
Abstract
Background:
Hyperthyroidism has been associated with increased all-cause mortality. Whether the underlying cause of hyperthyroidism influences this association is unclear. Our objectives were to explore whether mortality risk and cause of death differ between Graves' disease (GD) and toxic nodular goiter (TNG).
Methods:
This is an observational cohort study, using record-linkage data from nationwide Danish health registers. A total of 1291 subjects with GD and 861 with TNG, treated in a hospital setting, were identified and followed for a mean period of 11 years. Cases were matched 1:4 with nonhyperthyroid controls with respect to age and sex. The hazard ratio (HR) for mortality was calculated using Cox regression analyses. All analyses were adjusted for comorbidity using the Charlson score.
Results:
Both GD (HR=1.42 [95% confidence interval (CI) 1.25–1.60]) and TNG (HR=1.22 [CI 1.07–1.40]) were associated with increased all-cause mortality. After stratification for the cause of death, GD was associated with increased mortality due to cardiovascular diseases (HR=1.49 [CI 1.25–1.77]) and lung diseases (HR=1.91 [CI 1.37–2.65]), whereas TNG was associated with increased cancer mortality (HR=1.36 [CI 1.06–1.75]). When analyzing mortality in GD using TNG individuals as controls, there was no significant difference in all-cause mortality between GD and TNG. However, GD was clearly associated with a higher cardiovascular mortality (HR=1.39 [CI 1.10–1.76]) compared to TNG.
Conclusion:
Both GD and TNG, treated in a hospital setting, are associated with increased all-cause mortality. The causes of death differ between the two phenotypes, with cardiovascular mortality being significantly higher in GD.
Introduction
The most frequent causes of hyperthyroidism are Graves' disease (GD) and toxic nodular goiter (TNG) (15). Clearly, there are major differences in the epidemiology and clinical features of these two phenotypes (16). GD is the most prevalent cause of hyperthyroidism in iodine-sufficient areas, whereas TNG is more frequent in iodine-deficient areas (17). Although GD and TNG are seen in all ages, GD more often than TNG affects younger individuals (16). Thus, it is likely that the consequences with respect to mortality differ between GD and TNG (13). Evaluation of a possible difference between GD and TNG with respect to mortality has only been carried out in two studies (6,9). The findings are conflicting, as Nyirenda et al. (6) failed to show an increased mortality in any of the two phenotypes, while Metso et al. (9) demonstrated that TNG but not GD was associated with increased mortality.
Based on the nationwide Danish health registers, we aimed to investigate whether mortality risk and cause of death differ between incident cases of GD and TNG.
Materials and Methods
Data sources
The Danish Civil Registration System (DCRS) covers information on demographics, vital status, and date of death of all persons in Denmark (18). DCRS is based on a unique 10-digit personal identification number (CPR number) assigned to all persons. The CPR number allows record linkage between a large number of administrative databases on an individual level. From the DCRS, we identified a random 5% sample of the Danish population alive on April 2, 1968 (start of DCRS), from the birth cohorts 1870–2001 (n=339, 481).
The Danish National Patient Registry (DNPR) includes registrations of admissions to hospitals since January 1, 1977. In addition to inpatient treatments, outpatient admissions have been registered separately since January 1, 1995 (18). As thyroid patients in Denmark are most often treated as outpatients in a hospital setting, we have included the vast majority of thyroid patients in the observation period who are registered in the DNPR. In line with this, the finding that misclassification of hyperthyroidism occurs in <2% of cases makes the register very valid for our purpose (19). All registrations are according to the International Classification of Diseases (ICD).
The Danish National Prescription Registry (DNPrR) provides information on all prescriptions of drugs dispensed from Danish pharmacies since 1995 (18). Coding for medical products is according to the Anatomical Therapeutic Chemical (ATC) classification system.
Definition of hyperthyroidism
Individuals were identified as hyperthyroid if they were registered with GD or TNG in the DNPR. GD was defined by the ICD-10 codes E05.0, H05.2, or H06.2, as well as with the ICD-8 codes 242.08, 242.09, 242.00, or 242.01. TNG was defined by the ICD-10 codes E05.1 or E05.2 and the ICD-8 code 242.19. The first date registered in the DNPR was chosen as the date of diagnosis.
Mortality
Data on mortality were obtained from the DCRS (18). In addition to all-cause mortality, we analyzed for death due to cardiovascular diseases (ICD-8 codes 390–458 and ICD-10 codes I00–I99), cancer diseases (ICD-8 codes 140–207 and ICD-10 codes C00–C97), lung diseases (ICD-8 codes 464–493 and 508–519 and ICD-10 codes J00–J99), and diabetes mellitus (ICD-8 codes 249–250 as well as the ICD-10 codes E10–E14).
