
Abstract
Background:
Ultrasound and ultrasound-guided fine-needle aspiration biopsy are considered the most effective approaches for both identifying and classifying thyroid nodules. However, despite continuing improvements in scanner technology and refinements in ultrasound/cytological classification guidelines, indeterminate findings still lead to diagnostic lobectomy under general anesthesia. This study aims to investigate the feasibility of applying a modified noninvasive electrical impedance spectroscopy (EIS) approach to classifying thyroid nodules.
Method:
To increase nodule classification sensitivity, we developed a new EIS-based model that introduces an optimized inductance component, which increases the measured signal-to-noise ratio of capacitance variation in and about thyroid nodules. Our model then measures the change of resonance frequency when the positive reactance of the system inductor cancels out the negative reactance of the nodule capacitance in a multi-frequency electrical signal scan. The system is termed “resonance-frequency–based electrical impedance spectroscopy” (REIS). A portable REIS system with multiple probes was assembled and preliminarily tested in our clinical facility. From an ongoing prospective study, an initial data set of 160 REIS examinations including 27 verified cancer cases was used. From the data set, a number of EIS signal features was extracted and analyzed. A multi-feature–based Bayesian Belief Network was built to classify the detected thyroid nodules. A receiver operating characteristic data analysis method was applied to evaluate classification performance.
Results:
The results showed that (i) the median resonance frequency measured by the probe nearest to malignant nodules was in general lower than that measured in benign cases, and (ii) the median descending slope of EIS signal sweep curves computed from cancer cases was larger than that computed from benign cases. The Bayesian Belief Network yielded a classification performance as measured by the area under the receiver operating characteristic curve of 0.794 [with a 95% confidence interval of 0.709–0.863].
Conclusions:
The study demonstrates that noninvasive measurement of REIS signal features may potentially provide useful supplementary information to assist in classifying between malignant and benign thyroid nodules. Such an approach may ultimately lead to a reduction in the number of unnecessary thyroid surgeries.
Introduction
Recently, a number of new technologies have been investigated with these specific aims in mind. Several examples of these novel techniques include modified 3D ultrasound imaging technologies based on Doppler (11) or contrast-enhanced method (12), ultrasound elastography (13), elastic scattering spectroscopy (14), electrical impedance tomography or spectroscopy (15), positron emission tomography (16), and time-resolved magnetic resonance angiography (17). Among these imaging modalities, ultrasound elastography has attracted extensive research interest recently, but results have been preliminary and controversial. While some studies have suggested that ultrasound elastography is a promising method (18,19), others have concluded that this method is not superior to conventional ultrasound in predicting malignancy of thyroid nodules (20,21). Since interpreting ultrasound images is largely subjective with inter-observer variability, researchers have also attempted to develop computerized diagnostic schemes to quantitatively extract and analyze image features to improve diagnostic accuracy and consistency. Several studies have shown that these computerized schemes could potentially improve classification performance of thyroid nodules (22,23). In addition to imaging-based testing methods, there has been an extensive effort in detecting and/or predicting malignancy of thyroid nodules using a variety of molecular tests that include the use of genetic biomarkers (24) and/or microRNA expression profiling (25). However, these molecular tests are costly, and US-FNAB is ultimately required to extract genetic material. The addition of molecular markers may also decrease the overall diagnostic specificity (26).
In our group, we have been investigating a different noninvasive and easy-to-use thyroid nodule diagnostic and/or classification method that is based on a modified electrical impedance spectroscopy (EIS) model. The new model is not an imaging device. It classifies between malignant and benign thyroid nodules based on the analysis of detected electrical impedance signals at and near the resonance frequency when the detection probes of the new EIS device are placed in direct contact with the patient's neck and perform the multi-frequency electrical impedance signal scans. For this purpose, we have designed and assembled a portable, low-cost, and easy-to-use resonance-frequency–based electrical impedance spectroscopy (REIS) device. We are in the process of testing the feasibility of applying this REIS system in classifying between malignant and benign thyroid nodules in a limited single-institution prospective clinical study. The study procedures and preliminary data analysis of results from the initial 160 examinations are reported in this article.
Materials and Methods
The REIS concept
It has long ago been observed that malignant (cancer) and non-malignant (benign alterations and normal) cells exhibit different local dielectric properties and, as a result, electrical conductivity and capacitance differences are measurable in malignant versus normal and/or benign tissues (27). Using this underlying characteristic, EIS technologies aimed at detecting abnormalities and classifying these as malignant or benign tissues in a variety of human organs including the thyroid have been developed and tested (28). Studies have shown, for example, that EIS may be more accurate than ultrasound in differentiating between inflammatory and malignant lymph nodes; this approach is particularly promising for characterizing cervical, axillary, and inguinal adenopathy (29). Previous EIS approaches were based on a simple parallel electrical RC (resistance and capacitance) model in which resistance of tissue is assumed constant while capacitance changes between malignant and normal or benign tissue. The differences in capacitance between the neoplastic and normal tissue result primarily from changes in cellular water content, varying amounts of extracellular fluid, changes in local blood flow, and alterations in membrane proteins. Because the malignant tissue typically shows substantially higher capacitance (C) and conductivity values than normal or benign tissue (27), electrical impedance—Z=R+j/(2πfC), where both resistance, R, and electrical current frequency, f, are constant—of malignant tissues is reduced. However, unlike in vitro electrical impedance measurements of the excised human tissue (e.g., nodules), the in vivo (non-invasive) detection of small changes in capacitance levels of a malignant thyroid nodule through a patient's neck is difficult and sometimes unreliable due to the deterioration of electrical field signal penetration through the normal surrounding tissue, which generates electrical signal noise. Hence, we proposed to test a new EIS measurement concept of adding an inductive impedance component (L) into our modified EIS-based thyroid nodule detection and classification model, as shown in Figure 1.
