
Abstract
Aims:
The objectives of this study were to compare long-term outcomes after total thyroidectomy (TT) or thyroid lobectomy (LT) in a large cohort of patients with papillary thyroid microcarcinoma (PTMC), and to determine whether tumor size (≤0.5 cm vs. >0.5 cm) has a significant impact on the extent of surgery.
Methods:
We evaluated 2014 patients with PTMC who underwent TT with central compartment node dissection (CCND; n=1015) or LT with CCND (n=999) between March 1986 and December 2006 and for whom complete follow-up data were available for at least 5 years (median 11.8 years, range 5–26 years). Using propensity score matching to reduce the impact of treatment selection bias and potential confounding in an observational study, we compared overall survival and disease-free survival in the overall cohort and in patients with tumors ≤0.5 cm and >0.5 cm in size.
Results:
After adjustment for differences in baseline clinicopathologic risk factors, we observed no significant differences between the LT and the TT groups in the risk of death (hazard ratio for the LT group 1.05, 95% confidence interval [CI] 0.71–1.47, p=0.890) and locoregional recurrence (hazard ratio for the LT group 3.08 [CI 1.99–8.05], p=0.194) in the overall matched cohort. Similar results were observed when we compared LT and TT in patients with tumors ≤0.5 cm and >0.5 cm.
Conclusions:
The long-term rates of death and locoregional recurrence were similar in patients with PTMC who underwent LT with CCND and those who underwent TT with CCND. Therefore, completion thyroidectomy may not be recommended unless recurrence after LT is definitely detected in low-risk PTMC patients, and close follow-up is adequate in these patients. Moreover, tumor size greater than or less than 0.5 cm was not a significant determinant of the extent of surgery in patients with PTMC.
Introduction
There is no universal agreement about the natural course of PTMC, thus creating controversy concerning the diagnosis and treatment of PTMC. Furthermore, it is not yet possible to confidently identify PTMCs that would take an aggressive course if left untreated. Treatment recommendations range from observation alone to vigorous intervention featuring total thyroidectomy (TT), prophylactic cervical lymph node dissection, and adjuvant radioactive iodine (RAI) ablation. Accordingly, no consensus has yet been reached on the biological aggressiveness of PTMC or on which therapy is the most appropriate. Moreover, the impact of several clinicopathologic risk factors on prognosis, including tumor size, is ambiguous. Although the prognostic importance of tumor diameter (≤0.5 cm vs. >0.5 cm) has been investigated by many clinicians, the effect of tumor diameter on prognosis remains unclear (5,7,8).
Most studies evaluating the proper extent of surgery for PTMC have been retrospective in design. A prospective, long-term, randomized study in a large number of patients, however, may not be feasible owing to the need for an extensive follow-up duration, the costs associated with such a study, and, particularly, its ethics constraints (4). Consequently, it is not currently possible to determine the prognosis of patients with PTMC or the proper therapeutic approach in these patients. We therefore compared long-term outcomes after TT or thyroid lobectomy (LT) in a large cohort of patients with PTMC, using propensity score matching to adjust for the uncontrolled assignment of surgical extent in these patients. In addition, we evaluated whether tumor size, ≤0.5 cm or >0.5 cm, had a significant impact on determining the extent of surgery in patients with PTMC.
Materials and Methods
Study population
From March 1986 to December 2006, a total of 5042 patients with PTC (of all tumor sizes) underwent initial surgical therapy at our institution. Of these, 2441 patients (48.4%) had PTMCs ≤1 cm in diameter, with 1270 undergoing TT and 1171 undergoing LT. Complete follow-up data for major clinical events were available for 2014 patients (82.5%), including 1015 (79.9%) of the TT group and 999 (85.3%) of the LT group (p=0.1834). Patients were followed-up for a median of 11.8 years (range 5–26 years). All histopathologic diagnoses were reviewed and verified by endocrine pathologists using World Health Organization criteria. The study protocol was approved by our Institutional Review Board. Details of patients' presentations, surgical and pathologic findings, adjunctive treatments, and follow-up data were obtained from our Thyroid Cancer Database.
