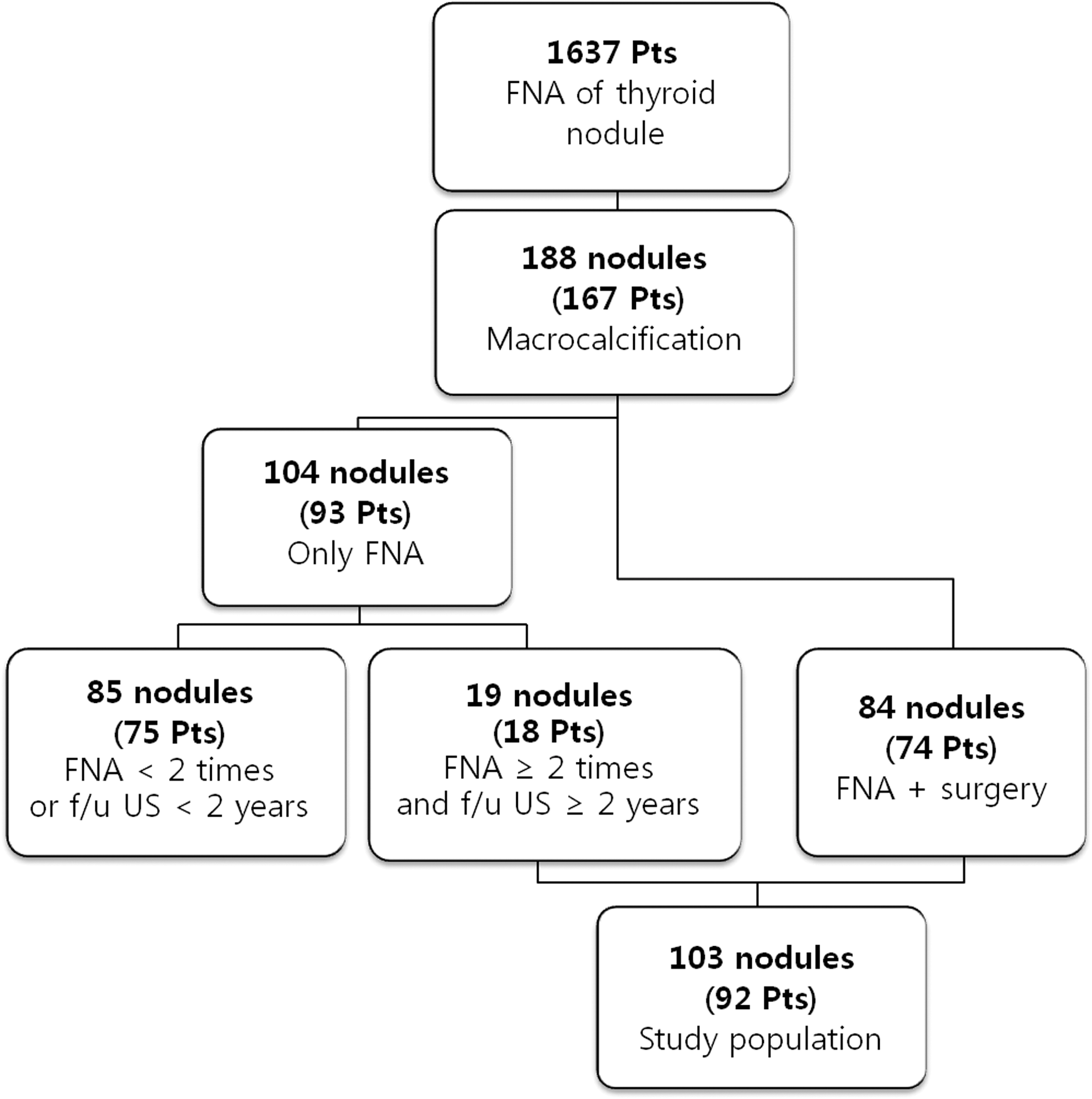
Flow chart of the study group. FNA, fine-needle aspiration; f/u, follow-up; Pts, patients; US, ultrasound.