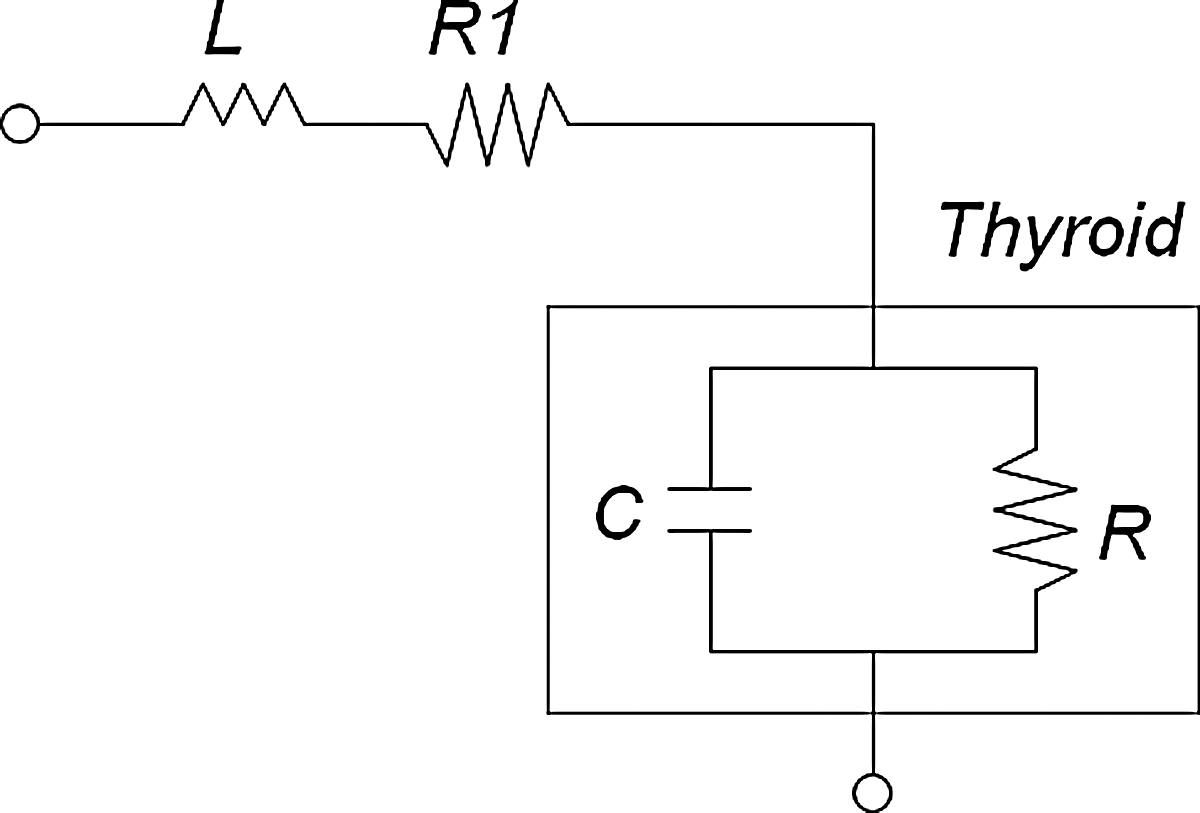
An electrical impedance spectroscopy (EIS) model for thyroid nodule classification.
In our modified model, a multi-frequency electrical signal sequence is applied and scanned through the human neck under examination. As the frequency increases, the impact of the capacitance (C) of the thyroid on the overall impedance decreases, while the impact of inductive reactance (L) of the EIS system increases. When the positive reactance of the inductor cancels out the negative reactance of the capacitor, this frequency is defined as a resonance frequency,
Assembly of a portable multi-probe REIS system
To investigate the feasibility of using this REIS-based concept for detecting and classifying thyroid nodules, we designed a prototype handheld REIS system for measuring multiple impedance signals of the neck. The system was built by Dhurjaty Electronics Consulting LLC (Rochester, NY) under an exclusive contract. The thyroid probe is designed for rapidly measuring impedance between multiple pairs of detection probes over a wide range of frequencies at small increments. The major components of this handheld portable REIS system are shown in Figure 2A. The system includes three major components: a laptop computer, an electronic control box, and a handheld device that includes seven probes in which the central probe is a common (background) probe and is configured to be paired with six outer probes to form six signal measurement channels.
