
Abstract
Background:
Oral glucocorticoids are administered in moderate and severe cases of subacute thyroiditis (SAT), providing dramatic relief from pain and fever. However, there have been no reports regarding the optimal dose of prednisolone (PSL) for treatment of SAT. In this study, we used 15 mg/day of PSL as the initial dosage and tapered it by 5 mg every 2 weeks. We assessed the effectiveness of this treatment protocol.
Methods:
We examined 384 consecutive and untreated patients with SAT who visited our thyroid clinic between February 2005 and December 2008. We excluded patients who did not fit our protocol, and the final number of subjects was 219. When patients complained of pain in their neck or C-reactive protein (CRP) was still high, physicians were able to extend the tapering of the dose of PSL or increase it at 2-week intervals. The endpoint of the study was the duration of the PSL medication. We also compared the severity of thyrotoxicosis and rate of hypothyroidism after SAT between the short medication group (patients who recovered within 6 weeks) and long medication group (patients who recovered in 12 weeks or more).
Results:
The number of patients whose thyroiditis improved within 6 weeks and did not recur was 113 (51.6%), and 61 (27.9%) improved within 7 to 8 weeks and did not have a recurrence. The longest duration was 40 weeks. Seven patients (3.2%) needed increases in the dosage of PSL. Thyroid hormone (free thyroxine and free triiodothyronine) levels measured at the initial visit in the short medication group were significantly higher than those in the long medication group (p<0.05). Serum CRP, male-to-female ratio, body weight, and age showed no differences between the two groups. There were no differences in the rate of hypothyroidism after SAT between the two groups (p=0.0632).
Conclusions:
The treatment protocol that we employed had 15 mg/day of PSL as the initial dosage for the treatment of SAT, with tapering by 5 mg every 2 weeks, and was effective and safe for Japanese patients. However, 20% of patients with SAT needed longer than 8 weeks to recover from the inflammation.
Introduction
PSL at 40 mg/d has been the preferred initial dosage for treatment for SAT (2,6). There have also been reports of 25 to 60 mg/d of PSL being administered. However, there have been no reports about the optimal dosage of PSL for the treatment of SAT (7 –12). It is desirable to start with a minimal dosage of PSL and stop for a short duration because of the side effects of glucocorticoids. The first-line therapy for SAT in our hospital consists of the use of a small amount of PSL. Our treatment protocol has dramatic beneficial effects and few side effects. As indicated in our former report (13), the rate of permanent hypothyroidism after SAT was lower in patients who received PSL. We prefer to use small amounts of PSL rather than NSAIDs. In this study, we employed 15 mg/day of PSL as the initial dosage for the treatment of SAT and tapered it by 5 mg every 2 weeks. We assessed the effectiveness of this treatment protocol.
Subjects and Methods
We examined 384 consecutive and untreated patients with SAT who visited our thyroid clinic at Kuma Hospital between February 2005 and December 2008. SAT was diagnosed on the basis of swelling with pain and tenderness in the thyroid gland and laboratory findings of elevated C-reactive protein (CRP), elevated serum free thyroxine (FT4), decreased serum thyrotropin (TSH), and hypoechoic lesion(s) in the painful region of the thyroid gland on ultrasonography. We employed the diagnosis criteria established by the Japan Thyroid Association (Table 1) (14). Data on the included patients are summarized in Table 2. Anti-thyroid peroxidase antibodies (TPOAb) were negative at the initial examination. All patients with SAT showed characteristic features of a hypoechogenic area within a painful region of the thyroid gland by ultrasonography. Among 384 patients, 54 patients were not treated with medication, 33 patients were treated with NSAIDs, 9 patients dropped out of the treatment protocol, and 69 patients violated the treatment protocol. We excluded these patients and consequently the final number of subjects analyzed in this study was 219. Patients with diabetes mellitus or gastric ulcers were not treated with PSL. Twenty-six patients were men, 193 were women, and the mean age (±SD) was 48.59±10.42 years. Mean (±SD) serum levels of TSH, FT4, free triiodothyronine (FT3), and CRP were 0.091±0.442 mU/L, 2.5±1.1 ng/dL, 7.15±4.33 pg/mL, and 3.97±3.4 mg/dL. Of the 219 patients, 9 patients had a normal TSH level, 7 had a TSH between 0.3 and 0.1 mU/L, and 203 had a TSH <0.1 mU/L. Forty-three patients had a normal FT4 and 176 presented with a high FT4. The mean body weight was 55.27±10.44 kg (Table 2).
TSH, thyrotropin; FT3, free triiodothyronine; FT4, free thyroxine; CRP, C-reactive protein.
