
Abstract
Background:
Hypothyroidism is treated with oral levothyroxine. Some patients fail to attain adequate control because of poor compliance. Delaying breakfast to take levothyroxine on an empty stomach can decrease adherence to hypothyroidism treatment. The objective of this study was to evaluate whether administering levothyroxine with breakfast can maintain thyrotropin (TSH) levels in the therapeutic range, without major clinical changes.
Methods:
A prospective, randomized, open-label, crossover study was conducted to compare usual levothyroxine administration while in a fasting state with administration during breakfast. From September 2008 to April 2009, 45 patients with primary hypothyroidism who received levothyroxine were recruited. The patients completed 180 days of the protocol and were randomized to 90 days of each levothyroxine administration regimen (while fasting or with breakfast). Clinical and biochemical analyses were performed at baseline and on days 45, 90, 135, and 180. The primary outcome was TSH level.
Results:
Forty-two patients completed the protocol. The TSH level was higher for levothyroxine administration with breakfast than while fasting (2.89 vs. 1.9 mIU/L, p=0.028). Uncontrolled hypothyroidism (TSH ≥3.5 mIU/L) occurred regardless of the type of levothyroxine administration (p=0.26). No risk factors were identified for TSH elevation.
Conclusions:
Levothyroxine administration with breakfast could be an alternative regimen for patients who have adherence difficulties due to the need for delaying intake, and is more likely to cause variability in the TSH level, meaning the patient should be followed more closely. For patients in whom a specific serum TSH goal is important, taking levothyroxine while fasting is recommended.
Introduction
The recommended LT4 daily dose is 1.5–1.6 μg/kg body weight, and serum thyrotropin (TSH) represents the best marker for assessing the proper LT4 dose. The therapeutic target should be individually tailored based on the patient's diagnosis, age, and coexistent diseases (3,4).
However, a number of patients fail to show a clinical and biochemical response to the expected dose of LT4. Most frequently, the apparent ineffectiveness of LT4 therapy can be explained because of poor compliance (5,6). Additionally, impaired absorption can cause a lack of a response to LT4 treatment, due to malabsorption disorders or concomitant use of certain medications (7). Several studies have shown resistance to treatment with oral LT4 in patients with celiac disease (8,9), inflammatory bowel disease (7), lactose intolerance (10), Helicobacter pylori infection (11,12), and atrophic gastritis (13). Medications that are known to interfere with LT4 absorption when coadministered include calcium carbonate (14), ferrous sulfate (15), aluminum hydroxide (16), bile acid resins (17), sucralfate (18), raloxifene (19), sevelamer (20,21), and chromium picolinate (21).
The absorption and bioequivalence of different commercial LT4 preparations might be variable. Hence, switching from one compound to another may also result in alterations in the TSH level and in the adequate control of hypothyroidism (22,23).
The influence of food intake on LT4 absorption was first reported by Wenzel et al. (24). In their study, LT4 absorption was significantly better while fasting than with simultaneous food intake (79.3% vs. 63.9%, p<0.001). Benvenga et al. examined five patients in whom LT4 therapy failed to achieve the target serum TSH through ingestion of LT4 15 minutes prior to breakfast. Compared to euthyroid and hypothyroid controls, absorption studies demonstrated a delayed time to peak LT4 absorption with impairment in the early phase of the absorption. After a month of postponing breakfast for at least 60 minutes after LT4 ingestion, patients obtained a normal TSH level (25). In addition, there are studies showing that fiber supplements (26), soy protein (27), coffee (28), and grapefruit juice (29) can also reduce LT4 absorption.
Considering all of the mentioned factors that can interfere with LT4 absorption, the current recommendation is that LT4 should be taken on an empty stomach, in the morning, 30 to 60 minutes prior to breakfast. However, for some patients, this strict guidance affects compliance, considering that waiting until breakfast may interfere with the patient's daily routine. Because taking LT4 on an empty stomach in the morning can decrease compliance and interfere with the patient's daily routine, alternative therapeutic regimens have been studied.
A Dutch group has been studying the effects of changing LT4 intake to bedtime. First, in a pilot study with 11 patients, a significant improvement in thyroid hormone levels (TSH decreased from 5.1 to 1.2 mIU/L, and free T4 (FT4) and T3 levels increased) was observed when LT4 was taken at bedtime (30). Then, a randomized, double-blind crossover trial with 90 patients confirmed these findings (31). Compared to morning intake, there was a mean decrease in TSH of 1.25 mIU/L, a mean increase in FT4 of 0.07 ng/dL, and an increase in T3 of 6.5 ng/dL when LT4 was taken at bedtime.