Inclusion criteria were as follows: (i) malignant or benign nodules confirmed on histologic examination of surgical specimens after US-guided FNA and (ii) nodules not histologically confirmed that underwent FNA at least twice and follow-up US examinations for 2 years. We excluded 75 patients with 85 nodules because of loss to follow-up or an insufficient follow-up period. Finally, we included a total of 92 patients (63 women and 29 men) with 103 nodules and a mean age of 53.5 years. When evaluating the surgically resected specimen, only the target nodule was considered and correlated with the preceding FNA findings.
Sonographic evaluation and US-guided FNA were performed using an IU22 (Philips Medical Systems, Bothell, WA) or Acuson Sequoia 512 (Siemens Medical Solutions, Mountain View, CA) with a 5–12 MHz linear array transducer. FNA was performed by a faculty radiologist with over 8 years' experience in thyroid imaging, who supervises radiology residents in their second to fourth year of training. The sonographic findings of macrocalcified nodules were retrospectively reviewed by two radiologists blinded to the final pathologic diagnosis. FNA was performed by using the perpendicular method with a 21-gauge needle attached to a 10 mL syringe. Each nodule was aspirated at least twice.
The criteria in this study included macrocalcifications with a diameter of ≥3 mm. The macrocalcifications patterns were classified into four subtypes (Fig. 2): pattern 1, smooth total (eggshell) calcification (curvilinear hyperechoic structure parallel to the margin of the nodule that encompassed three quarters or more of the circumference); pattern 2, smooth partial calcification (curvilinear hyperechoic structure parallel to the margin of the nodule that encompassed less than three quarters of the circumference); pattern 3, irregular calcification (solitary linear or round hyperechoic structure with micro- or macrolobulation); and pattern 4, nodular calcification (solitary linear or round hyperechoic structure in the middle of the nodule surrounded by at least 1 mm of nodular tissue).
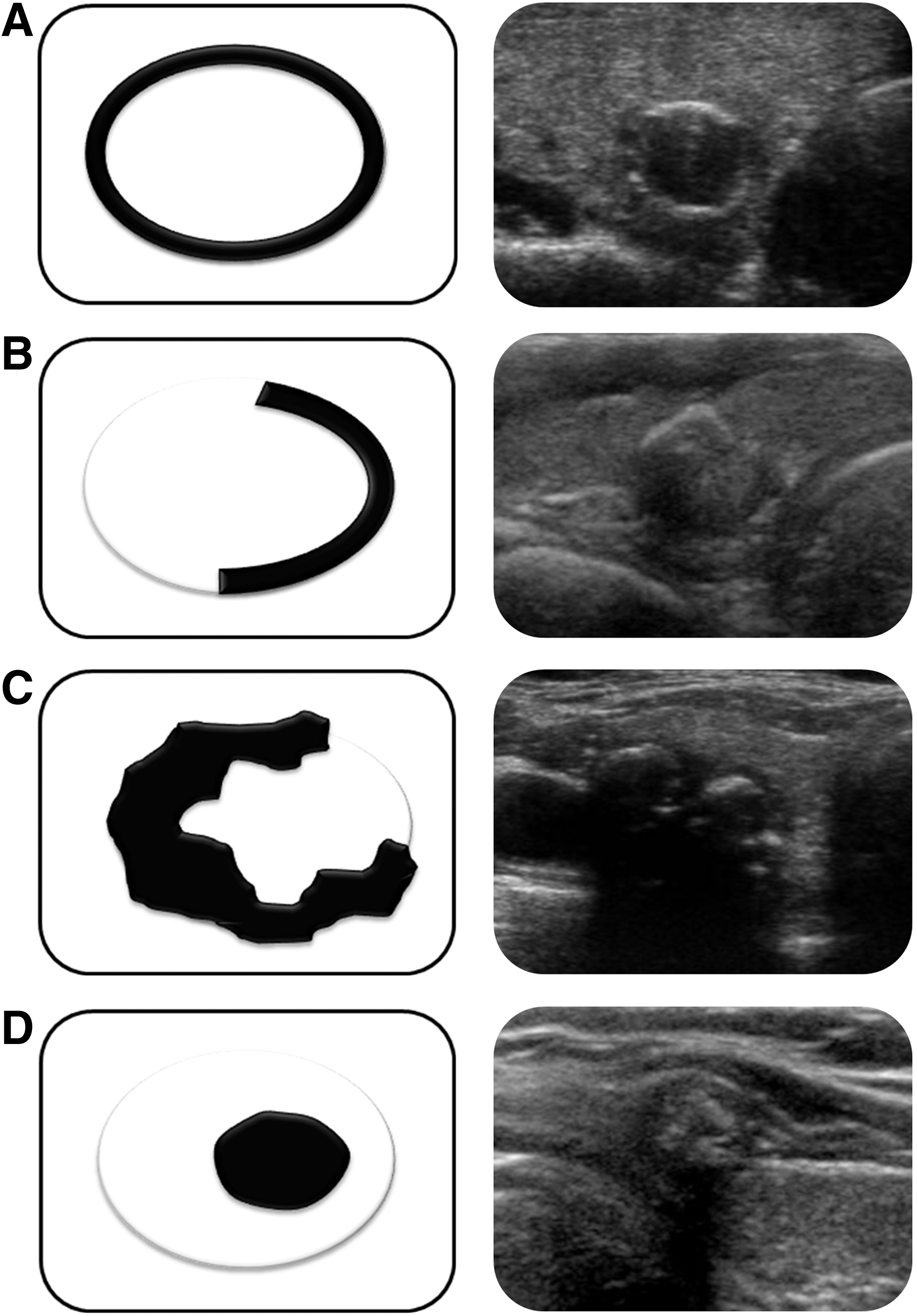
Schematics of macrocalcification according to four subtypes.
