
Abstract
Purpose:
To evaluate the diagnostic role of core needle biopsy (CNB) in sonographically suspicious thyroid nodules with initially benign cytologic results through a histologic analysis of CNB specimens.
Methods:
Between October 2008 and July 2011, 88 patients underwent ultrasound (US)-guided CNB for initially benign cytologic results with suspicious US features at our institution. In all, 85 patients with 85 focal thyroid nodules were included in the study after surgery or concordant benign readings following fine-needle aspiration biopsy (FNAB) and CNB. We evaluated the risk of malignancy, diagnostic performance of CNB, and histologic findings for these nodules.
Results:
Of the 85 nodules, 28 (32.9%) were histologically upgraded on CNB specimens including one case of atypia of undetermined significance (AUS), seven cases of follicular neoplasm, one case of suspicious for malignancy, and 19 cases of malignancy. Of these, 27 (31.8%) were finally confirmed as malignant, and one as follicular adenoma at surgery. The 27 malignant nodules included 21 papillary thyroid carcinomas (PTCs), five follicular thyroid carcinomas, and one Hürthle cell carcinoma. All PTCs were diagnosed from CNB readings of AUS suspicious for malignancy or malignancy. Follicular thyroid carcinomas and Hürthle cell carcinoma were diagnosed from CNB readings of follicular neoplasm. Histologic analysis of benign CNB specimens revealed severe fibrosis (96.4%), hemosiderin (21.4%), calcification (17.9%), granulation tissue (12.5%), and focal lymphocytic thyroiditis (12.5%).
Conclusions:
The histologic information obtained by analysis of CNB specimens may enable more confident diagnosis for benign nodules with suspicious US features and reduce the need for repetitive FNABs or diagnostic surgery.
Introduction
The use of core needle biopsy (CNB) to diagnose thyroid nodules has been minimally reported and is currently being investigated. Unlike the old technique of non–image-guided large-needle biopsy, US-guided CNB using a modern spring-activated biopsy needle is safe and tolerable (13 –22). Given that CNB provides a larger tissue sample, it may offer additional information and facilitate a more precise histologic diagnosis than that offered by FNAB for some cases of thyroid masses (23,24). Recent studies have supported this assumption by demonstrating that CNB is more useful than repeat FNAB in thyroid nodules read as nondiagnostic or atypia of undetermined significance (AUS) in terms of both reducing the frequency of inconclusive results and improving the diagnostic performance for malignancy (25 –27). However, to date, there are no studies that evaluate the diagnostic role of CNB for thyroid nodules with suspicious US features that have initially benign cytologic results.
The purpose of this study was to evaluate the diagnostic role of CNB in sonographically suspicious thyroid nodules with initially benign cytologic results through a histologic analysis of CNB specimens.
Materials and Methods
Patient selection
This retrospective study was approved by our institutional review board, and written informed consent was obtained from all patients before FNAB or CNB. We reviewed the medical records and US images of patients who underwent US-guided CNB for thyroid nodules in our institution between October 2008 and July 2011. Over this period, 600 thyroid nodules in 587 patients were subjected to US-guided CNB for reasons that included previous inadequate cytological results (n=157), indeterminate cytological results (n=208), benign cytological results but suspicious US features (n=88), or clinician or patient requests due to dense calcifications, strong fear of cancer, or unknown cause (n=147). Of these, we selected 88 focal thyroid nodules on which US-guided CNB had been performed owing to initially benign cytologic results with suspicious US features. Of the 88 nodules, two were excluded because they showed follicular neoplasm after CNB but were not surgically treated. One was excluded because CNB identified papillary thyroid carcinoma (PTC) but surgery was not yet performed. This study finally included 85 patients (67 women and 18 men; mean age, 52.4 years; range, 22–75 years) with 85 thyroid nodules. The mean size of the nodules on US was 18.6±13.6 mm (range, 5.1–70.0 mm). For malignant nodules (n=27), the diagnosis was based on histopathological reading after surgery. For benign nodules (n=58), the diagnosis was based on histopathological reading after surgery (n=1), and concordant benign readings of FNAB and CNB (n=57).
US-guided CNB procedures
US examinations were performed using one of two US systems: an iU22 unit (Philips Healthcare, Bothell, WA), or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear high-frequency probe (5–14 MHz). All US examinations and US-guided CNBs were performed by two experienced radiologists (J.H.B. and E.J.H.), who have 16 and 7 years of clinical experience, respectively, in performing and evaluating thyroid US images.
