
Abstract
Background:
Chemokine (C-X-C motif) ligand (CXCL)9 and CXCL11 play an important role in the initial phases of autoimmune thyroiditis (AT); however, their serum levels in patients with Graves' disease (GD) have never been evaluated in relation to thyroid function and treatment.
Methods:
To evaluate CXCL9 and CXCL11 serum levels in GD and to relate these parameters to the clinical phenotype, we measured CXCL9 and CXCL11 serum levels in 91 GD patients; 91 AT, 34 nontoxic multinodular goiters (MNGs), 31 toxic nodular goiters (TNGs), respectively; and 91 healthy controls (age- and sex-matched).
Results:
Mean CXCL9 and CXCL11 levels were higher in GD in comparison with controls, euthyroid AT, MNG, or TNG (p<0.05, ANOVA; CXCL9: 274±265, 76±33, 132±78, 87±48, and 112±56 pg/mL; CXCL11: 140±92, 64±20, 108±48, 76±33, 91±41 pg/mL, respectively). Hyperthyroid GD patients had significantly higher CXCL9 or CXCL11 than euthyroid or hypothyroid GD patients. GD patients with untreated hyperthyroidism had higher CXCL9 or CXCL11 than hyperthyroid or euthyroid GD patients under methimazole (MMI) treatment. Comparable CXCL9 and CXCL11 levels were observed in newly diagnosed untreated hyperthyroid GD versus untreated patients with relapse of hyperthyroidism after a previous MMI course.
Conclusions:
Serum CXCL9 and CXCL11 levels are associated with the active phase of GD both in newly diagnosed and relapsing hyperthyroid patients. The reduction of serum CXCL9 and CXCL11 levels in treated patients with GD may be related to the immunomodulatory effects of MMI.
Introduction
Th1 cells tend to produce the proinflammatory responses responsible for killing intracellular parasites and for perpetuating autoimmune responses, whereas Th2 cells are associated with the promotion of humoral immunity and of IgE and eosinophilic responses. The production of transforming growth factor (TGF)-β and IL-6 promotes the development of Th17 cells, a distinct type of effector T cell that induces tissue damage. Once Th17 cells are established, IL-23 also participates in their maintenance. Treg cells, which inhibit autoimmunity and protect against tissue injury, are induced by TGF-β in the absence of IL-6. Thus, TGF-β functions as a regulator of tissue-damaging Th17 cells when collaborating with IL-6 and as an activator of anti-inflammatory Treg cells when acting without IL-6 (1).
Chemokines are defined as small (8–15 kDa) proteins that induce chemotaxis and in some instances modulate the functional properties of different leucocytes during inflammation. Chemokines are grouped into four distinct families according to the number and spacing of two conserved N-terminal cysteine residues. Two chemokine families have multiple members: the CXC (two N-terminal cysteines separated by a single amino acid) family and the CC (two N-terminal cysteines adjacent) family. The remaining CX3C and C families each contain a single member only, CX3CL1 (fractalkine) and XCL1 (lymphotactin), respectively. The CXC chemokines are additionally subdivided into those that contain a glutamic acid-leucine-arginine (ELR) motif near their N-terminus (e.g., CXCL1 and CXCL8), and those that do not contain this motif. The non-ELR CXC chemokines can be further subgrouped based on their structure and target receptor. Three structurally related chemokines comprise the IFN-inducible non-ELR CXC chemokine subgroup: chemokine C-X-C motif ligand (CXCL)9, CXCL10, and CXCL11 (1 –5).
A number of properties distinguish CXCL9, 10, and 11 from the other non-ELR CXC chemokines and show that these chemokines are closely related. First, these molecules exhibit significant structural homology being more similar to each other than to any of the other non-ELR CXC chemokines (2). Second, the genes for these chemokines are all highly inducible by IFN-γ. Third, all three chemokines share the ability (albeit to varying degrees) to promote the directional migration of activated and memory, but not naive T cells. Finally, CXCL9, 10, and 11 all bind to a common receptor named CXCR3. Thus, these chemokines are considered appropriately as a distinct subfamily (3 –5).
Two distinct domains that contribute to CXCR3 internalization have been identified. The carboxyl-terminal domain and beta-arrestin1 are predominantly required by CXCL9 and CXCL10, and the third intracellular loop is predominantly required by CXCL11 (6). CXCR3 chemokines play an important role in the initial phases of Graves' disease (GD) and autoimmune thyroiditis (AT) (1).