The terminology and reporting of thyroid FNA results have been reported by the Bethesda System for Reporting Thyroid Cytopathology (19). The six diagnostic categories proposed by the Bethesda system are (i) nondiagnostic or unsatisfactory, (ii) benign, (iii) atypia of undetermined significance or follicular lesion of undetermined significance, (iv) follicular neoplasm or suspicious for a follicular neoplasm, (v) suspicious for malignancy, and (vi) malignant. Repeated aspiration was performed for nondiagnostic or unsatisfactory nodules and nodules with atypia of undetermined significance or follicular lesion of undetermined significance. Some nodules with repeated FNA that yielded a recurrent finding of atypia of undetermined significance were referred for surgery because of concerning clinical and/or sonographic features.
We regarded the nodules with a benign cytology on FNA that did not undergo histologic examination of surgical specimens, but showed the same benign results on repeated FNA and no changes on US for 2 years, as clinically benign nodules. The patients with a benign cytologic diagnosis that had a surgical specimen with a benign diagnosis, or were clinically benign nodules, were considered true negative cases. The cases with a cytologic diagnosis of malignant, suspicious for malignancy, follicular neoplasm or suspicious for a follicular neoplasm, or repeated atypia of undetermined significance on FNA that were diagnosed as malignant on histologic examination of a surgical specimen, were considered true positives. The false-positive category comprised the cases with a benign histology and a cytologic diagnosis of malignant, suspicious for malignancy, follicular neoplasm or suspicious for a follicular neoplasm, or repeated atypia of undetermined significance. A false-negative diagnosis encompassed the cases with a malignant histology that had been diagnosed as benign on cytology. The cases with a cytologic diagnosis of follicular lesion of undetermined significance and a benign or malignant final histologic diagnosis of the surgical specimen were considered true positive because of the diagnostic limitations of FNA for the differential diagnosis between follicular adenoma and carcinoma of the thyroid gland (20) (Fig. 3).