Study population
From the random 5% sample of the Danish population, individuals diagnosed with GD or TNG were identified. In order to include incident adult cases only, all cases diagnosed in 1977 and 1995 (the start of DNPR and the beginning of registering outpatient admissions respectively) and all individuals younger than 18 years of age were excluded. A total of 1291 individuals with GD and 861 individuals with TNG were identified. Using the 5% random sample, cases were matched with four controls with respect to age and sex, based on the principles of density sampling (20). All participants were followed until death or December 31, 2008.
Comorbidity
The Charlson score (CS) accounts for 19 disease groups by creating a weighted score on an individual level to optimize the prediction of the one-year mortality risk within each disease category (21). Although the CS was designed to estimate the one-year mortality in breast cancer patients, it has been validated in non-malignant phenotypes as well (22). In both cases and controls, the CS was calculated from individual records in the DNPR using relevant ICD codes. As many patients in Denmark with diabetes, cardiovascular disease (e.g., hypertension), and lung diseases (e.g., chronic obstructive lung diseases) are diagnosed and treated solely in primary care, we classified all users of anti-diabetics (ATC code A10), cardiovascular-related drugs (ATC codes B01, C01, C03, C07, C08, C09, or N02), and users of drugs for obstructive airway disease (ATC codes R03) registered in the DNPrR as having diabetes, cardiovascular disease, or lung disease respectively. For subjects with hyperthyroidism, the CS consequently reflects the time period from January 1, 1977 (start of DNPR) until the index date. In controls, the CS covers the time period from the start of the DNPR until the index date of the corresponding case.
Data analysis
The relationship between GD or TNG and all-cause mortality was evaluated using the Cox proportional hazards model. Because of potential competing risk, cause-specific mortality was evaluated using the method of Fine and Gray (23). Age was chosen as the underlying time variable, while time at risk was accumulated from the date of the diagnosis of GD or TNG (index date). Person years of follow-up were terminated at the date of death or end of follow-up (December 31, 2008), whichever came first. In all Cox analyses, the variable “pair” was used as a stratum variable, fixing the baseline hazard within each pair (cases and controls), while at the same time allowing this baseline hazard to vary freely between pairs (pair=1 case+4 controls). All other analyses were adjusted for age and sex.
To compare the prognosis of GD and TNG, we re-evaluated the risk of mortality in GD individuals, with TNG individuals as controls. These analyses were adjusted for age and sex.
Significance was defined as p<0.05 using two-tailed tests. All analyses were conducted using STATA version 11.0 (Stata Corp., College Station, TX).
Results
Baseline characteristics of the study population
The baseline characteristics of the individuals diagnosed with GD or TNG and followed for a mean period of 11 years are shown in Table 1. In general, individuals diagnosed with GD were younger and diagnosed at a younger age than the TNG cases. The mean age at the diagnosis of GD is higher than generally found, probably because individuals younger than 18 years of age were excluded. Neither follow-up time nor comorbidity, as measured by the CS, differed between the GD and TNG population.
All-cause mortality
All results from the mortality analyses are shown in Figure 1. Based on 1844 and 1624 diseased individuals from the GD and TNG study populations respectively, both GD and TNG were associated with increased all-cause mortality. Adjustment for the history of comorbidity did not significantly change this finding in either individuals with GD, as reflected by a hazard ratio (HR) of 1.42 [95% confidence interval (CI) 1.25–1.60] or TNG (HR=1.22 [CI 1.07–1.40]). Stratification for the mean age of diagnosis (GD, 55 years; TNG, 62 years) yield different results in GD and TNG. In GD, both the younger (HR=2.82 [CI 1.29–6.12]) and the older (HR=1.44 [CI 1.27–1.63]) age groups had a higher mortality. In TNG, this was only true for older individuals (HR=1.25 [CI 1.09–1.43]) and not for the younger ones (HR=0.47 [CI 0.17–1.35]).
