
Abstract
Aim:
There is little information regarding the reference range for thyroid hormones in preterm babies, especially those with very low birth weight (VLBW) of less than 1500 g. The objective of our study was to evaluate the relationship between thyroid hormone levels and postmenstrual age in a cohort of stable VLBW infants.
Method:
An observational cohort study of VLBW infants preparing for discharge from a high-dependency nursery in Singapore. The infants' free thyroxine (fT4) and thyrotropin (TSH) levels were assayed just before discharge and correlated with postmenstrual age, calculated as the sum of the duration of gestation at birth and chronological age in weeks.
Results:
fT4 and TSH levels were sampled in 129 ex-VLBW babies at a mean postmenstrual age of 38.5 (±4.6) weeks. The babies were born at a mean±SD gestation of 28.9±2.4 weeks (median 29.0 weeks, range 24.0–34.5 weeks) with mean±SD birth weight of 1081±268 g (median 1090 g, range 490–1490 g). Linear regression analysis revealed negative and fair correlation between fT4 and postmenstrual age (r=−0.302). The mean±SD fT4 level was 16.8±3.2 pmol/L (median 16.8 pmol/L, range 8.5–28.9 pmol/L). However, there was only a very weak negative correlation between TSH levels and postmenstrual age, both with (r=−0.116) or without logarithmic transformation. The mean±SD TSH was 4.56±2.50 mIU/L (median 4.42 mIU/L, range 1.0–13.5 mIU/L).
Conclusion:
Our study shows a fair and inverse correlation of fT4 with postmenstrual age in a large cohort of growing ex-VLBW infants, in keeping with maturation of the hypothalamic–pituitary–thyroid axis. It suggests that fT4 levels in growing infants are best compared to postmenstrual age-specific norms instead of a single reference interval.
Introduction
T
Preterm babies, particularly babies with very low birth weight (VLBW) of less than 1500 g, often have a delayed TSH elevation. A delayed TSH elevation has been attributed to immaturity of the hypothalamic–pituitary–thyroid axis, delayed production or secretion of thyroid hormones, and a limited response of the gland in a sick neonate (2). Rescreening of the VLBW infant for hypothyroxinemia is thus recommended to detect delayed hormone abnormalities that would otherwise have been missed during the initial screen at birth (3).
An optimal timing for rescreening thyroid hormones in the VLBW neonate is uncertain. Longitudinal measurements of thyroid hormone levels in VLBW babies has previously shown inconsistent results. While some authors found little or no correlation of thyroid hormones with gestation and postnatal age (4 –7), others reported a positive correlation of fT4 levels with gestational age in the first week of life (8 –10), at two weeks (11), four weeks (12), six weeks (13,14), and up to eight weeks of age (15).
The majority of VLBW infants are typically discharged when they have reached body weights of about 2 kg and are medically stable. This usually corresponds to postmenstrual ages (PMA) at or near term. While there are reference ranges for thyroid hormones in newly born infants, information on the range for the growing VLBW infant remains scarce (8 –15). Furthermore, normative reference intervals are population and assay dependent.
The objective of our study was to establish reference ranges of thyroid hormones in a cohort of VLBW infants as they were being prepared for discharge from hospital. A secondary aim was to evaluate the relationship between thyroid hormone levels and the infants' postmenstrual age. Our hypothesis was that a significant correlation exists between fT4 and the postmenstrual age of the infant.
Materials and Methods
This was an observational cohort study of infants at a high-dependency nursery at Singapore General Hospital, a tertiary care teaching institution. The study population included consecutive babies born between January 2009 and December 2011, with VLBW of <1500 g. Babies with a history of respiratory disorders (such as hyaline membrane disease) were included if they had recovered from the illness at the time of sampling. Babies who died, were diagnosed with major congenital anomalies, had blood-culture positive septicemia, or who were receiving inotropic or steroid therapy were excluded. Babies born to mothers with endocrine disorders or substance abuse were also excluded. Ethical approval for the study was granted by the SingHealth Centralized Institutional Review Board (reference 2011/617/E).
