
Abstract
Background:
Surgery and high-dose radioactive iodine (131I) treatment are the cornerstones in the treatment of differentiated thyroid cancer. Patients without 131I uptake on the post-therapeutic whole body scan (WBS), but with detectable thyroglobulin (Tg) during thyroxine withdrawal (Tg-off), are evaluated with an 18-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) for tumor localization within three months. The yield of 18F-FDG-PET imaging and clinical usefulness of a Tg-off cutoff value to predict a positive scan were assessed.
Methods:
From 2002 to 2011, 52 patients with a negative WBS and concurrent detectable Tg-off were evaluated. Thirty-five PET scans were performed during initial treatment, 17 after recurrent disease. Thirty-two patients were on substitution therapy, 17 were evaluated with endogenous thyrotropin elevation, and 3 after recombinant human thyrotropin stimulation. To determine the Tg-off cutoff value, a receiver operating characteristic curve was used.
Results:
Nine (17%) 18F-FDG-PET scans were true positive, 3 (6%) false positive, 36 (69%) true negative, and 4 (8%) false negative (sensitivity 69%, specificity 92%). In 13%, a true-positive scan resulted in a change in the clinical management. The area under the receiver operating characteristic curve is 0.82 [CI 0.64–0.99] (p<0.01), and the Tg-off cutoff value is 38.00 ng/mL (sensitivity 67%, specificity 95%). Ninety percent of 18F-FDG-PET true-positive patients had a Tg-off >2.00 ng/mL.
Conclusions:
An 18F-FDG-PET within three months after a negative WBS with detectable Tg-off showed additional tumor localization in 17% of the patients, leading to a change in clinical management in 13%. A clinically useful Tg-off cutoff value was not found, but 90% of positive 18F-FDG-PET scans occurred in patients with a Tg-off >2.00 ng/mL.
Introduction
Unfortunately, in some patients with detectable serum thyroglobulin (Tg) levels, the tumor cannot be localized by conventional imaging such as ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), and/or radioactive iodine (131I) whole body scan (WBS). Loss of uptake on the 131I WBS could indicate a loss of the tumors' ability to take up iodine, while the possibility to produce Tg is still preserved, as seen in some dedifferentiated tumors. Also, functional imaging could suffer from limitations of spatial resolution. Lesions smaller than 1 cm are below detection limits and can be missed. Although routine anatomical imaging is much more sensitive with a possibility of detecting subcentimeter lesions, these modalities suffer from low specificity of interpretation based on lesion size criteria alone. Furthermore, the anatomical imaging may even be more hampered by the altered anatomical condition after surgery.
Dedicated functional imaging modalities, like 18-fluorodeoxyglucose positron emission tomography (18F-FDG-PET), using radioactively labeled glucose (8,9) can be useful in visualizing tumor presence at an early stage in this patient group. Many studies have been published regarding the role of the 18F-FDG-PET in detecting residual or recurrent disease and in monitoring disease progression but mostly for tumor detection in WBS-negative, Tg-positive patients, with a reported sensitivity ranging from 57% to 100% and a specificity of 25–100% (9 –14). These studies describe the role of the 18F-FDG-PET in various time spans after the negative WBS; however, none of them focused on the early diagnostic value of 18F-FDG-PET imaging.
To improve the therapeutic yield of early 18F-FDG-PET imaging, patients could be selected based on their Tg level during thyroxine withdrawal (Tg-off) at the time of the post-therapeutic WBS. A correlation between the Tg level and a positive 18F-FDG-PET scan has been described by several authors (15,16). A Tg cutoff value of 10 ng/mL as an optimum level for both sensitivity and specificity is described, however, regardless of stimulated or unstimulated Tg (17 –19).
This study aimed to evaluate the additional value of the 18F-FDG-PET in the early diagnostic workup of DTC patients with a negative post-therapeutic WBS and concurrent detectable Tg-off. The secondary aim was to investigate whether the Tg-off level during 131I therapy can predict a positive 18F-FDG-PET in the early diagnostic phase and, if so, to determine a Tg cutoff value.
