
Abstract
Background:
Fine-needle biopsy of the thyroid gland is the most common interventional procedure used to diagnose thyroid diseases. Serious complications are rare in this procedure. They comprise an infection with abscess formation and hemorrhage. To date, only a few case reports have described an ultrasound diagnosis of active bleeding into the thyroid gland. We established such a diagnosis using computed tomography (CT).
Patient Findings:
A 74-year-old woman presented to the emergency department of our hospital with complications after fine-needle biopsy of the thyroid gland. Ultrasound revealed a large hematoma surrounding the gland. A subsequent CT scan confirmed the presence of hematoma and, moreover, showed active bleeding. This finding prompted rapid surgical intervention.
Conclusion:
CT has the capability to show active bleeding into the thyroid gland.
Introduction
Modern imaging techniques have the capability to diagnose not only the exact extent and composition of hematoma, but also active bleeding. We found three case reports describing an ultrasound diagnosis of active bleeding into the thyroid gland (3 –5) in the literature. However, to our knowledge, a computed tomography (CT) diagnosis of such a condition has not yet been reported.
We describe a case report of a CT diagnosis of active bleeding into the thyroid gland, which occurred after FNB.
Patient Report
A 74-year-old woman was treated for cardiac problems, hypertension, dizziness, and nausea in an outpatient internist practice. Her physical examination also revealed enlargement of the thyroid gland, and a subsequent ultrasound confirmed a nodular goiter with a larger nodule in the right lobe of the thyroid gland. FNB was indicated to determine the etiology of this nodule. To prepare the patient for biopsy, warfarinum natricum (warfarin; Orion, Espoo, Finland) medicated for paroxysmal atrial fibrillation was replaced by nadroparinum calcium (fraxiparine, Glaxo, Brentford, England) a week before the biopsy. The last dose of nadroparinum calcium was given 24 hours before biopsy. Ultrasound-guided FNB from the nodule in the right lobe of the thyroid gland was performed in the outpatient internist practice in the morning. Three samples were obtained using a 21G needle. The biopsy was without apparent complications, and the patient was clinically and subjectively in good condition immediately after the procedure.
