
Abstract
Pretibial myxedema (PTM) is a rare extrathyroidal manifestation of Graves' disease that requires treatment when the clinical picture is markedly evident. In addition to topical treatment with steroid ointments, there have been previous reports of subcutaneous injections of steroids. This procedure may cause nodular degeneration of the skin due to fat atrophy when standard needles are used. In the present study, we have tried a novel modality of treatment of PTM by injecting a solution of dexamethasone in the subcutaneous tissue using needles employed for mesotherapy. These needles are ≤4 mm long and deliver the medication within the dermis or the first layer of the subcutaneous fat. We have treated five patients, four with diffuse and one with elephanthiasic PTM. We utilized multiple injections of a solution of dexamethasone, lidocaine, and saline in the PTM plaque and in the pretibial area, both in the PTM plaque and in the area surrounding the lesions, once a week for three consecutive weeks. Two patients with a more severe form of PTM underwent another two cycles four to six weeks after initial treatment. Patients were studied before and after treatment by clinical assessment and ultrasound of the pretibial skin. The treatment was well-tolerated, with only moderate pain upon injection of the solution. One month after treatment, all patients showed improvement of PTM at clinical assessment and a reduction of the thickness of the lesions at ultrasound of ∼15%, involving mostly the dermis. Moreover, all patients reported amelioration of the leg appearance. The present study, although preliminary, shows that intralesion steroid injection with mesotherapy needles in PTM is effective and well tolerated, and does not cause undesired long-term modifications of the skin. More studies are warranted to standardize such treatment in larger groups of patients.
Introduction
PTM has been classified into three clinical forms: (i) diffuse PTM, characterized by hyperpigmentation and/or nonpitting edema of the skin associated with dilated follicular openings; (ii) nodular- or plaque-like myxedema, with sharply circumscribed dermal lesions; and (iii) elephantiasic PTM, in which a combination of nodules and edema is evident (10,11).
In most cases, PTM is mild and subclinical (12) with only aesthetic implications (7). In these situations, no specific treatment is generally required because up to 50% of patients have been reported to achieve a complete spontaneous remission after several years (7). In more severe cases, in which there is significant skin discomfort as well as a cosmetic issue, a number of therapeutic approaches have been proposed, including compressive dressings with topical corticosteroids (13,14) and intradermal injections of glucocorticoids (GCs) (7,15,16) or hyaluronidase (17). Hypodermal injections of triamcinolone have not been extensively used, and evidence of a long-term efficacy of this therapy is lacking (7). The occurrence of important adverse reactions, such as hypopigmentation, skin atrophy (18,19), and lumpy skin (15), has been reported and may have hampered a more widespread use of this treatment modality. A route of steroid administration that may avoid the skin degeneration associated with hypodermal injection into the subcutaneous tissue may be mesotherapy. Mesotherapy, also known as intradermotherapy, is carried out with needles 4–13 mm long, and has been originally employed in the management of chronic pain. It has also become popular in Europe for cosmetic applications. We have designed the present study to test the intradermal administration of steroids with mesotherapy needles in the treatment of clinically overt PTM. The outcome of this therapy has been assessed by pretibial skin ultrasound, which allows quantifying the degree of reduction of PTM skin lesions, as previously reported (12).
Materials and Methods
Patients
We studied, after collection of informed consent, 14 women aged 54.8±3.7 years (mean±SE) with PTM, 13 affected with GD and one with Hashimoto's thyroiditis (HT). The patient with HT was on levothyroxine replacement therapy, and 6 of 13 patients with GD were euthyroid after previous total thyroidectomy (three patients) or radioiodine therapy (three patients). One patient was euthyroid after methimazole withdrawal. The remaining six patients were euthyroid while on methimazole therapy. GO of variable severity was diagnosed in 12 of 14 patients; five patients had inactive moderate-to-severe GO after previous treatment with high doses of intravenous (i.v.) glucocorticoids. The remaining seven patients had mild GO limited to lid malposition or minimal to mild motility defects. All of these patients were subsequently submitted to orbital decompression because of marked residual proptosis. At clinical presentation, none of the patients had diffuse PTM: nine showed a nodular PTM, while a plaque-like or an elephantiasic form was observed in four patients and one patient respectively (Table 1). Mean PTM duration was 58.7±20.8 months. None of the patients underwent local therapy for PTM previously. One patient, who had PTM localized on the metatarsal region, had been treated four years previously for active GO with intravenous methylprednisolone (cumulative dose 7.5 g). During this treatment, the PTM did not improve but in fact progressively worsened, and for this reason the patient underwent mesotherapy.
