
Abstract
Background:
Papillary thyroid cancer (PTC) presents with local and distant metastases more frequently in children than in adults. However, hypoxemia secondary to pulmonary metastases has not been reported in the literature. Sorafenib is a small-molecule multikinase inhibitor used in radioactive iodine (131I)–refractive papillary thyroid carcinoma.
Patient Findings:
An eight-year-old boy presented with fever and hypoxemia and was found to have H1N1 viral pneumonia requiring mechanical ventilation and antiviral and glucocorticoid treatment. After initial improvement, he was readmitted one month later because of persistent hypoxemia. A high-resolution computed tomography of the chest and neck revealed multiple 1–4 mm nodules and necrotic lymph nodes on the right side of the neck. Left lung wedge resection and right deep cervical node biopsies were consistent with PTC. He underwent a total thyroidectomy with a central neck node dissection and postoperatively required prolonged mechanical ventilation. Due to the inability to be weaned from mechanical ventilation, treatment with sorafenib 200 mg daily (10 mg/kg/day, 250 mg/m2) was initiated. Eight days thereafter, ventilation support was discontinued and the child was extubated. However, he failed extubation secondary to supraglottic edema, and seven days later tracheostomy was performed. The dosage of sorafenib was increased to 200 mg twice daily (20 mg/kg/day, 500 mg/m2). After 52 days of therapy, a repeat computed tomography scan showed reduction in the lung nodule size to 1–2 mm. He underwent 131I therapy 87 days after sorafenib was started. A post-treatment scan showed extensive uptake throughout the lungs and thyroid bed, supraclavicular nodes, and cervical nodes.
Conclusions:
This is the first reported case of a pediatric patient with respiratory failure possibly secondary to diffuse micronodular PTC requiring mechanical ventilation and subsequent delay in definitive therapy. Sorafenib could be considered for gap therapy when 131I therapy cannot be administered in a timely manner. Treatment with this multikinase inhibitor does not seem to adversely affect the uptake of 131I in radiation-naïve patients.
Introduction
T
The usual presentation of differentiated thyroid cancer is a thyroid nodule rather than pulmonary findings. Although an upper respiratory tract obstruction with a large papillary thyroid tumor in an eight-year-old girl has been reported (3), a lower pulmonary manifestation of distant metastatic PTC before radioactive iodine (131I) ablation has not been reported as of yet. Other pulmonary manifestations, such as pulmonary fibrosis, is a rare outcome of 131I therapy in patients with pulmonary metastases (4,5).
Tumorigenesis on a molecular level involves an aberrant activation in the mitogen-activated protein kinase pathway of cell proliferation, differentiation, apoptosis, and survival. In adults, therapy with small-molecule multikinase inhibitor (MKI) has been well documented for treatment of non-131I-avid papillary tumors (6,7). An activating mutation in B-type Raf kinase (BRAF) has been implicated in aggressive differentiated thyroid cancer (8). Sorafenib, an MKI, prevents autophosphorylation of tyrosine kinase receptors, including vascular endothelial growth factor receptor, platelet-derived growth factor receptor β, c-Kit, and receptor tyrosine kinase, and downstream RAF kinase, including mutant BRAF, thus potentially preventing tumor growth by antiproliferative, antiangiogenesic, and proapoptotic effects (9). The U.S. Food and Drug Administration approved this drug in 2005 for renal cell carcinoma and in 2007 for hepatocellular carcinoma in adults (10). Therapy with sorafenib in adult patients with 131I-refractory progressive differentiated thyroid cancer has resulted in stabilization of disease or partial response in selected cases (11,12). However, currently, MKIs are considered only for treatment of non-131I-responsive advanced thyroid cancer in a clinical trial setting (4). Further, sorafenib is not approved by the U.S. Food and Drug Administration for treatment of thyroid cancer in children.
Here we describe a pediatric patient with PTC presenting with hypoxemia associated with diffuse nodular disease secondary to pulmonary metastases and H1N1 influenza A pneumonia who required mechanical ventilation. The conventional treatment with glucocorticoids did not improve his respiratory status. As the desired therapy of 131I ablation was not feasible because of his intensive care unit status requiring hourly nursing care, treatment with sorafenib was pursued. The clinical course of the patient from presentation, treatment with sorafenib, treatment with 131I, to post-treatment is described. Clinical, biochemical, and radiographic data are reported.