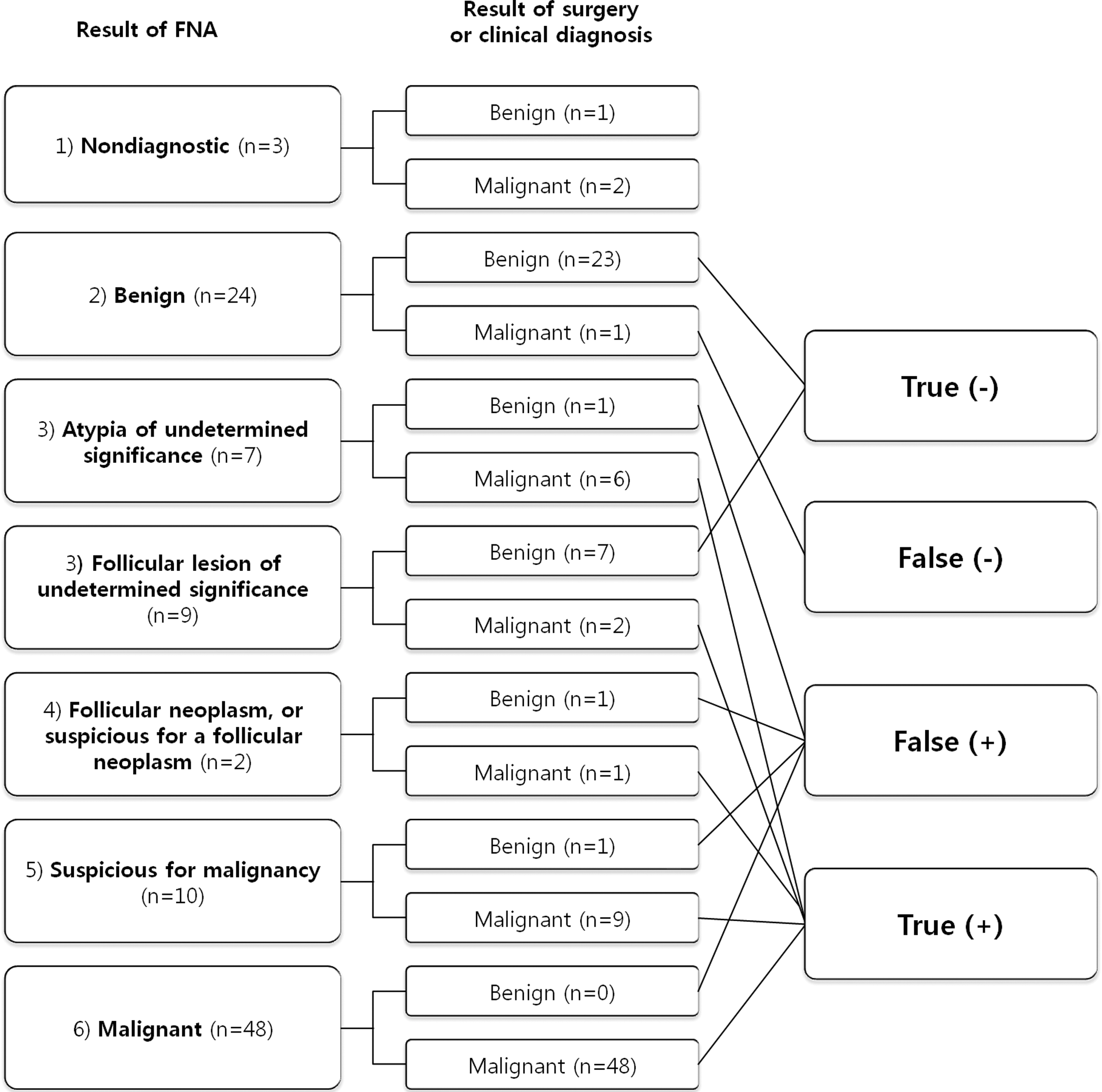
Flow chart of diagnosis. n, number of nodules; (−), negative; (+), positive.
Diagnostic yield, sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of FNA compared with final histologic outcome were calculated.