Patients 1–5 were treated with mesotherapy.
GD, Graves' disease; HT, Hashimoto's thyroiditis; eleph., elephantiasic; TRAbs, thyrotropin receptor binding antibodies; MMI, methimazole; LT4, levothyroxine; GO, Graves' orbitopathy; CAS, GO Clinical Activity Score; NOSPECS, GO Severity Score.
High serum levels of TRAbs (47.3±8.8 U/L, normal value <1.5) were found in all PTM patients in whom they were measured (10 of 14). PTM was asymptomatic in 9 of 14 patients, and was diagnosed after close examination of the skin. The five patients submitted to therapy were those complaining of itching, skin irritation, and difficulties wearing shoes, along with relevant cosmetic concerns. Images of PTM at baseline in two patients undergoing steroid treatment are shown in Figure 1A and C. Response to treatment was clinically assessed at two to three months in all patients after each cycle of DXM, and long-term follow-up was one year in one patient and seven years in three patients, while one patient was lost to follow-up after the short-term assessment due to the onset of major neurological disease (Fig. 2 and Table 2).
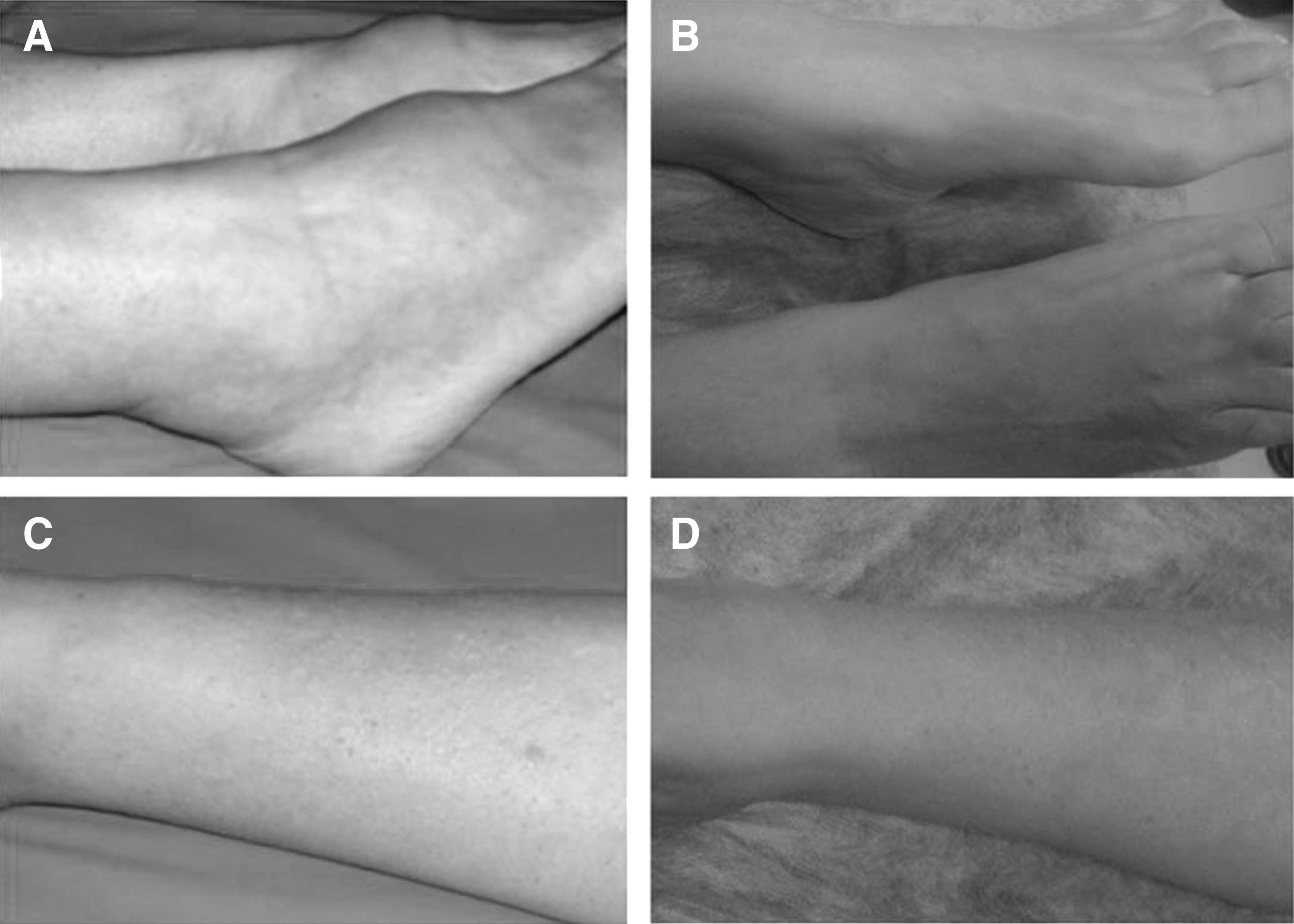
Clinical appearance of pretibial myxedema (PTM) before and after treatment. PTM of the pretibial region in patient 1 before
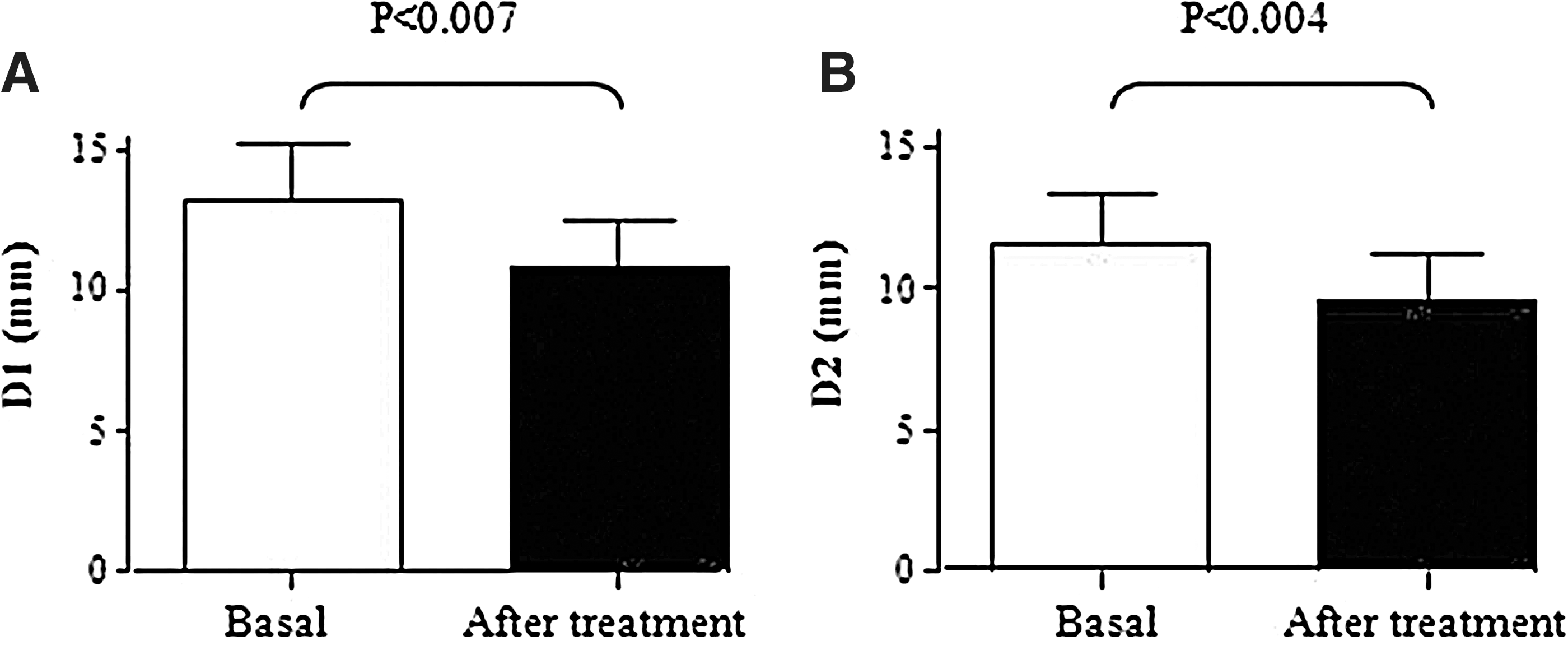
Changes in pretibial skin thickness, as assessed by ultrasound in five patients with PTM treated with injections of DXM. Changes in D1
Patient #4 was studied for one year after treatment. Patients #1, #3, and #5 were studies for seven years after treatment and showed a further reduction of D1 and D2.