Bach-Huynh et al. evaluated the effect of the timing of LT4 administration in relation to food on serum TSH (32). They studied 65 patients receiving LT4 for hypothyroidism or thyroid cancer, and randomized them to different treatment regimens, with intake of the LT4 while fasting, at bedtime, and with breakfast. Nonfasting regimens of LT4 administration were associated with higher and more variable serum TSH concentrations. The mean TSH was 1.06 mIU/L when LT4 was administered while fasting, 2.19 mIU/L when taken at bedtime, and 2.93 mIU/L when taken with breakfast (32).
Recently, our group published data about weekly LT4 as an alternative therapeutic option. A randomized, crossover study assigned 14 patients to daily or weekly doses of LT4 (33). The weekly treatment led to a transient increase in the FT4 level (1.91 vs. 1.16 ng/dL, p<0.01), without hyperthyroidism or cardiac symptoms on an echocardiographic evaluation. After six weeks, no statistically significant difference was found in the TSH level (3.45 vs. 1.87 mIU/L, p>0.05).
Considering that LT4 administration with breakfast could be a more convenient treatment scheme, even with the possibility of mild elevations of TSH, this study was designed to evaluate whether LT4 administration with breakfast may maintain TSH in an acceptable therapeutic range, without significant clinical changes.
Patients and Methods
Study design
This prospective, randomized, controlled, crossover study evaluated patients with primary hypothyroidism receiving substitutive doses of LT4 and the effect on the clinical and biochemical control (primary endpoint TSH level) of their disease comparing the usual LT4 administration while fasting with administration during breakfast.
Patients
Forty-five patients (5 males, 40 females; mean age 45.9±10.1 years, age range 28–65 years) with primary hypothyroidism receiving LT4 therapy were recruited at our center between September 2008 and April 2009.
The inclusion criteria were as follows: (i) age range between 18 and 65 years; (ii) patients with primary hypothyroidism of any cause, diagnosed and treated with LT4 for at least six months; (iii) patients with compensated disease, defined by a TSH level between 0.5 and 3.5 mIU/L; and (iv) patients with stable disease who had been on the same dose of LT4 for three months before the study enrollment.
The exclusion criteria were as follows: (i) pregnancy or lactation; (ii) patients with a serum TSH less than 0.5 or greater than 3.5 mU/L at the time of recruitment; (iii) patients with serious and debilitating chronic diseases, such as cardiac, pulmonary, gastrointestinal, and renal disorders or malignancy; (iv) use of medications that could potentially interfere with either the hypothalamic–pituitary–thyroid axis, the metabolism and peripheral action of thyroid hormones, or with LT4 absorption, such as calcium carbonate, ferrous sulfate, aluminum hydroxide antacids, bile acid resins, sucralfate, raloxifene, omeprazole, amiodarone, phenytoin, carbamazepine, and rifampicin; (v) patients with malabsorption disorders, including celiac disease, inflammatory bowel disease, chronic pancreatitis, and intestinal bypass surgery; and(vi) patients with coronary disease or cardiac arrhythmias.
Only patients taking two LT4 brands were recruited (Puran T4®, Sanofi-Aventis, São Paulo, Brazil; and Euthyrox®, Merck Serono, Rio de Janeiro, Brazil). The drugs were supplied by the respective companies for the study to ensure that the patients would take the same brand and batch during the study period (six months) and avoid potential effects of the variable bioequivalence.
The study protocol was approved by the local Institutional Human Research Ethics Committee, and all participants provided informed consent.
Methods
The patients completed 180 days on the protocol with 90 days of each LT4 administration regimen, that is, intake while fasting or during breakfast. The patients were randomized into two groups to determine the order for the treatment regimens. Group 1 included 23 patients who used LT4 after an overnight fast for the first three months, and then changed to taking LT4 with breakfast for the three final months; group 2 included 22 patients who used LT4 with breakfast for the first three months, and then took LT4 while fasting over the last three months. Each patient served as his or her own control.
During the fasting phase, in both groups, patients were instructed to wait for a minimum of 60 minutes between LT4 ingestion and subsequent breakfast, and during the breakfast phase, patients were told to take LT4 at the beginning of breakfast.