Statistical analyses were conducted using the kappa value (0.81–0.99, almost perfect agreement; 0.61–0.80, substantial agreement; 0.41–0.60, moderate agreement; 0.21–0.40, fair agreement; 0.20 or less, slight agreement) for consistency of the FNA and histologic results, the t test for analysis of the association between macrocalcification subtype and malignancy, and the chi-square test for cross-tabulation; p<0.05 was considered statistically significant. Statistical analyses were performed with SPSS version 18.0 (SPSS, Inc., Chicago, IL, USA) for Windows.
Results
There were 167 patients (132 women and 35 men) who showed 188 nodules with macrocalcifications and underwent FNA. The age of the patients ranged from 22 to 77 years (mean, 53.9 years) and the size of the nodules ranged from 3 to 26 mm (mean, 7.6 mm). Ninety-five (50.53%) nodules were benign, 80 (42.55%) were malignant, and 13 (6.92%) were nondiagnostic. The diagnostic yield of FNA of thyroid nodules with macrocalcification was 93.08%.
Eighty-five nodules were excluded for the following reasons: not histologically confirmed, loss to follow-up, or an insufficient follow-up period. Finally, the population of our study included 92 patients with 103 nodules. Eighty-four nodules were histologically confirmed after FNA. Nineteen benign nodules were not histologically confirmed after FNA, but underwent FNA at least twice and US follow-up examinations for 2 years; these nodules showed the same benign results on repeated FNA and no change of US findings during 2 years and were therefore considered clinically benign nodules. There were 69 malignant nodules (69.99%) and 34 benign nodules (33.01%; Table 1). Malignant thyroid nodules included papillary carcinomas in 66 nodules (64.08%) and follicular carcinomas in three (2.91%). Benign thyroid nodules included nodular hyperplasia in 29 nodules (28.15%) and follicular adenomas in five (4.86%). Surgery was performed in patients with nodules identified as benign or nondiagnostic on FNA if there was another accompanying malignant nodule or follicular neoplasm.
One hundred three nodules in 92 patients met the inclusion criteria as follows: (i) malignant or benign nodules confirmed on histologic examination of surgical specimens after US-guided FNA and (ii) nodules not histologically confirmed that underwent FNA at least twice and US follow-up examinations for 2 years. Eighty-four nodules were histologically confirmed after FNA. Nineteen benign nodules were not histologically confirmed after FNA but underwent FNA at least twice and US follow-up examinations for 2 years; these nodules showed the same benign results at repeated FNA and no change of US findings during 2 years, so were considered clinically benign nodules.
The sensitivity and specificity values were 98.51% and 90.91%, respectively. The positive predictive value and the negative predictive value were 95.65% and 96.77%, respectively, with an accuracy of 96%. The false-positive value and false-negative value were 9.09% and 1.49%, respectively (Table 2). Three nondiagnostic nodules on FNA were excluded for evaluation of diagnostic accuracy of FNA by comparison with the results of histologic examination and clinical diagnosis.
There were 19 nodules (18.45%) with pattern 1, 21 (20.39%) with pattern 2, 35 (33.98%) with pattern 3, and 28 (27.18%) with pattern 4 (Table 3). Pattern 3 had the largest number of nodules with macrocalcifications and also the largest number of malignant thyroid lesions. However, this was not statistically significant (p>0.05). Two nodules out of three follicular carcinomas had a pattern 1 and the other one had a pattern 2. For FNA and histologic examination, most patterns had a kappa value over 0.8, which indicates an almost perfect agreement. Pattern 3 had a kappa value of 0.5, but this was still consistent with a moderate agreement.
Data are presented as number (percent) of nodules.
There was no statistical difference between the benign and malignant nodules with regard to nodule size and patient age (p>0.05). The results of cross-tabulation between age, sex, size of calcification, pathologic result, and pattern of calcification were not statistically significant.