Materials and Methods
Patients
Between June 2002 and January 2011, 217 patients with DTC underwent an early 18F-FDG-PET scan at the University Medical Centre Groningen. We retrospectively selected 52 patients with a negative post-therapeutic WBS and either concurrent detectable Tg or Tg antibodies (TgAb) during thyroid hormone withdrawal and an 18F-FDG-PET within three months. We included both stimulated (endogenous and recombinant human thyrotropin [rhTSH]) and unstimulated 18F-FDG-PET scans. Patient characteristics are shown in Table 1 (20). Based on the retrospective design of the study, institutional review board approval was not required according to Dutch law.
Staging followed TNM, 5th edition (20).
T, tumor; N, nodes; M, metastases; SD, standard deviation.
Treatment protocol
All patients diagnosed with DTC were treated as described earlier and, since 2007, according to the Dutch guidelines (21 –23). They underwent total thyroidectomy and lymph node dissection as indicated, followed by Tg-off measurement and high-dose (1850–5550 MBq) 131I treatment (ablation therapy). Initial therapy (surgery and high-dose 131I therapy) was completed if there was no evidence of disease; that is, the diagnostic WBS showed no uptake and Tg became undetectable (<1.00 ng/mL) 3–6 months after the last 131I therapy. The patients then received regular follow-up with Tg-on measurement, clinical examination, and US of the neck. If additional 131I treatment was necessary, a post-therapeutic WBS was performed after 7 (since July 2010) or 10 days (until July 2010). The patients with no uptake on the post-therapeutic WBS (after additional 131I treatment), but with a detectable Tg, received anatomical imaging (US and/or MRI) to localize possible tumor deposits or to visualize a baseline situation according to our standard protocol. For patients in whom tumor localization could not be visualized or remained unclear, an 18F-FDG-PET scan was performed (Fig. 1). Anatomical imaging was repeated two or three times per year during the first two years and once or twice per year thereafter. Depending on the outcomes of imaging and Tg slope, the frequency of cross-sectional imaging was tapered slowly.
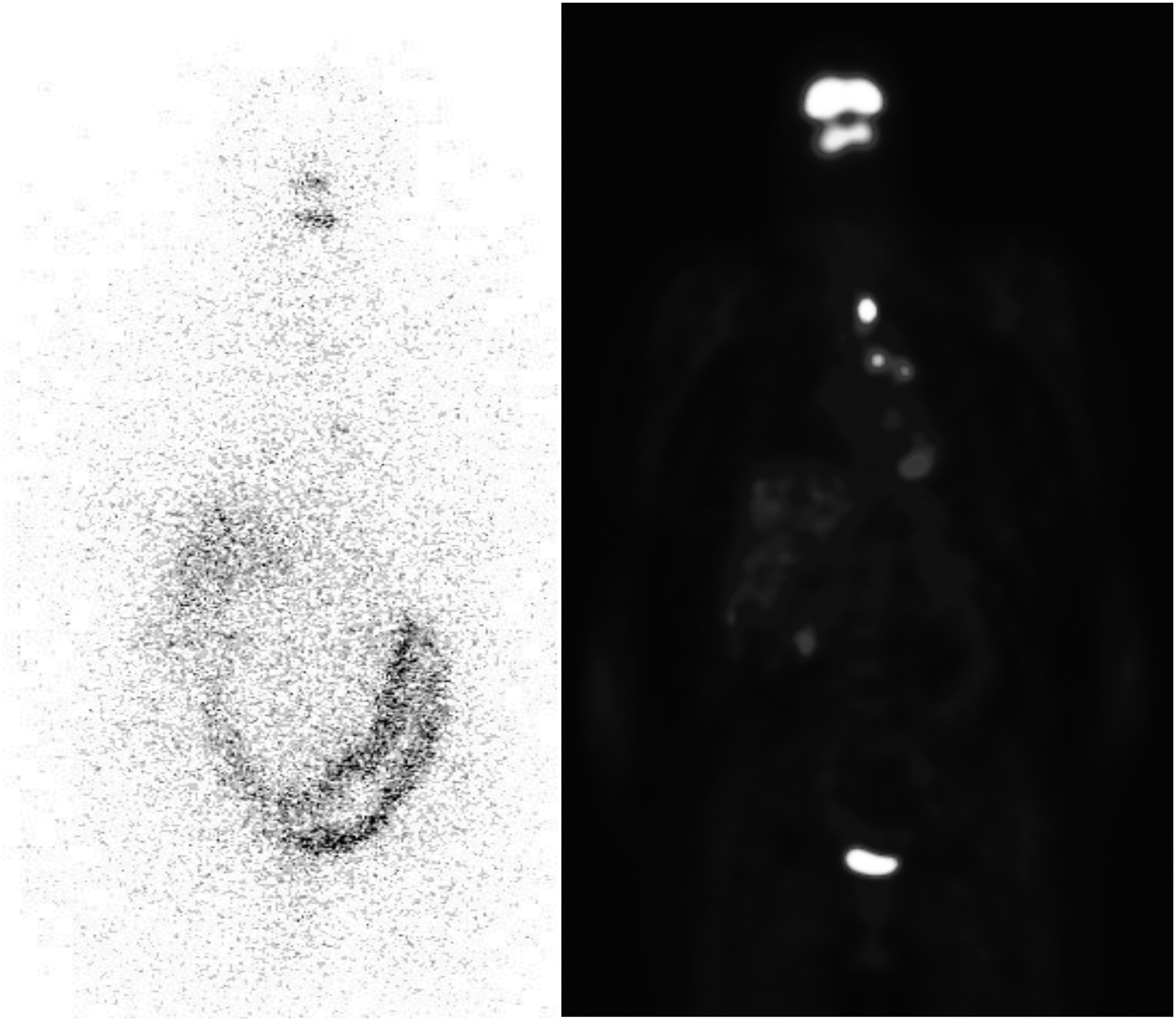
