
Abstract
Background:
Previous studies of thyroid cancer incidence in Wales have given varying results with suggestions of an excess of cases in geographic areas that were previously exposed to the radioactive fallout from the 1986 Chernobyl nuclear reactor incident. Our objective in this study was to provide an up-to-date comprehensive analysis of time trends in the incidence, geographical distribution, and survival from thyroid cancer in Wales.
Methods:
We identified thyroid cancer cases, registered from 1985 through 2010 in the Welsh Cancer Intelligence and Surveillance Unit (WCISU). Age standardized rates were determined from the European standard population. A Poisson regression model was fitted to assess temporal trends and rate ratios (RRs) and confidence intervals (CIs) were determined and compared across consecutive time periods: 1985–1997 and 1998–2010. Standardized incidence ratios were calculated for each of the 22 local authority areas. Relative survival and Kaplan–Meier curves were computed to analyze all cause and thyroid cancer–specific survival.
Results:
A total of 1747 thyroid cancer cases were registered from 1985 to 2010. Age standardized incidence rates were 2.8 and 1.2 per 100,000 population per year for females and males respectively. Incidence rates increased with time (RR 1.3 [CI 1.2–1.5], p<0.001; 1998–2010 vs. 1985–1997). The incidence of papillary cancer increased progressively over the study period (RR 2.22 [CI 1.91–2.57], p<0.001; 1998–2010 vs. 1985–1997), while rates for other (nonpapillary) histological subtypes remained static (RR 0.95 [CI 0.84–1.08], p=0.45; 1998–2010 vs. 1985–1997). We identified two geographical areas of increased incidence, but the spatial distribution of cases was inconsistent with exposure to radioactive fallout. Five-year relative survival from all-cause mortality improved from 74.2 [CI 66.8–80.1] in 1985–1989 to 82.6 [CI 77.1–86.9] in 2000–2004, but remained poor for patients over the age of 65 years (p<0.001, >65 years vs. 15–64 years) and patients with anaplastic thyroid cancer (p<0.001; anaplastic vs. other histological varieties).
Conclusions:
The incidence of thyroid cancer has increased in Wales, predominantly due to an increase in papillary cancers. The current geographical distribution of cases does not support a radiation effect in the region. Survival has remained poor for patients over the age of 65 years and those with anaplastic carcinoma.
Introduction
Only a few studies have specifically addressed the epidemiology of thyroid cancer in Wales (9,10). A survey of the period 1962–1984 identified a focus of increased cases in parts of North and Mid Wales, which was attributed to a high frequency of benign thyroid disorders in these areas (9). In the aftermath of the Chernobyl nuclear reactor incident in 1986, a radioactive cloud reached England and Wales, causing significant radionuclide contamination to areas experiencing heavy rainfall in northern England and North Wales at the time (11). In some affected areas, maximal concentrations of 131I in rainwater was estimated at 10,000 Bq/L, while radiocesium (137Cs) deposition in leafy vegetables reached concentrations as high as 400 Bq/L (11,12). Subsequent reports revealed an excess of childhood thyroid cancers in affected parts of northern England (13,14), but increased incidence or regional variations in cases were not confirmed in Wales (10). Initial studies in Wales were, however, limited by the absence of morphological details (9), incomplete clinical outcome data (9), and a relatively short study interval (10). Thus, it remains unresolved whether thyroid cancer rates in the region have risen in line with global trends, and whether a surplus of cases is to be found in areas exposed to radiation fallout. Our objective in this study was therefore to provide an up-to-date analysis of time trends in the incidence, geographical distribution, and survival from thyroid cancer in Wales using data from the national cancer registry for Wales.
Methods
The Welsh Cancer Intelligence and Surveillance Unit (WCISU) is the national cancer registry for Wales, and holds records for all malignant cancers dating back to 1972. The registry covers the entire resident Welsh population of about 2.9 million persons. The population of Wales is predominantly of white Caucasian ethnicity, with ethnic minorities comprising just 2.9% of the population. The demographic of the region has remained stable for a number of decades, with annual inward and outward migration rates accounting for <1% of the population. WCISU systematically collects data from multiple sources, including inpatient activity via the Patient Episode Database for Wales (PEDW), pathology laboratory data, and death certification registration. WCISU also receives information from other United Kingdom cancer registries for Welsh residents treated outside of Wales. Information routinely collected includes year of cancer diagnosis, year of birth, sex, local authority area of residence, site and morphology of cancer, and year and cause of death. The quality and completeness of WCISU data are subject to routine periodic validation, and a recent analysis using a stratified two-source capture–recapture technique showed 99–100% completeness in ascertainment of childhood cancers (15). Thyroid cancer cases, registered from 1985 through 2010, with the specific codes 193 in the international classification of diseases, ninth edition (ICD-9) or C73 in ICD-10 were identified from the database. Ethical approval for the study was granted by the Research Ethics Committee for Wales, reference 11/WA/0315.
