
Abstract
Background:
The lymph node yield (LNY) and the lymph node ratio (LNR) have been shown to be important prognostic factors in oral, colon, and gastric cancers. The role of the LNY and LNR in papillary thyroid cancer (PTC) is unclear. The aims of this study were to determine if a high LNR and a low LNY decrease disease-free survival rates. This study further aimed to determine an optimum nodal yield.
Methods:
A retrospective analysis was conducted of 198 patients with PTC undergoing total thyroidectomy with neck dissection between 1987 and 2011. The LNY and LNR were adjusted by relevant covariates in a multivariate Cox regression analysis with Andersen–Gill extension.
Results:
The LNR was associated with a decrease in disease-free survival (hazard ratio 3.2 [95% confidence interval 1.4–7.3], p=0.005). Patients with an LNR of 0.30 or higher had a 3.4 times higher risk of persistent or recurrent disease compared with patients with an LNR of 0.00 ([95% confidence interval 1.1–10.5], p=0.031). Conversely, patients with an LNR of 0.11 or lower had an 80% chance of remaining disease free during 5 years of follow-up. The LNY showed no significant independent effect and an optimum nodal yield was not determined.
Conclusions:
The LNR is an important independent prognostic factor in PTC and can be used in conjunction with existing staging systems. A clinical relevant cut-off point of 0.3 (one positive lymph node out of three total) is proposed. No prognostic implications for LNY were identified.
Introduction
The American Joint Committee on Cancer TNM classification and other staging systems have been designed to predict disease-specific survival but are less reliable in predicting the risk of persistent or recurrent disease (2). Recent studies have demonstrated lymph node yield (LNY, the total number of lymph nodes dissected) and lymph node ratio (LNR, the number of positive lymph nodes divided by the total amount of lymph nodes) to be independent predictors of regional failure and survival in oral squamous cell carcinoma (3,4). To enable better risk stratification and selection for adjuvant therapy, we suggest the LNR be used in conjunction with existing staging systems. Similar findings have been described for gastric, colon, and medullary thyroid cancer (5 –10).
Beal et al. (11) evaluated the impact of the LNY and LNR on overall survival in patients with papillary thyroid cancer (PTC) but were unable to demonstrate any significant relationship with LNR, and the role of LNY was unclear. Lang et al. (12) found an association between the LNR and stimulated postoperative thyroglobulin (Tg) in patients who underwent a prophylactic unilateral central neck dissection (CND), suggesting an increase in recurrence rate with a higher LNR. Recently Yip et al. (13) conducted a study in 253 patients, of which 49% underwent a formal neck dissection, and also found LNR to be an independent prognostic factor. Unfortunately, none of these studies have identified an LNR value that could be used in clinical practice.
The primary aim of this study was to determine whether LNY and LNR are predictors of recurrence and survival in patients with PTC. It is hypothesized that a high LNR reduces disease-free survival, and a high LNY increases disease-free survival. The secondary aim was to identify a minimal or optimum nodal yield.
Material and Methods
The Sydney Head and Neck Cancer Institute at the Royal Prince Alfred Hospital, Australia, maintains a prospective clinicopathologic database. A retrospective search including additional patients from Liverpool Hospital, Sydney, Australia, identified 248 patients with PTC who underwent a total thyroidectomy and CND and/or lateral neck dissection (LND) between 1987 and 2011. A maximum of 3 months after the primary surgery was allowed for a completion procedure or neck dissection (patients who underwent subsequent neck dissection for recurrent disease were not eligible for inclusion). There were 50 patients who were excluded for the following reasons: patients that underwent intraoperative lymph node sampling (Delphian or paratracheal lymph node removal but no en bloc dissection of the central compartment, n=16), incomplete patient data (n=32), and the presence of other head and neck malignancy (n=2), leaving 198 patients suitable for analysis. Mean follow up was 36 months.
Ultrasound was used as a routine preoperative investigation of patients with thyroid cancer. Computed tomography (CT) was used if there was concern regarding tracheal invasion or retrosternal extension of the thyroid gland. The main indications for central compartment therapeutic dissections were (i) bulky, palpable disease, (ii) nodal disease discovered at the time of thyroidectomy, or (iii) (incidental) finding of central compartment disease on CT or ultrasound. Patients with lateral neck disease usually underwent concurrent central compartment dissection. Indications for elective CND were large primary tumor or evidence of extrathyroidal extension.
