
Abstract
Background:
The X-linked inhibitor of apoptosis protein (XIAP) is associated with carcinogenesis, cancer progression, and metastasis through inhibition of the caspase-mediated apoptotic pathway. The BRAFV600E mutation is the most common genetic alteration and an established prognostic marker in papillary thyroid cancer (PTC). The prevalence of the BRAF mutation is very high and is up to 80% in Korean PTC patients. In the present study, we evaluated the potential role of XIAP expression as a novel prognostic marker to predict recurrence, in combination with the BRAFV600E mutational status.
Methods:
The study enrolled 164 patients with conventional PTC who underwent bilateral thyroidectomy followed by immediate 131I ablation. The presence of the BRAFV600E mutation was evaluated by direct sequencing. The degree of XIAP expression was evaluated by immunohistochemical (IHC) staining using a monoclonal antibody.
Results:
The BRAFV600E mutation was found in 123 of 164 patients (75%) with classical PTC. XIAP expression was positive in 128 of 164 patients (75%), and positive XIAP expression was significantly associated with the presence of lateral cervical lymph node metastases (p=0.01). XIAP expression was more frequent in BRAFV600E mutated PTCs than in BRAF wild type PTCs (p=0.048). The BRAFV600E mutation was significantly associated with cancer recurrence in study subjects (hazard ratio=2.98, p=0.039). PTCs positive for the BRAFV600E mutation but negative for XIAP expression had a significantly higher rate of recurrent PTC (hazard ratio=4.53, p=0.012).
Conclusion:
The evaluation of XIAP expression and BRAF mutational analysis was more useful for the prediction of cancer recurrence in patients with PTC than BRAF genotype alone.
Introduction
P
The BRAFV600E mutation is a promising prognostic biomarker that may help to optimize the management of PTC. Previous studies report that the BRAF mutation is associated with poor clinicopathological parameters and an increased rate of recurrence (4,5). Xing et al. reported that the BRAF mutation independently predicted PTC recurrence, even in conventionally low-risk patients (4). However, the prevalence of the BRAFV600E mutation in PTC ranges from 30% to >80%, depending on geographic area and iodine consumption (6). Although the prognostic value of the BRAF mutation may allow better risk stratification, this molecular marker is less useful and of limited value for clinical decision making in Korea, where up to 83% of PTC cases harbor the BRAFV600E mutation. Therefore, novel and effective molecular markers are required for predicting PTC recurrence in areas with a higher prevalence of the BRAFV600E mutation.
The X-linked inhibitor of apoptosis protein (XIAP) is a member of the IAP protein family that selectively binds and inhibits caspases-3, -7, and -9. XIAP blocks the downstream portion of the apoptotic pathway and inhibits cell death in response to multiple stimuli (7,8). XIAP expression is increased in a number of human malignancies, including colorectal, esophageal, ovarian, renal cell, hepatocellular, and prostate cancer (8). The functional and prognostic significance of XIAP expression in many cancers is still unclear (9,10). A previous study has reported higher XIAP expression in thyroid cancer compared to benign thyroid disease (11). We also confirmed that there was a significant association between XIAP expression and lateral neck lymph node metastases in patients with PTC (12).
In the present study, the association between XIAP expression and the BRAFV600E mutation was evaluated in conventional PTC cases. We also analyzed whether XIAP expression could be useful for the prediction of cancer recurrence in combination with BRAFV600E mutational status in Korean patients with PTC.
Materials and Methods
Patients
The study enrolled 164 consecutive patients diagnosed with classical PTC who underwent total or near-total thyroidectomy followed by immediate 131I remnant ablation between 1996 and 1998 according to a protocol established by the Endocrinology Division of the Asan Medical Center as previously reported (12). Information from the database was reviewed following approval from the Institutional Research Ethics Board. Patients with radioiodine uptake outside the thyroid bed on initial post-treatment whole-body scan (WBS) or any radioiodine uptake on the diagnostic WBS at one year after remnant ablation were excluded.
DNA isolation and evaluation of the BRAFV600E mutation
DNA was extracted from paraffin-embedded tumor specimens, and the presence of the BRAFV600E mutation was evaluated using polymerase chain reaction (PCR) amplification and direct sequencing, as previously reported (13). Each DNA sample was analyzed at least twice to confirm the status of the BRAFV600E mutation.
Thyroid samples and immunohistochemical analysis of XIAP
All thyroid specimens were stained using hematoxylin and eosin, and reviewed by two pathologists. A total of 164 paraffin-embedded specimens of classical PTC were analyzed. Protein expression of XIAP was evaluated by immunohistochemistry (IHC) with a monoclonal anti-XIAP antibody (BD Biosciences, Franklin Lakes, NJ) and diaminobenzidine were used, as previously reported (12).
The extent of staining was graded semi-quantitatively as follows: 0, no foci; 1+, rare or few foci; 2+, multiple foci; 3+, regional-diffuse staining. Staining intensity was also graded semi-quantitatively as follows: 0, negative; 1+, weak; 2+, moderate; 3+, strong. A PTC sample was classified as XIAP positive if the sum of the extent score and the intensity score was greater than or equal to four points.