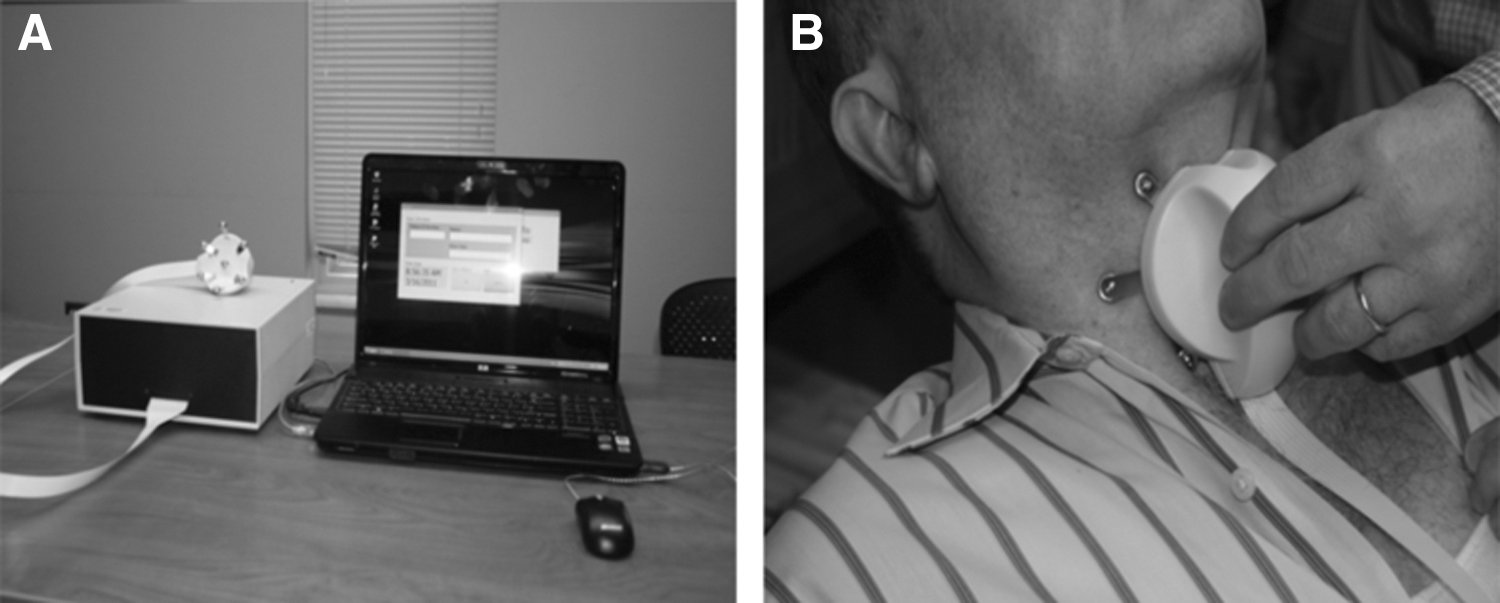
To enable and maintain good and reliable contact between the detection probes and the neck skin during the examination, all probes are spring-load mounted on the handheld sensor box. The electrical signal that is applied to the neck is 1.5 V and is swept over the frequency range from 200 kHz to 800 kHz in steps of 5 kHz. To conduct the REIS examination, an operator pushes the handheld probe device onto the patient's neck (Fig. 2B). Once the computer management program detects that all seven probes are in adequate contact with the neck, the electronic switch automatically turns on and electrical current signal scan (sweep) is performed through these six pairs of probes. During this process, the different paired probes are switched automatically when each measurement is completed. The complete REIS examination (scanning) time is approximately 8 sec. Each pair of probes produces three sets of EIS output signal sweeps representing signal amplitude (a), signal phase (p), and signal magnitude
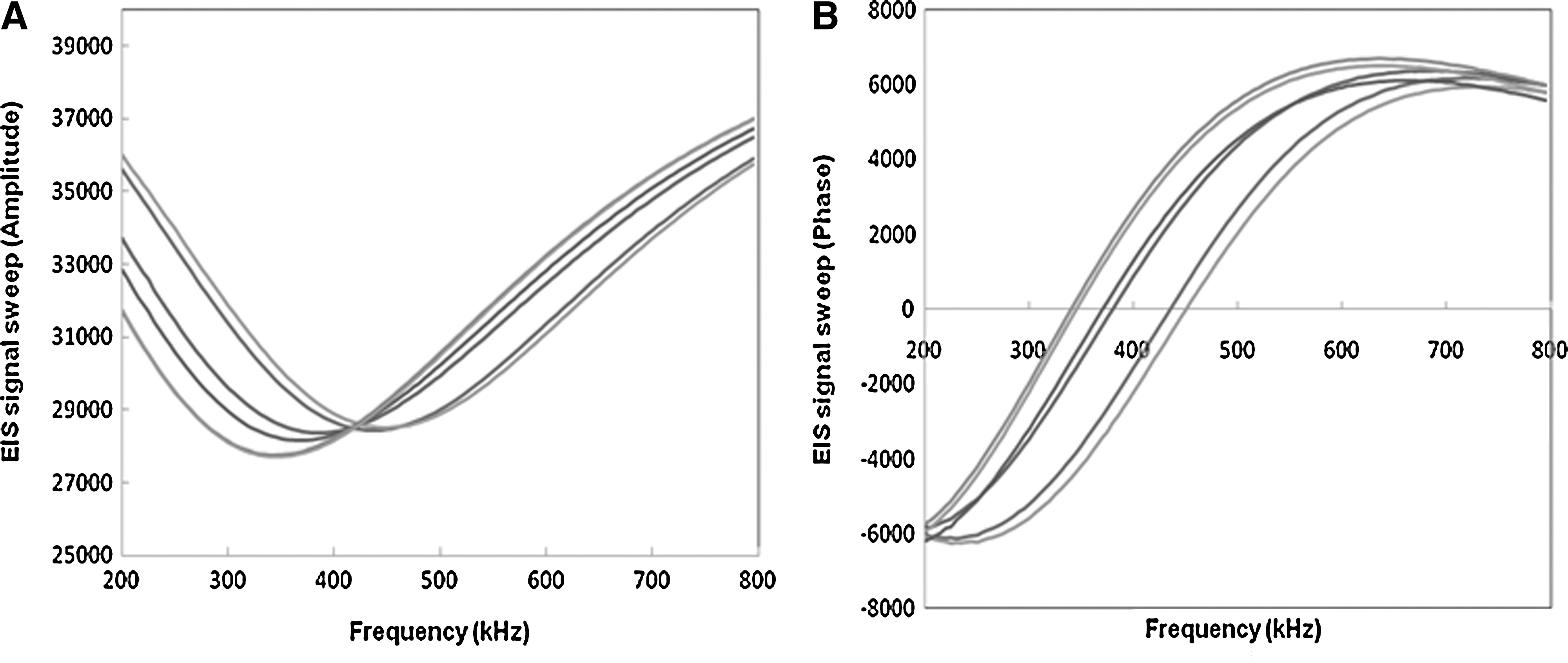
An example of six sets of recorded EIS output signal sweeps, including
Preliminary prospective data ascertainment
Under an institutional review board (IRB)–approved study and data-collection protocol, we are conducting a limited prospective study on consenting participants by performing the REIS examination on patients who undergo thyroid nodule diagnostic evaluations in our clinical facility. All health-care professionals who operate the system were trained prior to study initiation. The training process included familiarization with the recruitment and consenting protocol, proper operation of the system, correctly conducting data entry on the laptop computer (i.e., assigning each examination the correct identification number that can be later traced and matched by the honest brokers with the relevant clinical outcome), determination of the adequacy of contact signals required to obtain acceptable EIS measurements, as well as instructions on how to perform the required periodic quality-control procedures of the system. After completing the training, these health-care professionals performed the REIS examinations on consenting patients per our IRB-approved protocol. The REIS examination of each patient was performed prior to any invasive procedure (e.g., US-FNAB). During each examination, the operator assigned a unique sequential identification number to each participant. Each REIS examination was performed with the patient in a supine or a sitting (erect) position. All EIS output signal sweeps generated from multiple probe channels were recorded in a database and could also be monitored on the screen of the laptop computer for quality-control purposes. In the rare situation (e.g., significant motion of the patient during the REIS signal scanning process) that unacceptable EIS output signal sweeps appear on the laptop computer screen, the operator repeated the EIS examination.