Management strategy
In patients diagnosed with PTMC after a complete radiologic and histologic examination, the extent of thyroidectomy and RAI therapy were based on prognostic factors. An LT was performed if the following criteria were met by preoperative evaluation: a single lesion, no definite extrathyroidal invasion, no clinical lymph node metastasis, and no personal history of radiation therapy to the head or neck. A TT was performed if there were multiple lesions or bilateral lesions, or if a definite extrathyroidal invasion or a clinical lymph node metastasis was discovered during surgery. Preoperative evaluation of cervical lymph nodes in levels I–VI was made by US and neck computed tomography (CT). A prophylactic central compartment node dissection (CCND; pretracheal, prelaryngeal, and paraesophageal) was performed in all cases for accurate staging of PTMC and to manage the subclinical lymph node metastasis. A prophylactic ipsilateral CCND was performed if the following criteria were met by preoperative evaluation and intraoperative findings: unilateral lesion and no definite clinical lymph node metastasis was found in preoperative imaging or in intraoperative gross findings. A bilateral CCND was performed if there were multiple lesions or bilateral lesions, or if any sign of a definite clinical lymph node metastasis was discovered in preoperative imaging or during surgery. Most patients (excluding T1N0M0 patients) who underwent TT received low-dose (30 mCi) RAI for remnant ablation. High-dose RAI (>150 mCi) therapy was administered to patients with distant metastasis, more aggressive tumor histology, or T4 or N1b stages, and to selected patients with high thyroglobulin (Tg) concentrations but without definite metastatic lesions, after an RAI whole-body scan.
Although the final pathologic feature after LT revealed one of the equivocal risk factors such as minimal capsular invasion, incidental multifocal lesion, or micrometastatic central lymph node invasion, completion thyroidectomy has not been suggested. For these patients, we provide information regarding the option of close observation rather than immediate completion thyroidectomy, providing the information that the risk to life is negligible, but a troublesome recurrence in a lymph node of the neck is possible. For these patients, regular follow-up appointments, to include periodic physical examination and imaging by US or CT of the neck, should be scheduled. If a suspicious contralateral thyroid mass or enlarged cervical lymph nodes were subsequently found, ultrasound-guided fine-needle aspiration cytology has been performed. If a remnant thyroid cancer or a metastatic lymph node was thus identified, completion thyroidectomy has been performed. If patients underwent contralateral completion thyroidectomy within 6 months of their initial thyroid surgery, then it was considered part of the initial surgery.
All patients received levothyroxine therapy after initial surgery. Patients were clinically evaluated, including measurements of thyrotropin and Tg, 3 and 6 months after the initial treatment and yearly thereafter. Patients who received RAI ablation after TT underwent RAI whole-body scans 5 to 7 days later. All patients were evaluated by neck US and chest X-ray or CT 3 or 6 months after surgery according to clinical evaluation.
Statistical analysis
To reduce the impact of treatment selection bias and potential confounding in this observational study, we performed rigorous adjustments for significant differences in baseline characteristics of patients by propensity score matching. The propensity score was defined as the probability of being assigned to a given surgical group based on patient baseline clinical findings and tumor characteristics. We chose the 90% level to allow adequate power for subgroup analysis at a significance level of 0.05 in this retrospective study. Propensity score matching was performed for the entire cohort and separately for patients with tumor size ≤0.5 cm or >0.5 cm. After propensity score matching, the baseline covariates of the two groups were compared. Continuous variables were compared using the t-test or Wilcoxon rank sum test, and categorical variables were compared using chi-square statistics or the Fisher exact test, as appropriate. Statistical significance and the effects of treatment on outcomes were determined using statistical methods appropriate for matched data (9,10). In the propensity score–matched cohort, the risks of each outcome were compared with the use of Cox regression models, with robust standard errors that accounted for the clustering of matched pairs. In each propensity score–matched cohort, survival curves were constructed using the Kaplan–Meier method and compared using the log-rank test.