Data analysis
We determined European age-adjusted standardized rates (EASR) according to the standardized European population for the period 1985–2010. Incidence rates were calculated using mid-year population estimates obtained from the Office for National Statistics (ONS) (16). A Poisson regression model was fitted to assess temporal trends (17). Rate ratios (RRs) and confidence intervals (CIs) were determined and compared across two consecutive time periods: 1985–1997 and 1998–2010. For the graphical presentations, temporal trends in incidence rates are plotted as three-year moving averages to avoid marked year-to-year fluctuations in rates that are seen with relatively small patient numbers. The relationship between age and thyroid cancer incidence rates was examined using a linear regression model, with age at diagnosis as the predictor variable and incidence rate as the dependent variable. Data were grouped by the 22 local authority areas in Wales and standardized incidence ratios (SIRs) were determined for each of these areas. The SIR for an area was calculated as the ratio between the observed and expected number of thyroid cancer cases in that area. The expected number of cases was derived from the age- and sex-specific thyroid cancer rates for the whole of Wales (18). CIs were calculated for the SIR assuming a Poisson distribution (19). One- and five-year relative survival rates were estimated from the observed survival of the cohort divided by the probability of survival in the general population for the same period. Kaplan–Meier curves were computed to analyze all-cause as well as thyroid cancer–specific survival rates, and survival according to sex, age group, and histological subtype were compared using the log-rank test. A Cox regression model was used to determine the prognostic role of individual variables on thyroid cancer–specific death. Statistical analyses were performed using SPSS v16.0 (SPSS Inc., Chicago, IL). Stata statistical software release 12 (StataCorp LP, College Station, TX) was used for the Kaplan–Meier survival curves. The level of statistical significance at which the null hypothesis was rejected was chosen as 0.05.
Results
Incidence
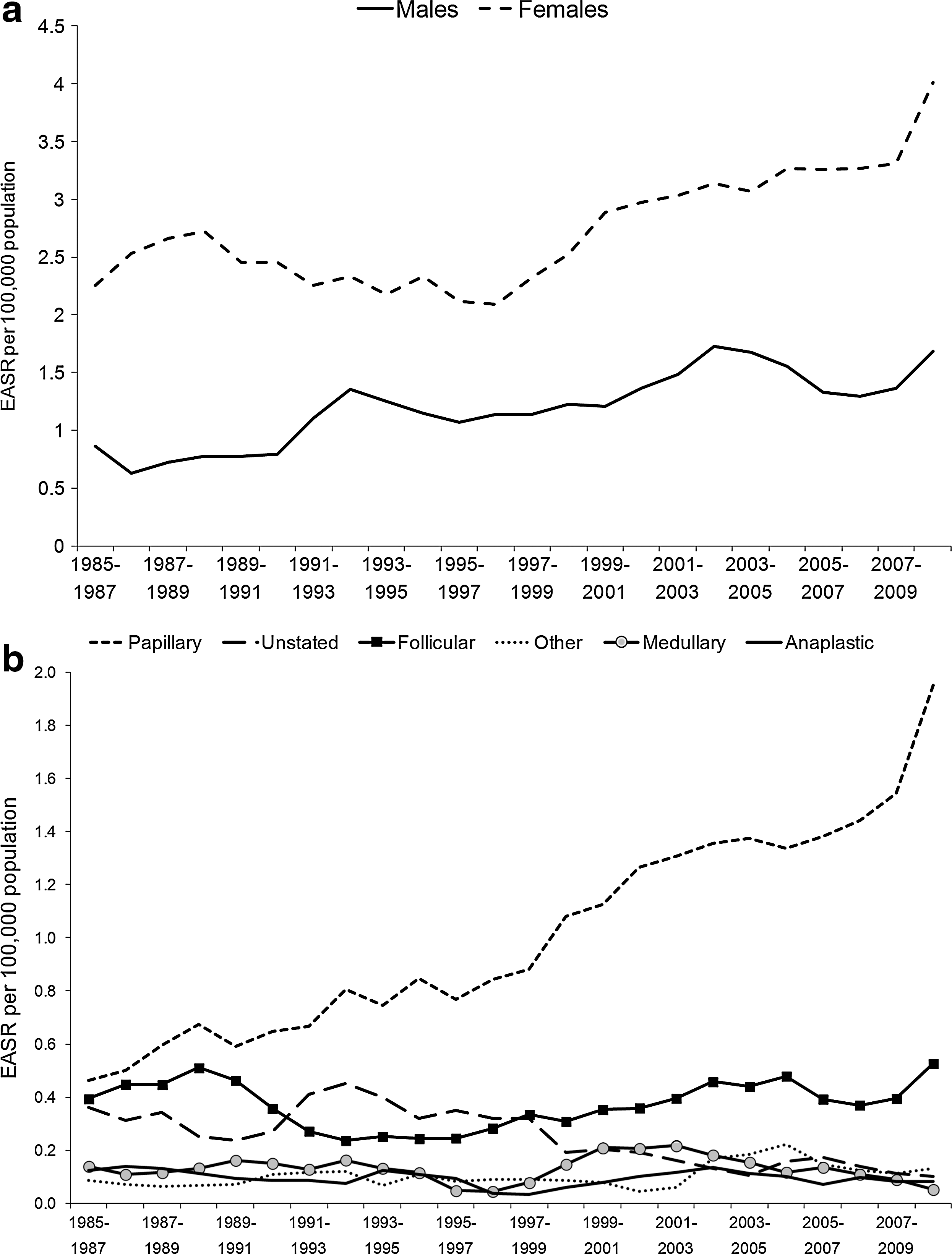