Routine thyroid function tests were used to determine study eligibility (TSH between 0.5 and 3.5 mU/L). Clinical and biochemical analyses were performed at baseline and at days 45, 90, 135, and 180. Telephone calls were conducted every 30 days to assess adherence to the treatment and possible complications. An interview was performed to evaluate the foods consumed at breakfast during the study period.
Biochemical analysis
Blood samples were drawn on the morning of each visit to measure TSH, free T4 (FT4), and total T3 (TT3), and were analyzed using a third-generation chemiluminescent immunoassay (Architect ci 8.200, Abbott Laboratories, Abbott Park, IL). The sensitivity of the assay for TSH is 0.0038 mIU/L. The normal reference ranges used were TSH=0.35–4.94 mIU/L, FT4=0.7–1.48 ng/dL, and TT3=58–159 ng/dL.
Food inquiry
To evaluate the dietary patterns for breakfast, all patients in the study answered a food inquiry. Patients reported food intake, using household measures, and later an assessment of the nutritional and caloric content of the meals was made using standard tables of food composition (34 –36).
Statistical analysis
Statistical analysis was performed using STATISTICA 8.0 software (Statsoft, Tulsa, OK). Data analysis was performed using analysis of variance (ANOVA) and Student's t-test. Analysis of the variable “TSH” was repeated using the Friedman nonparametric test. To compare the two treatment regimens, multiple regression analysis was applied, adjusting for age, sex, amount of calories at breakfast, and length of disease. The level of significance was set at 5%.
Results
Forty-five patients met the inclusion criteria and were randomized. Three patients withdrew during the course of the study; 42 patients completed the protocol, providing complete data for the 180 days of the study. Twenty-two started by taking LT4 in a fasting state (group 1), and 20 started by taking LT4 with breakfast (group 2). At enrollment, the clinical and laboratory characteristics were similar in the studied patients, with no statistically significant differences between the groups (Table 1).
Data are presented as mean ± standard deviation or as number (percent).
BMI, body–mass index; LT4, levothyroxine; FT4, free thyroxine; TT3, total triiodothyronine.
The food inquiry revealed that the most-consumed food items were coffee (88.1%), white sugar (81.0%), whole milk (71.4%), white bread (69.0%), margarine (59.5%), cheese (23.8%), savory biscuits (16.7%), nonfat milk (11.9%), whole wheat bread (9.5%), and fruits (9.5%). Patients consumed approximately 381±162 Kcal during a standard breakfast, consisting of carbohydrates (57.5%), fat (28.4%), protein (14.1), and nonsignificant fiber consumption. The breakfast calcium intake was 254.1 mg±62.6 mg.
During the study, there were no major clinical changes, and the investigated variables remained stable (blood pressure, heart rate, and weight), independent of the treatment regimen.
Regarding the laboratory parameters (Table 2), no significant changes occurred in TSH and FT4 levels in either group, independent of the form of LT4 administration. Changes in the TSH level were reanalyzed using the Friedman nonparametric test, and no significant variations were found (p=0.097 in group 1, and p=0.607 in group 2). There was significant variation in the serum TT3 in group 1. During the fasting phase (day 0 to 90), the TT3 remained stable (91.3 vs. 93.6 ng/dL, p=0.29). However, during the breakfast phase (day 90 to 180), TT3 decreased (93.6 vs. 84.9 ng/dL, p=0.026).
Data are presented as mean ± SD. Group 1: days 0–90, fasting phase; days 90–180, breakfast phase. Group 2: days 0–90, breakfast phase; days 90–180, fasting phase.
To compare hormonal variations at three different times in the study, an analysis of variance test was used. When a significant difference occurred between the three times, Student's t-test was used to evaluate differences between the two times (baseline vs. day 90, day 90 vs. day 180, and baseline vs. day 180).
In group 1, the TT3 differed significantly from day 90 to day 180 (p = 0.026).
TSH, thyrotropin.
When data from both groups were analyzed together, comparing the two therapeutic regimens (Table 3), TSH levels were higher with LT4 administration during breakfast than with conventional fasting (2.89 vs. 1.9 mIU/L, p=0.028), but they remained in the reference range.
Data are presented as mean ± SD (n = 42).
Additionally, LT4 administration with breakfast was more likely to cause fluctuations in serum TSH. When patients took LT4, in the fasting state, the mean variation in TSH was 0.27±2.88 mIU/L, and with breakfast, it was 1.01±2.91 (p=0.045).
