
Abstract
Background:
Massive amyloid deposition in the thyroid to the point of goiter formation is rare. Here we describe the clinical presentation and outcomes of five patients with amyloid goiter (radiographically confirmed goiter in the context of tissue-proven thyroid amyloidosis) encountered in the past 23 years at our institution.
Methods:
Mayo Clinic archives were searched between 1987 and 2010 for a diagnosis of “thyroid amyloidosis,” “amyloid deposits,” “amyloid deposition,” or “liquid chromatography consistent with amyloid.” Inclusion criteria were symptomatic thyromegaly; tissue confirmation of thyroid enlarged by amyloid deposits; and radiologic confirmation of thyroid enlargement.
Results:
Five patients were identified who met all inclusion criteria. Amyloid goiter etiology included both primary and secondary amyloidosis, and the goiters ranged in weight from 50 to 130 g each. Diagnosis was made by fine-needle aspiration biopsy with Congo red staining and, if needed, spectrophotometry. All five patients had histories of persistent hoarseness for several years before presentation with compressive symptoms referable to their enlarging thyroids, and all had some degree of thyroid dysfunction (both hypothyroidism and hyperthyroidism) by the end of our follow-up period, which ranged from 5 months to 13 years. Two patients underwent surgical interventions, two were managed conservatively, and in one, the goiter shrank after systemic therapy for amyloidosis.
Conclusions:
Our clinical observations suggest slower goiter progression and a higher prevalence of thyroid dysfunction than previously thought.
Introduction
Here, we present a case series of five patients, illustrating the history before evaluation, radiographic findings, tissue specimen, thyroid function, and clinical outcomes associated with this rare presentation of amyloidosis.
Methods
Mayo Clinic archives between 1987 and 2010 were searched for a diagnosis of “thyroid amyloidosis,” “amyloid deposits,” “amyloid deposition,” or “liquid chromatography consistent with amyloid.” The study period was selected on the basis of the best availability of the tissue registry and clinical databases. Inclusion criteria were symptomatic thyromegaly, tissue confirmation of thyroid enlarged by amyloid deposits, and radiologic confirmation of thyroid enlargement. Follow-up was conducted by medical record review and telephone interviews in September 2011. Patients with a diagnosis of thyroid medullary carcinoma were excluded.
The Mayo Clinic Institutional Review Board provided exempt approval for this study. The five patients identified had provided permission for their medical records to be used for research purposes. Written consent was not necessary because patient data were de-identified.
Results
Patient characteristics
Five patients were identified who met the inclusion criteria (Table 1). Each patient had either computed tomography (CT) or ultrasonography of the neck performed. Patient 4 had a surgical biopsy specimen, and the other four patients had fine-needle aspiration (FNA) biopsy specimens with Congo red staining; mass spectrometry also confirmed the diagnosis in patients 2 and 5. Patients 2, 4, and 5 had secondary amyloidosis, patient 3 had primary amyloidosis, and patient 1 had amyloidosis of uncertain origin (Table 1). The mean age at the time of initial local compressive symptoms was 52.6 years (range 33–85 years), and the mean age at the time of presentation to our institution was 57.2 years (range 46–87 years). Patients 2 and 4 reported a family history of thyroid disease.
AA, secondary amyloidosis; AL, primary amyloidosis; MALT, mucosa-associated lymphoid tissue.
Symptoms preceding evaluation for compressive goiter
Patients 2, 3, and 4 had a history of persistent hoarseness several years before the diagnosis of goiter, which may have been a result of thyroid enlargement. In patients 1 and 4, who eventually underwent thyroidectomy, considerable difficulty was encountered in identifying and dissecting the recurrent laryngeal nerve. Patients 1, 2, and 5 had no thyroid biochemical analyses before compressive symptoms developed, but patients 2 and 3 had symptoms of fatigue; patient 4 had a diagnosis of hypothyroidism and patient 3 had a diagnosis of thyrotoxicosis (Table 2). The average duration of thyroid-related symptoms before the diagnosis of an amyloid goiter was 2 years. Patients 3 and 4 had symptoms of compressive thyromegaly that preceded the diagnosis of systemic amyloidosis. In the 2 patients with secondary amyloidosis, the diagnosis of amyloidosis preceded the onset of compressive thyromegaly. In the patient with primary amyloidosis, the amyloid goiter was diagnosed within months of the initial diagnosis of systemic amyloidosis. Patient 1 underwent an upper endoscopy that revealed severe compression of the esophagus and a tracheal CT that also showed compression. Patient 4 had pulmonary function testing that revealed the presence of a fixed extrathoracic airway obstruction.
FT4, free thyroxine; NA, not available; RAI, radioactive iodine; TFTs, thyroid function tests; TPO Ab, thyroid peroxidase antibody; TSH, thyrotropin.
Documentation of enlarged thyroid
A clinically enlarged thyroid was diagnosed, and as estimated by palpation, the goiters ranged in weight from 50 to 130 g. Ultrasonographic findings included heterogeneous parenchyma and diffusely enlarged thyroids (Fig. 1). CT findings included diffusely enlarged thyroids with diffusely decreased density on precontrast images (Fig. 2).