A total of 1747 thyroid cancer cases were registered with the Welsh cancer registry in the years 1985–2010. The age standardized incidence rate of thyroid cancer was 2.0 per 100,000 per year over the entire study period (Table 1). Thyroid cancer was more common in females than in males (RR 2.50 [CI 2.25–2.78], p<0.001) and incidence rates rose steadily with increasing age (p<0.001 for trend). A sharp increase was observed after the age of 65 years in both sexes, with peak incidence above 85 years of age in males. For females, peak incidence was seen in the 75–84-year age group in 1985–1997, whilst in 1998–2010 the peak incidence was apparent in those over the age of 85 years (Table 1). Figure 1a shows time trends in incidence rates according to sex. A progressive increase in incidence was seen throughout the duration of the study period, with a higher rate in the latter time period (1998–2010) compared to the first half of the overall period (1985–1997) (RR 1.34 [CI 1.22–1.48], p<0.001). The increase in thyroid cancer incidence from 1985–1997 to 1998–2010 was evident in both males (RR 1.51 [CI 1.26–1.81], p<0.001) and females (RR 1.27 [CI 1.14–1.43], p<0.001), and did not differ between the sexes (p=0.09). The temporal increase in incidence was also seen across all age groups: 0–24 years (RR 1.86 [CI 1.23–2.82], p<0.001), 25–54 years (RR 1.56 [CI 1.33–1.72], p<0.001), and>55 years (RR 1.26 [CI 1.11–1.43], p<0.001).
Thyroid cancer incidence trends in Wales, 1985–2010, by
Rates per 100,000 population per year.
European Age-Standardized Rate per 100,000 population per year [CI].
World Age-Standardized Rate per 100,000 population per year [CI].
Histological subtypes
A histological diagnosis was recorded in 85% of all cases. The completeness of histological information improved over time, with a morphological diagnosis available in 91% of patients in the latter half of the overall study period. Papillary thyroid cancer was the most common histological variety, accounting for 47% of cases. The other histological groups comprised follicular (19%), anaplastic (7%), medullary (6%), and other/non-specific histology (21%). This latter group comprised 15% with a recorded diagnosis of carcinoma (NOS, not otherwise specified) and 6% with other miscellaneous diagnoses, including squamous-cell carcinoma, adenocarcinoma, and malignant lymphoma. Figure 1b shows time trends of thyroid cancer rates according to histological subtypes. Rates for papillary cancer increased progressively over the study period (RR 2.22 [CI 1.91–2.57], p<0.001), while rates for other (nonpapillary) histological subtypes remained static (RR 0.95 [CI 0.84–1.08], p=0.45). The frequency of patients with an unstated histological diagnosis reduced over time (RR 0.52 [CI 0.37–0.62], p<0.001), possibly reflecting improved data coding.