The CXC α chemokines inducible by IFN-γ, CXCL9, CXCL10, and CXCL11 are associated with Th1-mediated immune responses. Among them, CXCL10 is a prototype, and its serum levels are increased in several endocrine autoimmune conditions (7 –10).
Recent experimental evidence has demonstrated that CXC chemokines and particularly CXCL10 play an important physiopathological role in the initial phases of autoimmune thyroid disorders (8,11,12).
Expression of CXCL10 and CXCL9 is poor or absent in normal thyroid tissue, while both the chemokines and their receptor are present in most thyroid glands of patients affected by GD. CXCL10 and CXCL9 localize to infiltrating lymphocytes and macrophages, as well as to resident epithelial follicular cells. Of note, maximal expression of CXCL10 and CXCL9 was found in the thyroid gland of patients with recent-onset GD and correlated with IFN-γ (8,13). At the same time, it was shown that human thyrocytes in primary culture produce large amounts of CXCL10 when stimulated by IFN-γ (11).
We have previously shown that CXCL10 is associated with the active phase of GD, both in newly diagnosed and relapsing hyperthyroid patients, and that the reduction of circulating CXCL10 in treated patients with GD may be related to the immunomodulatory effects of methimazole (MMI) (14,15).
Increased expression of CXCL10 and CXCL9 was also observed in thyroid tissue specimens obtained from subjects affected by AT by immunohistochemistry (11), and high levels of CXCL9 and CXCL11 have recently been shown in patients with AT, in particular in the presence of hypothyroidism (16 –18). Furthermore, we have recently shown that IFN-γ and TNF-α are able to induce the secretion of the CXCL9 and CXCL11 chemokines in thyrocytes and fibroblasts of patients with GD and ophthalmopathy (19 –21).
Briefly, it has been hypothesized that Th1 cells secreting these chemokines (CXCL9, 10, 11) were originally attracted to the thyroid gland because of the thyroid autoantigens. In the thyroid, Th1 cells produce cytokines (such as IFN-γ and TNF-α) that can modulate the autoimmune response inducing the production of CXCL9, CXCL10, and CXCL11 chemokines not only by lymphocytes, but also from thyrocytes. These chemokines induce the migration of other Th1 lymphocytes into the thyroid, which in turn, secrete more IFN-γ and TNF-α, further stimulating the chemokine production by the target cells, thus initiating and perpetuating the autoimmune cascade.
To our knowledge, no study has systematically evaluated the IFN-γ inducible CXCL9 and CXCL11 chemokines in patients with GD in relation to thyroid function and treatment. The aim of the present study therefore was to measure serum CXCL9 and CXCL11 levels in patients with GD and to relate the findings to the clinical phenotype, in order to assess the potential benefit of routine assessment of these chemokines in the clinical management of such patients.
Materials and Methods
Patients
From the outpatient clinic, we prospectively studied 91 consecutive Caucasian patients with GD, without clinical signs or symptoms of Graves' ophthalmopathy (Table 1). The patients were referred to us by general practitioners or other hospitals because of the presence of hyperthyroidism or circulating thyroid autoantibodies or due to clinical suspicion of a thyroid disorder. The diagnosis of GD (14,15) was established from the clinical presentation (presence of a diffuse goiter, varying in size from normal to very large), thyroid hormones, and thyroid autoantibodies measurements (presence of antithyrotropin-receptor autoantibodies [TRAb], and/or thyroid ultrasonography [decreased, dyshomogeneous echogenicity, and diffuse goiter]). The majority of these patients had goiter (61%), the others showed a normal thyroid volume. A minority of patients (7%) were submitted to fine-needle aspiration (FNA) of thyroid nodules to exclude the presence of thyroid cancer or lymphoma; in these cases, cytology excluded the presence of a malignancy.
Mean group values were compared by ANOVA for normally distributed variables, otherwise by Kruskal-Wallis test. Proportions were compared by the χ2 test. Post hoc comparisons on normally distributed variables were carried out using the Bonferroni-Dunn test.
p≤0.05 vs. controls or vs. autoimmune thyroiditis.
p≤0.05 vs. controls and vs. multinodular goiters.
p≤0.05 vs. controls, vs. autoimmune thyroiditis, and vs. multinodular goiters.
p≤0.05 vs. controls.
TPOAb, antithyroperoxidase antibody; TgAb, antithyroglobulin antibody; TRAb, antithyrotropin-receptor antibody.