The infants' gestational age was determined from the mothers' last menstrual date or first trimester ultrasound scan. In the absence of an early dating scan, the Dubowitz (16) or Ballard (17) score was used to estimate gestation. Babies were classified as small for gestational age (SGA) or large for gestational age (LGA) if their birth weights fell below the 10th percentile or above the 90th percentile for gestation respectively on intrauterine growth charts. Clinical data were extracted from case records. Postmenstrual age (PMA, in weeks) was calculated as the sum of the duration of gestation at birth and chronological age in weeks. For example, a baby born at 26 weeks gestation who is 10 weeks old would have a postmenstrual age (PMA) equivalent to 36 weeks. Blood sampling for fT4 and TSH levels was carried out in the mornings in the week before discharge and usually timed to coincide with sampling for other tests. One mL of venous blood was taken for biochemical assays.
Collected serum samples were stored at 2–8°C if analyzed within 6 h or at −20°C until analysis. fT4 and TSH concentrations were determined on the UniCel® DxI 800 Access® immunoassay system (Beckman Coulter Inc., Chaska, MN, USA) using chemiluminescence detection methods performed at the hospital laboratory (18). Results were made available to medical staff within the day. Reference intervals for fT4 and TSH had recently been established on this platform, according to the infants' age of 5 days to <2 months (fT4 11.4–29.4 pmol/L, TSH 1.23–11.5 mIU/L) or 2 months to 5 years (fT4 8.5–20.4 pmol/L, TSH 0.271–7.71 mIU/L). Reference intervals were unavailable in those less than 5 days old because of unit policy to avoid sampling during the period of TSH surge in the first 5 days of life. Intra-assay coefficients of variance (CV %) for fT4 at 7.0, 32.0, and 61.5 pmol/L were 3.6, 3.2, and 2.0 respectively. Respective inter-assay CVs (%) for fT4 were 4.0, 3.1, and 3.0. Similarly, intra-assay CVs for TSH at 0.39, 5.6, and 34.4 mIU/L were 5.5, 4.6, and 4.2% respectively. Respective inter-assay CVs (%) for TSH were 5.5, 5.4, and 5.5.
Statistical analysis was performed using SPSS v17 (SPSS Inc., Chicago, IL). Statistical outliers were excluded using the Dixon Reed rule. Nonparametric statistics were employed for analysis. Upper and lower reference intervals were based on the 2.5th and 97.5th percentile cut-offs. Analysis of relationship between hormone levels and postmenstrual age was carried out using linear regression with Pearson's correlation coefficient and analysis of variance (ANOVA) for between-group differences after categorizing PMA into two-week gestation intervals. Logarithmic transformation of TSH was applied to obtain normal distribution. Values of p<0.05 were considered significant.
Results
The study population consisted of 147 VLBW babies over the three-year period. Of these, 14 died and 4 were excluded because of incomplete data or missing blood samples. No babies were born to mothers with thyroid disease or substance abuse. None of the infants was receiving inotropes or steroids at the time of sampling. This left 129 babies for analysis.
The babies were born at a mean±SD gestation of 28.9±2.4 weeks (median 29.0 weeks, range 24.0–34.5 weeks). They had mean±SD birth weight of 1081±268 g (median 1090 g, range 490–1490 g). Of 129 babies, 33 (26%) were born SGA, whereas only one (1%) infant was classified as LGA. Blood sampling for fT4 and TSH was performed at a mean±SD chronologic age of 9.6±4.7 weeks, corresponding to a postmenstrual age of 38.5±4.6 weeks, which would be equivalent to term. Median (range) postmenstrual age at sampling was 37.6 (33.0–57.0) weeks. Demographic characteristics of the study population are shown in Table 1. None of the infants received a diagnosis of a thyroid disorder. Offspring of 17 sets of multiple births (14 pairs of twins, 3 sets of triplets) showed similar thyroid hormone values within each set (data not shown).
Values are expressed as number (percentage). n=129.
AGA, appropriate for gestational age; SGA, small for gestational age; LGA, large for gestational age; LSCS, lower segment Caesarean section.
Figure 1 depicts the relationship between fT4 and PMA. Pearson's correlation coefficient, r, was equal to –0.302, indicating a negative and fair correlation between fT4 values and postmenstrual age (p=0.001). Table 2 shows mean±SD and median (range) fT4 values of the study population at different PMA categorized by two-week intervals. Analysis of variance showed significant between-group differences (p=0.02). The mean±SD fT4 level for the entire cohort was 16.8±3.2 pmol/L (median 16.8 pmol/L, range 8.5–28.9 pmol/L).