Patient
In July 2009, a previously healthy eight-year-old boy presented to an outside hospital with fever, myalgia, nonproductive cough, and right-sided neck swelling. Due to increased oxygen requirements, the child was transferred to our institution. On examination, he was significantly hypoxemic with an oxygen saturation of 91% on 100% non-rebreather mask. The neck examination revealed a mobile 1 cm right cervical lymph node. His chest x-ray showed diffuse infiltrates with nodular to reticular nodular appearance with confluent areas in the bases (Fig. 1A). Due to concerns of acute infection, bronchoalveolar lavage (BAL) was performed. Bronchoscopy did not reveal any anatomical defects in the airway. However, bloody effluent was noted after the third lavage without evidence of trauma at the site. Cytopathology revealed evidence of inflammation and reactive bronchoalveolar hyperplasic aggregates without evidence of necrosis or hemosiderin-laden macrophages. The BAL cell count revealed 4300 red blood cells, 160 white blood cells with 48% segmented neutrophils, 37% lymphocytes, and 15% monocytes. Studies were sent for bacterial culture and Gram stain; anaerobic, fungal, and acid-fast bacillus cultures and stain; pneumocystis direct immunofluorescent-antibody and polymerase chain reaction (PCR); respiratory syncytial virus direct immunofluorescent-antibody; and viral PCR for cytomegalovirus, adenovirus, human herpes virus-6, Epstein–Barr virus, varicella zoster virus, influenza A and B, parainfluenza, Mycoplasma pneumoniae, and modified acid-fast bacillus for Nocardia. Given the presence of bloody effluent, rheumatologic studies, including