Among the GD patients, 31 were untreated hyperthyroid patients (11 had a relapse of hyperthyroidism after a MMI course of 8–31 months), 50 were in treatment with MMI (2–34 months duration), while the other 10 were euthyroid and in remission after a previous course of MMI therapy of 1–36 months duration.
In terms of thyroid function, 48 were hyperthyroid (low thyrotropin [TSH] associated with high levels of free triiodothyronine [FT3] and/or free thyroxine [FT4]), 34 were euthyroid (normal TSH, FT3 and FT4), and 9 were hypothyroid (high TSH, with normal or low levels of FT4 and/or FT3) while being treated with MMI.
Controls
We used two different controls to compare the features of GD not associated with hyperthyroidism (Comparison 1) and those associated with hyperthyroidism (Comparison 2). The necessity for two different comparisons was due to the mean age of GD patients being 41 years (Table 1), while the mean age of patients with toxic nodular goiter (TNG) collected in the same period (used as control group of hyperthyroid GD) was 55 years; since serum CXCL10 levels are higher in older subjects (9), the Comparison 2 group excluded patients younger than 45 years in controls, with thyroiditis and GD, and with a matched age.
Comparison 1
Three control groups were used (Table 1). The first control group (controls I, n=91) consisted of a random sample of the general population (matched by sex and age±2 years, with GD patients) from the same geographic area in whom a complete thyroid work-up (history, physical examination, TSH, FT3, FT4, antithyroglobulin [TgAb] and antithyroperoxidase [TPOAb] antibody measurements, and ultrasonography) was available, and excluded the presence of thyroid disorders.
A second control group was made by 91 patients with euthyroid chronic AT (matched by sex and age±2 years, with GD patients; Table 1). The diagnosis of AT (22) was established from the clinical presentation (presence of a firm goiter, varying in size from small to very large, with a lobulated surface), thyroid hormones and thyroid autoantibodies measurements, and/or thyroid ultrasonography (decreased, dyshomogeneous echogenicity).
A third control group comprised 34 patients with nontoxic multinodular goiter (MNG) extracted from the same random sample of the general population (matched by sex and age ±2 years, with GD patients). The majority of these patients had a normal thyroid volume, some showed goiter (41%). All these patients were submitted to FNA to exclude the presence of thyroid cancer; cytology confirmed the absence of a malignancy.
Comparison 2
In the same period we collected the clinical history and the blood samples of 31 patients affected by TNG (diagnosed by thyroid scintigraphy) (Table 2). All patients were hyperthyroid, and the majority of them had a goiter (69%). All these patients were submitted to FNA to exclude the presence of thyroid cancer; cytology confirmed the absence of a malignancy. Owing to the fact that the mean age of the patients with TNG was 55 years and that serum CXCL9 levels are higher in older subjects, Comparison 2 was made by matching TNG patients by age (±3 years) and sex with controls (i.e., hyperthyroid patients with GD, or thyroiditis; Table 2).
Mean group values were compared by ANOVA for normally distributed variables, otherwise by Kruskal-Wallis test. Proportions were compared by the χ2 test. Post-hoc comparisons on normally distributed variables were carried out using the Bonferroni-Dunn test.
p≤0.05 vs. controls or autoimmune thyroiditis.
p≤0.05 vs. controls and vs. toxic nodular goiter.
p≤0.05 vs. controls, vs. autoimmune thyroiditis, and vs. toxic nodular goiter.
p≤0.05 vs. controls.
TSH, thyrotropin.
In all patients and controls, a blood sample was collected in the morning, after overnight fasting, and serum was kept frozen until thyroid hormones, TSH, thyroid autoantibodies, and CXCL9 and CXCL11 measurements.
All study subjects gave their informed consent to participate in the study, which was approved by the local Ethical Committee.
Ultrasonography of the neck and FNA
Neck ultrasonography was performed by the same operator, who was unaware of the results of thyroid hormone, autoantibody, and CXCL10 measurements (Esaote, Florence, Italy; AU5 with a sectorial 7.5 MHz transducer). Thyroid volume was calculated using the ellipsoid formula, as previously described (14,15). The presence of hypoechoic and dyshomogeneous echogenicity was arbitrarily rated at three levels (0=normal echogenicity; 1=slightly hypoechoic and dyshomogeneous; 2=severely hypoechoic and dyshomogeneous) in order to evaluate structural abnormalities of thyroid tissue associated with thyroid autoimmunity (14,15). The presence of thyroid nodules was recorded, and nodules with a diameter >10 mm were submitted to ultrasonography-guided FNA, which was performed by the same operator, using a free-hand method as already described (14,15).