Follow-up protocol
Patients were treated according to the institutional initial treatment and follow-up strategy, which has been previously reported (14). Diagnostic WBS with 147 MBq 131I and measurement of thyroglobulin and antithyroglobulin antibody level during thyroid hormone withdrawal were carried out 6–12 months after remnant ablation in every patient, and thereafter every one or two years on the basis of clinical suspicion in high-risk patients. Recurrence was defined as the appearance of pathologically proven malignant tissue and/or the appearance of metastatic lesions in the lungs, bones, and/or in brain during the follow-up periods.
Ethics statement
Formalin-fixed, paraffin-embedded tumor specimens were obtained from archival paraffin blocks after approval from the Institutional Review Board of the Asan Medical Center. Informed consent was exempted by the board.
Statistics
Categorical variables are presented as numbers and percentages, and continuous variables as means±standard deviations or median values with a range. The Student's t-test was used to compare continuous variables such as age and tumor size after confirming normality. Fisher's exact test or the chi-square test was used for the comparison of categorical variables between each group. The Kaplan–Meier method was used to generate survival curves, and log-rank of trends performed for the comparison of recurrence-free survival between each group. The Cox proportional hazards model was used to analyze prognostic markers for recurrence-free survival. The relative risks for recurrent PTC are presented as the hazard ratios (HR) and confidence intervals (CIs), which were calculated using binomial distribution. p-Values are two-sided throughout, and p<0.05 was considered statistically significant. R v2.15 and the R libraries Survival, Car, and Cairo were used to analyze data (R Foundation for Statistical Computing, Vienna, Austria;
Results
Association between clinicopathological parameters and BRAFV600E mutations in PTC
A total of 164 patients (28 men and 136 women) with a mean age of 44±13 years were enrolled. The BRAFV600E mutation was found in 123 of 164 patients (75%) with classical PTCs. The clinical and pathological characteristics of the study patients are shown in Table 1. The presence of the BRAFV600E mutation was significantly correlated with a larger tumor size (p=0.03), and was marginally associated with male sex (p=0.06). There was no significant association between the BRAFV600E mutation and age, tumor multifocality, lymphovascular invasion, extrathyroidal invasion, cervical lymph node metastasis, or American Joint Committee on Cancer (AJCC) 2002 tumor-node-metastasis (TNM) stage. (15).
Data are expressed as mean±SD or as number (percent). Classification of LN metastasis was based on the American Joint Committee on Cancer/Union for International Cancer Control Tumor–Node–Metastases (AJCC/UICC TNM) staging system (15).
WT, wild-type; N1a, cervical lymph node (LN) metastasis at level VI (i.e., pretracheal, paratracheal, or prelaryngeal/Delphian LN); N1b, metastasis defined as unilateral, bilateral, or contralateral cervical or superior mediastinal LNs.
XIAP expression and clinicopathological parameters in PTCs
XIAP expression was positive in 128 PTCs (78%) and negative in 36 PTCs (22%). XIAP immunostaining was evaluated semi-quantitatively, and 31 (19%), 81 (49%), and 27 (16%) of specimens were assigned intensity scores of 1+, 2+, and 3+ respectively (Table 2). Concerning the extent of the staining, 130 (82%) of 164 specimens were scored 2+ or 3+. A PTC sample was considered XIAP positive if the sums of the extent score and the intensity score was equal to or greater than four. There was a significant association between positive XIAP staining and BRAFV600E mutated PTC (p=0.048). As shown in Table 2, among 123 patients with the BRAFV600E mutation, 101 (82%) stained positive and 22 (18%) stained negative for XIAP.
Data are expressed as number (percent). p-Values were calculated using Fisher's exact test.
The intensity of XIAP staining was graded semi-quantitatively as follows: 0, negative; 1+, weak; 2+, moderate; 3+, strong.
The extent of XIAP staining was also graded semi-quantitatively as follows: 0, no foci; 1+, rare/few foci; 2+, multiple foci; 3+, regional/diffuse staining.
WT, wild-type; XIAP, X-linked inhibitor of apoptosis protein.
Clinical and pathological parameters were also analyzed according to XIAP expression status in the same study subjects (12). XIAP-positive PTC was not associated with age, sex, tumor size, multifocality, lymphovascular invasion, extrathyroidal extension, or AJCC TNM staging. However, the frequency of lateral cervical lymph node metastasis was significantly higher in patients with XIAP-negative tumors (31%) compared to those with XIAP-positive tumors (11%, p=0.01).
Prediction of recurrent PTC by BRAFV600E mutational status and XIAP expression
The median follow-up period of the study subjects was 11 years after initial treatment (range: 1–14 years), and recurrences were detected in 38 of 164 patients (23%). There was significantly more recurrence in patients with BRAFV600E -mutated PTC compared to patients with wild-type BRAF (p=0.030; Fig. 1A). In an unadjusted model, the HR for recurrence in BRAFV600E -mutated PTC was 2.98 compared to PTC with wild-type BRAF (p=0.039; Table 3, Model 1). However, further adjustment for age and sex attenuated the risk of recurrence (HR=2.72, p=0.06; Table 3, Model 2).