The treatment protocol that we used was as follows: 15 mg/day of PSL was administered as the initial dose for the treatment of SAT and was tapered by 5 mg every 2 weeks (Fig. 1). Subjects were monitored once every 2 weeks. If patients complained of pain in their neck or if the CRP was still high, PSL treatment was extended and the dosage was then tapered or increased in some cases. If SAT recurred after discontinuation of PSL, PSL was administered again. Anti-ulcer drugs were administered to all patients. The endpoint of the study was the duration of the PSL medication. We also compared the severity of thyrotoxicosis and rate of hypothyroidism after SAT between groups defined by duration of treatment. The short medication group included patients who recovered within 6 weeks, and the long medication group included patients whose recovery required 12 weeks or more. Additionally, we studied the relationship between serum thyroid hormones (FT4 and FT3) concentrations and the duration of the PSL medication. We also studied the relationship between serum CRP concentrations and the duration of the PSL medication.

Study protocol; 15 mg/day of prednisolone (PSL) was administered as the initial dosage for the treatment of subacute thyroiditis and was tapered by 5 mg every 2 weeks.
Laboratory methods
TSH, FT4, and FT3 concentrations were measured using chemiluminescent immunoassays (Architect TSH, Architect FT4, and Architect FT3, respectively; Abbott Japan Co., Tokyo, Japan). Normal ranges are 0.3–5.0 mU/L for TSH, 0.7–1.6 ng/dL for FT4, and 1.70–3.70 pg/mL for FT3. Serum levels of anti-thyroglobulin antibody (TgAb), anti-thyroid peroxidase antibody (TPOAb), and anti-TSH receptor antibody (TRAb) were measured using an electrochemiluminescence immunoassay (ECLusys 2010; Roche Diagnostics Japan Co., Tokyo, Japan; normal range: <39.9 IU/mL for TgAb, <27.9 IU/mL for TPOAb, and <1.9 IU/L for TRAb). CRP (normal range, <0.5 mg/dL) was measured using a routine automated analyzer (Hitachi 7170S Clinical Analyzer, Tokyo, Japan).
Statistics
FT4, FT3, and CRP levels between the short medication group and long medication group were compared using the Mann–Whitney test. Differences in the rate of hypothyroidism after SAT were evaluated by the chi-square test. Correlation analyses between serum thyroid hormones and the duration of the PSL medication were performed using Spearman's rank correlation test.
