
Abstract

A 52-year-old woman was investigated for persistently high serum thyroglobulin after total thyroidectomy. Her medical history was significant for systemic lupus erythematosus (SLE) and also indolent cutaneous marginal zone B cell lymphoma (MZL). Her SLE, which featured intermittent joint pain and lymphadenopathy, had been diagnosed 16 years earlier and was quiescent under treatment with hydroxychloroquine. Her MZL, which had presented five years earlier as a swelling on her left thigh, had been treated with surgical excision and localized external beam radiotherapy to the affected area. MZL recurred four years later in the right buttock. It was treated with external beam radiotherapy and rituximab. A subsequent positron emission tomography (PET) scan, performed as part of routine monitoring for recurrence of MZL, detected a lesion in the left lobe of the thyroid. Fine-needle aspiration biopsy of the lesion revealed cytology consistent with papillary carcinoma of the thyroid. She underwent total thyroidectomy with central lymph node clearance and was commenced on thyroxine.
The final pathology showed an 8 mm classical papillary carcinoma with one of two central lymph nodes involved. She underwent thyroid remnant ablation with 4 GBq of radioactive iodine (RAI) with stimulation by recombinant human thyrotropin (rhTSH). The posttherapy scan showed uptake in the thyroid bed but no metastatic disease. Her baseline postsurgical serum thyroglobulin was 290 μg/L, and it rose to 831 μg/L after RAI with rhTSH. She tested negative for thyroglobulin antibodies. Eight months later, her thyroglobulin was 597 μg/L. She underwent an off T3 surveillance scan, which showed a faint diffuse accumulation of tracer in the thyroid bed. She was given a treatment dose of 4.2 GBq RAI. However, the posttreatment scan showed no uptake of tracer in the thyroid bed. The high serum thyroglobulin prompted further evaluation with a PET scan, which showed mildly increased tracer uptake in multiple bilateral small upper cervical lymph nodes and one small right infraclavicular lymph node. The same lymph nodes were identified on a computed tomography (CT) scan of the neck and chest. Ultrasound-guided biopsy of the cervical lymph nodes showed mixed lymphoid cells with no evidence of thyroid carcinoma. Despite the negative biopsy findings, the cervical lymph nodes were still considered to be the likely source of thyroglobulin.
Sixteen months after her initial thyroidectomy, she had a bilateral level 2–5 neck dissection with additional clearance of the right central lymph nodes. Surgery was complicated by left-sided Horner's syndrome. There was no evidence of malignancy in any of the 28 lymph nodes removed. Serum thyroglobulin remained elevated at 184 μg/L.
A year later, a surveillance CT scan found a new mixed-density soft-tissue nodule in the lower neck extending into the suprasternal notch. Fine-needle aspiration biopsy of the lesion showed a small number of highly atypical cells with nuclear features suggestive of papillary thyroid carcinoma. An 18F-fluorodeoxyglucose (FDG)–positron emission tomography (PET)/CT scan confirmed the soft-tissue mass in the suprasternal notch and also found an FDG avid subcarinal lymph node and multiple soft-tissue deposits in the lower limbs. An inguinal lymph-node biopsy discovered a recurrence of MZL, and the patient was given a further course of rituximab. A third neck operation to excise the suprasternal lesion identified and removed a group of level 7 pretracheal and thymic lymph nodes. However, the final histopathology revealed that the lymph nodes contained MZL and not papillary thyroid carcinoma.
Repeated neck ultrasound did not reveal any likely source for the detectable thyroglobulin. After further interdisciplinary discussion, the patient received a further dose of RAI following rhTSH. A PET scan was also performed. However, both PET and RAI iodine scans failed to demonstrate abnormal uptake. After rhTSH stimulation, thyroglobulin paradoxically decreased (see Fig. 1), and this raised the possibility of assay interference.