Thyroid blood flow
Thyroid blood flow (TBF) by color-flow Doppler (CFD) was studied in all patients (14,15). The CFD pattern was defined as normal (or type 0) of TBF was limited to peripheral thyroid arteries; type I, TBF mildly increased; type II, TBF clearly increased; or type III, TBF markedly increased (14,15).
Laboratory evaluation
Thyroid function and thyroid autoantibodies were measured as previously described (22). Circulating FT3 and FT4 were measured by commercial radioimmunoassay kits (AMERLEX-MAB FT3/ FT4 Kit; Amersham, UK). Serum TSH (DiaSorin, MN, USA) and TPOAb and TgAb (ICN Pharmaceuticals, CA, USA) were evaluated by immunoradiometric assay methods. TRAb autoantibodies were measured with the use of a radioreceptor assay (Radim, Pomezia, Rome, Italy) (normal range 0–1 IU/mL). For TgAb and TPOAb, positivity was set at >50 and >10 IU/mL, respectively.
Serum CXCL9, CXCL11, IFN-γ, and CCL2 levels by ELISA
Serum CXCL9 levels were assayed by a quantitative sandwich immunoassay using a commercially available kit (R&D Systems, Minneapolis, MN), with a sensitivity ranging from 9.0 to 15.5 pg/mL and a mean minimum detectable dose of 5.6 pg/mL. The intra- and interassay coefficients of variation were 4.7% and 5.8%.
Serum CXCL11 levels were assayed by a quantitative sandwich immunoassay using a commercially available kit (R&D Systems), with a sensitivity ranging from 2.1 to 4.5 pg/mL and a mean minimum detectable dose of 12.1 pg/mL. The intra- and interassay coefficients of variation were 4.9% and 6.8%.
IFN-γ (Th1 cytokine) and CCL2 (Th2 chemokine) concentrations were also measured in serum using commercially available kits (R&D Systems). The mean minimum detectable level was 2.5 pg/mL for IFN-γ and 4.6 pg/mL for CCL2; the respective intra- and interassay coefficients of variation were 3.1% and 5.9% for IFN-γ and 4.3% and 5.2% for CCL2.
Data analysis