In the evening of the same day, the patient was brought to the emergency department of our hospital with neck swelling, which was more pronounced on the right side. Subjectively, the patient felt pain on the right side of her neck, pain during swallowing, increasing pressure on the neck, and difficulties breathing. Objectively, there was noticeable swelling and stiff resistance on the neck, being more prominent on the right side. An ultrasound examination was performed. An anechoic mass without evident vascularization was found anteriorly from the heterogeneous right thyroid lobe corresponding to hematoma (Fig. 1). The patient was hospitalized.
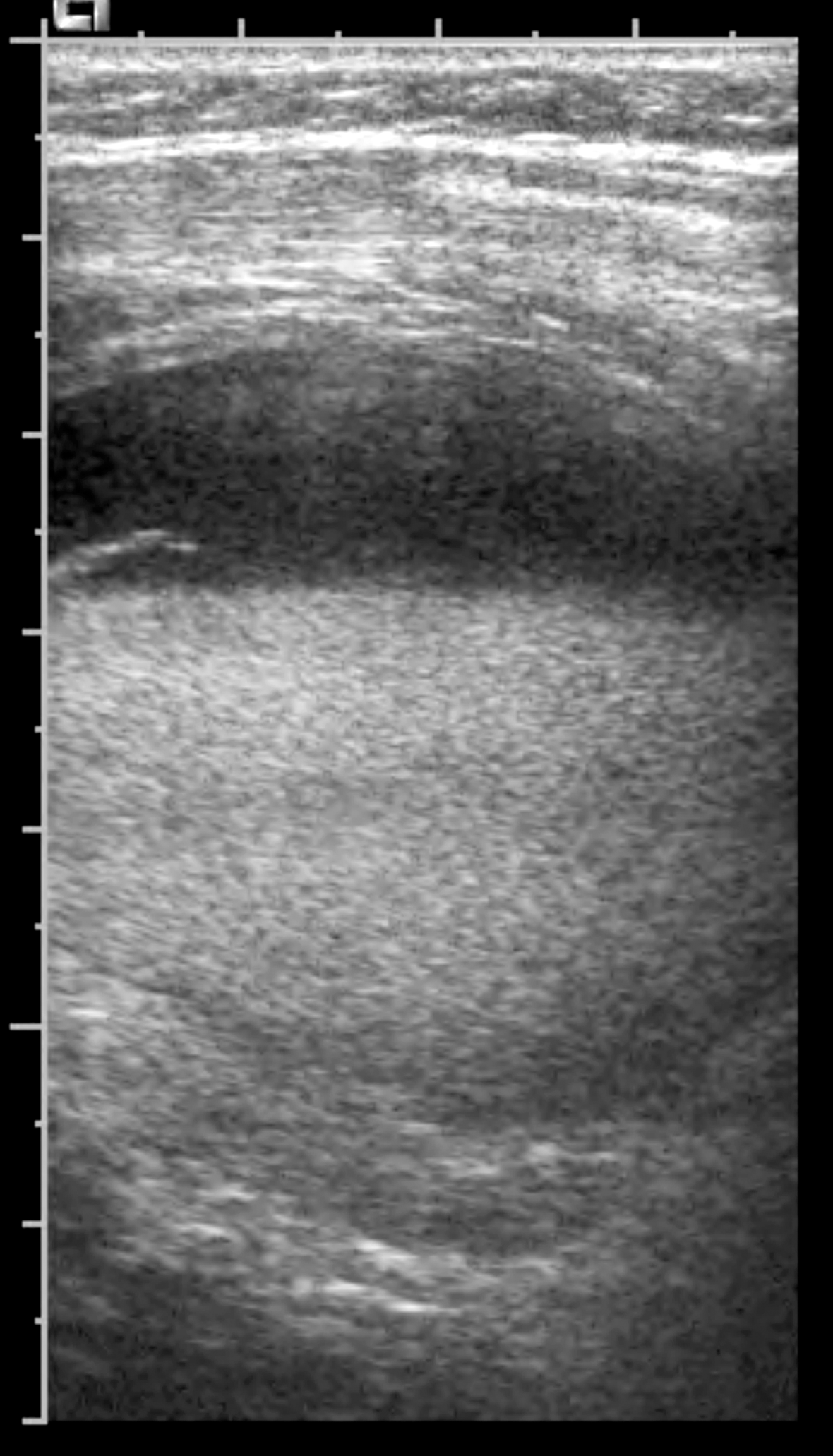
An ultrasound image in the transversal plane obtained over the right lobe of the thyroid gland shows a heterogeneous mass with fluid suggesting the presence of a hematoma. This lesion was found bilaterally, but was more prominent on the right side. Doppler mode did not reveal any active bleeding.
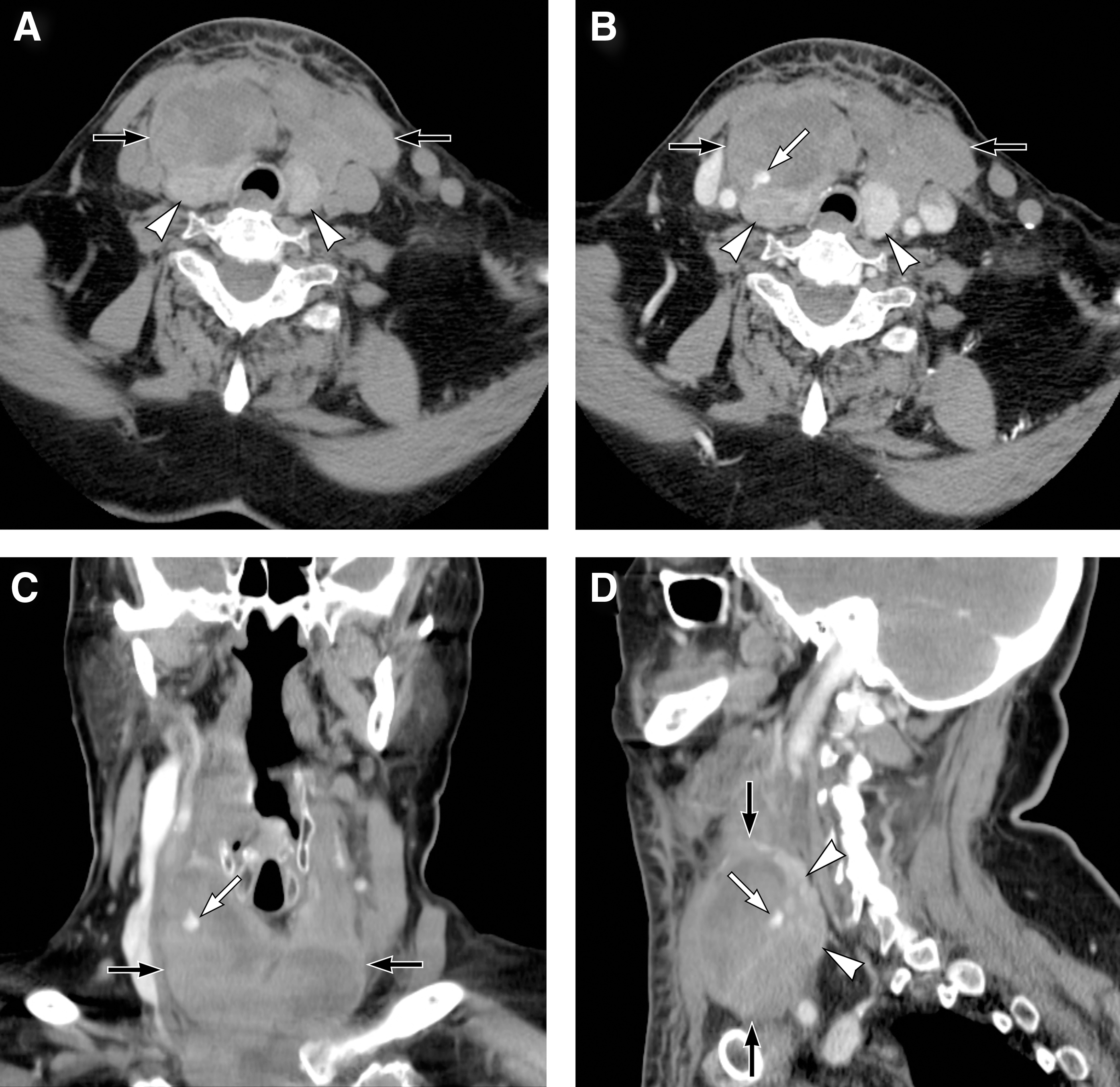
The next morning, the patient's condition deteriorated, with her neck being red and her skin warm. Due to the clinical symptoms, a CT scan of the neck was ordered by an otorhinolaryngologist. A heterogeneous density of both lobes of the thyroid gland was present on unenhanced CT scans, together with a hematoma measuring 83 mm×50 mm×64 mm located anteriorly to the thyroid gland. The hematoma extended from the base of the oral cavity to the level of the sternum. A CT scan performed after intravenous iodine contrast administration showed a dense area within the hematoma, close to the right thyroid lobe, corresponding to active bleeding (Fig. 2).
(
Based on the CT findings, urgent surgical intervention was performed. It revealed numerous clots under the infrahyoid muscles and active bleeding in the anterior part of the right lobe of the thyroid gland. It was acutely managed with a ligature suture of the superior thyroid artery followed by right-side hemithyroidectomy.
Histology of the right thyroid lobe confirmed a nodule 23 mm in diameter, which was in contact with the capsule. Microscopic examination revealed a colloid nodule with focal regressive changes and numerous lymphoid aggregates without oncocytic transformation of the follicular epithelium. The postoperative period was uneventful. The patient was discharged on the second postoperative day without complaints.
Discussion
Complications after FNB of the thyroid gland are relatively frequent, but in the majority of cases, they are of minimal clinical importance. The most common complications include soreness at the injection site, local irritation, or minor hematomas. Only a small percentage of bleeding complications is really serious. In a retrospective study, Khoo et al. reported clinically important bleeding complications in 3 out of 311 patients (6).