Results
The duration of the PSL administration is shown in Figure 2. The number of patients whose thyroiditis improved within 6 weeks and did not recur was 113 (51.6%) and 61 (27.9%) improved within 7–8 weeks and did not recur. The longest duration was 40 weeks. Seven patients (3.2%) needed increases in the dose of PSL: 30 mg was required in two patients and 20 mg was required in five. One hundred six patients took PSL for 7 weeks or more. Of these, the CRP was still high in 17 patients at 6 weeks. Eighty-nine patients had pain or tenderness at 6 weeks; of these, 13 needed an increase of PSL to 15 mg and 10 needed 10 mg of PSL. There was only one patient who complained of epigastric pain, which was likely caused by PSL.
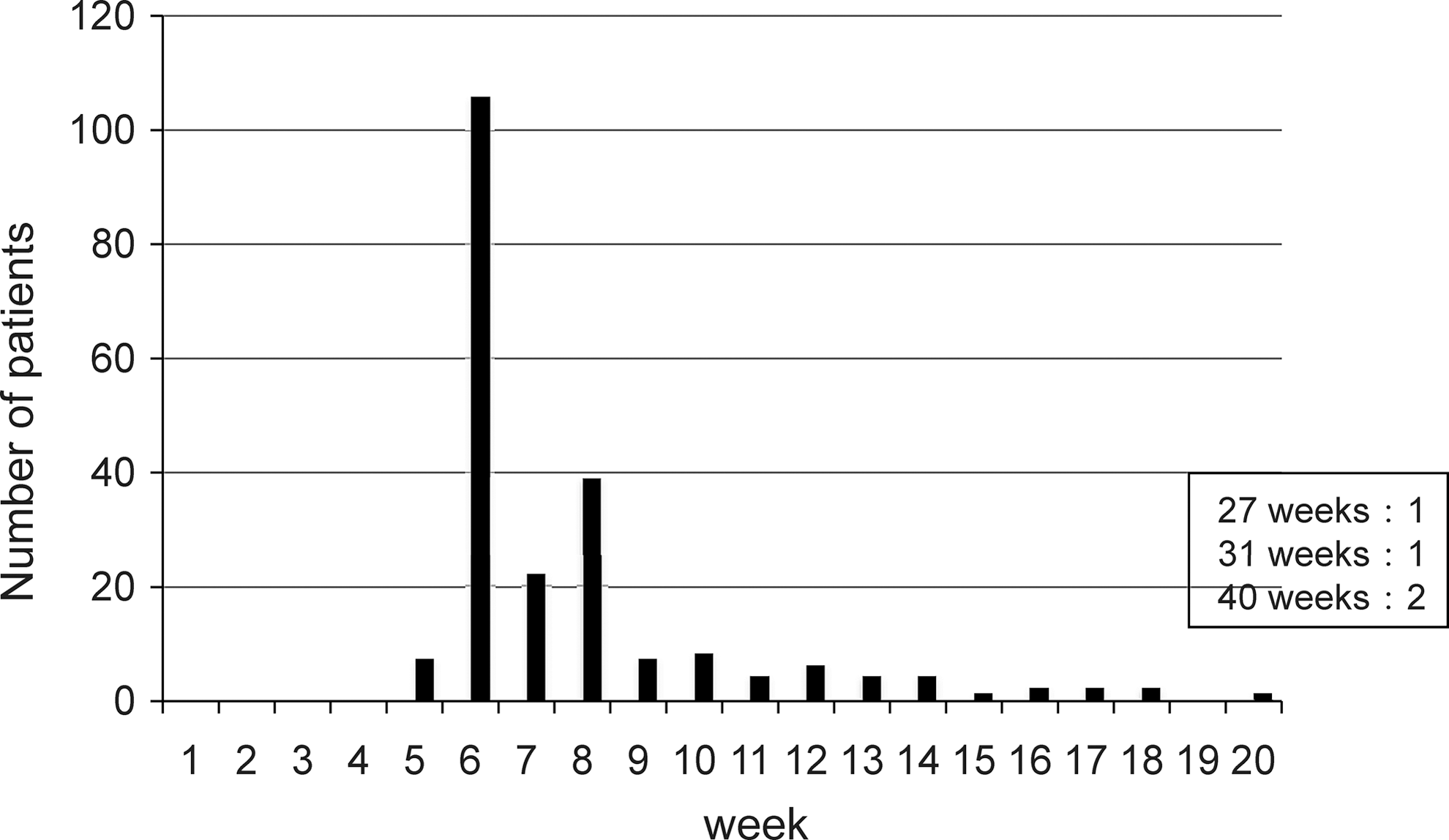
Duration of prednisolone administration.
We divided patients into two groups to clarify the characteristics of patients with SAT who required a long treatment. Thyroid hormone (FT4 and FT3) levels measured at the initial visit in the short medication group were significantly higher than those in the long medication group (p<0.05). Serum CRP, male-to-female ratio, body weight, and age showed no differences between the two groups. There were no differences in the rate of transient or permanent hypothyroidism after SAT between the two groups (p=0.0632) (Table 3).
NS, nonsignificant.
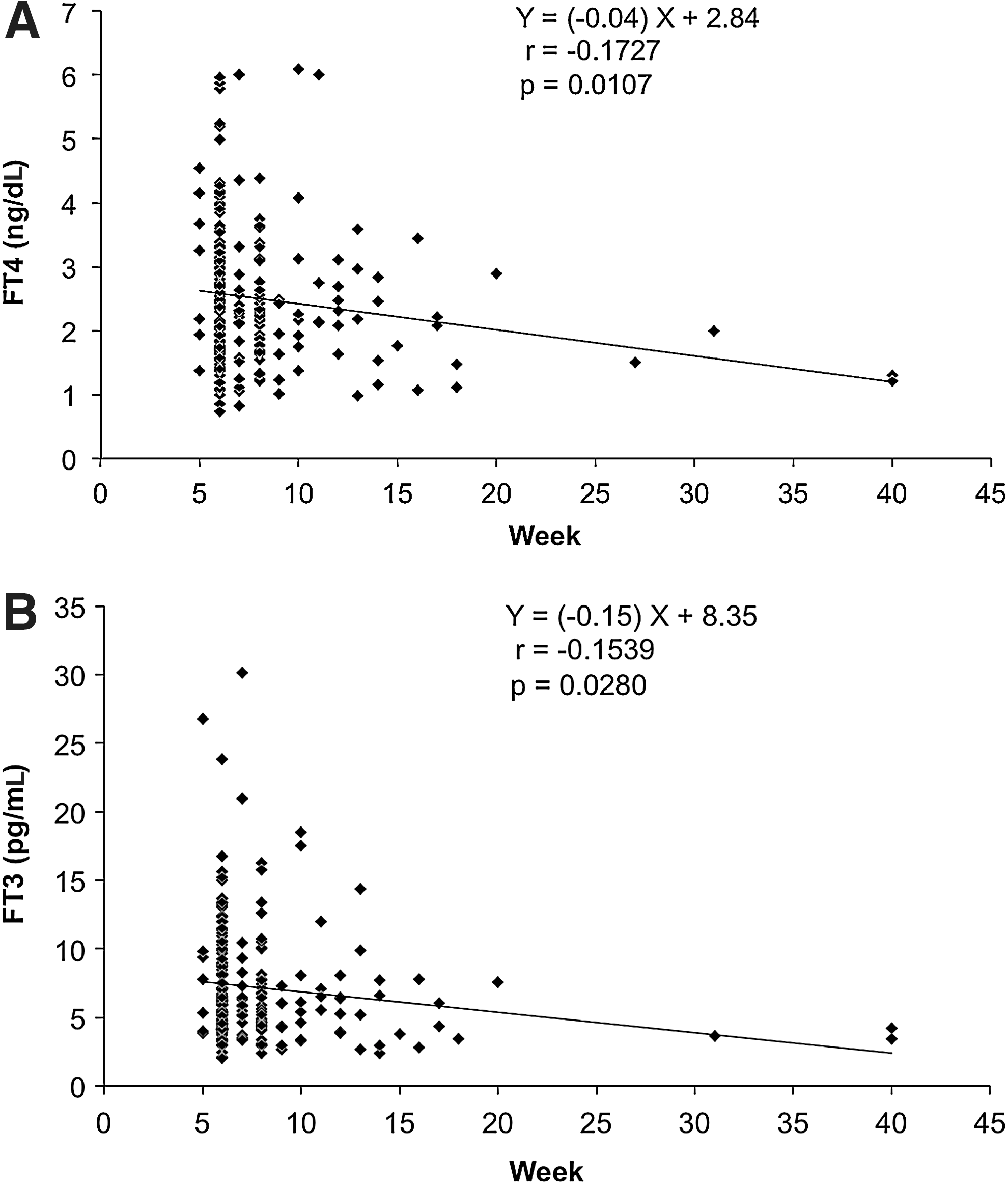
There was a significant negative correlation between the duration of the PSL medication and serum concentrations of both FT4 (r=−0.1727, p<0.05) and FT3 (r=−0.1539, p<0.05) (Fig. 3). No correlations were found between serum CRP concentrations and the duration of the PSL medication.
Discussion
We have summarized previous reports regarding the treatment of SAT in Table 4. In these reports, 25–60 mg/day of PSL was used for the initial treatment of SAT. Management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists recommend 40 mg/day of PSL as the initial dosage for the treatment of SAT (6). However, these recommended initial dosages do not have strong supporting evidence because the number of treated patients was small and initial doses of PSL were not fixed in these studies.
PSL, prednisolone.