anti-neutrophil cytoplasmic antibody, antibasement membrane antibodies, anti-double-stranded DNA, anti-nuclear antibody, and rheumatoid factor studies, were conducted and the results were normal. Of these studies, the only study that was positive was influenza A with PCR specific for the H1N1 virus. Cystic fibrosis was ruled out by a negative sweat chloride test. On the basis of the presence of inflammatory cells along with a positive PCR for H1N1 influenza A virus, it was concluded that the child had influenza A pneumonia. He developed worsening hypoxemia requiring mechanical ventilation for two days. Treatment with a beta-agonist (albuterol), systemic glucocorticoids (prednisone), and antiviral therapy (oseltamivir) was instituted. He was discharged home on room air with SpO2 of 93% after 16 days.
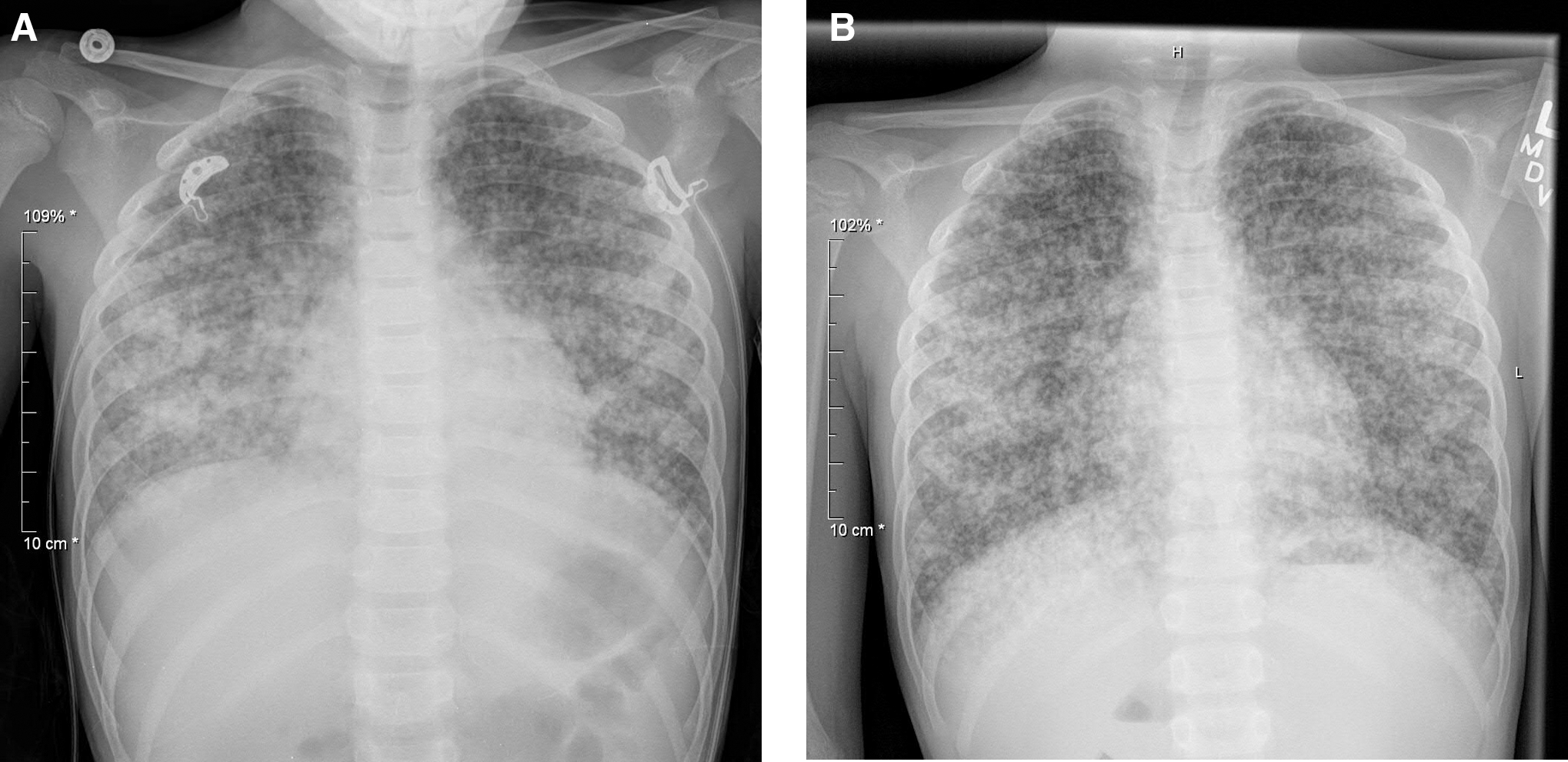
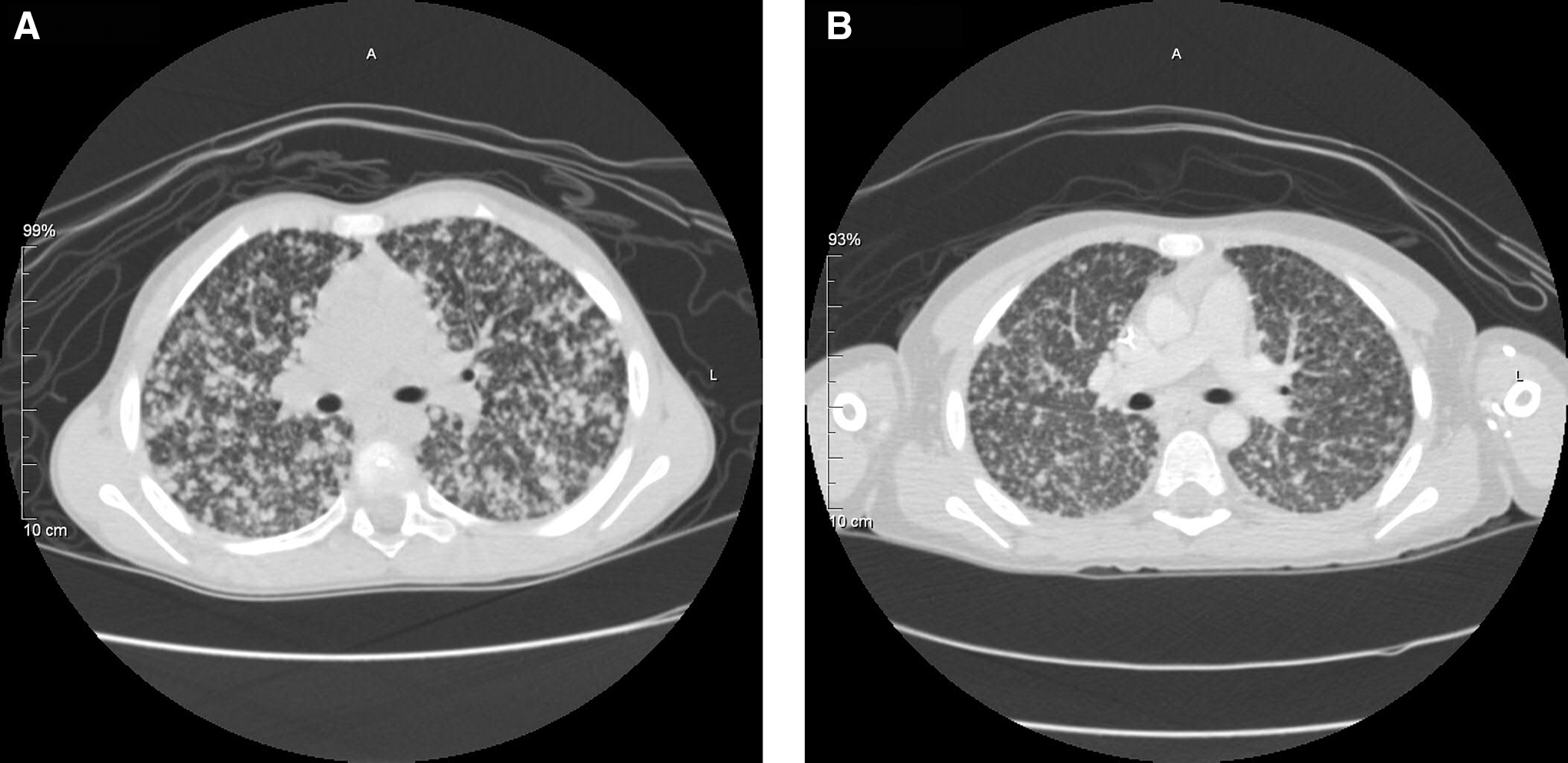
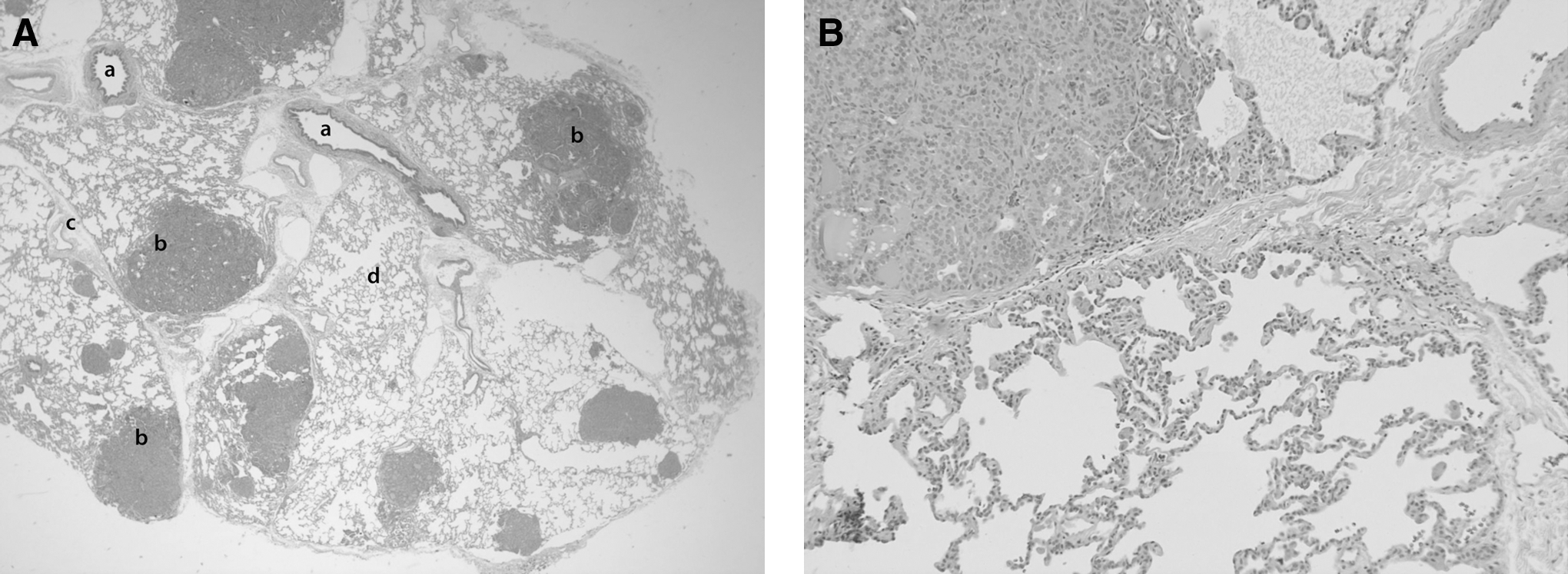
He returned for a follow-up visit with the pulmonologist in late August 2009, four weeks after hospital discharge. He was afebrile, but oxygen saturations were 85–89% on room air. Thus, he was re-admitted for further evaluation. The repeat chest x-ray (Fig. 1B) did not show any significant improvement from the initial chest radiograph. Viral PCR from nasal washings was negative for influenza A. High-resolution computerized tomography (CT) scan of the neck and chest showed multiple necrotic lymph nodes on the right aspect of the neck and multiple nodules throughout the lungs measuring 1–4 mm (Fig. 2A). Given the results of the extensive work-up on his previous admission, the decision was made to proceed with lymph node