A 75-year-old woman diagnosed with T3N1M0 papillary thyroid carcinoma. Left: A post-therapeutic 131I whole body scan shows physiological uptake in the nasal and oral pharynx, liver, and bowel; otherwise negative scan. Right: A 18F-FDG-PET scan 1 month later shows physiological uptake in the brain, heart, liver, and bladder and multiple suspicious lesions in the mediastinum; positive scan. Despite palliative radiotherapy, the patient developed progressive disease. 131I, radioactive iodine; 18F-FDG-PET, 18-fluorodeoxyglucose positron emission tomography.
Curation was defined as undetectable Tg-on (i.e., Tg during substitution therapy) and no visible tumor either on diagnostic imaging or on physical examination for at least one year. Recurrence was defined as detectable Tg-on, visible tumor on either diagnostic imaging or physical examination, or histologically confirmed tumor after initial curation.
Persistent disease was defined as continuous microscopically (Tg, histopathological) or macroscopically (physical examination, imaging) detectable disease.
18F-FDG-PET protocol
Of the 52 18F-FDG-PET scans, 35 were performed after initial treatment and 17 scans were performed after 131I therapy for recurrent disease. Of the 35 patients with primary disease, 27 patients (77%) were on substitution therapy and 5 patients (14%) were imaged after thyroid hormone withdrawal while undergoing the 18F-FDG-PET scan. The remaining three patients (9%) were rhTSH-stimulated. Of the 17 patients with a PET scan performed after treatment for recurrent disease, 12 patients (71%) underwent endogenous TSH stimulation and 5 patients (29%) were on substitution therapy (Fig. 2). All the patients were asked to fast with free water intake for 6 hours before injection of 18F-FDG. Blood glucose was measured at the beginning of the procedure. If the blood glucose level exceeded 180 mg/dL (10 mmol/L), the 18F-FDG-PET scan was canceled. Patients who were rhTSH-stimulated received an injection with 0.9 mg rhTSH 48 and 24 hours before the PET scan. Until 2007, 18F-FDG-PET scans were carried out 90 minutes after the intravenous administration of 5 MBq of 18F-FDG/kg body weight. From 2008, this was done after 60 minutes. Most patients (n=43) were scanned on an Ecat Exact HR+PET camera (Siemens, Hoffman Estates, IL). Since November 2009, seven patients were scanned on a Biograph mCT (PET/64-slice CT) camera (Siemens). Before August 2004, two patients were scanned on an ECAT 951/31 PET camera (Siemens).