Geographical distribution
Figure 2 shows the distribution of thyroid cancer cases across the various local authority areas in Wales, mapped according to the 2010 local authority boundaries. This was based on the place of residence for individual patients at the time of diagnosis. The standardized incidence ratios for the local authority areas are presented in Supplementary Table S1 (Supplementary Data are available online at
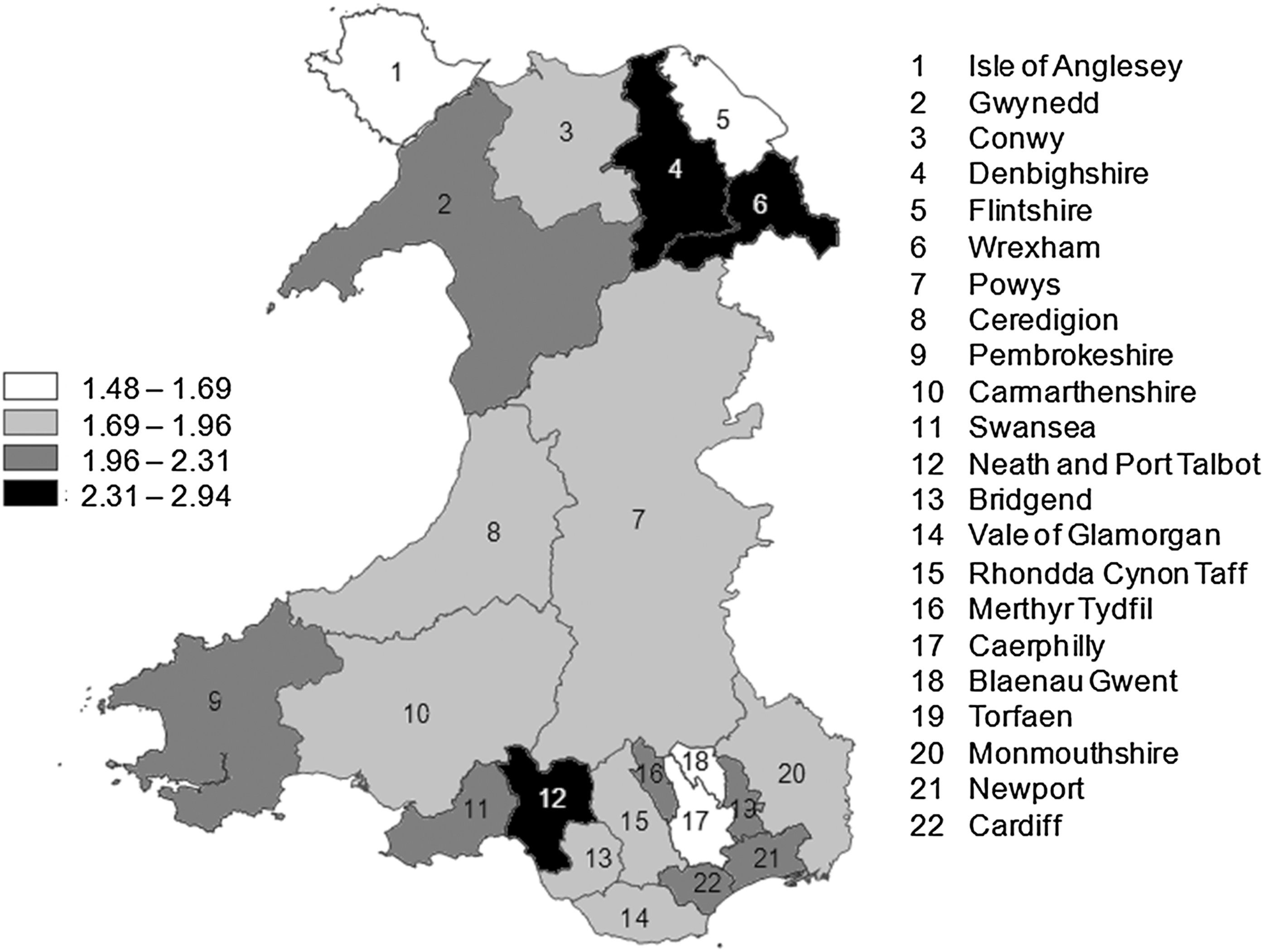
Thyroid cancer incidence by Welsh local authority areas, 1985–2010.