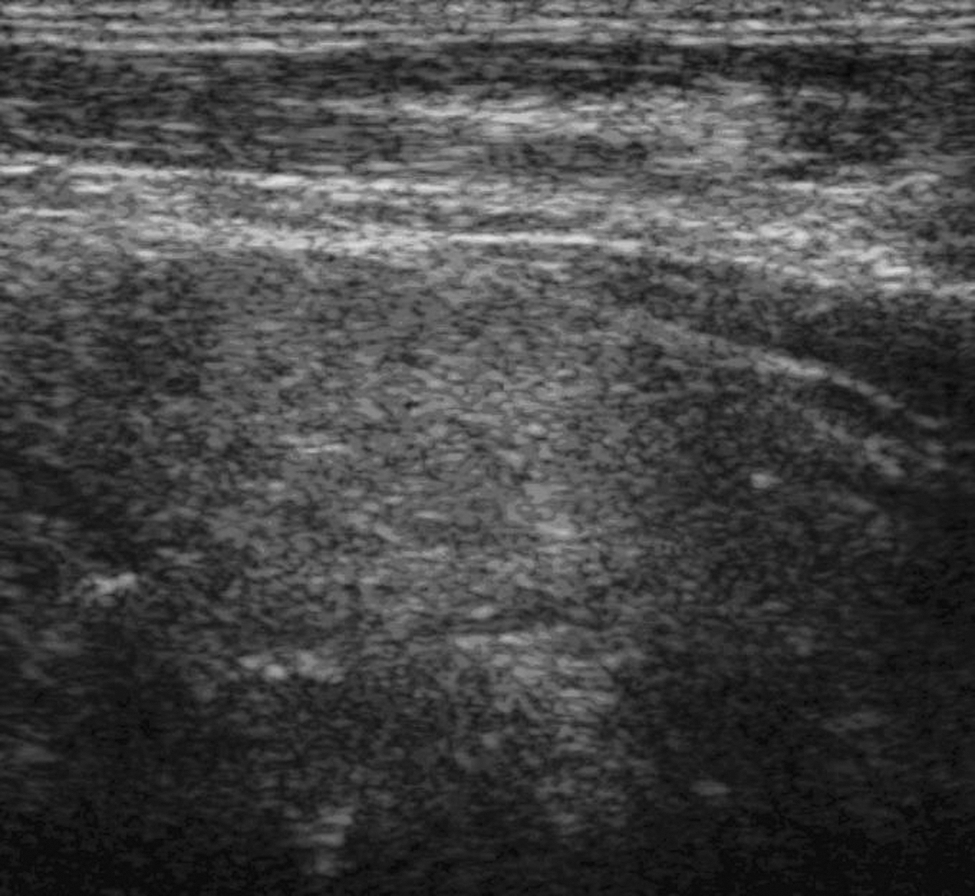
Ultrasonography from patient 1 revealed heterogeneous, diffuse enlargement of the thyroid with parenchymal hyperechogenicity. The right lobe of the thyroid is shown.

Computed tomography of the neck of patient 4 revealed massive asymmetric thyroid enlargement and coarse calcification with tracheal compression.
Tissue diagnosis
Patients 1, 2, 3, and 5 had FNA biopsies with Congo red staining (Fig. 3); patients 1, 2, and 5 had core biopsies. These biopsies were performed to evaluate for amyloid infiltration and exclude other infiltrative thyroid conditions. The location of the biopsy sampling was left to the discretion of the physician performing the procedure; in the absence of a discrete nodule, a random biopsy of the parenchyma was performed. Mass spectrometry confirmed the diagnosis of amyloidosis in patients 2 and 5. Surgical specimens were available from patients 1 and 4. In patient 1, the surgical specimen weighed 130 g and revealed diffuse oncocytic changes with diffuse amyloid infiltration. The surgical specimen of patient 4 showed findings consistent with low-grade mucosa-associated lymphoid tissue lymphoma with extensive amyloid deposition.

Thyroid function
By the time these patients presented to our institution, patients 1, 2, and 4 had hypothyroidism (two had been evaluated for fatigue and received a diagnosis of hypothyroidism 2 years before goiter formation; in the third patient, hypothyroidism developed after a previous thyroid surgery) (Table 2). Patient 3 had been diagnosed with Graves' thyrotoxicosis managed by methimazole several months before the diagnosis of goiter. Patient 5 was euthyroid, but subsequently developed subclinical hypothyroidism. Thyroid peroxidase antibodies were available only for patients 3 and 5, and both were normal, at less than 20 and 1 IU/mL, respectively (reference value <9 IU/mL). By the end of our follow-up period, all patients had some degree of thyroid dysfunction.
Management and outcome
Patient 1 had received 60 mCi at another institution to reduce the size and compressive symptoms of the goiter (no scan or uptake was available before treatment); this resulted in a transient improvement in dysphagia symptoms for 6 months. However, compressive symptoms recurred and worsened over the next 6 months, and he underwent a near-total thyroidectomy with cricopharyngeal myotomy, which was complicated by bilateral vocal cord paralysis. Follow-up revealed that he died 8 years later of unknown causes (Table 3).