All reported p-values are two-sided, with p-values <0.05 considered statistically significant. SAS software (SAS Institute, Cary, NC), version 9.1, and the R programming language were used for statistical analyses.
Results
Patient characteristics
Of the 2014 patients who fulfilled the selection criteria, 1015 underwent TT and 999 underwent LT; their baseline characteristics are shown in Table 1. When we divided the overall cohort into two separate subgroups based on tumor size, we found that 894 had tumors ≤0.5 cm and 1120 had tumors >0.5 cm in diameter. Of the patients with tumors ≤0.5 cm, 382 (42.7%) underwent TT and 512 (57.3%) underwent LT; of the patients with tumors >0.5 cm, 547 (48.8%) underwent TT and 573 (51.2%) underwent LT. Table 1 shows that patients in both subgroups who underwent TT were significantly older and had higher rates of extracapsular invasion and cervical lymph node metastasis. Although all operations were undertaken with the intent of performing CCND, no lymph nodes were found histopathologically in 116 cases.
Open technique (conventional open method by 6–8 cm transverse collar incision), mini-incision technique (open method by mini-incision, <4cm), endoscopic technique (totally endoscopic method via gasless transaxillary approach).
The extent of MRND include sublevels IIa, III, IV, and Vb. However, if an enlarged or suspicious LN at level I, IIb, or Va was encountered by palpation or by preoperative imaging, those compartments were included in an en bloc dissection.
The extent of selective neck dissection include LNs along with internal jugular chain nodes (sublevels IIa, III, and IV).
LT, thyroid lobectomy; TT, total thyroidectomy; LN, lymph node; CCND, central compartment node dissection; MRND, modified radical neck dissection.
Follow-up and treatment outcomes for the overall cohort
To date, in this cohort of 2014 patients, 15 patients (0.7%) died, none due to a disease-specific cause. Two patients (0.1%) showed distant metastases at the initial diagnosis, and were excluded from the analysis of recurrences. The postoperative RAI whole-body scans revealed a lung metastasis in one patient and multiple bone metastases in the other patient. In the patient with the lung metastasis, the post-therapeutic scan after 350 mCi RAI treatment did not show any significant abnormal uptake, and serum Tg was undetectable after levothyroxine withdrawal. The patient with multiple bone metastases received a cumulative dose of 1700 mCi RAI and external radiation after initial surgery, and is still receiving treatment.
Locoregional recurrence was observed in 126 patients (6.3%), and the recurrence sites were 98 patients (4.9%) in regional neck nodes, and 28 (1.4%) in the remnant thyroid gland or operative bed. All of these recurrences were confirmed by cytologic or histopathologic findings. Nineteen (0.9%) TT patients showed increased Tg concentrations (Tg >10 ng/mL) after thyrotropin stimulation, but without a definite metastasis on imaging. However, none of the study patients developed distant spread during our follow-up period.
The 10-year overall survival and disease-free survival rates for the overall cohort were 98.9% and 94.2%, respectively. At 10 years, the cumulative incidence of the definite locoregional recurrence was 4.2%, but no patient showed evidence of distant metastasis. By 20 years, 6.1% of patients had experienced a recurrence either within the neck nodes or remnant thyroid gland. In addition, locoregional recurrence rates after LT did not differ significantly from those seen after TT, with the recurrence after LT at 5, 10, and 20 years being 1.9%, 4.3%, and 6.5%, respectively, compared with recurrence rates after TT of 2.3%, 4.1%, and 5.9% (p=0.2780).
Characteristics of patients matched for propensity score
Propensity score matching of the entire population yielded a total of 506 matched pairs, including 224 and 260 pairs of patients with tumors ≤0.5 cm and >0.5 cm in diameter, respectively. In these matched cohorts, there was no longer any significant difference in any covariate between those who underwent TT and those who underwent LT (Table 2).