Therefore, on an empirical basis, we employed 15 mg/day of PSL as the initial dosage for the treatment of SAT to examine the efficacy of a small amount of PSL. In this study, 80% of patients with SAT improved within 8 weeks. An important point to emphasize is that 96.8% of patients with SAT did not need more than 15 mg of PSL for the treatment of SAT. Since the mean body weight of subjects was 55.27 kg, 0.27 mg/kg of PSL as the initial dosage for the treatment of SAT was effective.
In previous studies using larger amounts of PSL, recurrence rates were 20% to 35% (2,9,11). The rates of patients who needed a longer period of PSL treatment were similar to our study, suggesting that the effectiveness of smaller amounts of PSL (15 mg) is the same as larger amounts of PSL in the treatment of SAT. Moreover, few side effects of PSL were observed in the subjects studied here. However, it must be noted that there may be a slight bias regarding side effects because physicians did not select PSL treatment for patients with diabetes mellitus or gastric ulcers. It is necessary to keep in mind that less severe side effects (weight gain, serum glucose levels, blood pressure, etc.) could have been overlooked because we did not use a systematic approach for evaluating side effects.
Interestingly, thyroid hormone levels measured at the initial visit were significantly higher in the short medication group than in the long medication group. This finding suggests that destruction of the thyroid was more severe in the short medication group than in the long medication group at the initial visit. In the long medication group, mild destruction may persist for a long period. There were no characteristic findings in the long medication group. We had expected that the rate of hypothyroidism after SAT would be higher in the short medication group than in the long medication group because of severe destruction of the thyroid; however, the results did not support this hypothesis. Our results indicate that patients with SAT and mild thyrotoxicosis at an early stage did not recover faster than patients with severe thyrotoxicosis.
In summary, the treatment protocol of 15 mg/day of PSL as the initial dosage for the treatment of SAT with tapering by 5 mg every 2 weeks was effective and safe for Japanese patients. However, 20% of patients with SAT needed longer than 8 weeks to recover from the inflammation. Dose adjustments of PSL according to body weight (0.27 mg/kg of PSL) for other ethnic groups may be necessary.