From this ongoing prospective REIS study, we assembled an initial testing data set involving 190 patients. After excluding 30 indeterminate cases (the final diagnostic results are currently unavailable), the actual testing data set used in this study involved 160 REIS examinations acquired from 135 female and 25 male patients. The final diagnostic outcome was obtained from pathology reports for each of the participants, and these outcome data were used to establish a “truth file” for providing the reference (“ground truth”) in evaluating the REIS testing or feature classification results. Based on the final diagnostic outcome, this data set of 160 cases included 27 cases depicting at least one verified malignant thyroid nodule (classified as cancer cases) with the remaining 133 cases depicting only verified benign nodules. Table 1 shows the case distribution based on the Bethesda system for reporting thyroid cytopathology (30). Tables 2 and 3 summarize the demographic information of the patients diagnosed with malignant and benign nodules used in this study. In the 27 cancer cases, 34 malignant nodules were detected and verified by pathology. Hence, in the cancer cases, 20 depicted one malignant nodule, and seven had two malignant nodules. In 133 benign cases, 158 benign nodules were detected and verified by pathology. Of the 34 malignant nodules, 24, 3, and 7 were ultimately graded as cancer stage II, III, and IV, respectively. Histology reports identified 24 malignant thyroid nodules as papillary and 10 as papillary encapsulated follicular carcinomas. Among 133 benign cases, 28 were indeterminate cases by US-FNAB (rated as grades of III and IV in a Bethesda system rating) and thus had thyroid surgeries for lesions that eventually proved to be benign. The histology results showed a variety of nodules with a mixture of benign cells in these cases (i.e., 18 cases involving nodular thyroid hyperplasia, 8 including chronic lymphocytic thyroiditis, and 6 having follicular adenomas). The sizes of all detected nodules in the testing data set were first measured by ultrasound. If the patient had thyroid surgery, dominant nodules within the specimen were measured in one axis during the pathology examinations. Table 4 shows the distributions of recorded nodule sizes measured by both ultrasound and pathology examinations for both malignant and benign nodule groups. The nodule size measured in the pathology examinations could be different from that measured by ultrasound depending on the size of the excised specimen or actual malignant region inside the nodule.
FNA, fine-needle aspiration.
Data analyses and REIS signal classification
To test the feasibility of using REIS-based signal data to classify between malignant and benign cases, we analyzed several specific features computed from the recorded EIS output signal sweeps. Since our REIS system has six pairs of detection probes, the probe that is closest to the nodule in question should have the highest sensitivity. However, unlike imaging-based approaches (e.g., ultrasound), our REIS is not an imaging modality. Hence, the exact location of the thyroid nodule is unknown. As a malignant thyroid nodule is expected to exhibit lower impedance and thus lower resonance frequency among the six pairs of detection probes, we selected the probe pair that generated the lowest resonance frequency for data analyses. For each EIS output signal (magnitude) sweep curve, we computed the following four features: (i) the resonance frequency value (F 1); (ii) the resistance-based impedance value at the resonance frequency (F 2); (iii) the descending slope of the EIS signal sweep curve below the resonance frequency (F 3); and (iv) the ascending slope of EIS signal sweep curve above the resonance frequency (F 4). We visually analyzed potential discriminatory power for each feature individually by plotting the box plots between malignant and benign cases. We then used a receiver operating characteristic (ROC) data analysis method to compute the overall performance levels when applying each of the features individually as a classifier to distinguish between the malignant and benign cases. The area under ROC curve (AUC) computed using a maximum likelihood algorithm–based ROC program (ROCKIT, University of Chicago, Chicago, IL) was used as a summary index in the performance assessment.
In addition to classification of the malignant and benign cases using each feature individually, we computed and compared the correlation coefficients among these features. Since combining partially correlated feature data may enable an improvement in classification performance, we selected features with relatively low correlation to build and test a Bayesian Belief Network (BBN). BBN is a classification tool that uses a probabilistic learning approach to inference based on the assumption that optimal decisions can be made by reasoning the probability distribution through the observed data. Using a directed acyclic graph structure in which nodes correspond to the selected features and connections between nodes represent direct probabilistic influence among the involved features, BBN provides the flexibility for specifying dependence and independence of variables in a reasonably natural way (31). The BBN built in this study has one decision or class classification node and several dependent nodes represented by the selected features with lower correlation. The complete conditional probability table applied to build the BBN was automatically generated using a publicly available BBN optimization software tool (the BN Power Constructor and Predictor, University of Alberta, Edmonton, Canada). Using the established conditional probability table, the BBN was then applied to classify the test cases into malignant or benign groups based on the BBN-generated likelihood (or probability score) of a test case being malignant (e.g., from 0% to 100%).