Values are given as mean±SD for normally distributed variables, otherwise as median and interquartile range. Mean group values were compared by ANOVA for normally distributed variables, otherwise by the Mann-Whitney U or Kruskal-Wallis test. Proportions were compared by the chi-square test. Post hoc comparisons of normally distributed variables were carried out using the Bonferroni-Dunn test. Multivariate analysis was performed by multiple linear regression analysis using CXCL9 or CXCL11 as the dependent variable and age, TSH, and FT3 as covariates.
Results
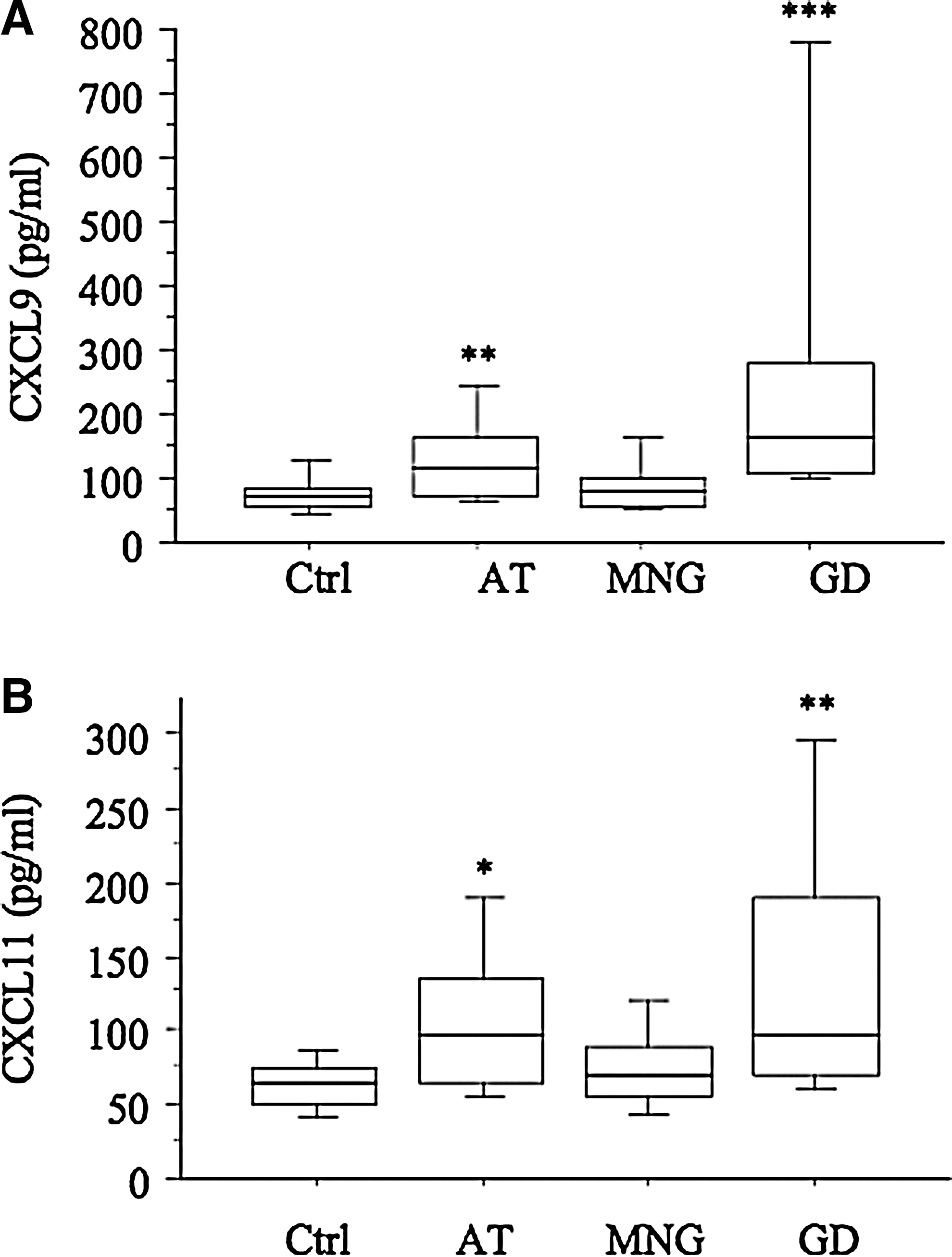
The demographic and clinical features of GD patients and controls are reported in Table 1. The mean CXCL9 levels were significantly higher in patients with GD, than in controls or in patients with euthyroid AT or MNG (Fig. 1).
Distribution of serum CXCL9
In GD patients, serum CXCL9 levels were significantly higher in patients older than 50 years (p=0.043, ANOVA), in GD patients with a hypoechoic pattern (55%; p=0.012, ANOVA), and in those with hypervascularity (68%; p=0.015, ANOVA; Table 3), while no significant difference was observed in relation to the presence of goiter, TPOAb, TgAb, or TRAb positivity. In a multiple linear regression model including age, TSH, and FT3, only age and FT3 were slightly but significantly related to serum CXCL9 levels (Table 4).
FT3, free triiodothyronine; CI, confidence interval.
Patients with GD and hyperthyroidism had significantly higher CXCL9 levels than euthyroid or hypothyroid GD patients (p=0.01, ANOVA; Fig. 2A), lower TSH (p<0.001), and higher FT4 (p<0.001), FT3 (p<0.001), and TRAb levels (p<0.001), and higher degrees of hypervascularity (p=0.001) (Table 5), while there was no significant difference in thyroid volume, echogenicity, and TgAb and TPOAb titers.

Patients with GD and hyperthyroidism (Hyper) had significantly higher CXCL9
GD patients with untreated hyperthyroidism had higher CXCL9 levels than hyperthyroid patients treated with MMI, or euthyroid patients treated with MMI (p=0.001, ANOVA; Fig. 3A). CXCL9 levels were not significantly different in newly diagnosed untreated hyperthyroid patients in comparison with untreated patients with relapse of hyperthyroidism after a previous MMI course (Table 3).