and lung wedge biopsy. Pathology of the left lung wedge resection and the right deep cervical node (2 cm×1 cm) biopsy revealed numerous metastatic tumor nodules that were solid and glandular with follicular architecture. Tumor cells had nuclear grooves, inclusions, and psammoma bodies consistent with extensive metastatic papillary thyroid carcinoma (Fig. 3A). Lung parenchyma was not involved by tumor and no lymphocytic infiltration of the interstitium was noted. There was no diffuse alveolar damage or fluid in the airspace. There was some compression and invasion of the alveolar space (Fig. 3B) and occasional atelectasis was present adjacent to the tumor.
A preoperative staging with CT scan of neck and chest noted disease in levels II, III, IV, V, VI, and VII, a staging of T4b, N1b, and M1. In early September 2009, the boy underwent a total thyroidectomy with a central neck dissection, but the tumor that was densely adherent to the carotid artery was left behind. Tumor cells were negative for a somatic BRAF mutation in exons 11 and 15. Treatment with levothyroxine, calcium, and calcitriol for hypothyroidism and hypoparathyroidism was initiated. Preoperatively, the boy was intubated and required continued mechanical ventilation for respiratory insufficiency postsurgery. Despite therapy with high-dose glucocorticoids and sildenafil (for assistance in weaning off of nitric oxide), he was unable to be successfully weaned from mechanical ventilation. He had a persistently elevated oxygen requirement (FiO2 of 69%) in the pressure regulated volume control (PRVC) mode with the following settings: tidal volume 200 mL, positive end expiratory pressure (PEEP) 10, and rate of 18.