Hematomas compressing the airways and causing acute respiratory distress are the most serious complication in association with FNB. Although very uncommon, they frequently require urgent surgical management (1,3,7 –9).
Why can FNB of the thyroid gland cause acute bleeding, and why is early and rapid diagnosis important? Acute bleeding after FNB usually occurs following disruption of the wall of a larger vascular structure. The thyroid gland is located near the great neck vessels, and therefore there is a higher risk of injury if the nodules are located in vicinity of these vessels. A vessel supplying the thyroid gland can also be injured during FNB. The gland itself can be highly vascularized in certain chronic disorders, and some nodules can also be hypervascularized and susceptible to bleeding. An increased risk of bleeding after FNB is also found in patients with coagulation disorders or those treated with antiplatelet or anticoagulant therapy; this was also the case in our patient. Although the patient was appropriately prepared for FNB, anticoagulation was probably a main contributing factor for the bleeding. Last but not least, the risk of bleeding is also dependent on the diameter of the needle used for FNB. To yield sufficient diagnostic information, it is possible to use a 25G needle (1,6). In our case, however, biopsy was performed in a private practice using a 21G needle.
Imaging to assess for complications after FNB typically includes ultrasound examination as first line modality. It can demonstrate hematomas and abscess formation, among others. It has been reported that ultrasound with Doppler technique is capable of diagnosing active bleeding or pseudoaneurysm (3 –5). A CT scan is usually used in these situations in cases with discrepancies between ultrasound and clinical findings, or in those with unclear clinical symptoms. A CT scan can precisely demonstrate hemorrhagic (and other) complications, including active bleeding. To diagnose active bleeding, the use of iodine contrast material is necessary.
With the use of modern multidetector-row CT scanners, active bleeding is found more often, particularly in the abdomen. However, a CT diagnosis of active bleeding into the thyroid gland has not yet been published.
Conclusion
Although clinically important bleeding after FNB of the thyroid gland is rare, it can be a life-threatening condition. In such a situation, an early and accurate diagnosis is essential. Our case, and three other case reports (3 –5) describing the diagnosis of active bleeding into the thyroid gland, show the capability of modern imaging techniques to diagnose active bleeding into the thyroid gland preoperatively.
Footnotes
Author Disclosure Statement
No competing financial interests exist for all authors.