Two patients underwent conservative management, with continued observation and levothyroxine replacement. Patient 2 reported that her goiter continued to enlarge during the 3 years of treatment, but her compressive symptoms of hoarseness and intermittent dysphagia were stable; she denied any supine dyspnea, and her main concern was cosmetic in nature. Patient 5 had a relatively stable goiter weight of 80–90 g about 16 years after the initial goiter diagnosis, and he eventually died of complications related to amyloidosis.
Patient 3 underwent stem cell transplantation for systemic amyloidosis and high-dose dexamethasone therapy; her goiter shrank from an estimated 50 g to 30 g. Follow-up 6 years after the goiter was diagnosed and 5 years after dexamethasone revealed stability of her goiter size. She has continued to have transient hoarseness but denied any dysphagia or supine dyspnea.
Patient 4 had been diagnosed with a goiter in her early 30s and had undergone debulking surgery to relieve compressive symptoms 15 years after her initial diagnosis. The goiter recurred 5 years after the first surgery, and because of symptoms of worsening dysphagia, she underwent a right thyroid lobectomy and isthmectomy. Because of extensive adhesions, the left thyroid lobe was left intact to preserve the recurrent laryngeal nerve. At follow-up 12 years after her second surgery, she reported that the goiter had become visibly larger, and she continued to have intermittent dysphagia.
Patient 5 had been diagnosed with amyloidosis attributable to Crohn's disease. He was in his mid-40s when he presented to our institution with a progressively enlarging goiter; examination revealed a thyroid of about 80–90 g. Thyroid FNA biopsy with mass spectrometry confirmed the diagnosis of an amyloid goiter. During the next decade, he remained biochemically and clinically euthyroid, although with worsening local pressure symptoms from the goiter. Initially, surgical intervention was not sought by the patient because he considered the symptoms tolerable. Thirteen years after the patient's initial diagnosis, subclinical hypothyroidism developed. He died shortly thereafter from complications associated with systemic amyloidosis.
Discussion
Clinically recognized cases of amyloidosis resulting in thyromegaly are rare. However, amyloid deposits in the thyroid are common. In 1949, Dahlin (7) performed autopsies on 44 patients with primary and secondary amyloidosis and found amyloid in the thyroid in 80% of cases with primary amyloidosis and 59% of cases with secondary amyloidosis, but “clinical enlargement of these organs was not observed” (8).
It is likely that many cases of mild thyroid enlargement caused by amyloid deposits remain undiagnosed if they are clinically silent. Some of the case reports in the literature included cases identified at autopsy, suggesting that they were not associated with clinical signs (6). In this series, FNA biopsies were performed in each patient to evaluate for amyloid infiltration and exclude other infiltrative thyroid conditions. If the inclusion is limited to patients with histologic confirmation of the presence of amyloid, as well as radiographic confirmation of thyroid enlargement, it is apparent that this entity is very rare.
The growth of amyloid goiters may not always be rapid, but may continue to progress over many years. Although many of the case reports in the literature involve acutely enlarging goiters, it is likely that there is a reporting bias, with a predilection for the most impressive, fulminant cases. In these reported cases of an acute, massive enlargement of the thyroid, the goiter had likely been present and progressing for a period, but it was clinically recognized only when a symptomatic threshold was breached.
Compressive symptoms and thyroid dysfunction are fairly common (9 –16). Long-term follow-up of these cases has provided us with the ability to observe the natural history of this disease process, with follow-up ranging from 6 to 31 years. In all three patients whose thyroid was left intact, thyroid dysfunction developed at some point during the follow-up period: one had hypothyroidism, one had thyrotoxicosis, and one had subclinical hypothyroidism.
CT and ultrasonography images are characteristic, and enlargement is frequently diffuse and bilateral (17). Fat deposition is often seen in amyloid goiters (Fig. 3A–C), which accounts for the increased echogenicity seen on ultrasonography (Fig. 1) and the low attenuation values seen on CT (Fig. 2) (17 –24).
Diagnosis is made by FNA biopsy with Congo red staining and, if needed, spectrophotometry (15,25 –27).
Patient 1, who had undergone radioactive iodine treatment at another institution, had transient relief from dysphagia but eventually required surgical intervention. Surgical intervention may occasionally be needed but can be technically difficult. Colchicine therapy has been described in the treatment of goiters related to secondary amyloidosis, with one case of progressive enlargement when the colchicine was stopped (28). In that patient, reinitiation of colchicine did not halt goiter growth, and therefore surgery was necessary (28). In some patients, partial regression can occur with therapy of amyloidosis, as was observed in our patient 3, who was previously described elsewhere (4).
Our observations suggest that clinically significant amyloid goiters are rare, goiter progression may be slower than previously thought, and thyroid dysfunction is relatively common.
Footnotes
Author Disclosure Statement
The authors declare that no competing financial interests exist.