Relationship between free thyroxine (fT4) levels and postmenstrual age (PMA) of the ex-preterm cohort. Pearson's correlation coefficient r=−0.302.
*p=0.02; ** p=0.5.
fT4, free thyroxine; TSH, thyrotropin.
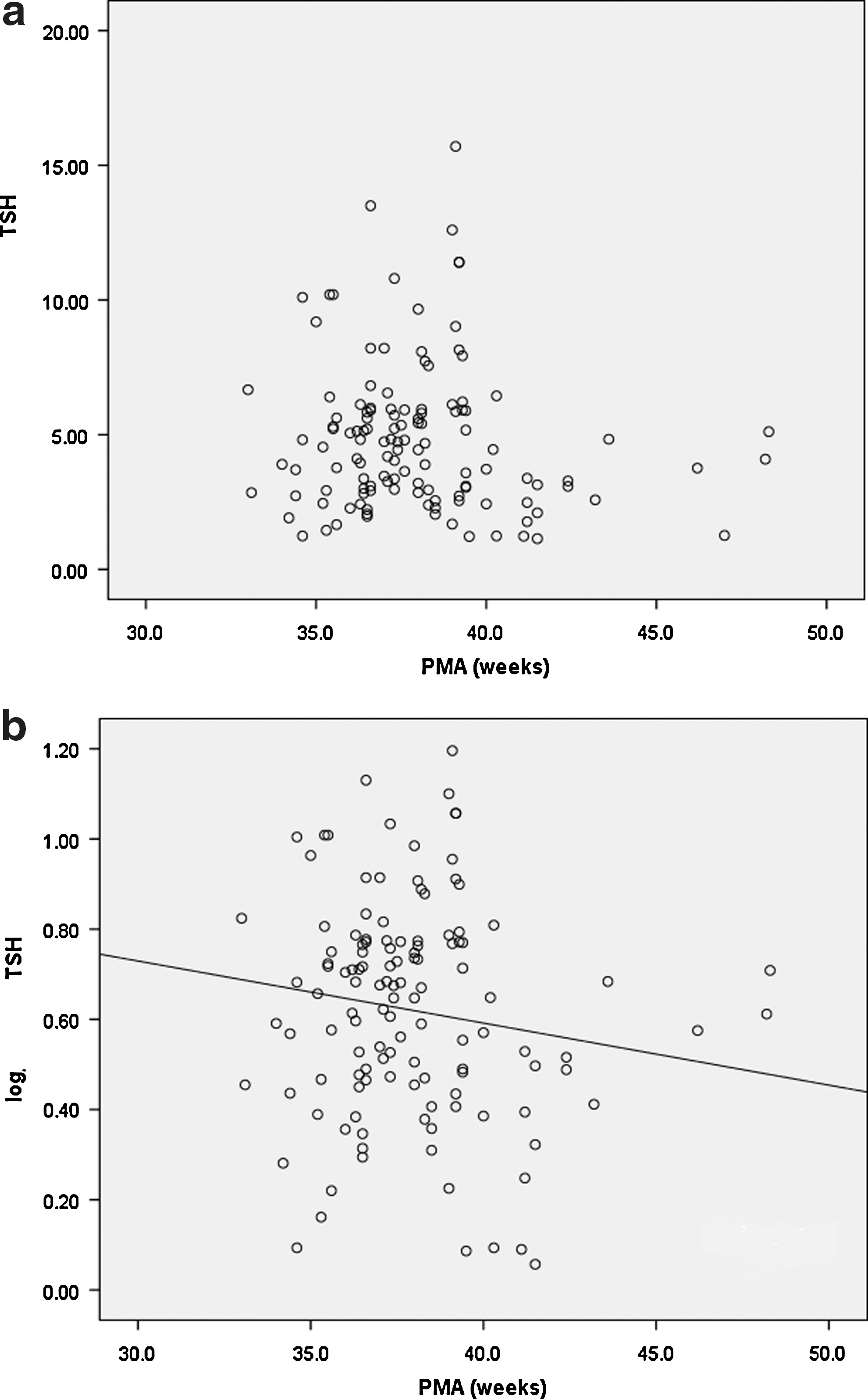
Table 2 shows that the mean±SD TSH of the cohort was 4.56±2.50 mIU/L (median 4.42 mIU/L, range 1.0–13.5 mIU/L). Analysis showed no significant differences when the values were categorized by two-week intervals. Figure 2a depicts the relationship between TSH and postmenstrual age. As correlation analysis showed only a very weak negative correlation (r=−0.116), reanalysis was carried out after logarithmic transformation of TSH values. Log-TSH values similarly did not show a strong correlation with postmenstrual age when categorized as two-week intervals (Fig. 2b). ANOVA showed no significant between-group differences (p=0.5).
