
Abstract
Background:
Accurate assessment of thyroid status during pregnancy is vital for maternal and fetal health. Because free thyroxine (FT4) values in pregnancy vary widely between methods, assessment of total T4 (TT4) and FT4 index (FT4I) may be superior to FT4 in pregnant women. However, trimester-specific reference intervals for FT4I have not yet been established. In this longitudinal self-sequential survey, we aimed at determining the trimester-specific reference range for FT4I in healthy Iranian women with singleton pregnancies.
Methods:
A total of 466 healthy pregnant women were evaluated. After exclusion of women with history, ultrasonographic, or laboratory evidence of any thyroid disorder or iodine deficiency and those who were positive for thyroid autoantibodies, 152 women entered the study. Serum thyrotropin (TSH), TT4, and triiodothyronine-resine uptake were measured by an immunoassay method. Reference intervals were defined as 5th and 95th percentiles, using the bootstrap-based procedure.
Results:
Mean values in the first, second, and third trimesters were 1.7±1.5, 1.9±1.8, and 1.9±1.8 mIU/L for TSH; 12.9±3, 14.4±3.1, and 13.6±3.3 μg/dL for TT4; and 12.8±3.5, 14.2±3.3, and 13.5±3.8 for FT4I, respectively. Reference intervals in the first, second, and third trimesters were as follows (respectively): TSH—0.2–3.9, 0.5–4.1, and 0.6–4.1 mIU/L; TT4—8.2–18.5, 10.1–20.6, and 9–19.4 μg/dL; and FT4I—8.5–19, 9.7–21, and 8.7–20.4. Serum TSH had no significant correlation with TT4. Serum TSH had a significant but weak correlation with FT4I only in the first trimester (r=−0.24, p=0.006).
Conclusion:
This study, for the first time, establishes the trimester-specific reference intervals for FT4I in a reference population of normal iodine-sufficient pregnant Iranian women.
Introduction
The vast physiological changes in maternal hormones and binding proteins during pregnancy complicate the assessment of normal levels of most hormones (7) and necessitate the establishment of gestation-specific reference intervals. The thyroid stimulatory effect of beta human chorionic gonadotropin (β-hCG) increases thyroid hormone production and inhibits thyrotropin (TSH) secretion through a negative feedback mechanism. On the other hand, higher T4 binding globulin (TBG) concentrations as a result of an estrogen-induced increase in its synthesis and a reduced renal clearance will result in higher total T4 (TT4) and transiently lower free T4 (FT4) values during pregnancy (7).
Despite the recent developments in sensitive biochemical assays, and rapid advances in understanding gestation-dependent trends of these hormones, clinically useful gestation-specific reference ranges are rarely available (8 –10). The available results are inconsistent and should not be generalized because of differences in ethnicity, maternal iodine status, laboratory assay methods, and variable rigor for the selection of the reference population and sample size, among others (11,12). Most data are derived from cross-sectional studies on different women from different gestations, instead of longitudinal self-sequential surveys (13).
Many studies focused on employing first TSH and then FT4 (14 –18) as main primary tests for evaluation of the thyroid function during the gestational period; however, increased TBG and decreased serum albumin induced by gestation can influence FT4 immunoassay results in a method-specific manner. Due to existing debates regarding the accuracy and reliability of most FT4 immunoassay results during pregnancy, traditional approaches for FT4 estimation [TT4 and FT4 index (FT4I)] may be superior to FT4 measurement by immunoassay in order to assess thyroid status during pregnancy. FT4I alterations during pregnancy have been shown to be consistent with the expected effect caused by TBG and hCG. However, trimester-specific reference intervals for FT4I have not yet been established in a reference pregnant population.
We carried out a self-sequential longitudinal study to investigate trimester-specific reference values for FT4I. We also assessed trimester-specific reference values of TSH and TT4 in normal pregnant women from Tehran, an iodine-sufficient area of Iran.