Discussion
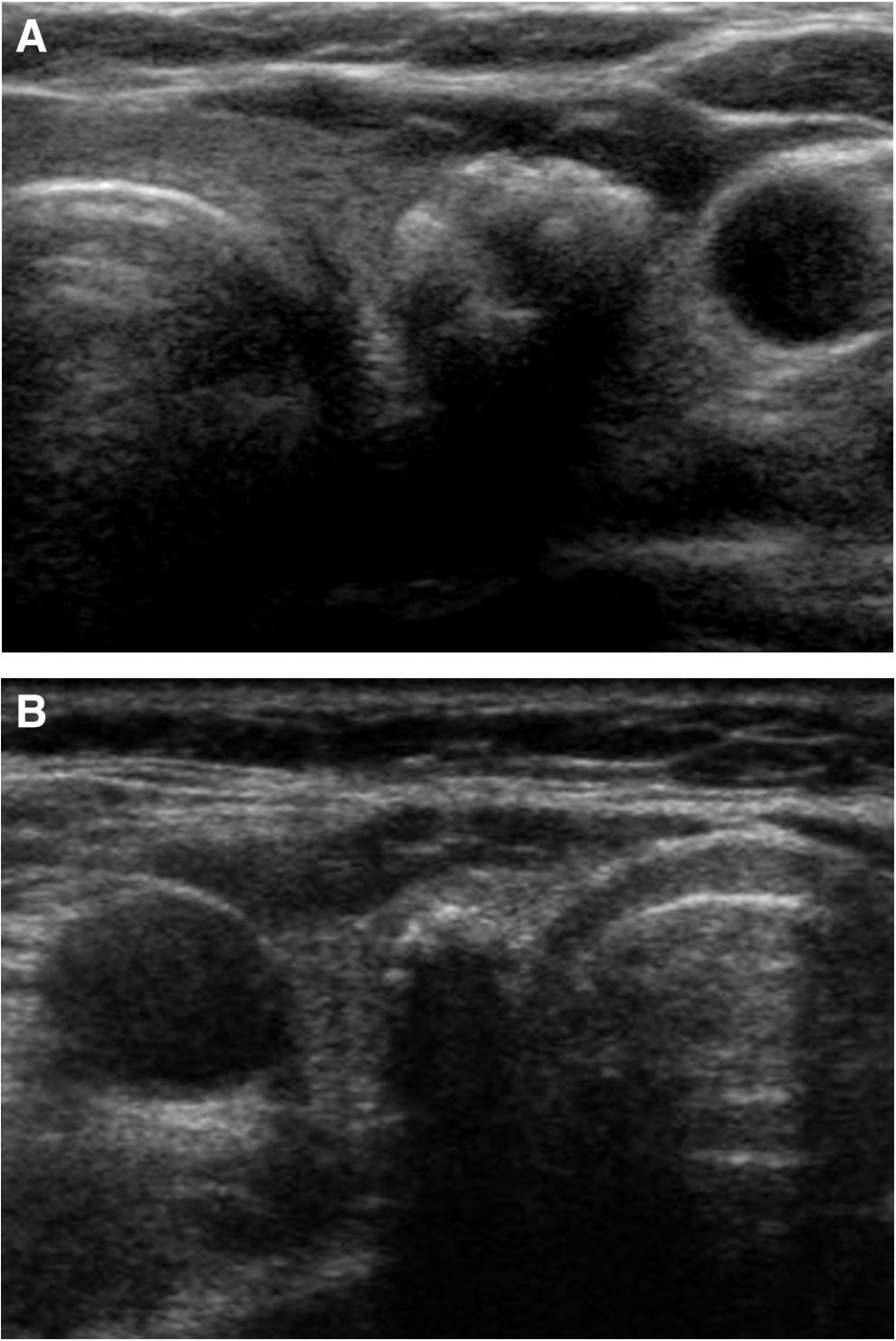
Thyroid calcifications may occur in both benign and malignant thyroid disease. Microcalcifications have a well-known association with thyroid malignancy (13,21,22). Although several reports have refocused the attention on thyroid macrocalcifications (3 –8), the results regarding macrocalcifications are controversial. Recent studies reported that macrocalcifications are also associated with malignancy, primarily papillary thyroid carcinoma (8 –12) (Fig. 4). A peripheral or eggshell calcification within a thyroid nodule was thought to be an indicator of benignity, with few exceptions (23). However, Taki et al. (7) reported six cases (43%) of malignancy in 14 cases of histologically proven thyroid nodules with eggshell calcifications. According to Kim et al. (10), among 93 histologically proven thyroid nodules with eggshell calcification, 59 (63.4%) were malignant, and 34 (36.6%) were benign. Ten (53%) out of 19 thyroid nodules with eggshell calcification were malignant in our study, in agreement with other recent studies (Fig. 5). Therefore, macrocalcifications should not exclude a nodule from further investigation. This was acknowledged by the latest American Thyroid Association guidelines, with the recommendation that all cases of nodular calcification be assessed for malignancy (9).