D1, skin layer including the epidermis, the dermis, and the subcutaneous tissue; D2, skin layer including only the subcutaneous tissue up to the muscular fasciae; ST, short-term assessment 2–3 months post-therapy; LT, long-term assessment at one and seven years post-treatment.
Thyroid and ophthalmological assessment
Serum TSH, free triiodothyronine, and free thyroxine concentrations and anti-thyroid antibody levels (antithyroglobulin [TgAbs] and antithyroperoxidase [TPOAbs]) were measured with an automatic immunoassay system (AutoDELFIATM; Perkin Elmer™ Life Sciences [Wallac Oy], Turku, Finland) while serum TRAbs, detected as serum TSH binding inhibitory immunoglobulins (TBII), were measured using a second-generation immunoassay (Lumitest TRAK human; Brahms AG, Henningsdorf/Berlin, Germany).
Ophthalmological assessment included lid fissure and Hertel measurements, color vision, cover test, Hess–Lancaster screen, visual acuity, tonometry, fundus examination, and visual field in order to assess the clinical activity score (CAS) (20) and severity of endocrine ophthalmopathy, according to a recent consensus paper (21).
PTM ultrasonography
Ultrasound (US) study at a depth of 15–20 mm of the pretibial skin region was performed by a US scanner (Esaote/Hitachi, Genoa, Italy) equipped with a 13 MHz probe. The same radiologist performed US on consecutive patients as they were referred by our endocrine unit. Patients were not asked if they had received any treatment and were examined two months or more after DXM injections, without any US or photographic images of previous assessment available to the investigator. The accuracy of this technique in comparing patients with clinically overt PTM with normal controls, as well as GD patients without skin involvement, has been previously validated by our group (12) and recently reproduced by others (22). In our study, two skin layers were identified and measured (Fig. 3A): D1, which includes the epidermis, the dermis, and the subcutaneous tissue; and D2, which only includes the subcutaneous tissue up to the muscular fasciae. A schematic representation of skin layers identified and measured as D1 and D2 are summarized in Figure 3A. At each assessment, skin lesions were scanned entirely, and D1 and D2 were measured in the area of maximal thickness. Although skin lesions were variable, including the metatarsal skin in one patient and the posterior region of the leg in another patient, we only considered the maximal thickness of the more typical pretibial region for the purpose of a more homogeneous statistical analysis. In patients who underwent mesotherapy, skin lesions were assessed by US two to three months after each cycle of treatment and on long-term follow-up at the same time as clinical evaluation. The US study of the pretibial skin region was also performed in five patients with GD without PTM and 11 controls.