To determine disease-free survival, events were defined as (i) surgery for PTC more than 3 months after primary surgery, (ii) radioactive iodine (RAI) treatment more than 12 months postthyroidectomy, (iii) radiological evidence of disease supported by biopsy or nuclear scan, or (iv)>2 ng/mL stimulated serum Tg (sTg) levels at least 6 months after RAI ablation. A cut-off stimulated Tg level of 2 ng/mL was chosen according to the criteria on absence of persistent disease according to the latest American Thyroid Association Thyroid Guidelines (14). Patients with sTg levels >2 ng/mL or showing clinical or radiological evidence of disease at 12 months postthyroidectomy are said to have persistent disease. Patients with no objective criteria for persistent disease at 12 months postoperative who subsequently develop disease are classified as having recurrent disease.
All statistics were two-sided, with p<0.05 considered significant. Analyses were performed with PASW Statistics version 18.0 (SPPS Inc., IBM Corp., Armonk, NY) and STATA version 11.0 (StataCorp LP, College Station, TX). A purposeful technique for selection of covariates was used to develop a final multivariate model, including significant covariates and potential confounders (established prognostic factors) (15). Kaplan–Meier survival estimates and multivariate Cox regression analysis with Andersen–Gill extension to allow for multiple event analysis were used to analyze associations with disease-free survival of the LNR and LNY as continuous (with square root transformation) and as categorical variables (16).
Results
The study population consisted of 198 patients with a median age of 45.0 years (range, 17.8–94.3 years). Relevant clinicopathologic data are summarized in Table 1.
Including tall cell (n=5), solid (n=4), and diffuse sclerosing (n=3) variants.
PTC, papillary thyroid carcinoma.
All patients underwent a total thyroidectomy and CND or LND (Table 2), and 14 underwent a completion thyroidectomy. The majority of neck dissections were elective (58%). Of the 50 patients classified as N0, nine underwent a therapeutic neck dissection. The distribution of patients by neck dissection type is shown in Table 2. RAI ablation was administered to all patients except nine with micropapillary carcinoma. Four patients received external beam radiotherapy. Initial treatment is summarized in Table 3.
Total amount of lymph nodes dissected (median).
Amount of positive lymph nodes/total amount of lymph nodes dissected (median).
CND, central neck dissection; LND, lateral neck dissection; LNY, lymph node yield; LNR, lymph node ratio.
Total amount of millicuries received.
RAI, radioactive iodine; EBRT, external beam radiation therapy.
During follow-up 145 patients remained disease free, 38 patients had persistent disease, and 15 patients developed recurrence as summarized in Table 4. Of the 53 patients with persistent or recurrent disease, 16 had multiple treatments, giving a total of 80 events for analysis. During the same period 238 patients underwent total thyroidectomy for PTC without neck dissection. Disease-free survival for both groups was not statistically different (p=0.13).
Lymph node ratio
LNR (with square root transformation), involved margins, tumor size, bilateral neck dissection, and extrathyroidal extension were significantly associated with disease-free survival on univariate analysis. Age above 45 years, sex, and multifocality were added as clinically relevant variables to the multivariate Cox regression analysis (Table 5). In the final multivariate model LNR as a continuous variable has a hazard ratio (HR) of 3.2 ([95% confidence interval (CI), 1.4–7.3], p=0.005) in a comparison of an LNR of 1 with 0.
LNR after square root transformation as a continuous variable (1 unit=0.10).
As a continuous variable (1 unit=10 mm).
HR, hazard ratio; CI, 95% confidence interval.
To assess clinical relevant cutoff points, patients were divided into 10 LNR groups and then combined into four groups according to their HR. Fifty-four patients were node negative (20%), 22 had an LNR of 0.01–0.11 (HR 1.1 [CI 0.2–4.6], p=0.931), 56 an LNR of 0.12–0.29 (HR 2.1 [CI 0.6–7.2], p=0.225), and 132 an LNR of 0.30–1.00 (HR 3.4 [CI 1.1–10.5], p=0.031; Table 6). Unadjusted disease-free survival curves according to these groups are shown in Figure 1A and predicted disease-free survival at the mean of the other covariates is shown in Figure 1B.