Survival
Survival was determined for five-year diagnosis periods for all-cause and thyroid cancer–specific mortality (Table 2). One and five-year relative survival from all-cause mortality improved from 79.5 [CI 73.0–84.5] and 74.2 [CI 66.8–80.1] respectively in 1985–1989 to 86.6 [CI 81.7–90.3] and 82.6 [CI 77.1–86.9] respectively in 2000–2004 (Table 2). However, the CIs for these survival rates are wide. The effects of age, sex, and histology on survival were analyzed using Kaplan–Meier survival curves (Figs. 3 –5). Survival was analyzed separately for thyroid cancer and all-cause mortality for the two time periods 1985–1994 and 1995–2004. Factors that significantly reduced survival were male sex, age over 65 years, and anaplastic histological subtype. Males had reduced survival from all-cause mortality in both time periods (Fig. 3). However, reduced thyroid cancer–specific mortality was only seen in males in the latter time period (1995–2004) (Fig. 3). Reduced survival for both thyroid cancer–specific and all-cause mortality was seen in patients over the age of 65 years (Fig. 4). Patients with anaplastic thyroid cancer had the worst outcomes overall (Fig. 5), and in addition they had poorer survival compared to the other histological groups combined (p<0.001).

Kaplan–Meier curves for thyroid cancer survival according to sex:

Kaplan–Meier curves for thyroid cancer survival according to age:
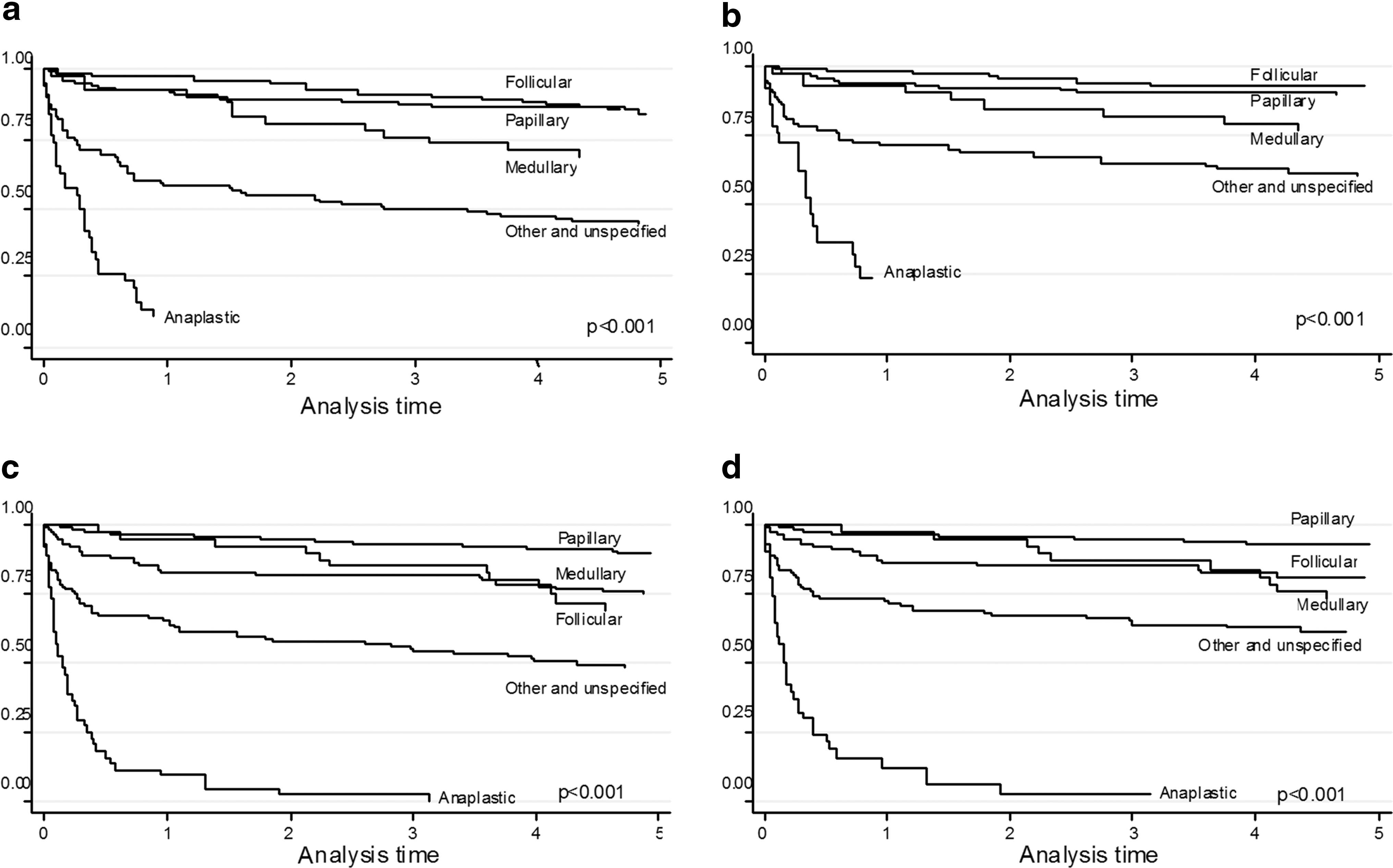
Kaplan–Meier curves for thyroid cancer survival according to histology:
NA, not able to produce reliable estimates, since the number of deaths in the analysis is very small; NP, not possible to calculate five-year survival for cases diagnosed in 2005–2009 at present.
We performed stepwise Cox regression analysis to determine the prognostic effect of individual variables on thyroid cancer–related mortality. Factors that were entered into the multivariate model included age, sex, and histological type. Thyroid cancer–related death was higher for male sex (Hazard ratio (HR) 1.32 [CI 1.07–1.62], p=0.01), older age (HR 1.69 [CI 1.57–1.81], p<0.001, per 10-year increase in age), and anaplastic histological variety (HR 2.00 [CI 1.51–2.62], p<0.001).
Discussion