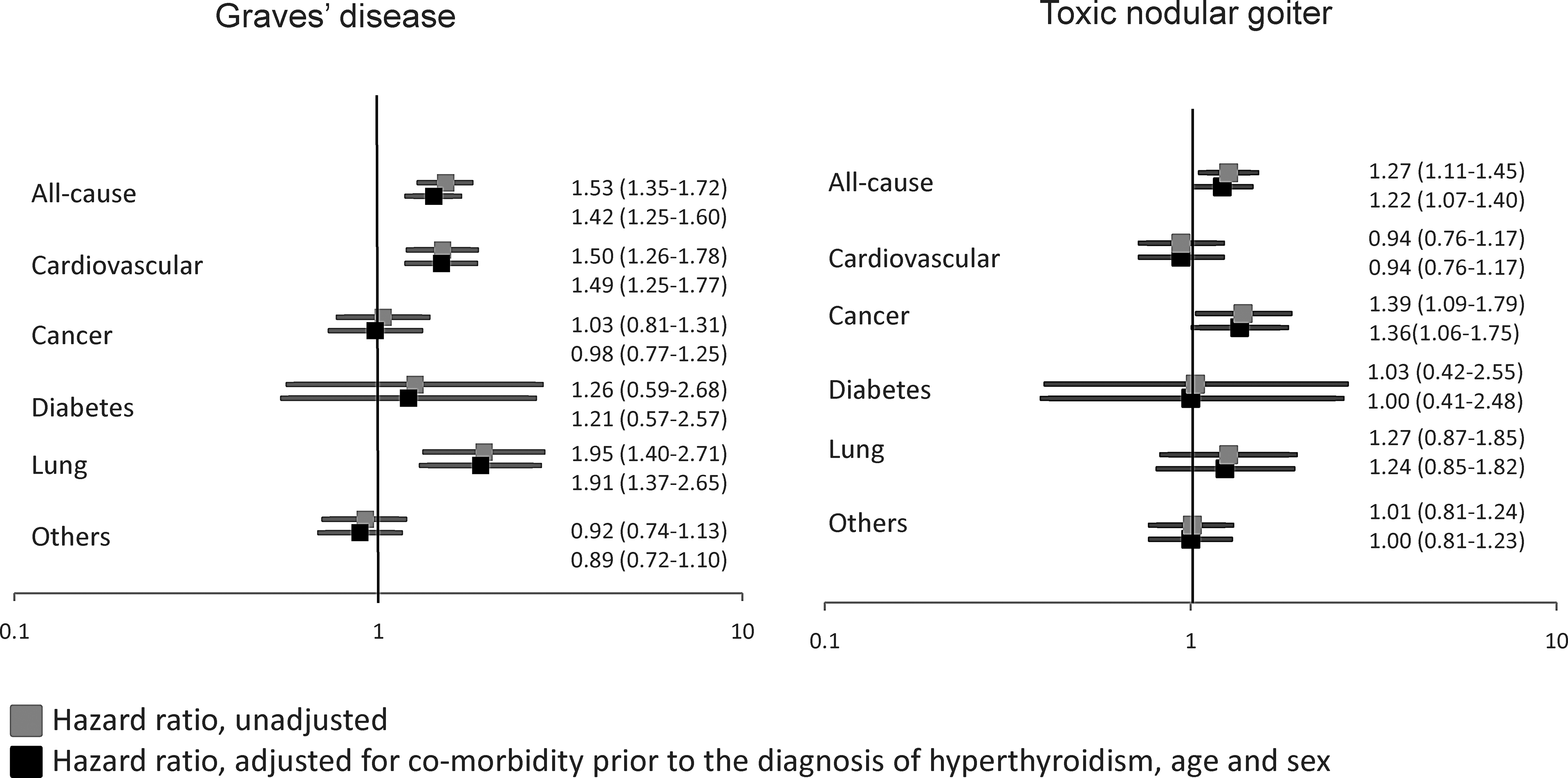
Hazard ratio of mortality with 95% confidence intervals in individuals diagnosed with hyperthyroidism according to the cause of hyperthyroidism.
Disease-specific mortality
The disease-specific mortality of individuals identified with GD and TNG is shown in Figure 1. After adjustment for the history of comorbidity, GD was associated with increased cardiovascular mortality (HR=1.49 [CI 1.25–1.77]) and increased mortality from lung disease (HR=1.91 [CI 1.37–2.65]; Fig. 1A).
In contrast to GD, TNG was associated with an increased mortality from cancer, even after adjustment for the history of comorbidity (HR=1.36 [CI 1.06–1.75]; Fig. 1B).
Graves' disease versus toxic nodular goiter
Overall, there was no significant difference in all-cause mortality between GD and TNG (Table 2). However, when compared with TNG, GD was associated with a significantly higher cardiovascular mortality (HR=1.39 [CI 1.10–1.76]).
GD, Graves' disease; TNG, toxic nodular goiter; HR, hazard ratio; CI, 95% confidence interval.
Discussion
As previously demonstrated for hyperthyroidism, irrespective of its cause (12), both GD and TNG, treated in a hospital setting, were associated with increased all-cause mortality. In addition, after stratification for the cause of death, GD was associated with significantly higher mortality from cardiovascular diseases compared to TNG.