US-guided CNBs were performed using a disposable 18-gauge double action spring-activated needle (1.1 or 1.6 cm excursion; TSK Ace-cut; Create Medic, Yokohama, Japan) after local anesthesia with 1% lidocaine. Using a freehand technique, the end of the biopsy needle was advanced into the edge or within the nodule, and the stylet and cutting cannula of the needle were then fired sequentially. After CNB, each patient was observed, and a firm, local compression of biopsy site was applied for 10–20 minutes.
Analysis of US findings
US images were retrospectively reviewed independently by the same radiologists (J.H.B. and E.J.H.), who performed the procedures. Both reviewers had no knowledge of the patients' clinical histories, previous imaging results, or cytopathology results. Any discrepancies between the two reviewers were resolved by consensus. The US findings of the nodules were evaluated for the following features: shape (oval-to-round, irregular, or taller than wide), margins (well-defined, ill-defined, or spiculated), echogenicity (hyperechoic, isoechoic, hypoechoic, marked hypoechoic), presence of echogenic dots suggesting microcalcifications, and presence of macrocalcifications. The suspicious US features were interpreted as nodules with the presence of at least one malignant US finding including taller than wide shape, spiculated margin, marked hypoechogenicity, and presence of micro- or macrocalcifications. Nodules without suspicious US features were defined as benign.
Analysis of histologic results
CNB and surgical specimens were reviewed by an experienced pathologist (D.E.S.), who has 8 years of experience in thyroid cytopathology. Given that the diagnostic criteria of CNB have not been standardized for thyroid nodules, diagnoses based on CNB histology were categorized into the six categories of the Bethesda System as follows (25,28,29). A nondiagnostic CNB reading included (i) absence of any identifiable follicular thyroid tissue, (ii) presence of only a normal thyroid tissue, and (iii) tissue containing only few follicular cells insufficient for diagnosis. The benign CNB readings included colloid nodules, nodular hyperplasia, lymphocytic thyroiditis, Graves' disease, and postpartum thyroiditis. The AUS reading for CNB included nodules in which some atypical cells were present but were not sufficient for establishing the diagnosis of “suspicious for malignancy” or “malignancy.” Nodules with histologic features favoring follicular neoplasm were categorized as ‘‘suspicious for follicular neoplasm or follicular neoplasm.’’ The “suspicious for malignancy” or “malignancy” CNB readings were selected when the specimen exhibited atypical features that were insufficient for definite diagnosis of malignancy or had unequivocal features of cancer, respectively. Immunohistochemistry data were not used as a basis for these readings.
When the nodule showed concordant benign results on a CNB specimen with a FNAB, it was further analyzed to reveal the histologic findings according to its components. The histologic findings evaluated included fresh hemorrhage, hemosiderin, fibrosis, tissue granulation, calcification, infarction, atypia, mitoses, metaplasia, vascular proliferation, and focal lymphocytic thyroiditis (30 –32). Any histologic findings not included in the list above were also included in the report of the pathologist.
Statistical analysis
Statistical analysis was performed using the SPSS software package (version 19.0 for Windows; SPSS, Chicago, IL). Categorical data were summarized using frequencies and percentages. The chi-square test and Mann-Whitney U test were used to evaluate the relationship between the variable factors and benignity or malignancy of the nodules. A p-value of <0.05 was considered statistically significant.
Results
CNB results and final diagnosis
Of the 85 sonographically suspicious thyroid nodules with initially benign cytologic results in our study cohort, 28 (32.9%) were histologically upgraded on CNB specimens, including one case of AUS, seven cases of suspicious for follicular neoplasm or follicular neoplasm, one case suspicious for malignancy, and 19 cases of malignancy (Fig. 1). There was no case of nondiagnostic reading, and one case of inconclusive reading including nondiagnostic and AUS (1.2%) after CNB. At the time of surgery, of the 28 histologically upgraded nodules, 27 (31.8%) were finally confirmed as malignant and one as follicular adenoma. The clinical and demographic characteristics were not significantly different between benign and malignant nodules (Table 1). Pathologic results of 27 malignant nodules included 21 (77.8%) PTCs, five (18.5%) follicular thyroid carcinomas, and one (3.7%) Hürthle cell carcinoma. All PTCs were diagnosed from CNB readings of AUS (1/1), suspicious for malignancy (1/1), and malignancy (19/19). Follicular thyroid carcinomas and Hürthle cell carcinoma were diagnosed from CNB readings of suspicious for follicular neoplasm or follicular neoplasm (6/7). Using the CNB results of suspicious for follicular neoplasm or follicular neoplasm, suspicious for malignancy, and malignancy as positive for detecting nodules that required surgery in the next management plan, the diagnostic sensitivity, specificity, positive predictive value, and negative predictive value of CNB were 96.4%, 100%, 100%, and 98.3% for follicular neoplasm and thyroid cancer. Table 2 shows the comparison of the CNB results and final diagnosis for the nodules.