The current study extends previous analysis of thyroid cancer trends in Wales. Our study has been facilitated by the availability of a single robust cancer registry in Wales that has systematically collected records over the past four decades. The ethnic homogeneity and relative stability of the population limit confounding influences from ethnicity and migration that may be difficult to control for in larger, more dynamic, heterogeneous populations. More so, regional differences in exposure to radioactive fallout in Wales present a unique backdrop to observe the potential effects of environmental radiation on thyroid cancer risk. Here, we show that the incidence of thyroid cancer in Wales has risen progressively over the last two decades and that this trend is almost exclusively due to an increase in the incidence of papillary thyroid cancers.
The incidence of thyroid cancer in our study is similar to other parts of the United Kingdom, but is relatively lower than in countries such as the United States and Israel (4,9,20 –23). We also observed an age-related increase in thyroid cancer incidence, with peak rates occurring after 65 years. This age trend is similar to data from some other parts of the United Kingdom such as Scotland (20), but differs from several other reports elsewhere, which show earlier peak rates of occurrence (24). While these differences will require further clarification and monitoring, the rising frequency of papillary thyroid cancers observed in this study is consistent with the vast experience elsewhere, including the United States (5), Canada (24), Australia (25), Denmark (26), and Italy (27). A number of studies have demonstrated that most of this increase is due to the detection of small-sized papillary cancers (5,21,22), a trend driven by modern diagnostic practice such as the growing use of fine-needle aspiration biopsy and increased access to imaging techniques like ultrasound, computerized tomography scans, and positron emission tomography scans (28). As clinical practice in Wales is not different from other countries in this respect, it is perhaps the case that increased detection of thyroid cancers is at least partially responsible for the increased incidence rates in the region.