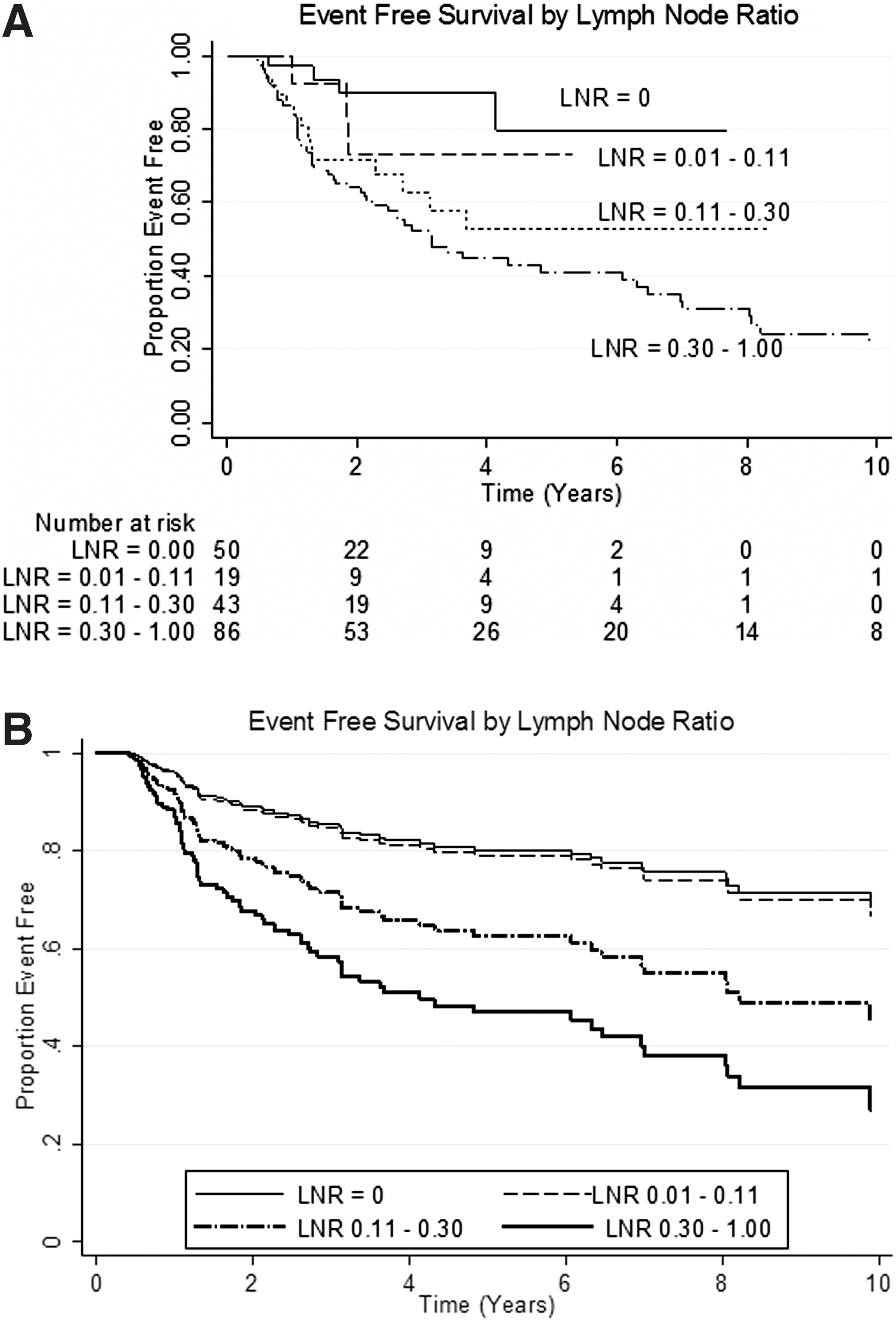
In reference to LNR=0.00.
As a continuous variable (1 unit=10 mm).
On subgroup analysis of patients who underwent elective CND versus patients who underwent therapeutic CND, both groups showed that an LNR above 0.30 predicts a 5.9 ([CI 1.7–19.8], p=0.004) and 6.8 ([CI 1.8–25.1], p=0.004) increased risk of disease, respectively.
Lymph node yield
On univariate analysis with LNY as a continuous variable, a significant HR of 1.012 was found ([CI 1.002–1.021], p=0.021; 1 unit=1 lymph node). However, after the number of positive lymph nodes was adjusted for, this increase (rather than the expected decrease) in risk of persistent and recurrent disease was no longer observed (LNY HR 0.999 [CI 0.986–1.011], p=0.826; total positive LN HR 1.041 [CI 1.022–1.060], p<0.001). Similar results were found in a multivariate model consisting of a square root transformed LNY and total amount of positive lymph nodes, sex, age above 45 years, multifocal tumor, excision margin, tumor size, and extrathyroidal extension (Table 7).