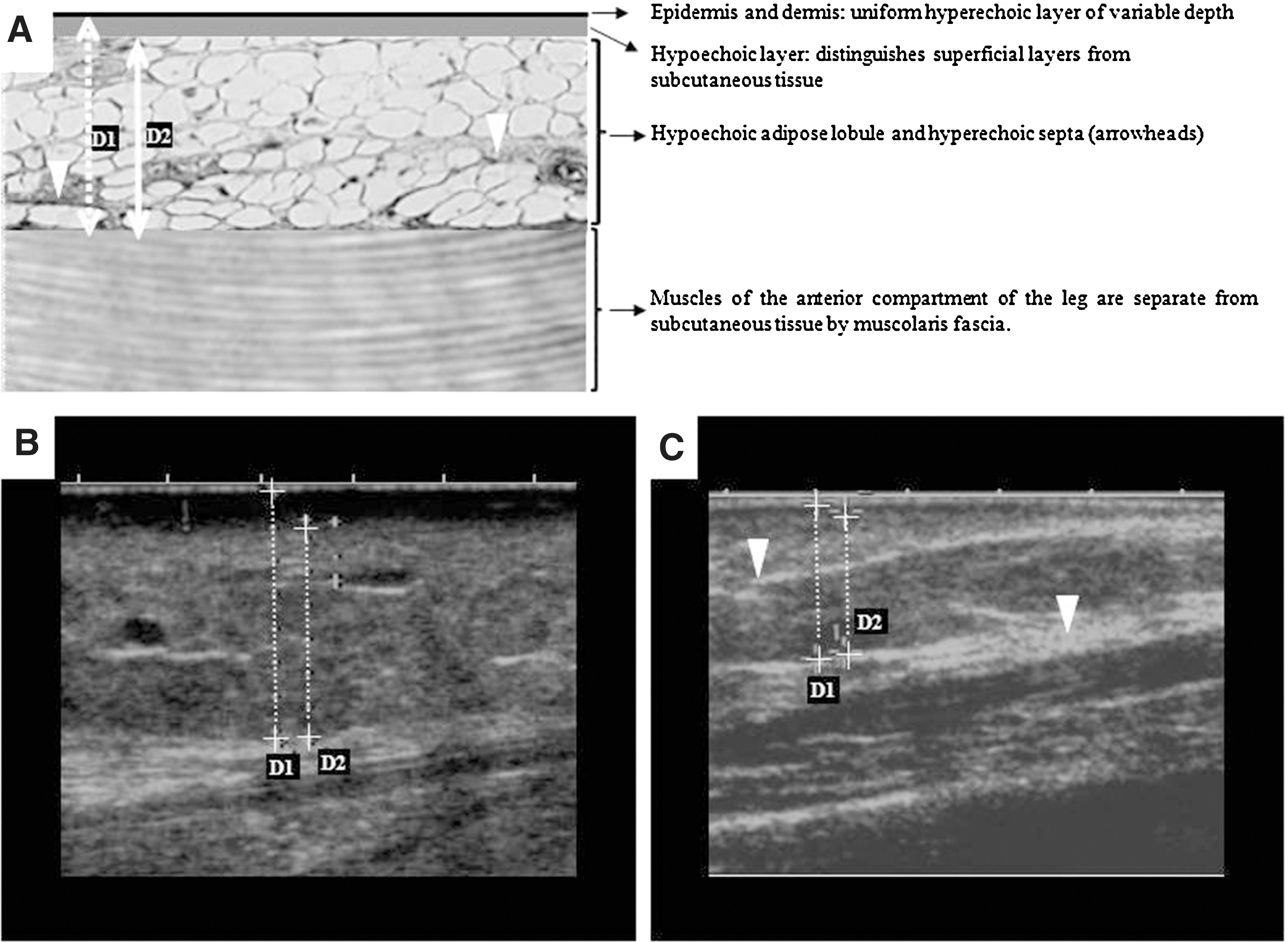
Ultrasound assessment of the pretibial skin area in pretibial myxedema. Schematic representation of skin layers
Therapeutic protocol
After baseline US scanning of the pretibial region, five patients were treated with intradermal steroid therapy. Only one patient had been previously treated (nine months before) with i.v. methylprednisolone pulses for active GO. Inclusion criteria for treatment were the presence of symptoms, more severe form of PTM, relevant cosmetic concerns, and no previous specific therapy for PTM.