RAI, radioactive iodine.
Treatment outcomes for matched cohorts
After adjustment for baseline covariates, there were no significant differences in the 10-year rates of death and locoregional recurrence between the TT and LT groups in the 506 matched patient pairs (Table 3). Figure 1 shows the long-term rates (5-, 10-, 15-, and 20-year follow-up) of clinical outcomes according to the extent of surgery in the overall matched cohort. Similarly, the risks of death and locoregional recurrence did not differ between the TT and LT groups in the 224 matched pairs of patients with tumors ≤0.5 cm in diameter (Fig. 2 and Table 3) or in the 260 matched pairs of patients with tumors >0.5 cm in diameter (Fig. 3 and Table 3). Therefore, the extent of thyroidectomy was not significantly associated with a higher rate of locoregional recurrence in both subgroups. However, the hazard ratios for each end point of locoregional recurrence showed nonsignificant trends toward higher risk among patients with large tumors (tumor size >0.5 cm) who underwent LT than those who underwent TT.

Kaplan–Meier curves of outcomes in overall patients matched for propensity scores who underwent thyroid lobectomy (LT) or total thyroidectomy (TT).
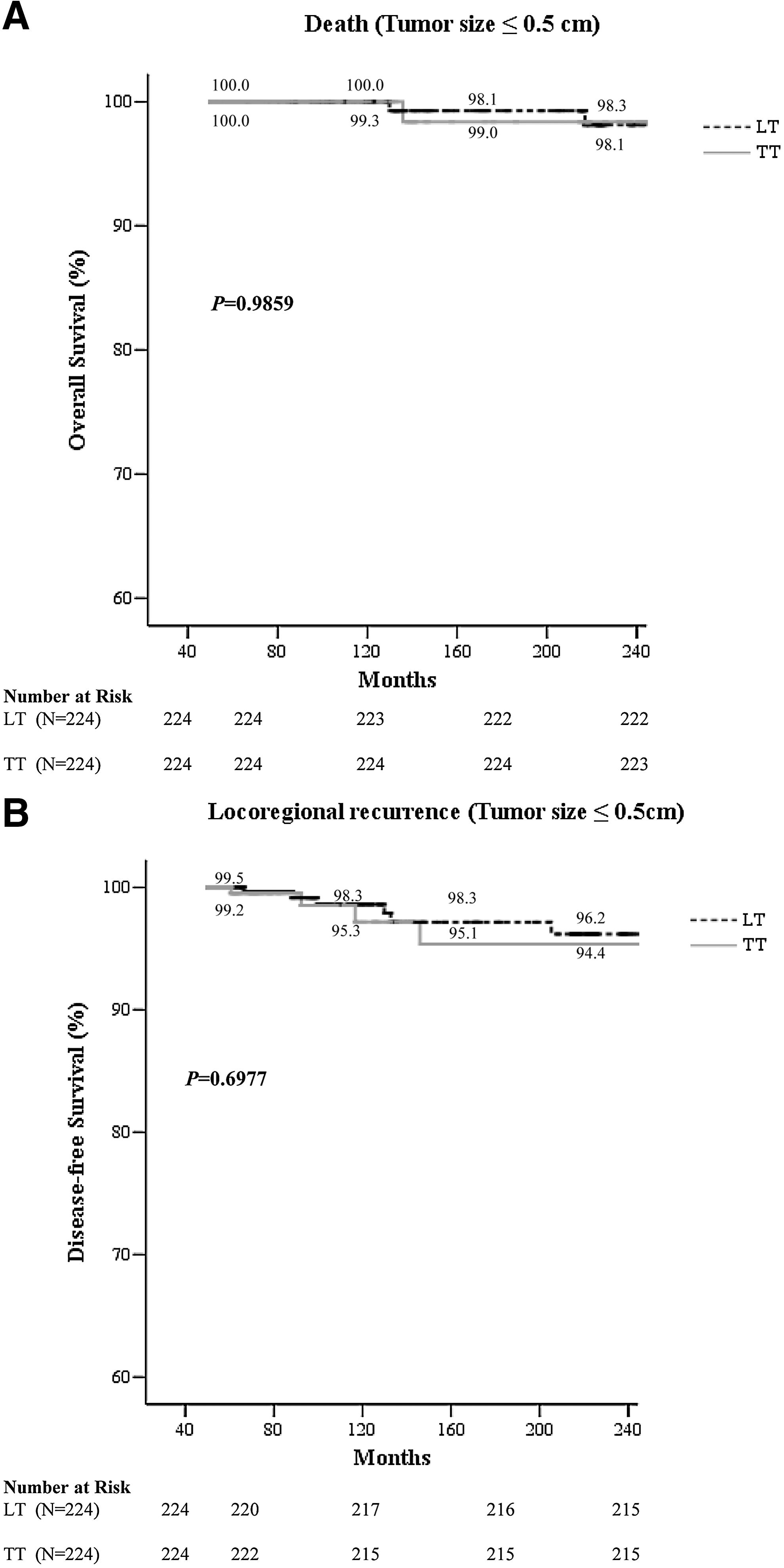