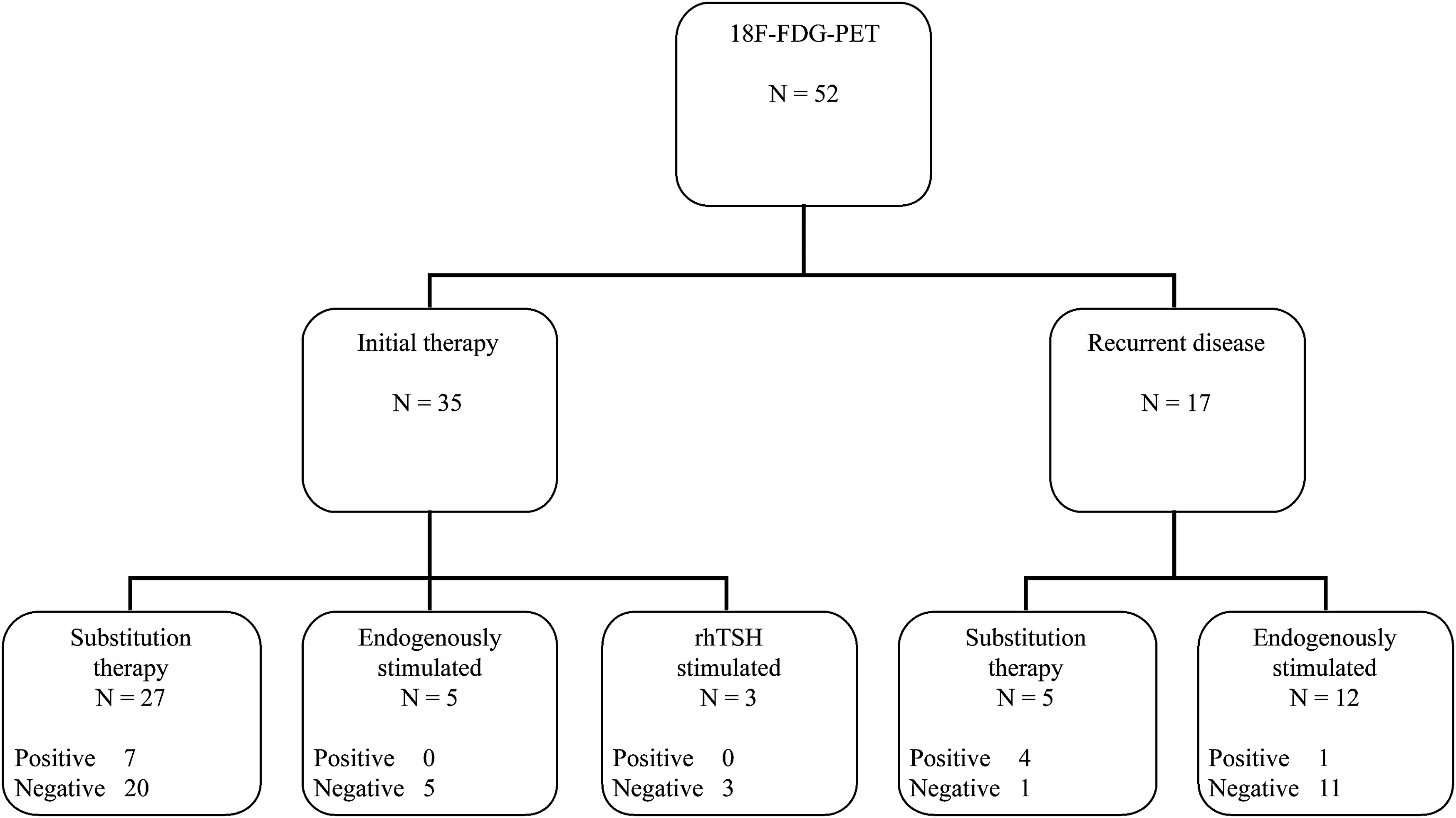
Proportion and outcome of 18F-FDG-PET scans after stimulation of endogenous TSH, with rhTSH, or on substitution therapy. TSH, thyrotropin; rhTSH, recombinant human TSH.
For this study, all scans were blindly re-evaluated after randomization by one of two experienced nuclear medicine physicians (A.H.B. and H.T.T.P.). In case of discrepancy between the original report and the re-evaluation, the scan was again blindly evaluated by the other nuclear medicine physician to reach agreement. In cases of remaining incongruity, A.H.B. re-evaluated the scans taking into consideration the clinical and imaging information that was available until the scan date, and a definitive decision was made.
Scoring of 18F-FDG-PET
The 18F-FDG-PET was considered true positive if lesions were histologically confirmed, or when conventional imaging (CT, MRI, US) showed an anatomical substrate, or if the subsequent 131I WBS during follow-up showed corresponding uptake (12). When the 18F-FDG-PET was positive, but other imaging modalities showed no tumor activity, and/or Tg-on remained undetectable and no histological confirmation was obtained for at least one year, it was considered false positive. It was considered true negative if conventional imaging showed no tumor localization and Tg-on remained undetectable for at least one year. If the 18F-FDG-PET scan was negative, but other imaging modalities did show tumor activity and/or histological confirmation was obtained, it was considered false negative.