At the end of both treatment regimens, there were patients with an elevated serum TSH≥3.5 mIU/L, which was considered to be above the ideal therapeutic range in this trial. When patients took LT4 on an empty stomach, six patients (14.3%) had a TSH ≥3.5 mIU/L compared to 10 patients (23.8%, p=0.26) who took the medication during breakfast. The TSH levels after 90 days of each treatment regimen are shown in Figure 1.
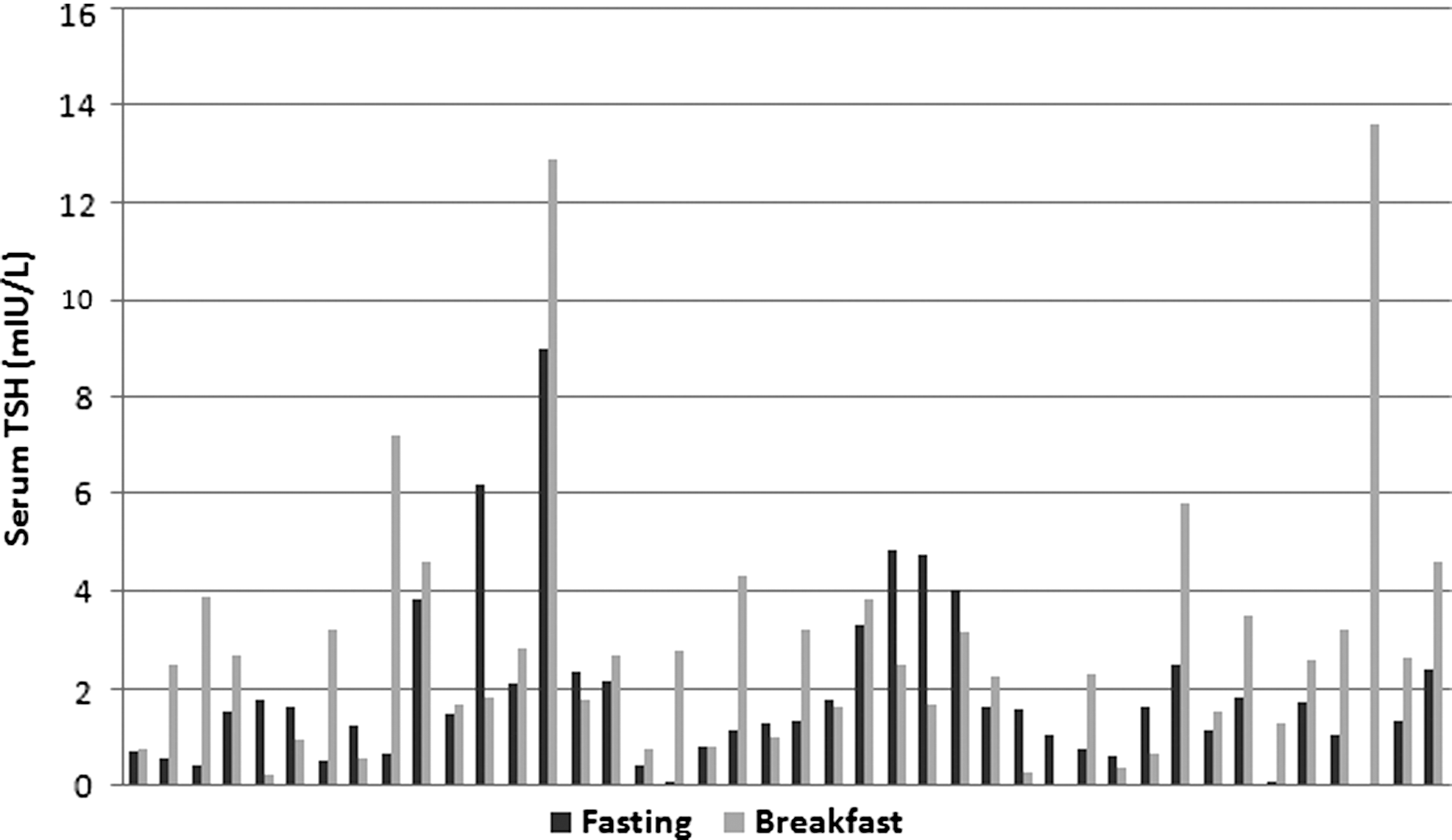
Serum thyrotropin concentrations for each participant after 90 days of taking levothyroxine while fasting (black column) or with breakfast (gray column).