Data indicate the number of nodules.
All CNB results of AUS, suspicious for malignancy, and malignancy were confirmed to be papillary thyroid cancers.
CNB results of FN/SFN readings were confirmed to be one follicular adenoma, five follicular thyroid carcinomas, and one Hürthle cell carcinoma.
AUS, atypia of undetermined significance; FN/SFN, follicular neoplasm or suspicious for follicular neoplasm.
Histologic analysis of benign nodules
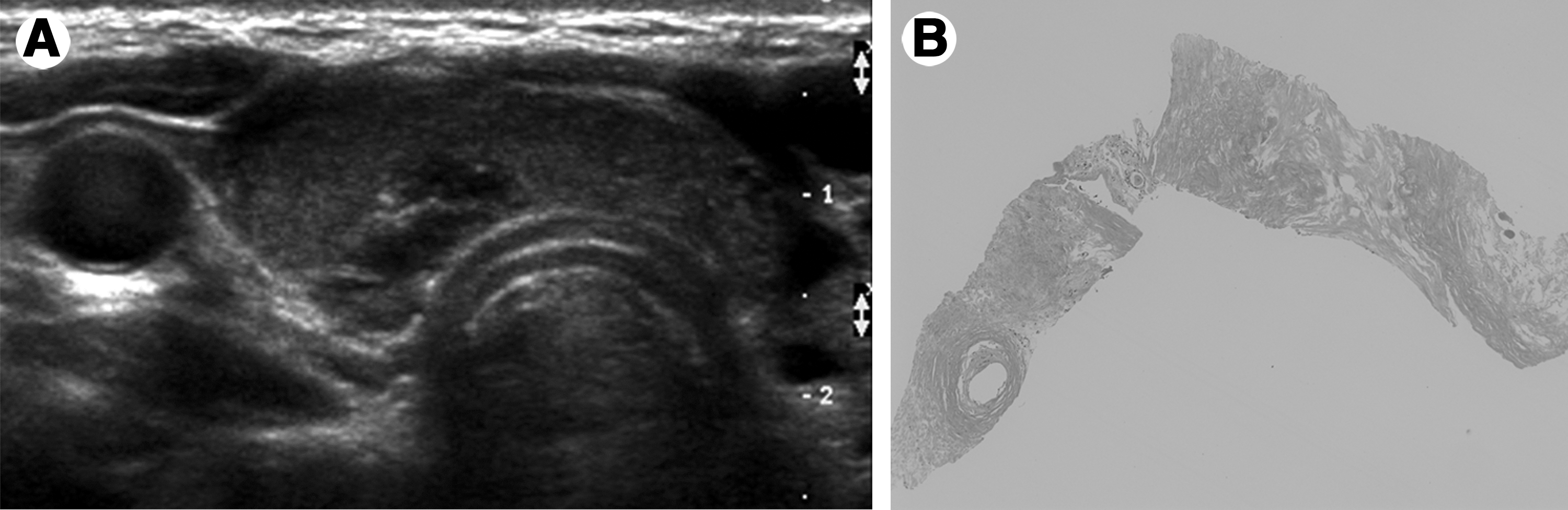
Following analysis of FNAB and CNB specimens, 57 thyroid nodules with suspicious US features showed concordant benign results. Although a CNB specimen was not available for one of the nodules, the remaining 56 were further analyzed to reveal histologic findings according to their components (Table 3). The CNB specimens revealed severe fibrosis in 96.4% of the nodules with varying frequencies of hemosiderin (21.4%), calcification (17.9%), tissue granulation (12.5%), and focal lymphocytic thyroiditis (12.5%). Most CNB specimens of benign nodules showed a small number of follicular cells against a background of tissue that had undergone severe fibrosis (Fig. 2).
Among the seven CNB specimens that revealed focal lymphocytic thyroiditis, four CNB specimens showed many plasma cell infiltrates mixed with lymphocytes, and three CNB specimens showed only lymphocytic infiltrates without appreciable damage of follicular cells or diffuse oncocytic metaplasia. Two CNB specimens showed occasional granulomas without necrosis in adjacent area of granulation tissue. One CNB specimen showed follicular cells with squamous metaplasia.