Laboratory methods
Routinely, the presence of Tg and TgAb was evaluated. During the inclusion of this study, from 2002 to 2011, different Tg and TgAb immunoassays were used in our hospital, as has been described previously (7). All assays were calibrated against the International Standard CRM-457.
Statistical methods
Data are expressed as mean±standard deviation (SD) for values with normal distribution, and median with range for values with non-normal distribution. Differences in parameters were tested using the Mann–Whitney U-test. A receiver operating characteristic (ROC) curve was used to determine an optimal Tg cutoff point for a positive outcome of the 18F-FDG-PET. Differences were accepted to be statistically significant at a two-sided p<0.05. All statistical tests were carried out using PASW Statistics 18.
Results
Patients
Fifty-two patients were included. In 35 patients, 18F-FDG-PET scans were performed after initial treatment and 17 scans were performed after 131I therapy for recurrent disease. Of the 35 patients with primary disease, 27 patients (77%) were on substitution therapy and 5 patients (14%) underwent thyroid hormone withdrawal while undergoing the 18F-FDG-PET scan. The remaining three patients (9%) were rhTSH-stimulated. Of the 17 patients with a PET scan performed after treatment for recurrent disease, 12 patients (71%) underwent endogenous stimulation and 5 patients (29%) were on substitution therapy (Fig. 2). The median TSH value of the 28 substituted patients was 0.036 mU/L (0.04–4.68), that of the 16 patients undergoing thyroid hormone withdrawal was 33.5 mU/L (4.10–240.00), and that of the 1 rhTSH-stimulated patient was 140.00 mU/L. In seven patients, TSH measurements were not available.
18F-FDG-PET
Of the 52 18F-FDG-PET scans, 9 (17%) were true positive, 3 (6%) were false positive, 36 (69%) were true negative, and 4 (8%) were false negative, leading to a sensitivity of 69% and specificity of 94%, and a positive and negative predictive value of 75% and 90%, respectively (Figs. 2 and 3; Table 2). Of the nine patients with a true-positive scan, five underwent additional surgery and two patients received additional radiotherapy. Two patients were treated based on their symptoms in a palliative setting. One patient was known to have concurrent metastatic breast cancer; the other patient had an irresectable recurrence after 27 years, for which radiotherapy was already given eight months before the 18F-FDG-PET scan.