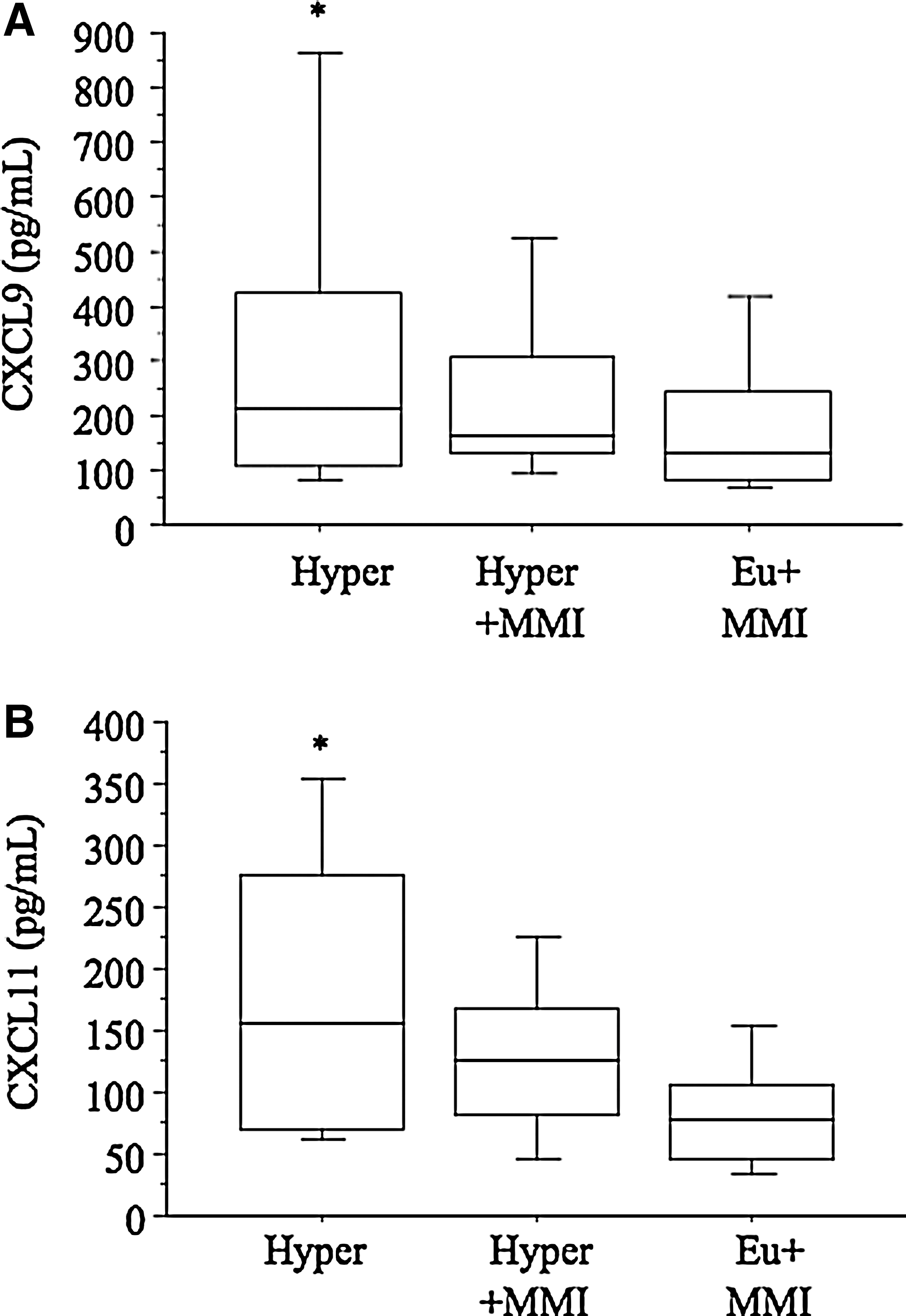
Patients with GD with untreated hyperthyroidism (Hyper) had higher CXCL9
MMI-treated patients who were euthyroid had higher CXCL9 levels than patients in remission of hyperthyroidism without treatment (p=0.001, ANOVA; Table 3).
By defining a high CXCL9 level as a value of at least 2 SD above the mean value of the control group (>142 pg/mL), 54% of patients with GD, 27% with AT, 3% of controls, and one of the MNG patients had high CXCL9 levels (p<0.001, χ2; Table 1). No relationship was observed between CXCL9 and disease duration.
Patients with GD had higher levels of CXCL9 than patients with euthyroid AT or TNG or age- and sex-matched controls (Table 2).