Materials and Methods
Study population
A total of 466 pregnant women in the first trimester of pregnancy attending antenatal care clinics in the mother and child health care centers of two general hospitals of Tehran were consecutively recruited from November 2004 to November 2006. Only women with singleton pregnancies were enrolled. Inclusion criteria required documentation that thyroid-related measurements were available in all three trimesters. Of these 466 women, 147 subjects were ultimately excluded for the following reasons: they self-reported preexisting thyroid disorders, they were taking medications affecting thyroid function, or they were not available in all trimesters or lost to follow-up (referring elsewhere for delivery or nonviable pregnancy). The study cohort then consisted of 219 healthy pregnant women. A further 98 women were excluded on the basis of laboratory results of overt hypothyroidism (TSH >4.5 mIU/L and T4 <5.5 μg/dL) or hyperthyroidism (TSH <0.1 mIU/L and T4 >14.5 μg/dL), or a TSH >10 mIU/L (for subclinical hypothyroidism), positive serum thyroid peroxidase and thyroglobulin antibodies (TPOAb >40 IU/mL and TgAb >100 IU/mL, respectively), low urinary iodine level (<150 μg/dL in two out of three measurements in the first trimester), and a hypoechoic or enlarged thyroid gland (thyroid volume >30 mL) by ultrasonography. Those with subclinical hyperthyroidism (serum TSH levels <0.1 mIU/L) were not excluded due to the physiological TSH suppression during pregnancy. Finally, 152 healthy iodine-sufficient women with viable, singleton pregnancy comprised the cohort study.
Methods
Trained midwives informed the participants about the rationale of the study and asked them to give supplementary written consent to allow for laboratory measurements and thyroid ultrasonography. The obstetric history was taken using a standard questionnaire and physical examination was performed. Gestational age was calculated from the first day of the last normal menstrual period and gestational age <15, 15–28.9, and >29 weeks comprised the first, second, and third trimesters of pregnancy. Serum samples were taken in the first, second, and third trimesters for assessment of TSH, TT4, TPOAb, and TgAb. At initial presentation, before the end of the first trimester, three separate urine samples, and in each of the second and third trimesters one urine sample was obtained for measurement of urinary iodine concentration (UIC). The thyroid volume of pregnant women was also measured using ultrasound (Portable 7.5 MHz, SSD 2100 DXΠ Aloka, Japan) in all trimesters. The volume of each lobe was calculated by the formula: V (mL)=0.000479×length×width×depth (mm3).
Laboratory measurements
The UIC was measured in random urine samples using a manual method based on the Sandell–Kolthoff technique (19). Measurement of TT4 was done by a radioimmunoassay method and TSH was measured by an immunoenzymometric assay using commercial kits (Izotop, Budapest, Hungary) and a gamma counter (Wallac Wizard; Wallac Oy, Turku, Finland). Intra- and interassay coefficients of variation were 3.3% and 6.2% for TT4 and 3.9% and 7.1% for TSH, respectively.
Statistical analysis
Since serum TSH had a non-Gaussian distribution, log-transformed values were used for TSH. The reference interval of each hormone in each trimester was determined by calculating the 5th and 95th percentiles (i.e., a central 90% interval) using the bootstrap technique. Repeated measures were employed to compare differences in thyroid hormones among groups with different gestational ages. Pearson correlation was applied to evaluate the correlation of log-transformed TSH values with FT4I and TT4. p-Values <0.05 were considered statistically significant.
Results
The mean age of the study population was 25.3±5 years (range 18–45). Mean±standard deviation of gestational age during the study visits at the first, second, and third trimesters was 12.2±3.7, 23.8±1.8, and 35.7±1.5 weeks, respectively. Among 216 pregnant women, 30 (13.9%) were TPOAb positive, 42 (19.4%) were TgAb positive, and 17 (7.9%) were positive for both TPOAb and TgAb. The mean thyroid volume in the first, second, and third trimesters was 9.05±4.1, 10.15±4.3, and 10.9±5.1 mL, respectively. Table 1 shows trimester-specific percentiles for FT4I, TSH, and TT4, based on the data of this study.