Because conventional therapy with 131I was not feasible given his clinical condition requiring intensive care unit admission, treatment with sorafenib was explored. After extensive discussion with the family regarding potential risks and benefits of the therapy, the off-label use of sorafenib 200 mg daily (200 mg/m2) was initiated 11 days after surgery. Serial biochemical studies, including complete blood count, electrolytes, phosphorous, liver function tests, amylase, and lipase, were unremarkable. Thyroglobulin values were reported as above 3000 ng/mL with positive thyroglobulin antibodies; however, the dose of levothyroxine was not a thyrotropin (TSH)-suppressive dose (3.6–50.6 IU/mL). The patient developed mild desquamation of the hands and feet, but overall he tolerated sorafenib therapy well. After 8 days of sorafenib administration, mechanical ventilation was weaned to extubation settings (in PRVC mode FiO2 of 28%, tidal volume 200 mL, PEEP 6, and rate of 4) and the child was extubated; however, extubation failed because of severe supraglottic edema. Seven days later, a tracheostomy tube was placed, but resulted in bilateral pneumothoraces. Thereafter, recovery was slow due to needs for sedation, chest tube drainage, and acquisition of endotracheal Klebsiella pneumoniae and Pseudomonas aeruginosa infections. On the basis of the clinical condition of continued pulmonary support and persistence of elevated thyroglobulin levels, the sorafenib dose was increased to 200 mg twice daily (400 mg/m2), 30 days after initiation of sorafenib. Ten days later, he no longer required oxygen supplementation.