Results
The mean values of the measured resonance frequency values (F 1) were 382 kHz and 439 kHz for the malignant and benign case groups respectively. The average difference between the two case groups measured by feature (F 1) was 14.9%, and the average differences for the other three features (F 2, F 3, F 4) between the malignant and benign case groups were 0.07%, 8.4%, and 7.5% respectively. Figure 4 shows the box plots of four individual features for malignant and benign case groups. The boundaries of the box plots represent the 25% percentile, median, and 75% percentile of the measured feature data distribution in the corresponding case group. The figure shows that feature F 1 has the best discriminatory power among the four features. Meanwhile, the median resonance frequency (F 1) as measured in cancer cases is lower than that measured in the benign cases. There is no observable difference in the mean resistance-based impedance values at the resonance frequency (F 2) between the malignant and benign case groups. These observations are in general agreement with expectations that capacitance levels in malignant cases should increase but resistance levels should remain relatively constant. Although comparing the box plots generated by two slope-based features—F 3 shows a larger separation between malignant and benign case sets as compared with F 4—the two features are highly correlated with a correlation coefficient of r=−0.88. On the other hand, the correlation coefficient between F 1 and F 3 is relatively low (r=−0.46).
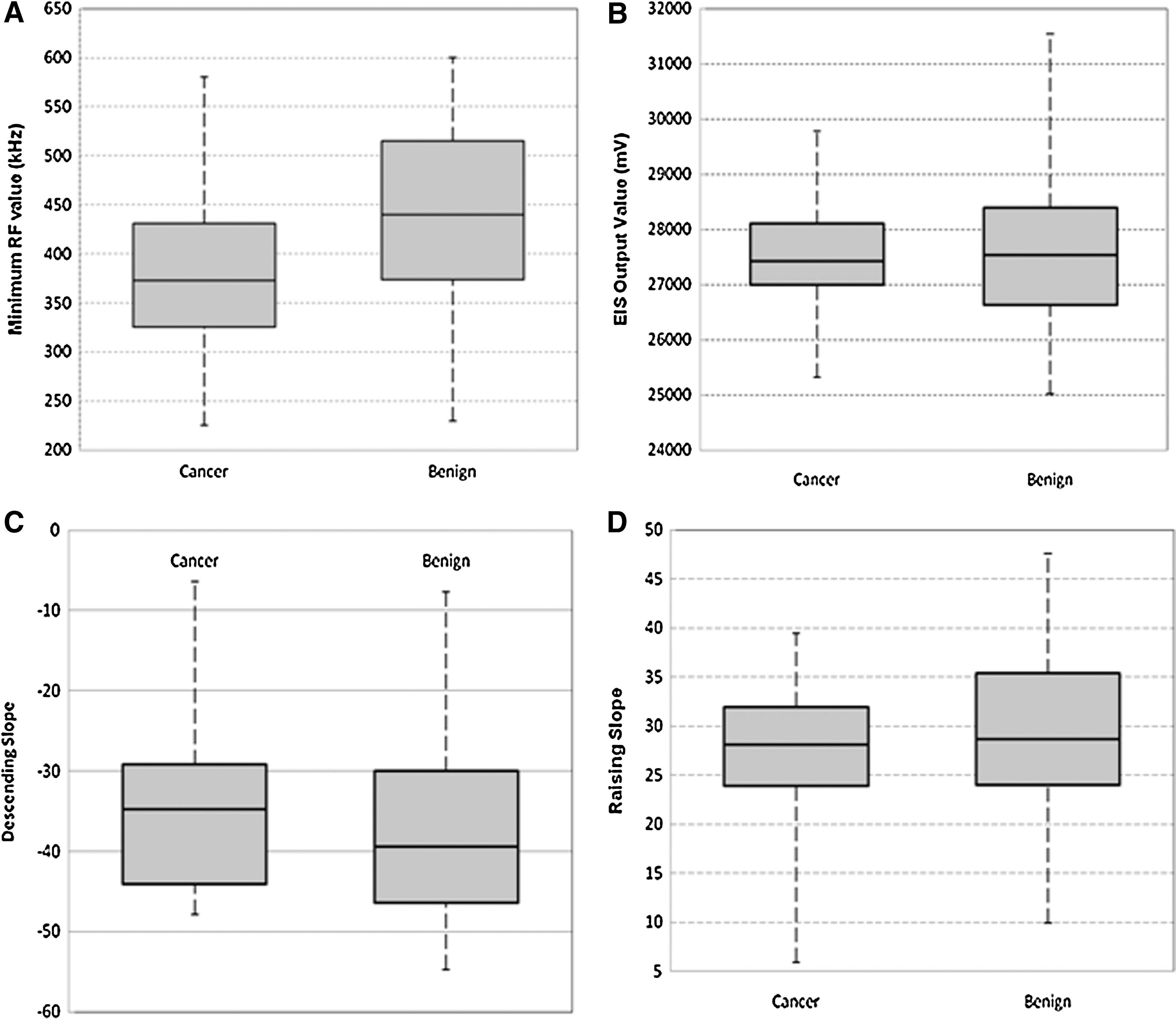
Box plots of four EIS signal features in cancer and benign cases including
Using the resonance frequency feature (F 1) alone to classify between the malignant and benign cases, the computed AUC was 0.692 [with 95% confidence interval (CI) of 0.588–0.782], while using feature F 3 alone, the AUC was 0.601 [CI 0.482–0.711]. The corresponding two-tailed p-value computed from the difference of these two AUC values is 0.041. Since these two features are not highly correlated, a simple BBN involving three nodes—one decision (or classification) node and two dependent feature nodes (F 1 and F 3)—was built (Fig. 5), and it was applied to classify between 27 malignant and 133 benign cases in the data set. The computed AUC was 0.794 [CI 0.709–0.863]. Figure 6 compares two ROC curves generated using a single feature (F 1) and the BBN involving two features (F 1 and F 3). Using the BBN achieved a significantly higher classification performance level as compared with the single feature-based classifier (p<0.01). In this rudimentary and very preliminary analysis, the BBN correctly diagnosed 23 of 27 cases depicting malignant thyroid nodules (85% sensitivity) and 81 of 133 cases with benign nodules (61% specificity). The results also showed that the detection sensitivity of the BBN did not depend on the nodule size (Fig. 7).