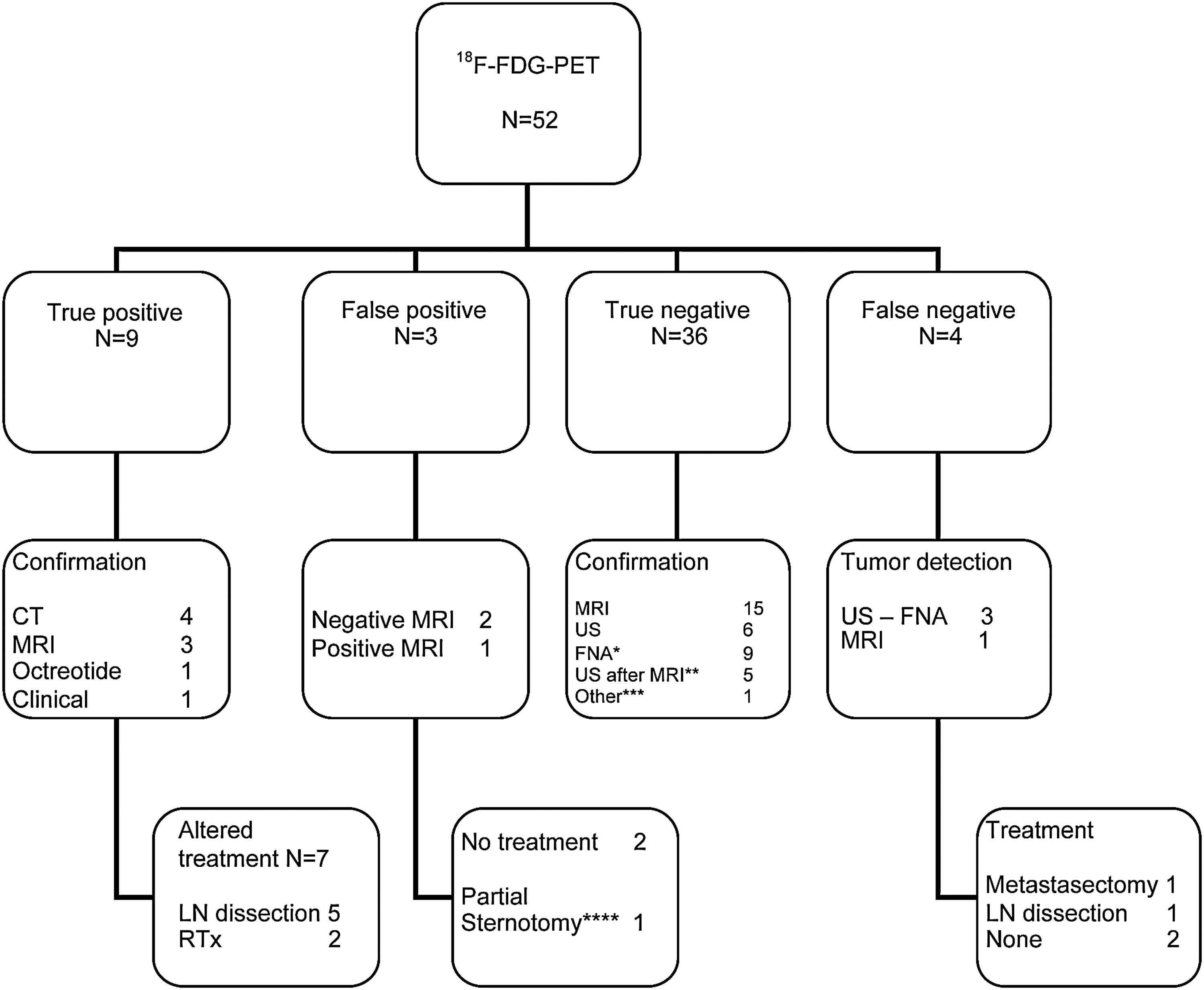
Flowchart clinical outcome 18F-FDG-PET. *FNA was performed after positive MRI, US, or both and was negative in all cases. **US performed after false-positive MRI, all negative. ***In one patient, US was omitted because of logistical reasons. ****Histological confirmation of tumor was not obtained. CT, computed tomography; FNA, fine needle aspiration; LN, lymph node; MRI, magnetic resonance imaging; RTx, radiotherapy; US, ultrasound.
18F-FDG-PET, 18-fluorodeoxyglucose positron emission tomography; Init, patients after initial therapy; Rec, patients after recurrent disease; Tg-off, thyroglobulin during thyroxine withdrawal.
Two patients with a false-positive scan did not receive additional therapy because repeated US and MRI did not show any anatomical substrate that could be confirmed by fine needle aspiration. Both patients did not show recurrent disease during more than eight years of follow-up. One patient with a false-positive scan had a sternotomy with resection of retrosternal tissue based on abnormal uptake on the PET scan, but showed normal thymus and lymph nodes without malignancy on histological examination. None of the patients with a true-negative scan received additional treatment, and these patients have not been diagnosed with a recurrence after a median follow-up of 7.1 years (1.3–11.1).
Of the four patients with a false-negative scan, one underwent additional lymph node dissection and one had a metastasectomy (both with histological confirmation of cancer), whereas two did not undergo additional therapy because there was no metastasis growth as was shown by CT and chest radiography.
Contingent uptake
In eight patients, non–thyroid-cancer-related focal uptake was seen on the 18F-FDG-PET scan. In one patient, FDG-avid lesions were seen in the axilla. Subsequent CT and MRI showed normal lymph nodes. In another patient, a suspicious FDG-avid lesion was seen in the dorsal neck, but based on its extreme dorsal location, it was considered as non–thyroid cancer related. One scan showed suspicious focal uptake in the adrenal gland region, and on five other scans, focal bowel uptake suggestive for intestinal polyps was seen. Because of the locations, possible metastases of thyroid cancer seemed unlikely and these incidental lesions were therefore considered negative for thyroid-related cancer. All these patients were monitored for more than five years and received additional imaging, which did not show malignant characteristics.