TSH, thyrotropin; TT4, total thyroxine; FT4I, free thyroxine index.
The percentiles and average values of FT4I increased markedly after the first trimester, reached a peak in the second trimester (p<0.001), and fell in the third trimester. Significant differences were observed in FT4 average values among trimesters (p<0.001).
TSH mean values rose significantly in the second trimester (p=0.007) followed by a nonsignificant decrease in the third trimester (p=0.8). The TSH reference intervals showed that a lower TSH reference limit of 0.2 mIU/L occurred in the first trimester in comparison with the second and third trimesters of 0.5 and 0.6 mIU/L, respectively. The upper reference limit of TSH of 3.9 mIU/L in the first trimester increased to 4.1 mIU/L in the second trimester, but remained unchanged in the last trimester. A significant difference was observed in mean values of TSH among trimesters (p=0.008).
Figure 1 depicts the trends of the reference intervals during the three trimesters for TSH, TT4, and FT4I. The percentiles and average values of TT4 increased markedly after the first trimester, reached a peak in the second trimester (p<0.001), and fell in the third trimester (p=0.01) (Table 1). Significant differences in TT4 values (p=0.05) were found between the first and the third trimesters.
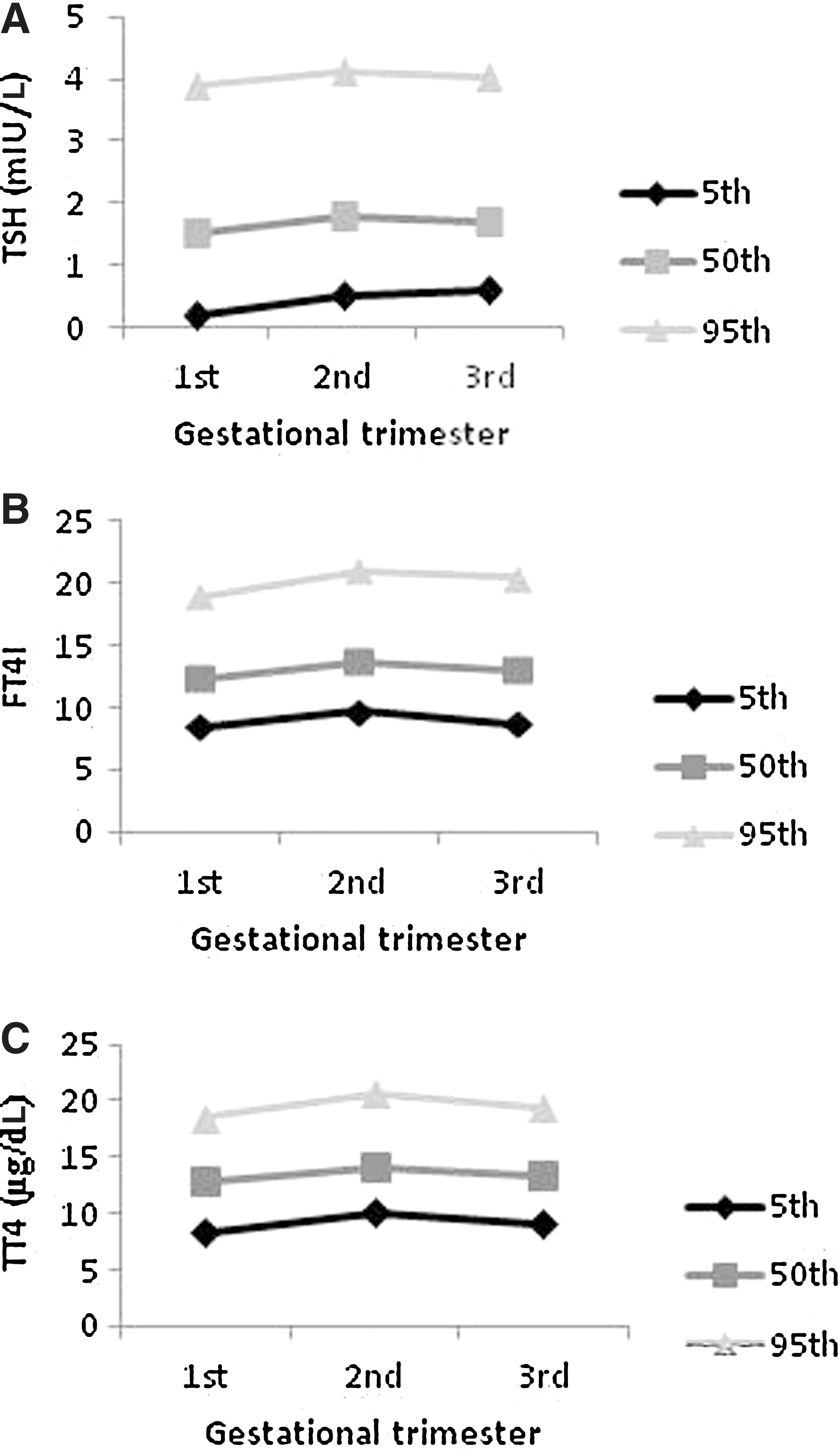
Trends of reference intervals during three trimesters of pregnancy for TSH
Serum TSH had no significant correlation with TT4. A significant but weak inverse correlation was found between serum TSH and FT4I in samples of all three trimesters of pregnancy (r=−0.26, p<0.001), as well as in the first trimester (r=−0.24, p=0.006).
Discussion
To the best of our knowledge, this is the first longitudinal study performed worldwide, which provides trimester-specific reference ranges for FT4I during pregnancy in an area of iodine sufficiency.
Based on American Thyroid Association guidelines, a single serum TSH determination is the first-line screening variable and the most sensitive parameter to reliably detect thyroid dysfunction (20); however, in most situations it is imperative for clinicians to have access to an accurate and reliable method for estimation of FT4 concentrations, especially regarding the association between isolated hypothyroxinemia and impaired fetal