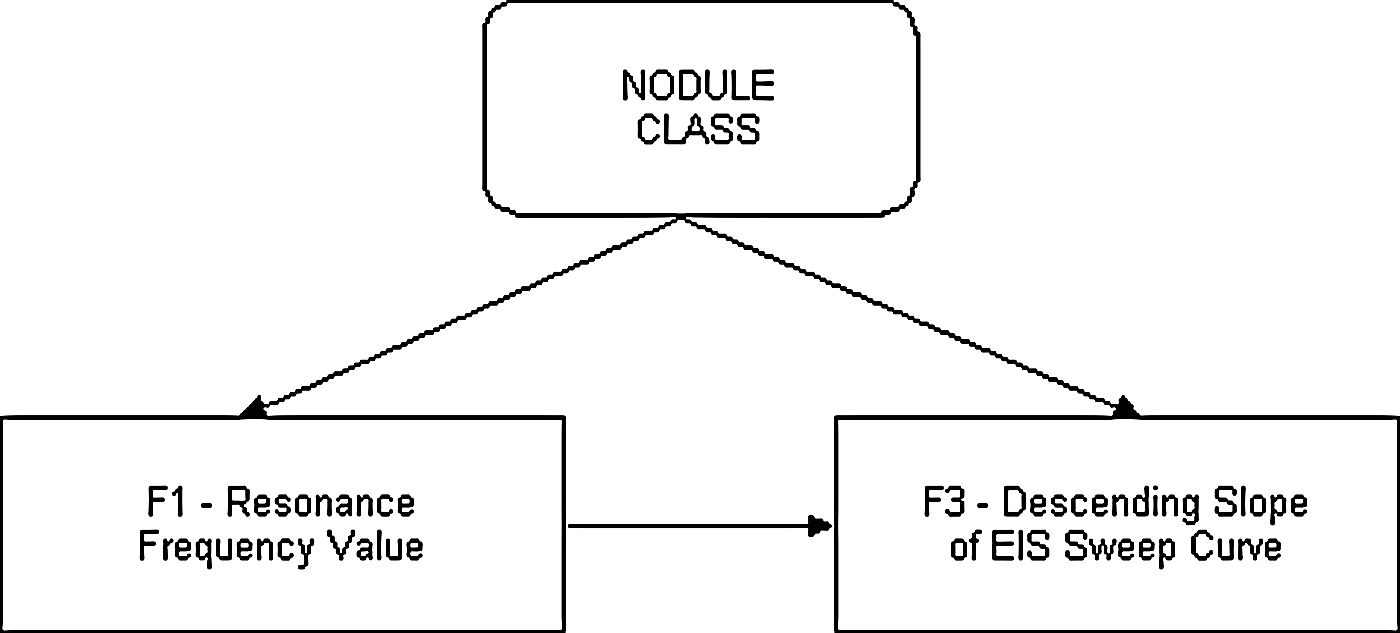
Illustration of the Bayesian Belief Network (BBN) built for this study.
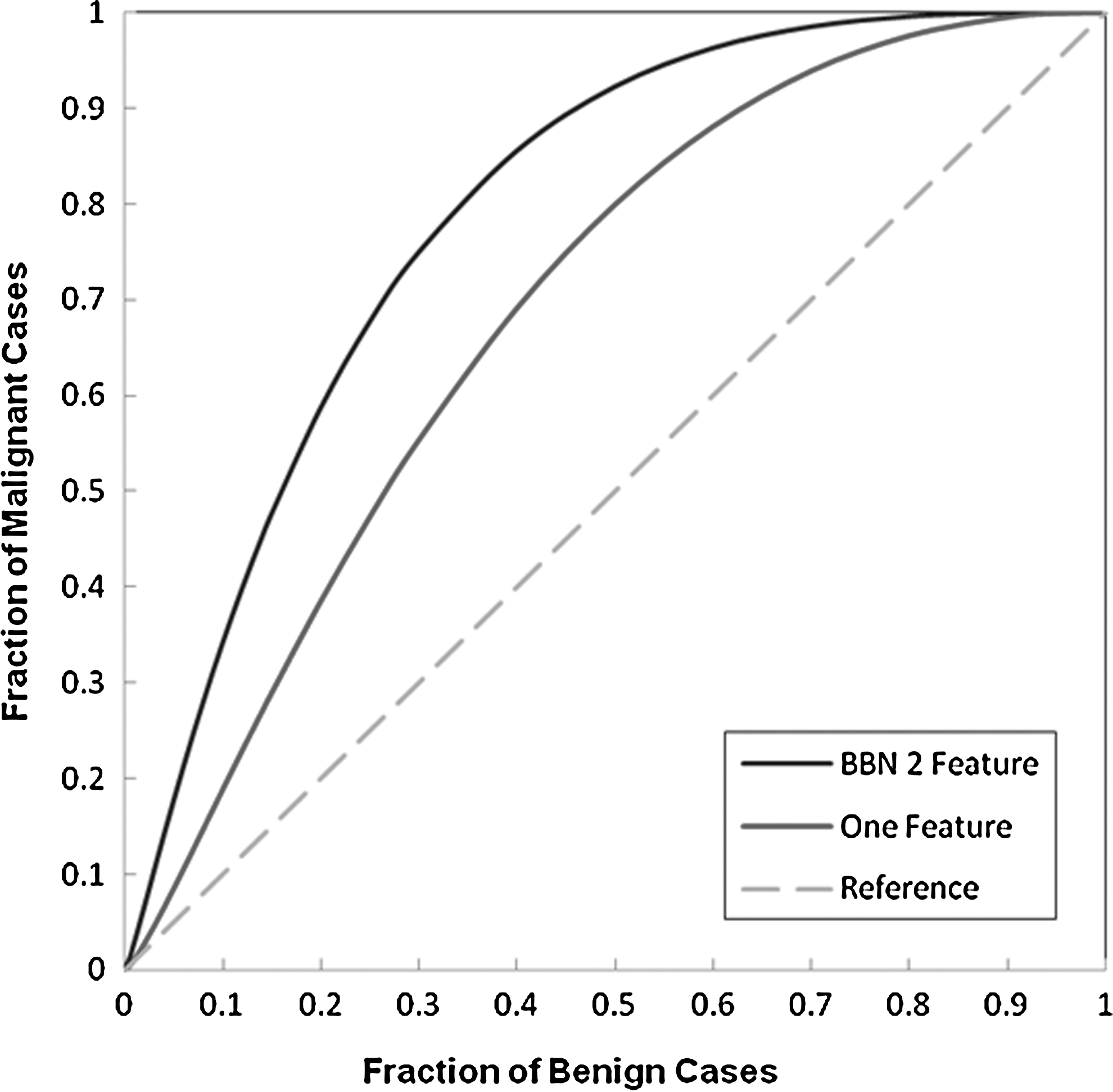
Comparison of two receiver operating characteristic (ROC) performance curves. The middle curve was generated using one feature only (F 1), and the top curve was generated using a simple BBN with two features (F 1 and F 3). The areas under the curves are 0.794, 0692, and 0.500 for the BBN, the one feature