A solution of 3 mL of dexamethasone (DXM; 1.3 mg/mL) and lidocaine (6.7 mg/mL) in saline was injected in each affected leg by multiple pricks, moving from the surrounding unaffected skin to the center of the lesion. Specifically, at each treatment session, we performed 2 pricks/cm2 in the unaffected peripheral area of the PTM lesion and 3–4 pricks/cm2 in the nodule or plaque. We treated the entire nodular or plaque skin area in one session. At the end of the procedure, the treated area was covered with a sterile dressing, which the patient removed ∼2 h later. The mesotherapy needles employed measured 0.4 mm×4 mm (27-gauge), allowing for deep intradermic injections. Each patient received three consecutive treatments at one-week intervals for a total cumulative dose of 12 mg of DXM per leg. Two of the five patients (#1 and #4), affected with the more severe forms of PTM, had a partial therapeutic response after the first three cycles of treatment, and were therefore submitted to another two cycles at four and six weeks after the initial treatment.
Statistics
One way analysis of variance and paired t-tests were used (SPSS 8.0 for Windows) as appropriate. Since the involvement of pretibial skin was bilateral and rather symmetrical, for statistical analysis, D1 and D2 were calculated as the mean of the measurements of the two legs. All values are reported as mean±SE.
Results
Baseline pretibial skin US measurement
Mean D1 was 13.2±2.6 mm in PTM patients and 6.55±0.38 mm in GD patients without PTM (p=0.0008) and 6.6±0.43 mm in controls (p=0.0003). Mean D2 was 11.5±1.8 mm in PTM patients and 5.1±0.70 mm in GD patients without PTM (p=0.005) and 5.2±0.45 mm in controls (p=0.0002; Table 3). No significant differences were found between D1 and D2 values of GD patients without PTM and normal subjects, thus confirming the usefulness and the sensitivity of skin US in the diagnosis of PTM.
PTM, pretibial myxedema.
Response to treatment
In the patients treated with intradermal steroid mesotherapy, two to three months posttherapy, US assessment of the pretibial skin lesion showed a significant reduction of D1 to 10.8±1.7 mm (p<0.007) and D2 to 9.5±1.7 mm (p<0.004; Fig. 2 and Table 2). A further decrease of D1 and D2 was observed in the longest follow-up in four out of five patients. Specifically, one patient was lost to longer follow-up; one patient (#4) showed a reduction of 31% and 27% in D1 and D2 respectively at the one-year follow-up (Table 2); three patients (#1, #3, and #5) were studied seven years after treatment, and mean reductions of 40% and 29% in D1 and D2 (Table 2) were observed. In these four patients, skin improvement was evident at the first posttherapy clinical assessment, and no further treatment was planned because the patients were satisfied with the outcome. In addition, we did not observe long-term skin atrophy or changes in skin color within the treated areas on follow-up. The skin pictures of two of these patients (#5 and #3) before (Fig. 1A and C) and after therapy (Fig. 1B and D) clearly show the effect of treatment: Patient #5 had PTM localized in the metatarsal area and had to wear her shoes open and of one or two sizes larger than before the onset of her skin alterations; Patient #3 had a nodular form of PTM on her leg. In both patients, treatment restored normal skin appearance. Figure 3 shows the skin US study before (Fig. 3B) and after (Fig. 3C) therapy in a patient with the elephantiasic form (Table 2, Patient #4). This patient received another two injections of DXM at four and six weeks and had, at baseline, a typically enlarged hypoechoic layer in the dermis, which decreased after therapy. Treatment was well received by all patients, who reported subjectively progressive reduction of skin itching in the lesion and improvement of the cosmetic appearance. The patients only complained of moderate pain upon injection of the therapeutic solution, particularly in the cases when nodular or plaque lesions were treated. They did not require additional therapy for pain.
Over a follow-up of between one and seven years, treated pretibial skin lesions did not show appearance of either atrophic or lumpy skin in any of the patients.