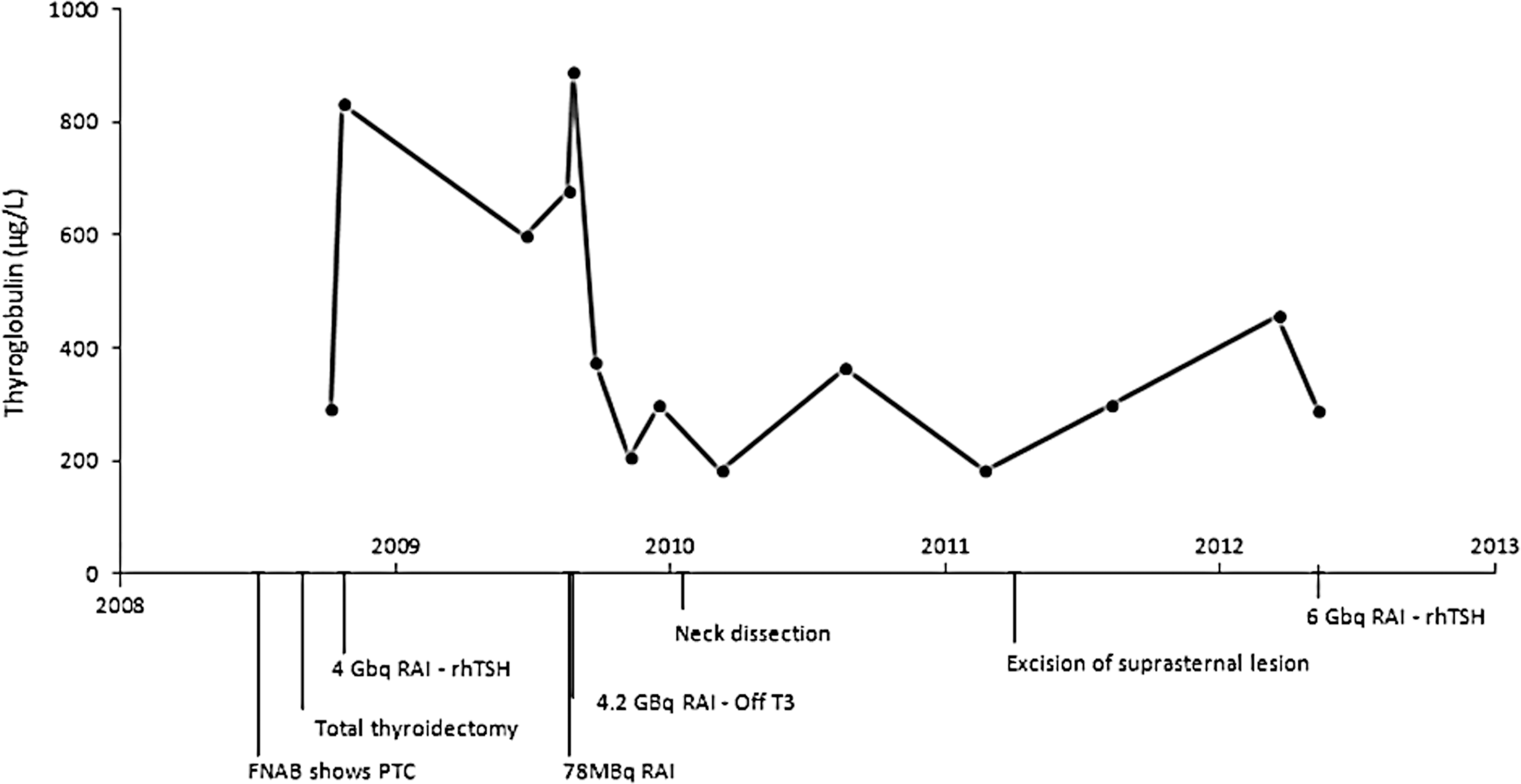
Thyroglobulin levels over time.
In subsequent assays, the sample was found to have poor linearity on serial dilutions. Although thyroglobulin had been tested at two different laboratories, they both used the same method (Siemens Immulite 2000). Repeat testing after incubation with a commercial heterophile antibody blocking preparation gave a result of 2.2 μg/L. Testing the sample with an alternate method (ElisaRSR Tg) produced a thyroglobulin result of 0.05 μg/L.
Heterophile antibodies are weak avidity, multispecific antibodies against poorly defined antigens. Some bind the antibody components of immunoassays and hence cause positive or negative interference. The reported prevalence of heterophile antibody interference in modern thyroglobulin assays ranges from 0.03% to 3% (1 –4). Interference rates vary according to the assay method as well as the patient population.
Artifactual elevation of tumor markers such as thyroglobulin may lead to unwarranted diagnostic procedures or therapy. Heterophile antibodies should be considered when thyroglobulin measurements are not consistent with clinical and imaging findings.
Footnotes
Author Disclosure Statement
No competing financial interests exist.