As the child no longer required respiratory support, in preparation for 131I treatment, residual disease was reassessed with thyroid ultrasonography that noted a 4.2 cm×1.5 cm×1.8 cm mass within the right thyroid bed. A follow-up CT scan with and without contrast of the neck and chest confirmed residual soft tissue in the posterior right thyroid bed with adenopathy behind the right carotid sheath, posterolateral to the right carotid sheath, and extending into the suprahyoid region, and it revealed multiple pulmonary nodules (1–2 mm) (Fig. 2B). The neck lesions were excised in a second surgical procedure that revealed matted nodes and scar tissue in the right paratracheal region with extension into the thoracic inlet superior to the subclavian vein with nodes into the right jugulodigastric region. Pathology revealed papillary thyroid carcinoma (diffuse sclerosing variant) with dense fibrous tissue and metastatic to three of the seven lymph nodes. He recovered from this surgery without pulmonary support within 24 hours. He was discharged home on sorafenib, levothyroxine, calcitriol, calcium (for postsurgical hypoparathyroidism), and sildenafil (on a weaning regimen) after 2.5 months of hospitalization. Nineteen days after the second surgery, the quantitative thyroglobulin (with negative antibodies) level was 691 ng/mL with a concomitant TSH of 0.5 IU/mL.
In preparation for ablation of residual PTC with 131I, the child was placed on a low-iodine diet for two weeks. One week before the administration of 131I, sorafenib was discontinued. Rather than discontinuing thyroxine before ablation, the patient received two doses of recombinant human TSH (Thyrogen; Genzyme, Cambridge, MA), and treatment with prednisone for five days. In December 2009, he received 100 mCi of 131I. One week postablation, the scan revealed extensive uptake throughout the lungs and the thyroid bed, supraclavicular nodes, and cervical nodes.
After 131I treatment, the patient continued on levothyroxine, calcitriol, and calcium with serial monitoring with physical examination, thyroid studies, thyroglobulin values, comprehensive metabolic panel including phosphorous, and complete blood count measurements. Between December 2009 and June 2010, quantitative thyroglobulin values increased from 691 to 2053 ng/mL. A second treatment with 100 mCi 131I was orally administered in September 2010. Nine days post-treatment, the whole body scan showed activity in the right neck, mediastinum, and lungs with possible decrease in lung activity. Although the tumor appeared 131I-avid, 20-days post-treatment, a positron emission tomography scan was performed to look for other disease manifestations that is not 131I-avid. It showed scant evidence of metabolic activity. Thyroglobulin levels continued to be elevated between 1828 and 2592 ng/mL 5 months after the second dose of 131I (with TSH values averaging of 0.7 IU/mL) and the child required supplemental oxygen. Thus, after discussion, re-treatment with sorafenib was considered. In February 2011, sorafenib (200 mg twice daily) was reinstituted. Within one month, on suppressive levothyroxine therapy, quantitative thyroglobulin values decreased from 2592 to 767 ng/mL and within 4 months, the thyroglobulin levels declined to ∼200 ng/mL and they remain at this level at the time of the writing of this article (December 2012). The patient has not required oxygen since May 2011. He continues on sorafenib 200 mg twice daily with cycles of 3 weeks on and 1 week off medication since May 2011.
Discussion
Here we describe an eight-year-old boy with PTC metastatic to lymph nodes and lung parenchyma with persistent respiratory distress and hypoxemia. The presence of diffuse nodular metastatic PTC throughout the pulmonary parenchyma may have contributed to respiratory insufficiency. Although initially it appeared that this child's presentation was due to infection with H1N1 virus, during the second hospitalization, respiratory distress persisted, as did hypoxemia in the absence of evidence of H1N1 infection. Further, the chest radiographs of patients with H1N1 viral infection do not reveal peripheral nodular opacities; rather, they display enhanced peribronchial markings or multifocal areas of consolidation (13).
Although other lung diseases should be considered, extensive evaluation during his first admission did not reveal any other infectious, autoimmune, or genetic causes for his pulmonary disease. Furthermore, pathology evaluation of the lung biopsy did not show signs of viral pneumonia or acute respiratory distress syndrome such as lymphocytic infiltration of the interstitium or edematous air space, respectively. Presence of bloody effluent with fresh red blood cells but without hemosiderin staining suggests a fresh bleed during the lavage rather than a previous pulmonary hemorrhage.
In retrospect, the initial report in the BAL study noted reactive bronchoalveolar hyperplastic aggregates, which were likely tumor clusters. Although it has been suggested that the diagnosis of PTC could be made on cytopathology evaluation on a BAL specimen (14), it was not until re-evaluation that we appreciated that these cells were originating from papillary thyroid carcinoma.