Transverse US image of a hypoechoic nodule with nodular calcification (pattern 4). The results of FNA and histologic examination were papillary carcinoma.
Transverse US image of a hypoechoic nodule with smooth calcification (pattern 1). The result of FNA was atypical follicular cells suggestive of follicular neoplasm, and the result of histologic examination was minimally invasive follicular carcinoma.
Malignancies associated with eggshell calcifications have mostly been diagnosed as papillary carcinomas or anaplastic carcinomas (7,10,11,24), and only four cases of follicular carcinomas with eggshell calcification have been reported (25,26). In our study, two nodules out of three follicular carcinomas showed eggshell calcification (pattern 1) and the other showed a partial peripheral calcification (pattern 2) (Fig. 5). Follicular carcinomas should be included in the differential diagnosis of a thyroid nodule with eggshell calcification (25), but further studies with a larger sample size are warranted.
Several diagnostic tests, such as radionuclide scanning, high-resolution US, FNA, and core-biopsy, have been used to select the patient population requiring surgical intervention. Recent studies have shown that among all these diagnostic modalities, FNA is the most accurate, cost-effective, and simplest screening test for the rapid characterization of thyroid nodules. The routine use of FNA has reduced the rate of unnecessary surgery for thyroid nodules and has doubled the percentage of cancers found in the surgical material (14,27,28).
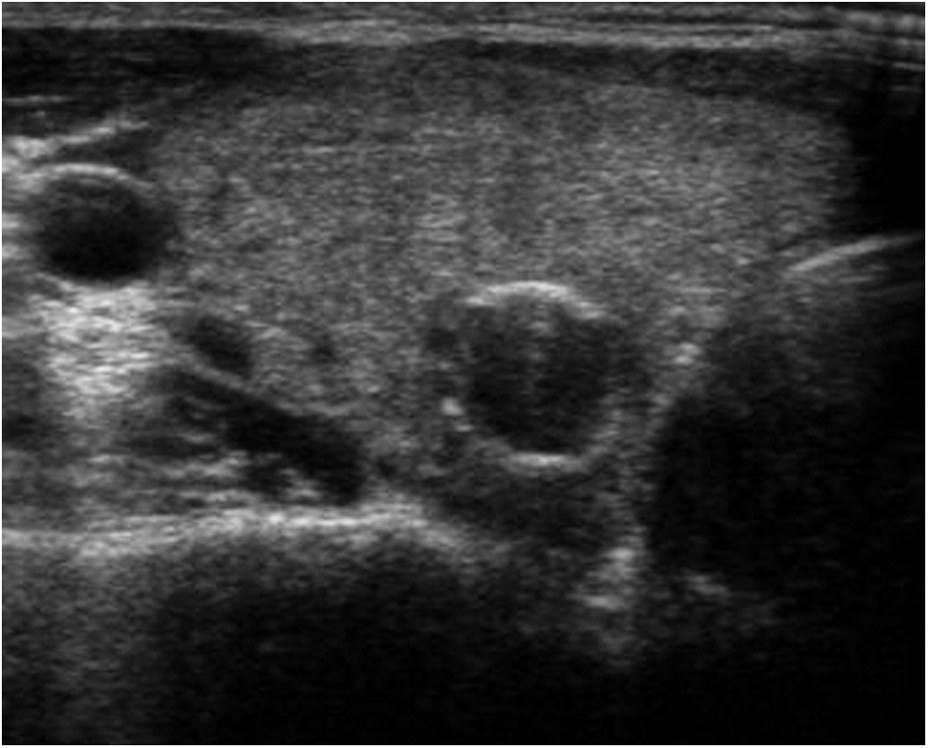
However, it has been reported that FNA has a false-negative rate of 11%–25% and FNA results may be insufficient or nondiagnostic in up to 20% of patients (5,16,17,29). One of the common causes of nondiagnostic sampling is calcified lesions. In addition, Khoo et al. (5) reported that 24.1% of thyroid malignancies with calcifications in their study population had benign preoperative FNA results. In our study, 13 (6.92%) of 188 nodules that were subjected to FNA were nondiagnostic and 10 (76.92%) nodules with pattern 3 were nondiagnostic. Furthermore, there was one false-negative diagnosis with pattern 3 (irregular calcification; Fig. 6). The irregular calcification in pattern 3 tends to be harder and is associated with a lack of parenchyma; this might explain the nondiagnostic or false-negative diagnoses in this pattern.