psychomotor development and decreased intelligence quotient (21). Laboratories usually adopt the ranges provided by manufacturers; however, differences in iodine intake and ethnicity of the pregnant women compromise the value of adopting the manufacturer ranges across different populations. Currently, there is uncertainty regarding the diagnostic accuracy of most FT4 immunoassays during pregnancy, as these methods cannot accurately reflect real FT4 changes during pregnancy. FT4 measurements are in the picomole range and technically difficult due to the possible interference by higher T4 concentrations that are measured at the nanomolar level. Recent reports indicate that serum FT4 measurement is more method dependent as current immunoassays cannot directly measure serum FT4 and are sensitive to alterations in binding proteins that occur during gestation (22,23). Most immunoassays underestimate FT4 values in comparison with other methods, such as equilibrium dialysis or online solid phase extraction–liquid chromatography/tandem mass spectrometry (LC/MS/MS), which is considered as a major advance and appears to have a higher specificity than immunoassays (23). Free thyroid hormone concentrations measured by LC/MS/MS correlate generally to a greater degree with log TSH values compared to concentrations measured by immunoassays (24). However, these accurate methods are expensive and are not available in many institutions. Significant inaccuracies were observed for FT4 immunoassays due to alterations in binding proteins and decreased values of FT4 were observed by most immunoassays in a study by Sapin et al. comparing the results of FT4 measurements by direct equilibrium dialysis and nine immunoassays with various T4-binding capacities (25). Lee et al. compared the diagnostic accuracies of two FT4 immunoassays with TT4 and FT4I, and found that measurement of FT4I may provide a more reliable estimate for FT4 (26). Therefore, FT4 measurements with immunoassays during pregnancy must be interpreted with caution.
TT4 and FT4I retain an appropriate inverse relationship during pregnancy and appear to provide more reliable FT4 estimates (26,27). In the current study, however, a correlation between TSH and TT4 and an inverse correlation between TSH and FT4I were detected only in the first trimester of pregnancy.