classifier, and the reference (chance) line respectively. The difference between the two ROC curves is statistically significant (p<0.01).
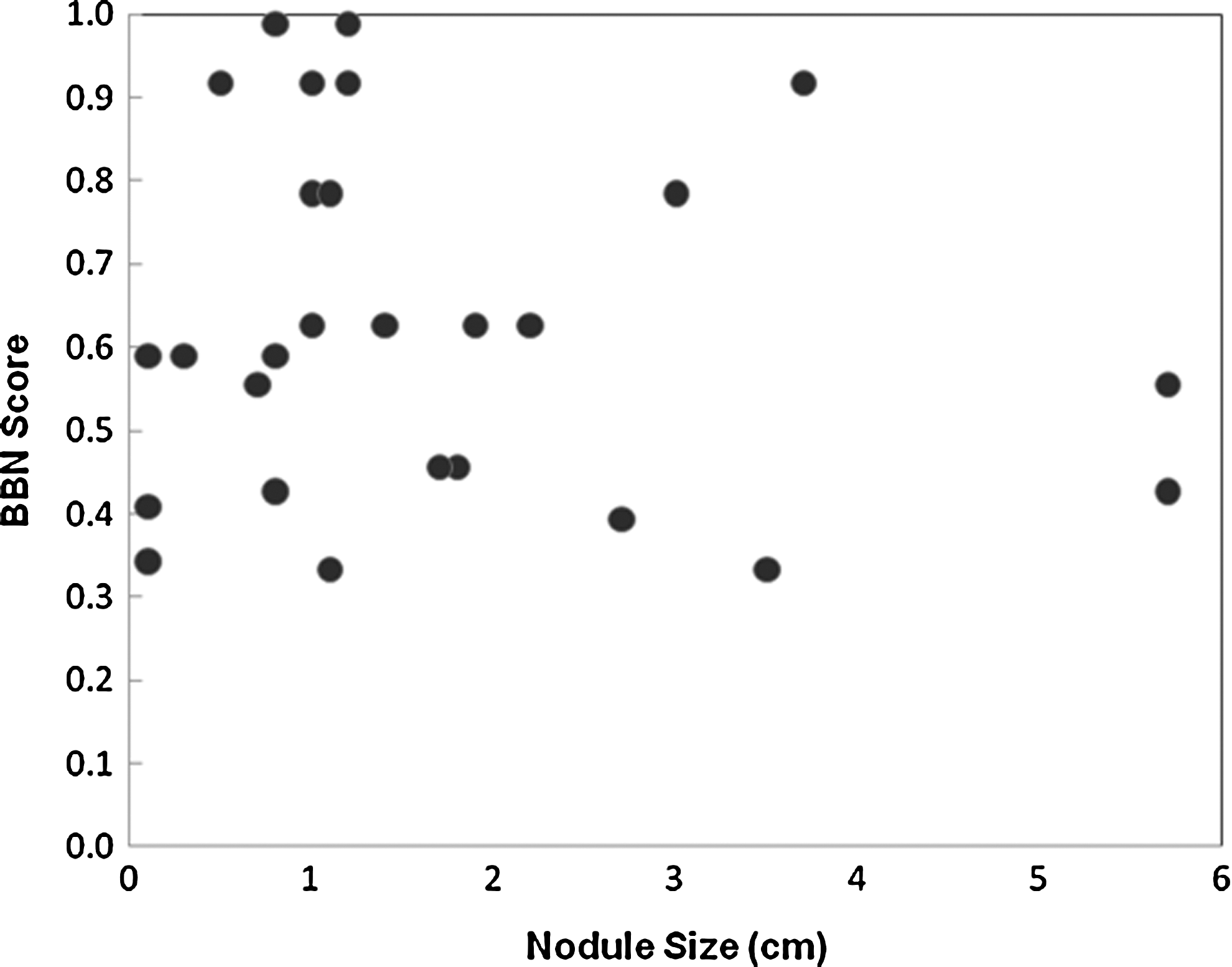
Distribution of BBN classification scores as a function of the sizes of malignant nodules in the 27 cancer cases (as determined by pathology examination). In the seven cases depicting two malignant nodules, the nodule size of each case is then represented by the sum of two nodule sizes.