In the breakfast regimen, comparing patients whose TSH increased to ≥3.5mIU/L with those who maintained a serum TSH in the range of 0.5 to 3.5 mIU/L, no differences were found when a multivariate analysis was performed that included age, sex, LT4 dose, duration or etiology of hypothyroidism, meal characteristics (caloric content or protein, carbohydrates, fat, fibers, and calcium content), and specific foods consumed during breakfast (coffee, milk, sugar, bread, biscuits, butter, fruits, and cheese).
All of the patients were asked at the end of the study about their timing preferences for LT4 administration. Seventeen patients (40.5%) chose the conventional fasting administration because they already had established a routine for LT4 intake, 14 patients (33.3%) preferred the breakfast regimen and 11 patients indicated no preference.
Discussion
This study shows that, despite a mild TSH elevation, TSH levels remained in an acceptable therapeutic range when LT4 was administered with breakfast. No significant clinical changes occurred due to this modification.
Our data show that, even under optimal conditions (fasting state, close follow-up), the control of hypothyroidism can be compromised, most likely due to poor compliance, but when LT4 is administered with food, the risk of raising the TSH is higher.
Analyzing individual patient data, some patients who took LT4 with breakfast had a stable TSH during the entire protocol (76.2%), while others experienced significant elevations in TSH levels (23.8%). When possible causes for an elevated TSH were investigated, no differences were found concerning individual patient characteristics or consumption of different foods. Therefore, in some patients, the intestinal absorption of LT4 may be unaffected by concomitantly ingested food, while in others it is affected. However, we did not identify any characteristic that can guide the clinical decision regarding which patients could receive LT4 with breakfast without the risk of raising the TSH level.
Another consideration is that the breakfast consumed by patients in this study (usual for the Brazilian population) is lighter than that consumed in other countries whose residents have a habit of eating more in the morning, including bacon and eggs. A breakfast with a higher caloric content or higher protein or fat content, as is frequent in North America, could cause greater interference in LT4 absorption.
As in our study, Bach-Huynh et al. conducted a three-period crossover design study that showed higher TSH levels, but still within the therapeutic range, when LT4 was taken with breakfast instead of the fasting state (32). In their study, the TSH concentrations were more stable when LT4 was taken on an empty stomach, and the nonfasting regimen was more likely to cause significant variations in TSH levels (0–19 mIU/L). In our study, the breakfast regimen resulted in an oscillation in TSH levels (0–13 mIU/L), but the fasting regimen also showed important variations in TSH levels (0–9 mIU/L), demonstrating that the timing of LT4 administration is not the only factor that can induce changes in TSH levels.
Considering that the breakfast regimen is more practical and convenient for some patients, it is possible that in the daily routine, outside of a research environment, our results would be different because the study intended to maximize adherence by close monitoring with telephone calls and frequent follow-up visits. Additionally, the profile of the patients who participated in the study protocol may be biased toward patients with good compliance.
Administering LT4 with breakfast can increase the TSH level, but if the serum TSH is not outside of the desired range, no major clinical consequences will occur. Moreover, taking LT4 with breakfast is a more convenient option, and in the case of a mild TSH elevation, increasing the LT4 dose could lower the TSH level.
In conclusion, our study shows that LT4 administration with breakfast is safe, well tolerated, and can be offered as an alternative regimen to patients who have adherence difficulties with taking LT4 while fasting. Because this therapeutic option is more likely to cause variability in TSH levels, the patient should be followed more closely, and the clinician should be aware that adjustments to the LT4 dose might be necessary. For patients in whom a specific serum TSH goal is important, such as pregnant women and patients with thyroid cancer or cardiac disease, the ingestion of LT4 while fasting is recommended to avoid the risk of iatrogenic subclinical thyroid disease. Large, double-blinded, randomized studies are necessary to confirm our results.
Footnotes
Acknowledgments
We would like to thank Dr. Karin Regina Luhm, Marcia Olandoski, and Ary Elias Sabbag Junior, who assisted us with the statistical analysis. We are grateful to Frischmann Aisengart Laboratory, especially Dr. Mauro Scharf, who processed our samples at no cost. The medications used in this study were graciously supplied by Sanofi-Aventis and Merck Serono. We also thank Rafaella Jugend for her nutritional assessment. We are also grateful to the patients who participated in this study.
Author Disclosure Statement
No competing financial interests exist.