LNY after square root transformation as a continuous variable (1 unit=1 lymph node).
The total amount of positive lymph nodes after square root transformation as a continuous variable (1 unit=1 lymph node).
As a continuous variable (1 unit=10 mm).
Discussion
The presence of lymph node metastases upgrades patients above 45 years with small papillary thyroid carcinomas from stage I to stage III for central neck disease and from stage I to IVa for lateral neck disease in the 7th edition of the AJCC staging system (17). This implied increased risk of death and recurrence reflects the prognostic importance of regional lymph node involvement. However, it is unknown whether the same risk can be applied to a patient with 1 metastasis out of 20 lymph nodes removed compared with a patient with 19 positive nodes out of 20.
Clinical application of the LNR
The LNR is considered a numerical reflection of the burden of metastatic disease in a neck dissection. A large number of positive nodes or a low number of total nodes removed results in a high LNR. The same number of positive nodes divided by a larger total number of lymph nodes removed will result in a lower LNR. It is important to note that the LNR is not only influenced by disease burden but also by the extent of the neck dissection and pathological examination. Because of this, the LNR is thought to be a more sophisticated measurement than the total amount of positive lymph nodes or the nodal classification used in the TNM system because it takes into consideration extent of treatment and quality of pathological reporting.
Several authors have found increasing LNR to be associated with worse disease-related outcomes; however, no studies have identified an LNR that could be used in clinical practice. We have found the LNR to be an independent predictor of disease-free survival in PTC (HR 3.2 [CI 1.4–7.3], p=0.005; 1 unit=0.10) and importantly have demonstrated that an LNR above 0.3 predicts a 3.4 times higher risk of persistent or recurrent disease ([CI 1.1–10.5], p=0.031). Thus our estimates suggest that patients who have metastases in at least one out of three lymph nodes have more than 3 times the risk of needing retreatment within 5 years postsurgery than patients without nodal metastases. Conversely, 80% of patients with <10% of lymph nodes involved by metastatic disease will remain disease free over the same period. Therefore, the use of the LNR in conjunction with existing staging and classification systems is likely to help guide the requirements for frequency and intensity of follow-up.
Elective versus therapeutic neck dissection
Elective neck dissections in the treatment of PTC continues to be a subject of debate (18 –25). The Royal Prince Alfred Hospital and Liverpool Hospital have applied elective central compartment disease selectively, and of the 198 patients included in this study, 115 (58%) underwent an elective dissection. It is interesting that there was no difference in the value of LNR between patients undergoing elective or therapeutic CND; however, the HR for an LNR of 0.3 was greater in the CND group compared with the total group of patients (CND and LND).
Lymph node yield
The LNY did not independently predict disease-free survival when adjusted for significant and relevant covariates (HR 1.0 [CI 0.986–1.011], p=0.826). On univariate analysis, the LNY actually showed an increase in risk of persistent or recurrent disease. This is because patients with more positive lymph nodes also have a higher total amount of lymph nodes dissected. Given that the LNY was not a significant predictor of disease status, we were unable to suggest a minimum value of lymph nodes to be removed with a neck dissection.
Limitations of this study
The prospective collection of data over the past 25 years limits but does not eliminate the known limitations of a retrospective study. Variability due to differences in surgical technique and pathological assessment are difficult to overcome, and measurements such as LNR are particularly susceptible to both. By retrospectively reviewing all operation and pathology reports, this study has attempted to minimize this.
This study found a range of 6–65 lymph nodes counted, dependent on the type of neck dissection performed (Table 3). Although the LNR and LNY were adjusted for the type of neck dissection performed, no subgroup analysis was performed due to the limited number of patients included.
Approximately 20% of patients with thyroid cancer have anti-Tg antibodies (26), but sTg is not considered a reliable tumor marker in these patients. Follow-up in these patients is based on clinical and radiological signs of disease. Potentially, this may have led to some patients being regarded as disease free despite having subclinical persistent disease.
Conclusions
This study found the LNR to be an independent predictor of disease-free survival in patients with PTC. A clinical relevant cut-off point of 1 positive out of 3 total lymph nodes is suggested. The LNY was strongly associated with the total amount of positive lymph nodes and no optimum nodal yield was determined.
Footnotes
Acknowledgment
This was a multicenter study conducted at The Sydney Head and Neck Cancer Institute, Royal Prince Alfred Hospital, Sydney, Australia, and Liverpool Hospital, Sydney, Australia.
Disclosure Statement
No competing financial interests exist.