Discussion
In this preliminary study, we have performed a novel treatment for PTM by injecting steroids in the dermis with mesotherapy needles. We have obtained a significant and permanent reduction of pretibial skin dermal infiltration and improvement in patient discomfort. Steroid therapy is generally used in severe forms of PTM based on its anti-inflammatory/immunosuppressive effect. Glucocorticoids also downregulate the synthesis of GAGs that are the main component of PTM (23). Oral pentoxifylline has also been employed in two studies, in association with topical (24) or intralesional (25) steroids. In the former study, a complete resolution of the skin lesions was observed at four months, while the PTM receded earlier (three months) in the latter patient, with only a few residual slightly indurated plaques. While topical application of steroids with occlusive dressing has long been considered the treatment of choice (2,7), local injections of steroids have been used in the past in an attempt to obtain a more localized effect in the intradermis skin layers, while avoiding the adverse effects of systemic administration. This treatment modality has been abandoned, however, due to occurrence of skin atrophy and/or changes in skin color in the treated area caused by atrophy of subcutaneous fat. Moreover, relapse of myxedema on the injection sites has also been reported (15).
Mesotherapy is a specific method of drug delivery, consisting of intra- or subcutaneous injections, for the treatment of localized pathological conditions. It was originally developed for the management of pain in arthritis, tendonitis, neuralgias, and other musculoskeletal diseases (26 –30). Solutions of different drugs have been employed, including, among others, nonsteroidal anti-inflammatory drugs, benzodiazepines, and local anesthetics. Although it has become most popular for the application of various cosmetics, mesotherapy has only anecdotally been reported to be effective, and to our knowledge, there are no clinical trials designed to test the efficacy of this therapeutic modality. For that reason, it is often considered as a nonconventional medical technique. In the present study, we aimed to experiment with local steroid administration by mesotherapy, since we expected it to be well tolerated and to bear a very low risk of side effects such as postinflammatory hyperpigmentation, edema, or ecchymoses.
Corticosteroids have been previously administered by mesotherapy only in combination with acyclovir for the treatment of herpetic neuralgia, and no dosage or treatment protocol have been described (26). In this study, the concentrations of DXM in the therapeutic solution and the injection protocol were based on our personal experience, due to the lack of previous reports in the literature. Although, to some extent, locally injected DXM might be absorbed and act systemically, we believe that the therapeutic response of PTM is unlikely due to a systemic effect in these patients. The total dose of DXM administered to our patients was 24 mg, and is in fact comparable to as little as 80 mg of orally administered prednisone and to 60 mg daily of orally administered prednisolone tapered down in three months in the systemic therapeutic approach (7). Moreover, the patient with PTM treated for active GO with i.v. methylprednisolone did not show clinical improvement of the skin lesion. She only had a significant reduction in skin thickness of 60% for D1 and 51% for D2 in the metatarsal region after mesotherapy with DXM.
Our treatment was well accepted, as patients only reported moderate pain upon injection. No changes in skin color, skin degeneration, or atrophy were observed, in contrast with what has been reported after local steroid injections with standard needles. The therapy produced significant improvement of PTM even at the first posttherapy clinical assessment, with reduction of edema and skin hyperemia, and no further therapy was required. In addition, US evaluation of the pretibial skin area, as previously reported by our group (12) and recently confirmed by others (22), showed a significant reduction in skin thickness: up to 15% at the level of the dermis and up to 22% in the subcutaneous tissues layers two months posttherapy, and as much as 40% and 29% respectively at long-term follow-up. All patients were satisfied with the outcome, since they all reported a subjective improvement in leg appearance, associated with a reduction in the thickness of the plaques or the nodules.
These results have to be considered preliminary because of the small number of patients treated. These data, nevertheless, suggest that the use of mesotherapy can be effective in PTM by inducing a stable improvement of symptoms and signs and a significant reduction in the characteristic infiltration of the pretibial skin region.
Footnotes
Acknowledgments
This work was supported in part by MURST, Rome, and by Fondazione Cà Granda, IRCCS, Milan, Italy.
Author Disclosure Statement
No competing financial interests exist.