Transverse US image of thyroid nodule with irregular calcification (pattern 3).
During the FNA procedure, the needle may be introduced parallel or perpendicular to the transducer according to the preference of the examiner (30). We performed FNA by using the perpendicular method. By insertion of the needle in a plane perpendicular to that of the scanner, the distance from the skin entry site through the tissues of the neck and into the nodule is shorter than that of the parallel approach. We considered that the structures posterior to the thyroid gland such as the vertebral bodies and paraspinal muscles could provide support to aid penetration of the calcified wall in the perpendicular approach. In contrast, in the parallel approach, the trachea is located medial of the calcified nodule, is movable, and cannot play a role in providing support. In pattern 4 (nodular calcification), the nodular tissue surrounding the calcification is the target for FNA. Using the perpendicular approach, the needle tip, the peripheral noncalcified portion, the intratumoral calcified portion, and the vertebral body are located in a straight line. Therefore, detecting the resistance of the calcified wall facilitates the FNA and makes it more accurate. Thus, the perpendicular approach in FNA of thyroid nodules with macrocalcifications might have contributed to the higher rate of diagnostic yield in our study than in previous reports. However, we did not assess the statistical data to support this result; further prospective studies are warranted.
Bright stippled hyperechogenic dots of calcification, with or without shadow, and sized 2 mm (sometimes 1 mm) or less have been considered as microcalcifications, and macrocalcification has been defined as all calcifications that are not microcalcifications (4,16,31). In contrast to authors who choose a cut-off diameter of either 2 or 1 mm, we selected a cut-off diameter of 3 mm as the criterion for macrocalcifications in order to clearly distinguish between micro- and macrocalcifications and as a practicable minimal size for FNA.
The terminology and reporting of thyroid FNA results have been summarized in the Bethesda System for Reporting Thyroid Cytopathology (19). This classification scheme has achieved its purpose of standardization of thyroid-reporting cytopathology, as evidenced by several publications (32). The results of a recent study also showed a high overall accuracy, indicating that The Bethesda System for Reporting Thyroid Cytopathology represents a reliable and valid reporting system for thyroid cytology (33).
Our study has limitations owing to its retrospective design. First, there is the possibility of an unavoidable selection bias because of the criteria used to select our study population. Second, patients with obviously benign results on FNA did not undergo surgery, which might have resulted in relatively fewer benign nodules in our study. Third, because of the small sample size, evaluation of the association between macrocalcification subtype and malignancy is not statistically significant. Further large-scale prospective studies are needed to overcome these limitations.
In conclusion, a thyroid nodule with macrocalcifications is not a reliable criterion for malignancy. FNA of thyroid nodules with macrocalcifications has a high diagnostic yield and a reliable accuracy, and consistency between cytology and surgery was almost perfect. Therefore, FNA is a good screening method to identify malignancy of thyroid nodules with macrocalcifications.
Footnotes
Disclosure Statement
No competing financial interests exist.