Discussion
Although reference ranges for thyroid hormones are easily available for term infants, there is scarce information about the range in preterm babies. Interpretation of thyroid hormone values in preterm infants after the first week of life is fraught with difficulty. Reasons for this include a lack of agreement of the definition of a “healthy” preterm baby (4), maturational changes in fT4 that often occur in the last trimester of pregnancy, and nonthyroidal illnesses such as respiratory distress syndrome that may potentially affect thyroid hormone values (14,15). Furthermore, concurrent therapy with inotropes and steroids were shown to increase hormone levels. Yet, it is important to diagnose hypothyroidism in the preterm infant, as early diagnosis has been shown to lead to better outcomes.
Rescreening the VLBW infant will detect cases of late TSH elevation, but there is no consensus about an optimal timing for rescreening. We chose to assay thyroid hormone levels in VLBW infants around the time of discharge from hospital, since the ex-VLBW infant is likely to be relatively “healthy” before discharge, with little need for medication apart from nutritional supplements. Since the hypothalamic–pituitary–thyroid axis in the preterm infant is still maturing, a single reference interval irrespective of gestation can potentially lead to misclassification. Reference intervals are furthermore population-specific and dependent on the assay method. It cannot be assumed that the VLBW infant growing to a postmenstrual age near term would have an identical reference range of thyroid hormone values as those born at term.
In our study, the mean ±SD fT4 for the cohort of ex-VLBW infants was 16.8±3.1 pmol/L when assayed at a mean postmenstrual age of 38.5 weeks, while the 2.5th and 97.5th centiles were 11.13 and 24.53 pmol/L respectively. These values lie well within the range of 11.4–29.4 pmol/L that had been previously established for term infants aged 5 days to <2 months. In particular, the fT4 range of ex-VLBW survivors at 38 weeks (11.3–25.8 pmol/L) was similar to that of normal newborns (9.9–19.4 pmol/L). Likewise, the TSH range of ex-VLBW survivors at 38 weeks (2.0–10.8 mIU/L) was similar to that of normal newborns (2.1–16.8 mIU/L).
There was fairly good and inverse correlation of fT4 with postmenstrual age (r=−0.302), in keeping with the maturation of the hypothalamic–pituitary–thyroid axis. The correlation suggests that fT4 levels in growing VLBW infants are best compared to postmenstrual age–specific norms instead of a single reference interval. Our results are in agreement with those of Adams et al. (8) and Reuss et al. (9), but differ from those who found no correlation with gestation or postnatal ages (4,5,6,7). On the other hand, there was only a very weak correlation (r=−0.116) of TSH around the postmenstrual age of 38.5 weeks, with or without logarithmic transformation.
To our knowledge, this is the first report showing a fair and inverse correlation of fT4 with postmenstrual age in a large cohort of stable growing ex-VLBW infants. The advantage of rescreening ex-VLBW babies just before discharge lies in the ability to interpret results during the period of time when the infant would be relatively free of illnesses that are often diagnosed soon after birth. Availability of reference intervals for thyroid hormones based on postmenstrual age enables the neonatologist to classify correctly for clinical decision making. Further studies will be required to see if these results can be extended to similar populations using different assay methods.
Footnotes
Acknowledgments
We thank Ms. Stephanie Fook-Chong, Biostatistician, Department of Health Services Research for Statistical Analysis, and Associate Professor Fabian Yap, Senior Consultant, Endocrinology Service, Department of Pediatric Medicine, KK Women's and Children's Hospital, Singapore, for the manuscript review.
Author Disclosure Statement
There were no conflicts of interest for the authors arising from this study.