Tg levels
Five patients with positive TgAb were excluded from all calculations with Tg levels. Analyses were performed on the remaining 47 patients.
The median Tg-off value during 131I therapy was 8.40 ng/mL (0.18–1870.00), and the median TSH-off value during 131I therapy was 65.00 mU/L (14.00–224.00). The optimal Tg-off cutoff value to predict a positive scan was determined by an ROC curve analysis. The area under the ROC curve is 0.82 [CI 0.64–0.99], p<0.01. The optimal cutoff value with a Tg-off of 38.00 ng/mL resulted in a sensitivity of 67% and a specificity of 95%. Ninety percent of patients with a positive 18F-FDG-PET have a Tg-off >2.00 ng/mL. Ninety percent of patients with a negative 18F-FDG-PET have a Tg-off <22.00 ng/mL (Fig. 4).
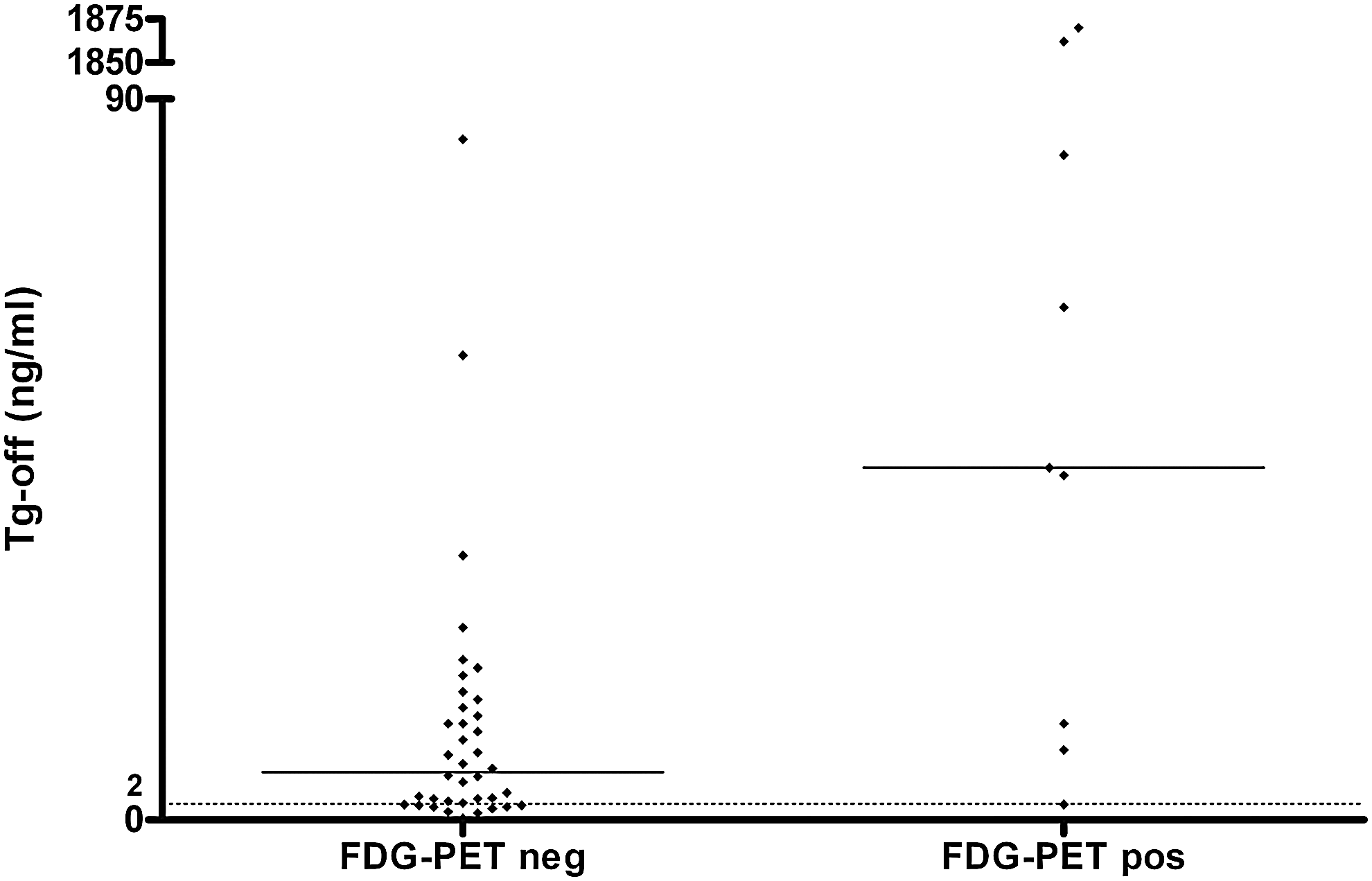
Tg-off values per patient during 131I therapy. The dotted line represents a Tg level of 2.00 ng/mL. Black lines represent median Tg values of groups (5.95 and 44.00 ng/mL, respectively). Tg, thyroglobulin; Tg-off, Tg during thyroxine withdrawal.