A true increase in thyroid cancer incidence is, however, possible. The link between thyroid cancer and exposure to atmospheric irradiation is well recognized, exemplified by the unprecedented rise in thyroid cancer cases observed in many parts of Europe in the wake of the Chernobyl incident (8,29). A possible radiation effect on thyroid cancer incidence in Wales is of interest, since high levels of soil and livestock contamination were detected in the northern Welsh areas in the days following the Chernobyl incident (11,12). For a radiation effect to be plausible, we would expect a surplus of cases in high-exposure areas (northern local authority areas) relative to low-exposure areas (mid and southern local authority areas), especially in children, who are known to be more susceptible to the thyroid carcinogenic effects of radiation. However, we found little regional variation in thyroid cancer incidence even after our analysis was stratified by age and sex. Only two areas, Denbighshire and Swansea, had incidence rates exceeding the national average. This variation is unlikely to be explained by radiation, since Swansea was never exposed to the Chernobyl fallout, and excess cases were not recorded in the North Wales local authority areas that were exposed to radiation, other than Denbighshire. Thus, it is possible that the excess cases recorded in these local authority areas could have arisen by chance more so as the number of cases in individual areas was relatively small.
Furthermore, it seems plausible that geographical variations in thyroid cancer incidence were already present in England and Wales before the Chernobyl incident. In an analysis of the period 1962–1984, dos Santos Silva and Swerdlow identified areas of increased thyroid cancer incidence that included parts of North Wales and the coastal areas of Anglesey (9). This focus of cases was attributed to the high frequency of benign thyroid disorders in these areas using mortality data on “exophthalmic goiter” as a proxy for benign thyroid disease (9). A later study by Paterson et al. did not confirm these regional trends, although the geographical analysis in this report was restricted to relatively large administrative divisions (10). Of the original high-incidence areas identified by dos Santos Silva and Swerdlow, only Denbighshire in our study still records an increased thyroid cancer incidence. While this may imply that the initial focus of thyroid cancer risk is disappearing, we cannot exclude the possibility that differences in the completeness of coding data may explain some of these discrepancies.
Other factors are less likely to explain our findings. Increased thyroid cancer risk has been reported in association with radiation therapy for benign head and neck lesions, but this practice was never really prevalent in the United Kingdom. The occurrence of thyroid cancer may also be influenced by the iodination status of the population; papillary thyroid cancers are common in iodine sufficiency while follicular and anaplastic cancers become more prevalent in iodine deficiency states (30). Although Wales has enjoyed stable iodine nutrition status for a number of decades, recent dips in iodine nutrition have been observed in the region (31). Even though we recorded a lower ratio of papillary to follicular cancers than in some other iodine-replete populations, the absolute frequency of follicular cancers remained unchanged throughout the study period. Furthermore the current fluxes in iodine nutrition status in the United Kingdom are unlikely to have been in existence long enough to explain our findings. It is also possible that the improving quality of coding data, together with revisions in histological criteria for papillary thyroid cancers (32), could have contributed to an artificial increase in papillary cancers. However, the potential impact of these factors is perhaps modest at best.
Despite the rising incidence of thyroid cancer, survival has continued to improve in Wales. In a previous analysis, it was suggested that outcomes in the region were poorer than in the rest of Europe, based on a comparison of local thyroid cancer mortality rates with data from Europe (10). However, these comparisons were not stratified by age, sex, or histological subtypes. The current study suggests that survival has improved over time in Wales. The one- and five-year thyroid cancer–specific survival rates of 88% and 86% respectively, in 2000–2004, are comparable with data from Scotland (20). Some of these improvements in survival will no doubt be attributable to earlier diagnosis and prompt treatment of patients in regional multidisciplinary care networks.
Our study has limitations. As with all database research, our findings rely on the quality of the coded data. Detailed morphological coding was deficient in a small percentage of cases, and data on the size of the tumors were not routinely available, such that we were unable to determine the frequency of small tumors in our cohort, which would have clarified whether the observed trend was due to the increasing diagnosis of smaller tumors. Expansion of the currently held data sets for thyroid cancer in the Welsh registry to incorporate more comprehensive staging details will allow better insights into the factors driving the current trends.
We conclude that thyroid cancer incidence in Wales has increased in recent decades, mostly due to papillary thyroid cancers with good prognoses. Survival has continued to improve, whilst outcomes remain poor for undifferentiated histological subtypes and older patients. We identified two geographical areas of increased thyroid cancer incidence in Wales. The spatial distribution of cases, however, could not be explained by a radiation effect, and the increased incidence in these two areas may have arisen by chance. Continued monitoring of thyroid cancer incidence in the region will be essential in fully understanding these trends.
Footnotes
Acknowledgment
We thank the Welsh Cancer Intelligence and Surveillance Unit (WCISU) for providing data for the study.
Author Disclosure Statement
No competing financial interests exist.