Discussion
Our present study demonstrates that CNB has an excellent diagnostic performance for managing sonographically suspicious thyroid nodules with initially benign cytology results. Given that benign thyroid nodules, which comprise fibrotic and hemorrhagic tissue, can have suspicious US features, histologic information obtained from analysis of CNB specimens may improve the diagnostic accuracy.
There are two areas of clinical significance associated with nodules of initially benign cytologic results but suspicious US features. First, the risk of malignancy is significantly higher than those with benign US features (4 –7). Although most thyroid cancers grow slowly and have a good prognosis, even a small thyroid cancer can metastasize to other organs (33 –35). Delayed diagnosis of thyroid cancer may influence prognosis and thus cause medico-legal problems. Second, a mismatch of US and cytological results may require that a patient be subjected to repetitive FNABs, or even surgery, for the purposes of diagnosis (4 –7,36,37). Histological information obtained by a CNB specimen may improve diagnostic confidence in these nodules.
The causes of false-negative results following FNAB can be related to the nature of the lesions, intrinsic limitations of the procedure, and the manner, skill, and experience of the operator (38,39). False-negative results can also result from the subtle cytologic features of PTC, especially the follicular variant, or other causes of interpretation error (40). Given the inevitable limitations of FNAB for the diagnosis of thyroid nodules, many studies have reported the importance of repeat FNABs, especially for thyroid nodules with suspicious US features. In our study, 31.8% of initially benign cytologic results with suspicious US features were confirmed to be malignant. This correlates well with previous studies reporting a risk of malignancy between 20.4% and 56.6% in these nodules (4,5) and is quite different from the risk of malignancy (<3%) for nodules with initially benign cytologic results (29). When considering these study results, nodules with initially benign results should be managed differently based on the observed US features.
The value of CNB for the evaluation of thyroid nodules is currently under investigation. The American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association guidelines have reported that CNB may have a complementary role in selected cases of thyroid masses, such as repeated inadequate FNA cytology (24). Samir et al. (27) recently suggested that a combination of CNB and FNAB should be strongly considered as an alternative to surgery in individuals with two prior nondiagnostic FNABs. In addition, Na et al. (25) reported that CNB is more useful than repeated FNAB for diagnosis, as well as ensuring AUS readings after an inconclusive FNAB reading. Our study results revealed that CNB also has an excellent diagnostic performance for managing sonographically suspicious thyroid nodules with initially benign cytologic results. CNB readings that indicated a need for surgery showed a 100% positive predictive value for follicular neoplasm and malignancy.
The causes of benign nodules with suspicious US features are not well known. Several studies have revealed that benign cystic nodules can have suspicious US features on follow-up US after aspiration, spontaneous size reduction, or ethanol ablation (41 –44). It was also reported that a benign solid nodule can mimic PTC after size reduction on follow-up US (45). However, if the nodules are initially encountered in practice without previous analysis, FNAB is inevitably the first step in order to evaluate the nodule for malignancy. In addition, repetitive FNABs or even diagnostic surgery are common in nodules with suspicious US features to improve the diagnostic accuracy. In our current study, benign nodules with suspicious US features were histologically characterized by severe fibrosis and hemorrhage, with few follicular cells in CNB specimens. These histologic findings may explain the results of previous US studies that demonstrated suspicious changes of benign nodules after size reduction on follow-up US (41 –45). Benign nodules that show degenerative changes may have suspicious US features, such as an increase in the extent of fibrosis. Based on our study results, a better understanding of histologic information obtained from CNB specimens may improve the diagnostic accuracy of benign nodules that have suspicious US features, and may obviate the need for repeated FNABs or diagnostic surgery.
Our study has several limitations. First, its retrospective design may have introduced selection bias. Given that a certain percentage of nodules with initially benign cytologic results are clinically followed longitudinally regardless of US features, the prevalence of these nodules cannot be evaluated as well. Second, thyroid nodules with concordant benign FNAB and CNB results were regarded as benign; of note, clinical and US follow-up data were stable in all cases. Third, the diagnostic categories of CNB specimens have not been standardized yet. This aspect requires further research.
In conclusion, CNB is clinically useful in managing thyroid nodules with suspicious US features after an initial benign FNAB results. The histologic information obtained by analysis of CNB specimens may enable more confident diagnosis for benign nodules with suspicious US features and reduce the need for repetitive FNABs or diagnostic surgery.
Footnotes
Disclosure Statement
There is no conflict of interest regarding this article to be disclosed for any of the authors.