Discussion
Thyroid nodules are common and are usually benign. Despite an abundance of literature exploring discriminatory ultrasound features, and continued refinements in consensus guidelines, the appearance of thyroid nodules on ultrasound is often nonspecific. The current diagnostic gold standard—US-FNAB—also generates non-diagnostic or indeterminate results in a subset of cases, despite meticulous technique. In this data set, 21.1% (28 of 133) benign cases had thyroid surgeries solely for definitive diagnosis. The management of this significant subset of indeterminate nodules is difficult for the endocrinologist, endocrine surgeon, and patient. This management dilemma has prompted different and innovative approaches to be investigated. The ultimate goal of these efforts is eventually to enable a significant reduction in the number of unnecessary thyroid surgeries without compromising diagnostic accuracy. Although a large number of advanced imaging modalities and molecular/genetic biomarkers have been tested for this purpose, the specificity of these approaches remains relatively low. In this study, we have investigated and preliminarily tested a new approach that has a number of unique characteristics.
First, unlike previous efforts that have focused on generating the complicated electrical impedance signal distribution maps (images) that may associate specific signal patterns with malignant thyroid nodules (15), we investigated a new and simple EIS concept based on measuring changes in resonance frequency. We built a new EIS model that adds a special inductor into the detection signal scheme to increase signal-to-noise ratio of the measured signal differences for malignant and benign nodules. Although similar methods have been tested in our previous studies of the breast to assess risk of having or developing breast cancer (32,33), this general approach has not been applied to classify thyroid nodules in vivo to date. Our study suggests that the minimum resonance frequency measured from multiple pairs of probes (detection channels) and other EIS-based signal features around the resonance frequency carry useful supplemental information that may be applied to distinguish between malignant and benign thyroid nodules.
Second, our REIS system is not an imaging device, and it only detects the resonance frequency and other related EIS signal changes as a result of changes in tissue characteristics. Therefore, the detected REIS signal curves (Fig. 3) do not contain information on nodule location, nor can the curves distinguish between cases depicting one or multiple small nodules. Such differences make it difficult to compare our REIS approach directly with other imaging-based examinations, although our REIS method could generate diagnostic results that may not correlate highly with existing imaging modalities. For example, the detection and classification sensitivity of our REIS method does not depend on nodule size (Fig. 7) and is likely independent of differences in normal thyroid tissue density. This observation is consistent with our previous findings when applying a similar REIS-based approach aimed at detecting breast lesions (32).
Third, as compared with other imaging and non-imaging–based modalities, our REIS system is a portable, low-cost, and easy-to-use device. In our ongoing prospective study, the REIS system was assembled on a compact movable cart that could be easily moved from one examination room to another. The system can be set up quickly for reuse. The REIS signal scanning and recording is also fast with the examination lasting 8 sec. The total examination time, including preparation, positioning, data entering, and testing, should take ∼1–2 min. Our ongoing prospective study has demonstrated the feasibility of using this portable REIS device in a very busy clinical setting. Conducting our REIS examination is also safe, as the system generates a maximum current of 30 mA during the application of the electrical signal. Applying this handheld device to the neck skin is physically similar to holding a 1.5 V battery between one's fingers. There have not been any reports of sensation of an electrical current by patients undergoing the measurement to date. In addition, if the concept is validated, detecting and measuring resonance frequency should eventually be simple and reliable.
As this is a very preliminary study, it has several limitations. First, the size of our initial testing data set is small. Although unlike many other types of machine learning classifiers, there is no iterative training process used in building a BBN, the robustness of the BBN performance depends on the size and diversity of the data set. Therefore, the performance reported in this preliminary study has to be validated in future studies using larger and more diverse data sets. Second, we explored and tested only a very small number of EIS signal features. The recorded EIS output signal sweeps may carry more information that could potentially be used in distinguishing between malignant and benign thyroid nodules. Third, the classifier (BBN) yielded a relatively low specificity (61%). Because the majority of thyroid nodules are benign, as long as the applied method has high sensitivity, lower specificity may still be useful in helping to reduce a large number of unnecessary thyroid surgeries.
Although our preliminary observation showed a clear trend of reducing resonance frequency in cases depicting malignant nodules, the reproducibility of our REIS examination results has not been fully investigated as to whether or not using multiple repeated REIS tests on the same patient could achieve better performance, similar to using multiple repeated measures in other medical tests (e.g., pulmonary function tests). Whether and how this type of REIS examination would possibly enable clinicians to reduce the number of unnecessary thyroid surgeries without compromising the diagnostic sensitivity is clearly beyond the scope of this very preliminary study and has yet to be fully investigated and clinically validated.
In summary, correct classification of thyroid nodules remains a difficult task that has a high clinical impact. In this study, we preliminarily investigated a unique EIS-based concept and method using analyses of resonance frequencies detected by a multi-probe REIS system. Our observations are in general agreement with previous scientific assumption that higher capacitance levels of malignant thyroid nodules could be detected and measured in vivo (noninvasively) using this new resonance REIS-based approach. As our effort progresses and our REIS data set increases, we will continue to explore additional effective features that could improve our classifier's performance. Before one can realize the ultimate goal of developing a REIS-based thyroid nodule detection and classification tool that may be acceptable in clinical practice, a number of technical and operational issues have to be further investigated and the results appropriately validated.
Footnotes
Acknowledgment
This work is supported in part by Grant R21-CA154262 to the University of Pittsburgh from the National Cancer Institute, National Institutes of Health.
Author Disclosure Statement
There are no financial disclosures or conflicts of interest from any authors in this study.