
Abstract

Riedel's thyroiditis (RT) is a rare disease with extensive fibrosis of the thyroid gland outside its capsule and in the surrounding tissues. Usually, medical treatment is effective, with RT having a benign course, and mortality is rare (1). Here we present the case of a patient with RT involving fatal necrotizing cellulitis of the neck.
An 81-year-old man presented a history of 1-year of dysphonia and episodic dyspnea. He had been treated by surgery and external cervical radiotherapy for a thyroid neoplasm 35 years earlier without any further detailed information available about the nature of this disease. The patient had stopped smoking 50 years ago, and he had a 20-year history of arrhythmia controlled by digoxin and anticoagulation therapy. He was afebrile. Physical examination revealed an enlarged, hard, and fixed cervical mass and a subcutaneous tumor nodule in the region of the right thyroidectomy scar and fibroscopy revealed bilateral vocal fold immobility. Laboratory analysis showed raised inflammatory markers (a C-reactive protein of 305 mg/L, reference range: <20 mg/L) and a normal white blood cell count (6880/mm3). Laboratory tests for thyroid function were normal and antithyroperoxidase and antithyroglobulin antibodies were negative. A computed tomography scan of the neck showed a 5 cm enhancing thyroid mass predominantly affecting the right lobe with skin and laryngeal invasion, and a previous lobectomy was also noted (Fig. 1A). Surgical resection was impossible, therefore, a wedge biopsy was taken and a tracheotomy was performed. Histopathology showed fibrous tissue with collagen hyalinization and mononuclear inflammatory cells, with extension into the surrounding tissues (Fig. 1B). The normal tissues were replaced by a mass consisting of a dense matrix of hyalinized connective tissue. There were no mitotic figures and no granulomatous tissue. Based on clinical and laboratory findings, the diagnosis of RT was made and the patient was treated with corticosteroids (prednisone 1 mg/kg/d).
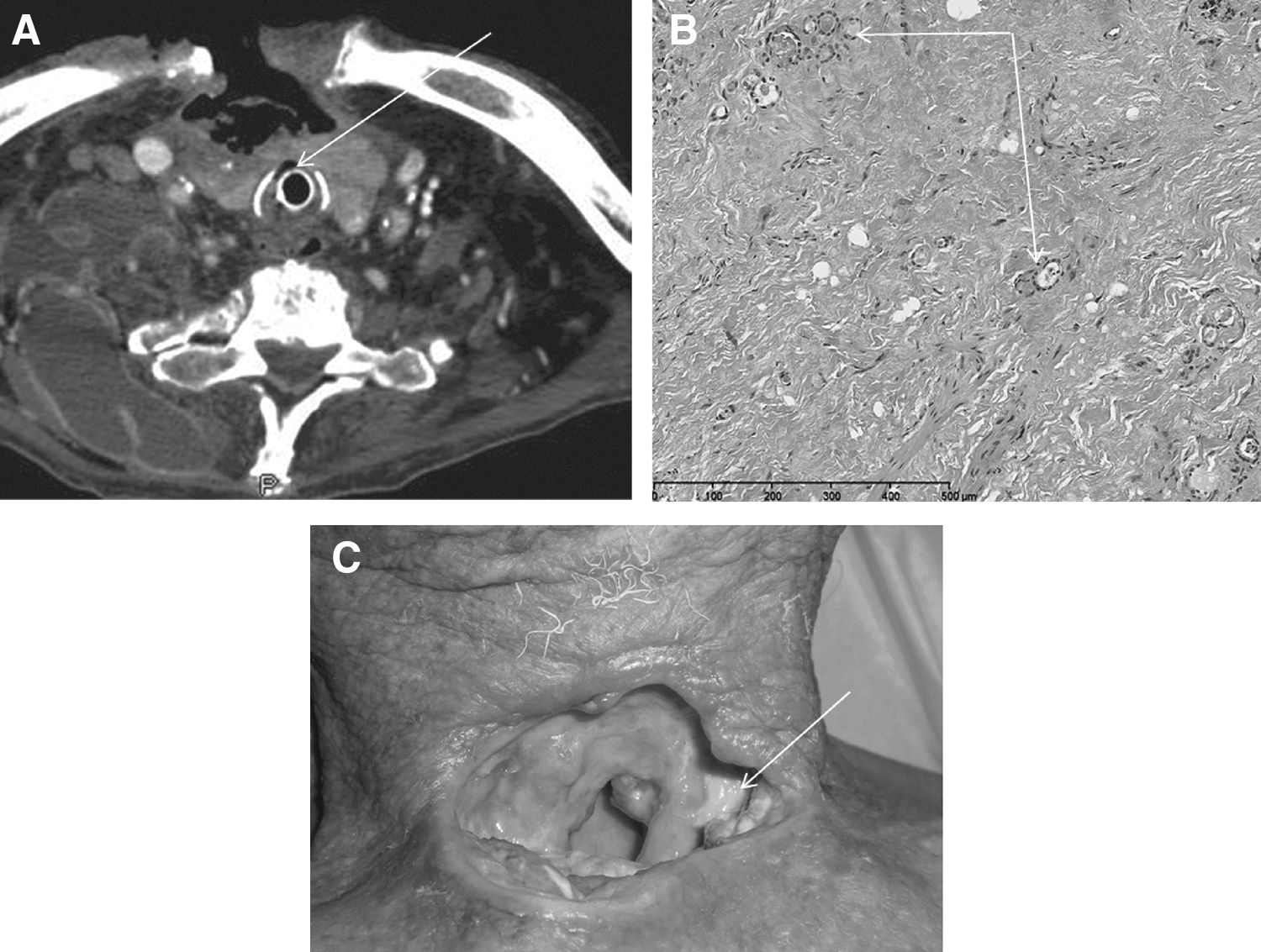
After 1 month with the wound healed, an excavation of the surface of the neck appeared around the tracheotomy (Fig. 1C). The patient developed septic shock secondary to infection of the cervical tissue necrosis, osteitis of the right sternoclavicular joint, and pleural empyema. Streptococcus constellatus was isolated and the patient was given intravenous antibiotic treatment appropriate for the microorganism (imipenem/cilastatin 2 g/d, vancomycin 30 mg/kg/d, and clindamycin 1500 mg/d). Moreover, surgical debridement of the tissue necrosis was performed. There was then a dramatic evolution with extension of cervical necrosis into the thorax, mediastinal collections, and bilateral pleural effusions. The patient died of severe sepsis 15 days after surgery.