Although the literature favors hyperthyroidism being associated with increased mortality (13), our findings, after stratification for the cause of hyperthyroidism, differ from previous studies. Thus, Metso et al. found that only TNG was associated with increased mortality (9), while Nyirenda et al. did not report increased mortality in either GD or TNG (6). Importantly, both of these studies included only radioiodine-treated patients (6,9), and the control for comorbidity was inconsistent. In contrast, we used a more robust method in the present study by obtaining complete coverage of GD and TNG from discharge diagnosis of both inpatients and outpatients, independent of the treatment modality. Additionally, we introduced a standardized and validated scale based on extensive coverage of comorbidity from both discharge diagnoses and prescriptions. The fact that comorbidity had no impact on the associations between either of the two phenotypes and mortality may indicate a direct relation between both GD and TNG on the one hand and mortality on the other hand.
Only a few studies have analyzed the association between hyperthyroidism and disease-specific mortality (5,7 –11). The majority of these studies link hyperthyroidism to increased cardiovascular mortality (7,9 –11). Even subclinical hyperthyroidism seems to be associated with increased cardiovascular mortality (24,25). However, none of these studies stratified for the cause of hyperthyroidism. In the present study, only GD was associated with increased cardiovascular mortality. In line with this, cardiac valve degeneration, as an example, mostly occurs in GD and other autoimmune thyroid disorders (26,27). In contrast, TNG, more frequently than GD, has been found to be associated with cardiac arrhythmia (28) and heart failure (29). However, this could obviously pertain to the higher age and consequently higher comorbidity in TNG individuals (16). Still, the exact pathophysiological mechanisms related to the different cardiovascular prognosis in GD and TNG require further investigations.
To our knowledge, no previous study has evaluated the risk of mortality from lung disease stratified for the cause of hyperthyroidism. In the present study, only GD was associated with increased lung disease mortality. The attributable risk of smoking in GD has been reported to be nearly twice as high as in TNG (45% vs. 28% respectively) (30). Therefore, the higher risk of lung-disease mortality might be related to a greater proportion of smokers in the GD group. Unfortunately, we have no information about smoking to allow us to draw any further conclusion.
The literature is ambiguous with respect to cancer mortality. At variance with the findings of Flynn et al. (5), three studies have reported increased cancer mortality in individuals diagnosed with hyperthyroidism (9,10,31). Two of these studies only included radioiodine-treated individuals (9,31). Since patients were not randomized to radioiodine therapy but probably were assigned to this form of therapy based upon other factors such as severity of disease and patient/physician preference, it follows that selection bias but also the unknown effect of the treatment modality could hamper the interpretation of mortality data. Unfortunately, the register-based design of the present study does not allow us to speculate on treatment modality and its possible influence on mortality. However, a meta-analysis has not shown an increase in cancer risk related to radioiodine treatment (32).
The strengths of our study include a large sample size, ascertainment of participants from nationwide population-based registers, use of standardized and validated procedures for evaluating the degree of comorbidity, and a mean follow-up period of 11 years. The long-standing tradition of treating thyroid patients in a hospital setting in Denmark minimizes the risk of selection bias. On the other hand, the smaller power in the comparative analyses (GD vs. TNG), the lack of information regarding the type of therapy, effect of treatment for benign thyroid disease, and lack of biochemical data are weaknesses in the present study. However, as patients would not have been randomized to divergent therapy options, differences in mortality would not necessarily pertain to differences in type of therapy but to a multitude of known and unknown parameters. Importantly, it seems counterintuitive that patients would be left untreated, and we therefore assume that all individuals were treated for hyperthyroidism. The fact that other investigators have compared different treatment modalities like radioiodine and surgery (33) and found no difference in mortality in relation to mode of therapy suggests that lacking such information is not crucial for our overall conclusions. Hyperthyroidism (34,35), cardiovascular disease (36), stroke, as well as life-span, demonstrate familial and to some degree individual clustering (37 –39). In line with this, having access to twins, we have previously shown that the association between hyperthyroidism and mortality might be explained by genetic confounding (12). Unfortunately, access to too few disease-discordant Danish twin pairs, after stratification for the cause of hyperthyroidism, did not allow us to include this aspect in the present study.
In conclusion, both GD and TNG, treated in a hospital setting, are associated with increased all-cause mortality. The causes of death differ between the two phenotypes, with cardiovascular mortality being significantly higher in GD. Whether this difference is related to the autoimmune component in GD, as recently suggested for the effect of autoimmune hypothyroidism on quality of life (40), needs further study.
Footnotes
Author Disclosure Statement
D.A., K.C., A.G., and T.H.B. have nothing to declare. F.B. and M.T. are enrolled as PhD students financed by the School of Endocrinology, University of Southern Denmark, Odense. F.B. has also received funding from the Danish Thyroid Patient Organization. L.H. is the recipient of an unrestricted research grant from the Novo Nordisk Foundation.