The mean CXCL11 levels were significantly higher in patients with GD than in controls or MNG patients (Table 1), and they were not significantly different from patients with euthyroid AT (Fig. 1B).
In GD patients, serum CXCL11 levels were significantly higher in GD patients with hypervascularity (p=0.041, ANOVA; Table 3), while no significant difference was observed in relation to the presence of goiter, TPOAb, TgAb, or TRAb positivity.
Patients with GD and hyperthyroidism had significantly higher CXCL11 levels than euthyroid or hypothyroid GD patients (ANOVA, p=0.03 respectively; Fig. 2B).
In a multiple linear regression model, including TSH and FT3, they were not significantly related to serum CXCL11 levels.
Patients with GD had significantly higher levels of CXCL11 than age- and sex-matched controls, while CXCL11 levels were higher, although not significantly, compared with euthyroid AT or TNG patients (Table 2).
GD patients with untreated hyperthyroidism had higher CXCL11 levels than hyperthyroid patients treated with MMI or euthyroid patients treated with MMI (p=0.006, ANOVA; Fig. 3B). CXCL11 levels were not significantly different in newly diagnosed untreated hyperthyroid patients compared with untreated patients with relapse of hyperthyroidism after a previous MMI course (Table 3).
Patients who were euthyroid while being treated with MMI or during remission of hyperthyroidism without treatment showed similar CXCL11 levels (Table 3).
By defining a high CXCL11 level as a value of at least 2 SD above the mean value of the control group (>104 pg/mL), 32% of patients with GD, 27% with AT, 2% of controls, and one of the MNG patients had high CXCL11 levels (p<0.001, χ2; Table 1). No relationship was observed between CXCL11 and the GD disease duration.
No significant relationship was observed between CXCL9 and CXCL11 serum levels in patients with GD by simple regression.
IFN-γ was detectable in the serum of 5% of controls, 6% of MNG patients, 45% of GD patients, and 37% of AT patients (p<0.0001, χ2). IFN-γ levels were similar in GD (12 [5.2–25.4] pg/mL, median and [interquartile range]), and in AT (10.1 [4.1–22.5] pg/mL; p=ns).
No significant relationship was observed among CXCL9, or CXCL11, or IFN-γ serum levels in patients with GD by simple regression.
CCL2 levels were similar in GD (403 [131–734] pg/mL, median and [interquartile range]), in AT patients (354 [154–673] pg/mL), MNG patients (339 [127–801] pg/mL), and controls (371 [143–724] pg/mL; p=ns).
Discussion
The results of the present study confirm that CXCL9 and CXCL11 serum levels are increased in newly diagnosed patients with GD, and demonstrate a strong association with the hyperthyroid phase of the disease, with a decrease of both chemokines with MMI therapy. Furthermore, high levels of CXCL9 and CXCL11 were strongly associated with hypervascularity. The relapse of hyperthyroidism was characterized by CXCL9 and CXCL11 serum levels similar to those observed in newly diagnosed hyperthyroid patients.
Other studies suggest that a prevalent Th1 immune response is involved in AT, while a predominant Th2 response is associated with GD (23 –26).
Our results are in agreement with some studies that have shown a prevalent Th1 immune response in the initial phase of GD (8,15). IFN-γ serum levels were higher in GD patients than in controls, confirming a Th1 involvement in GD and the results of previous studies (27 –29).
The increase of CXCL9 in hyperthyroid patients with GD is in agreement with previous studies showing the involvement of IFN-γ (27), TNF-α (30), and Th1 cytokines in GD (27,31 –35). Furthermore, the increase of serum CXCL9 in hyperthyroid patients with GD is in agreement with the results of another study that found that GD patients who relapsed or went into remission had significantly different levels of CXCL9 (36).
Moreover, it has recently been shown that IFN-γ and TNF-α are able to induce the secretion of the CXCL9 and CXCL11 chemokines in thyrocytes of patients with GD (11,19 –21).
In our series, the increase of CXCL9 and CXCL11 seemed not associated with hyperthyroidism per se; in fact, the serum levels of these chemokines were higher in hyperthyroid Graves' patients than in toxic nodular goiter. Therefore, the reported reduction of circulating CXCL9 and CXCL11 levels under MMI therapy could be reasonably ascribed to the well-known immunomodulatory effect of antithyroid drugs (37,38). This is also in agreement with the results observed for CXCL10 in GD patients treated with MMI (14,15,34).