We postulate that the compression and invasion of the air space with tumor cells led to the ventilation–perfusion mismatch. This observation leads to the hypothesis that the metastatic PTC could have led to severe hypoxemia requiring mechanical ventilation. We believe that in such cases, treatment with sorafenib could be considered for gap therapy while the patient recovers pulmonary function.
Although experience with sorafenib in pediatric patients is limited, there are few published reports of its use in the pediatric age population (15 –18). Waguespack and colleagues (18) described the successful treatment of a 14-year-old patient with progressive PTC. Widemann et al. (19) reported the results of a Children's Oncology Group Phase I trial of sorafenib in children with refractory solid tumors. The maximum tolerated dose in children with refractory solid tumors was 200 mg/m2. Only one of the six enrolled patients at this maximum tolerated dose level experienced dose-limiting toxicity—specifically, grade 3 liver alanine aminotransferase levels. However, there were no tumor responses to sorafenib in these heavily pretreated subjects (19). Children's Oncology Group recently completed enrollment on a phase II study of sorafenib, but the results are not yet available.
In PTC, treatment with sorafenib is usually reserved for patients with advanced non-131I-avid PTC. It was utilized in our patient during weaning from mechanical ventilation before treatment with 131I as well as post-treatment for continued reduction of thyroglobulin levels, and to avoid oxygen supplementation. During the initial administration of sorafenib, the child's pulmonary function improved dramatically, and he was discharged home without mechanical ventilation to proceed with 131I therapy. In our patient, sorafenib therapy was remarkably well tolerated. Aside from a moderate hand–foot skin reaction, no adverse events were noted. The patient's rash responded to treatment with moisturizing lotions without requiring additional interventions.
In our patient, treatment with an MKI did not seem to adversely affect the uptake of 131I based on the extensive uptake in the lungs on postablation scintigraphy studies. The positron emission tomography scan obtained after the second 131I therapy did not reveal additional tumor metabolic activity, and we interpret this as the tumor being responsive to 131I treatment. Hoftijzer et al. showed that in patients with PTC refractive to treatment with 131I, re-induction of responsiveness to this isotope could not be induced by sorafenib (7). Therefore, it seems likely that sorafenib neither increases nor decreases the avidity of PTC for iodine.
Quantitative thyroglobulin measurements are also helpful in monitoring the PTC disease state. In our patient, however, the thyroglobulin levels were initially higher than the assay limits and thus reported as above 3000 ng/mL. Further, the presence of thyroglobulin antibodies can interfere with the assay and result in false low serum thyroglobulin concentrations. For these reasons, in our patient, it was difficult to correlate disease extent to thyroglobulin levels early in the treatment.
Interestingly, our patient's tumor analysis did not show a BRAF mutation. However, in pediatric patients with PTC the most common oncogene is a rearrangement of RET/PTC leading to the activation of the RAF kinase pathway (14,20,21). Thus, the clinical response to treatment with sorafenib is likely still due to an effect on RAF kinase, or perhaps additionally by its effects on other tyrosine kinase receptors.
In conclusion, this case demonstrates that sorafenib could be considered in rare situations when definitive therapy needs to be delayed and/or in patients with progressive 131I-refractory PTC (18). This agent was easy to administer orally and in our experience only caused acute moderate dermatologic toxicity. Targeted therapy with multikinase inhibitors may have a role in the treatment of thyroid cancer in children as gap therapy or as adjuvant therapy in selected cases of advanced or complicated disease.
Footnotes
Acknowledgments
The authors would like to acknowledge the superb clinical care provided by the numerous physicians, nurses, and allied healthcare providers at All Children's Hospital. We would especially like to thank Dr. Waguespack for his willingness and expertise in assistance in the care of this patient. We also appreciate the pathology slides provided by Dr. Kenneth Washington, radiographic interpretation by Dr. Javier Quintana, and the 131I therapy provided by Dr. Brent Price. We appreciate Drs. Dorothy Shulman and Allen Root's mentorship in clinical guidance and in preparation of this article. We thank Mr. Mike Sexton for help with figure preparation. Most of all, we thank the patient and his family for letting us take part in his care.
Author Disclosure Statement
The authors do not have any financial interest to disclose.