Discussion
This study evaluated the yield of 18FDG-PET imaging in the early follow-up of patients with a negative post-therapeutic WBS and detectable Tg-off. We have shown that 18F-FDG-PET imaging performed within three months was true positive in 17% (9 out of 52) of patients with a negative WBS with concurrent detectable Tg, leading to a change in clinical management in the majority (7 out of 9 patients). We did not find a clinically useful Tg cutoff point that could serve as a suitable predictor for a positive 18F-FDG-PET scan, but 90% of the patients with a positive 18F-FDG-PET scan have a Tg-off>2.00 ng/mL. This underscores that in patients with a Tg-off >2.00 ng/mL, 18F-FDG-PET scanning could be a suitable diagnostic tool in the early workup.
Many studies have been published about the value of 18F-FDG-PET scanning in WBS-negative, Tg-positive patients (8 –10,13 –16,18,24) with a wide time range between WBS and 18F-FDG-PET scanning, varying from a few days before WBS, up until 23 years after. Some studies do not describe a time interval (8,9,15). Other studies also included WBS-positive and/or Tg-negative patients together with WBS-negative, Tg-positive patients without differentiating between stimulated or unstimulated Tg (8,18,24). To our knowledge, this is the first study with a strict selection of WBS-negative, Tg-positive patients and an early performed 18F-FDG-PET scan.
In the current American Thyroid Association guidelines, the role of 18F-FDG-PET scans in the early diagnostic follow-up is marginally described (25). This study supports arguments for the application of 18F-FDG-PET imaging in a selected group of patients during the early workup after a negative 131I WBS. However, further research with regard to costs and benefits of early 18F-FDG-PET scanning for survival and early treatment of a small patient group is necessary.
Our results show a change of clinical management in seven out of nine patients with a Tg-off value >2.00 ng/mL. This Tg level is much lower than that of earlier studies, which suggest a cutoff value of 10.00 ng/mL (17 –19). However, since different Tg assays were used over the years, this Tg cutoff value must be considered as an approximate value (26). If imaging remains negative but Tg remains detectable, the Tg slope or doubling time is important for monitoring disease (27). However, when Tg levels reflect active disease, adequate treatment should be initiated.
Some limitations are encountered in this study. Because of the retrospective design of this study, stimulated and unstimulated 18F-FDG-PET scans were included. The role of stimulation (either endogenous or rhTSH) before the 18F-FDG-PET is still unclear. Some studies show a higher uptake on the 18F-FDG-PET scan in patients undergoing stimulation with endogenous TSH or after rhTSH stimulation (10,12,14,28), while others found opposite results (24,29). Remarkably, our data do not suggest a lower yield of unstimulated 18F-FDG-PET scans; however, this may be due to chance because of the limited number of patients in our subgroups. Moreover, availability and high costs play a role in the consideration and the desirability of using rhTSH stimulation. Over time, we used three different PET scanners. The vast majority of our patients (n=45) were scanned on a PET stand-alone camera. Eight patients were scanned on a PET/CT camera. Sensitivity and specificity seem to improve going from a PET to PET/CT camera, which is in line with previous studies (30,31). However, the size of this group is too small to draw definite conclusions.
Conclusions
Our study shows that 18F-FDG-PET scanning in the early workup after a negative WBS with concurrent detectable Tg-off shows additional tumor localization in 17% (9 out of 52) of the patients and led to a change in clinical management in 7 of these 9 patients. Ninety percent of positive 18F-FDG-PET scans occurred in patients with a Tg-off>2.00 ng/mL; however, a clinically useful Tg-off cutoff value could not be determined.
Footnotes
Author Disclosure Statement
No competing financial interests exist.