Extensive surgery is inappropriate in the management of RT. Corticosteroids, tamoxifen, and immunosuppresive therapies are usually effective and can lead to long-term remission. During the follow-up of the patient reported here, the unusual feature was a rapidly progressing acute necrotizing cellulitis in the neck in a previously healthy and immunocompetent adult. To the best of our knowledge of the literature, this is the first case of necrotizing cellulitis of the neck with mediastinitis to be described. Our patient had been treated by external cervical radiotherapy for a thyroid neoplasm 35 years previously. Radiotherapy leading to late alterations in the mucosa, soft tissue, and skin might be a predisposing factor for the development of severe infection. Radiation causes vascular damage and the association with corticosteroid treatment may have increased the risk of head and neck infection. Three cases of necrotizing fasciitis have been reported in the literature associated with radiotherapy (2,3). The patients had had radiotherapy for head and neck malignancy 9 months (2) and 6 and 14 years (3) previously with no evidence of tumor recurrence. Pereira et al. (4) reported a fatal descending necrotizing mediastinitis secondary to acute suppurative thyroiditis in a healthy young woman. Causative agents of acute suppurative thyroiditis are often gram-positive bacteria. Our patient developed fatal septic shock secondary to an infection due to S. constellatus, a gram-positive, nonsporing, nonmotile, catalase-negative coccus of the S. milleri group (SMG). The SMG constitute part of the normal flora in the oral cavity, urogenital region, and intestinal tract, and several strains of this group have been reported to produce tissue-destroying enzymes such as collagenase and hyaluronidase (5). Therefore descending necrotizing mediastinitis due to SMG can have an aggressive course. Risk factors include poor dental hygiene, diabetes mellitus, alcohol excess, intravenous drug abuse, acquired immunodeficiency syndrome, and recent steroid therapy (6).
In conclusion, immunosuppressive therapy with glucocorticoids associated with a surgical open wound (tracheostomy) and vascular damage due to previous radiotherapy led to fatal neck necrotizing cellulitis in this previously healthy patient with RT. In patients with underlying risk factors as reported here, careful follow-up is necessary after introduction of corticosteroids.
Footnotes
Disclosure Statement
The authors have no conflict of interest to be disclosed.