Recently, it has been shown that MMI inhibits CXCL10 secretion in human thyrocytes. MMI decreased cytokine-induced CXCL10 secretion by reducing TNF-α-induced up-regulation of the IFN-γ receptor (39).
The site of production of CXCL9, CXCL10, and CXCL11 remains to be clarified. Cytokine production has been variably interpreted as sustained by thyroid follicular cells (TFCs) (40), by intrathyroidal lymphocytes (27), or from the activation of humoral reactions in sites other than the thyroid (41,42). However, the MMI-induced reduction of CXCL9 and CXCL11 levels in our GD patients suggests that both intrathyroidal lymphocytes and TFCs could be responsible for CXCL9 and CXCL11 production. These findings are in agreement with the observed reduction of CXCL10 levels after 131I treatment or thyroidectomy in GD patients, which suggests that the thyroid gland itself is the main source of circulating CXCL10 (43,44).
Patients with GD in remission after a previous course of MMI therapy show serum CXCL9 and CXCL11 levels similar to normal controls or euthyroid MNGs, but lower than patients with euthyroid AT. These data are in agreement with previous reports showing that CXCL10 expression was comparable to controls in patients with long-standing GD (8) and suggest that CXCL9, CXCL10, and CXCL11 are transiently involved in the active phase of GD, when an active inflammatory process is present, and the Th1-mediated immune response is prevalent, while it is no more significantly present when remission of the disease is achieved. This finding may be regarded as a result of the negative feedback of Th2 cytokines on IFN-γ production. This switch from a Th1 to a Th2 phenotype already reported in other long-standing autoimmune diseases appears to be present also in GD, in line with a previous report showing that lymphocytes obtained from orbital and thyroid tissue of patients affected by Graves' ophthalmopathy had a predominant Th1 profile, whereas patients with remote onset of hyperthyroidism had a large majority of Th2 lymphocytes (33). However, during relapse of hyperthyroidism, a new increase of CXCL10 is demonstrable, in line with a novel activation of the Th1-mediated immune response.
The increase of CXCL9, CXCL10, and CXCL11 in the active phase of GD is in agreement with findings arisen from previous reports in which these chemokines have been contemporarily assessed in the serum and cerebrospinal fluid of multiple sclerosis (MS) patients, showing significant modification in relation to the clinical phase of disease. Specifically, CXCL10 was higher in acute MS and lower in stable disease, suggesting a pathogenetic role for the chemokine in mediating clinical re-exacerbation of MS (45). In addition, the previously reported inverse correlation between CXCL10 levels and time from last clinical relapse, together with the finding that CXCL9, CXCL10, and CXCL11 are up-regulated during relapse in MS (46 –48), strongly supports this hypothesis.
The increase of CXCL9 and CXCL11 in patients with relapse of hyperthyroidism suggests that CXCL9 and CXCL11 could be used as prognostic markers in patients with GD after the remission of the hyperthyroidism with MMI treatment. Currently, this is typically addressed by the determination of TRAb, which represents the most useful addition to the clinical armamentarium and a low-cost assay in treatment planning; the major hurdle consists in increasing the sensitivity of the available assays for TRAb in order to be applied successfully to a greater proportion of patients with GD (49). We have failed to show a relationship between the differences of CXCL9 or CXCL11 concentrations and the presence of circulating TRAb, TPOAb, or TgAb, suggesting that the activation of the CXCL9 and CXCL11 system may be independent of autoantibody reactions in the thyroid.
Interestingly, circulating levels of CXCL9 in GD patients were higher than those of CXCL11. This finding is in agreement with the results of previous studies that have shown that in primary cultures of thyrocytes, obtained from GD patients, the treatment with TNF-α plus IFN-γ has a significantly higher synergistic effect on CXCL9 secretion than on CXCL11 release and reinforces the hypothesis that the thyroid gland itself is the main source of these chemokines (19,20).
In conclusion, IFN-γ–inducible chemokines CXCL9 and CXCL11 are associated with the active phase of GD both in newly diagnosed and in relapsing hyperthyroid patients. The reduction of circulating CXCL9 and CXCL11 levels in patients with GD treated with MMI may be related to the immunomodulatory effect of MMI. Future longitudinal studies in patients with GD will be necessary to assess the possible use of CXCL9 and CXCL11 serum levels as prognostic markers both in patients treated with MMI or after achievement of remission and as a possible addition to the TRAb assay.
Footnotes
Author Disclosure Statement
No competing financial interests exist.