Kaplan–Meier curves of outcomes in patients with tumors ≤0.5 cm in diameter matched for propensity scores who underwent LT or TT.
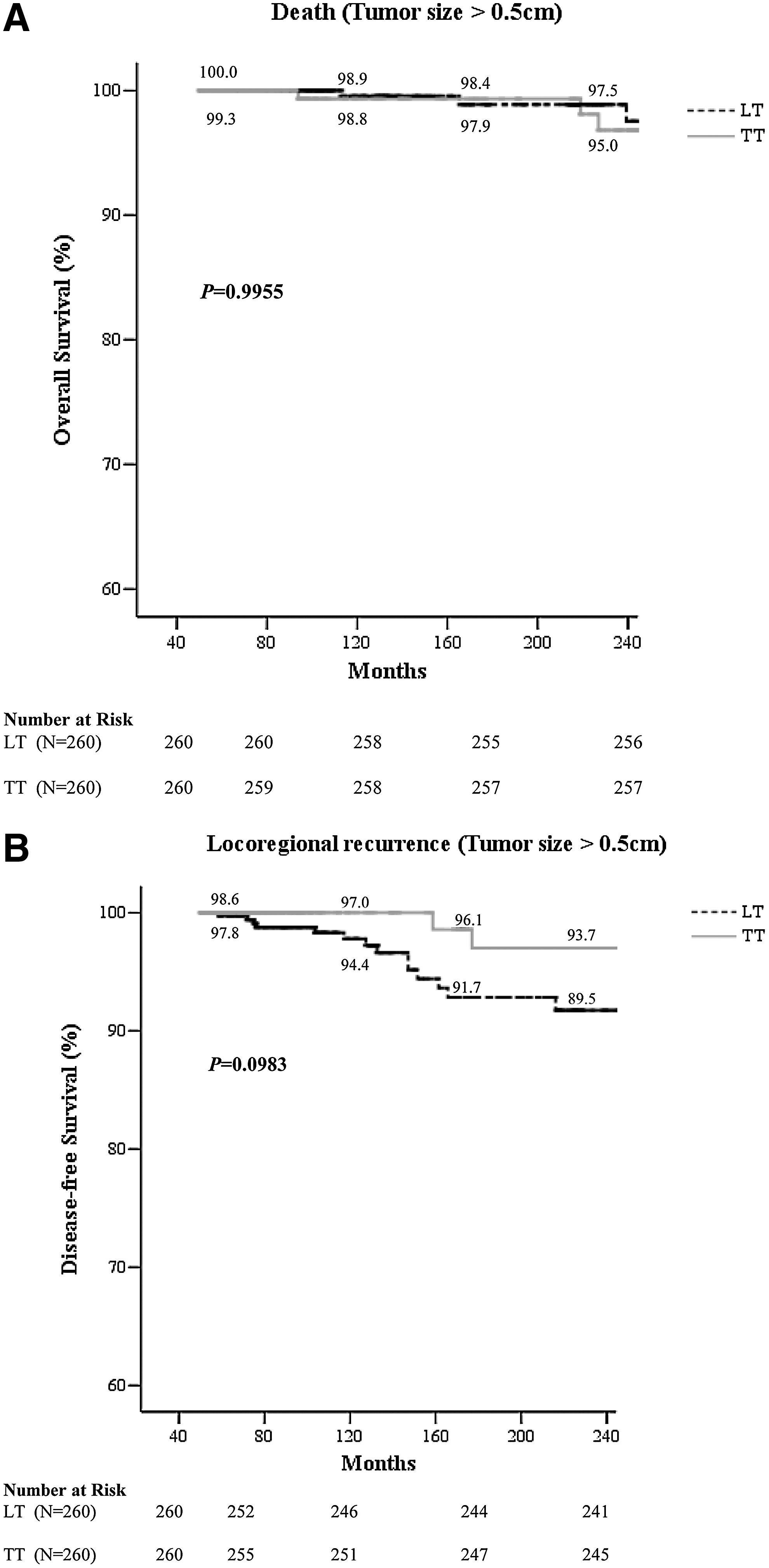
Kaplan–Meier curves of outcomes in patients with tumor >0.5 cm in diameter matched for propensity scores who underwent LT or TT.
CI, confidence interval.
Discussion
The primary outcome of our observational study was that patients with PTMC have an excellent long-term prognosis. In addition, the long-term outcomes of LT and TT were similar in a large cohort of patients with PTMC. To further determine the proper extent of thyroidectomy, we performed propensity score matching of the TT and LT cohorts, minimizing baseline differences between the original patient cohorts. We found that the long-term risks of death and tumor recurrence were similar in the matched cohorts, as well as in subgroups of patients with tumor size ≤0.5 cm and >0.5 cm.
While the prognosis of most PTMC patients is extremely favorable, tumor recurrence after initial surgical treatment remains a problem. When coupled with the generally indolent nature of PTMCs, the relatively small sample size and the short follow-up duration in previous studies may have resulted in biased outcomes (7,8,11 –15). We assessed outcomes in a long-term database of more than 2,000 patients, finding that the 10-year overall survival and disease-free survival rates were 98.9% and 94.2%, respectively. While tumor size is certainly not the sole determinant of outcome in patients with PTC, our findings show that PTMC is rarely life threatening.
Despite the increased incidence of PTMC, the optimal extent of thyroidectomy for these patients remains unclear. Treatment recommendations range from observation alone to vigorous intervention featuring TT, prophylactic CCND, and adjuvant RAI ablation. Although the guidelines of both the Revised American Thyroid Association (2009) and the European Thyroid Association (2006) recommend TT as the standard care for patients with PTC, and LT only for unifocal PTMC found incidentally (16,17), a group in Japan suggested that observation without surgery is safe for patients with small intra thyroidal PTMC (18). TT and post-RAI scans, after RAI therapy when necessary, and thyrotropin-suppressive hormonal therapy have been suggested for all patients with PTMC independent of tumor size by some extreme groups (8,12,19), while many experts favor LT without RAI (11,13 –15). Therefore, no consensus has yet been reached on the biological aggressiveness of PTMC or on which therapy is the most appropriate.