Due to differences observed in the TSH reference intervals between different trimesters in a single gestation and in comparison with those proposed by manufacturers in nonpregnant women, it is of utmost importance to apply the gestational age-specific reference range for TSH for a specific population in order to avoid misclassification of patients with thyroid dysfunction during pregnancy. The major discrepancy in TSH reference values in our data compared with other reports exists predominantly at the upper TSH reference limit, which is relatively higher than in most other reports (8,9,14,27). However, the studies by Marwaha et al. in India (15) and Dhatt et al. in the United Arab Emirates (28) reported much higher TSH upper reference values than the current survey. Our values of TSH reference limits are similar to those reported by Yu et al. in a study from China (13), a study that had the same self-sequential design. In agreement with previous studies, our results indicate that the derived reference intervals of TSH for pregnant women (0.2–3.9, 0.5–4.1, and 0.6–4.1 mIU/L in the first, second, and third trimesters, respectively) were narrower and lower from those proposed by manufacturers for nonpregnant women (0.2–4.5 mIU/L).
Trimester-specific reference intervals for TT4 have been determined only in two studies by Yan et al. in China (29) and Soldin et al. (27) in Sweden, and both reported lower values for TT4 compared with those observed in the current study.
The strength of our study includes the strict inclusion criteria as we considered maternal iodine status by measurement of urinary iodine levels, thyroid size and echogenecity by ultrasonography, and positivity for both TPOAb and TgAb, factors which have not been considered all together in most studies. The exclusion criteria in the present study are specific and derived from the combination of those recommended by the National Academy of Clinical Biochemistry (30) and the National Health and Nutrition Examination Survey (31) to provide a well-defined healthy population. In addition, maternal iodine sufficiency in our survey was verified by urinary iodine measurement. Another main strength is the self-sequential longitudinal design of our study, which has a narrower variation than interindividual variation caused by sampling error in cross-sectional studies on different groups. Hence, this reflects the changes of thyroid hormones during pregnancy more realistically than cross-sectional studies of different women at different stages of gestation. An additional strength of our study is the adequacy of sample size required for estimating reference values based on clinical laboratory standards (Clinical and Labaratory Standards Institute, formerly the NCCLS) (32) and the relevant application of nonparametric or parametric analyses based on the distribution of variables in our data, an important issue, which is overlooked in some studies.
Our study has some weaknesses. Although the sample size is enough for calculating reference intervals in the study population, the generalizability of these findings is hampered by the small number of women included in this longitudinal study and the exclusion criteria we have used. Therefore, the reference range cannot be applied to most individuals in the population and to a majority of Iranian women. We did not have access to information on gestational and prenatal complications, such as hyperemesis, preeclampsia, gestational diabetes, premature delivery, fetal death, or anomalies; for this reason, these were not considered in the exclusion criteria. The current survey is limited by lack of data regarding the pre- and postpregnancy period, although this does not interfere with the main goal of estimating trimester-specific reference values in our survey.
Conclusions
Results of the current survey establish reference values of thyroid hormones for pregnant Iranian women in order to accurately detect thyroid dysfunction during pregnancy. In addition, we have established the trimester-specific reference range for FT4I. Because of problems with accuracy and reliability of most FT4 immunoassay methods during pregnancy, and until tandem mass spectrometry becomes more widely available for accurate measurement of FT4, FT4I could be used for an accurate estimation of FT4 during pregnancy. As this study was only conducted within a homogenous population of Iran, we suggest to plan collaborative projects to diversify and corroborate the trimester-specific reference intervals for FT4I, so that they can be applied universally.
Footnotes
Acknowledgments
This study was supported by financial grants from the Research Institute for Endocrine Sciences (RIES), Shahid Beheshti University of Medical Sciences, Tehran, Iran. The authors would like to acknowledge the laboratory personnel of the RIES for their assistance. We also thank Ms. Niloofar Shiva for language editing of the article.
Author Disclosure Statement
No competing financial interests exist.