Controversy persists regarding the benefits of TT versus LT for patients with PTMC. Since TT is a more radical surgical procedure, it can eliminate the multifocal/bilateral disease that is frequently observed (8,19 –22). In addition, TT allows treated patients to be effectively monitored by RAI scanning and measurement of Tg levels, to detect persisting or relapsing disease. However, LT is a minimally aggressive surgical method used to manage PTMC. Proponents of this therapeutic approach emphasize the minimal morbidity associated with this procedure, which seems appropriate if a disease with a relatively benign biological behavior is to be treated. Moreover, several studies have found that no survival benefits were evident after more extensive thyroidectomy of PTMC patients (4,11,13 –18). It has also been recognized that LT preserves thyroid function, thereby reducing the requirement of lifelong need for hormone replacement therapy. Although recent studies have analyzed long-term outcomes in large numbers of patients with PTMC, these studies were retrospective in design, and the assignment of patients to TT and LT was not randomized (4,5,8,12 –15). To minimize these biases and confounding factors, we performed propensity score matching, thereby adjusting for baseline differences in clinicopathologic characteristics between groups. Therefore, even though our patients were not randomized, our study design can be regarded as an upgraded type of case-matched control study in which patients were matched for other clinicopathologic risk factors. According to our results, the 5-, 10-, 15-, and 20-year overall survival and disease-free survival rates after LT did not differ significantly from those seen after TT in both overall and matched cohorts. This result was consistent with those of previous studies (4,13 –15).
Although the impact of tumor diameter (≤0.5 cm vs. >0.5 cm) on the course of PTMC has been investigated in recent studies, the effect of tumor diameter on prognosis remains unclear (5,7,8,23). We explored the long-term outcomes after surgery in subgroups of PTMC patients with tumor size ≤0.5 cm and >0.5 cm by matching the TT and LT cohorts. While analyzing 1210 patients with tumors ≤0.5 cm in diameter, we found that 12.1% had multifocal cancers, with 22.5% having nodal metastases and 28.2% showing capsular invasion. Thus, among patients with PTMC, about one-fourth had tumors with all the properties of larger PTC. We also observed that the long-term risks of death and recurrence were similar in matched TT and LT cohorts of subgroups of patients with tumors ≤0.5 cm and >0.5 cm in diameter. Therefore, tumor size (0.5 cm) was not a significant factor in determining the extent of surgery for patients with PTMC.
The inherent limitation of this kind of study is its observational nature; therefore, the treatment strategy was not randomized. Analytically, our findings are subject to selection bias and confounding with respect to the relative severity of preoperative risks among PTMC patients who underwent TT and LT. To minimize these biases, we used propensity score matching, which has been reported to be superior to dose stratification or covariate adjustment. Despite these statistical adjustments, however, unknown confounders may have affected our results. In addition, our analysis is under-powered to detect significant differences in recurrence, especially when comparing TT with LT in subgroups with tumors ≤0.5 cm and >0.5 cm in size. Patients with tumors >0.5 cm who underwent LT showed nonsignificant trends toward higher event rates than those who underwent TT; these trends may have become significant in a larger patient cohort. Further a large, randomized comparison of TT and LT in patients with PTMC may provide more definitive data on the long-term prognosis of these patients, and suggest reasonable guidelines that would serve to aid decision making. Another unresolved issue in the present work is whether remnant ablation using low-dose RAI (30 mCi) impacts on long-term outcomes, compared with patient without ablation. Since RAI was administered in a non-overlapping fashion, propensity score matching for this variable could not be performed. Therefore, further clinical trials are needed to define the effectiveness of RAI remnant ablation. Furthermore, due to the insufficient data for the patients without prophylactic CCND, this study could not answer the question whether prophylactic CCND should be considered a routine for PTMC. The potential role of prophylactic CCND in PTMC patients remains a subject of debate.
In conclusion, we found that in matched cohorts of patients with PTMC who underwent routine prophylactic CCND, LT and TT were associated with similar long-term rates of death and recurrence. There is no need for recommending completion thyroidectomy unless recurrence after LT is definitely detected in low-risk PTMC patients. Regular follow-up appointments, to include periodic physical examination and imaging by US or CT of the neck, should be scheduled in these patients. Moreover, tumor size (0.5 cm) was not a significant factor in determining the extent of surgery for patients with PTMC.
Footnotes
Author Disclosure Statement
None of the authors have conflicts of interest or financial associations to disclose.