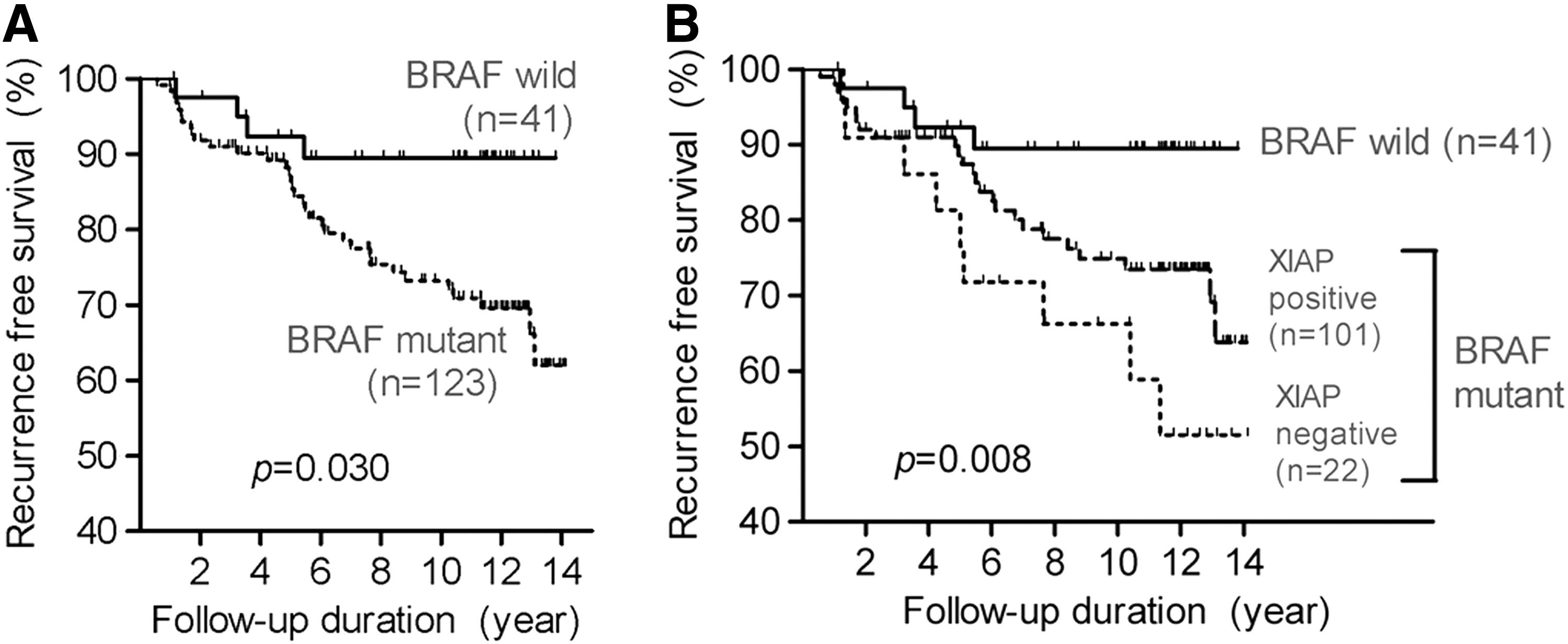
Recurrence-free survival according to BRAFV600E
mutational status
Values are unadjusted or adjusted hazard ratios (HRs) [95% confidence intervals (CIs)]. p-Values were calculated using the Cox proportional hazards model.
Model 1 was unadjusted. Model 2 was adjusted for age and sex. Model 3 was adjusted as for Model 2 with additional adjustments for tumor size, multifocality, and extrathyroidal extension. Model 4 was adjusted as for Model 3 and was also adjusted to include cervical lymph node metastasis.
Patients were next classified into three groups according to BRAFV600E mutational status and XIAP expression in the tumor. The first group contained BRAF wild-type PTCs (n=41), the second group contained BRAFV600E mutation-positive and XIAP-positive PTCs (n=101), and the third group contained BRAFV600E mutation-positive and XIAP-negative PTCs (n=22). The recurrence-free survival was significantly different between these three groups (p=0.008; Fig. 1B). The difference in recurrence-free survival between patients with BRAFV600E -positive, XIAP-positive PTC and those with BRAF wild-type PTC was borderline significant. However, there was significantly higher recurrence in patients with BRAFV600E -positive, XIAP-negative PTC (HR=4.53, p=0.012) compared to those with BRAF wild-type PTC (Table 3, Model 1). After adjustment for age, sex, tumor size, multifocality, and extrathyroidal invasion, a BRAFV600E mutation-positive and XIAP-negative PTC was significantly associated with recurrence compared to patients with a BRAF wild-type PTC (Table 3, Models 2 and 3). Further adjustment using cervical lymph node metastasis attenuated the risk of recurrence (Table 3, Model 4).
To clarify whether the cervical lymph node metastasis or XIAP negativity affects the risk of recurrence stronger in BRAFV600E mutant PTCs, multivariate analyses using the presence of cervical lymph node metastasis was performed (Table 4). The presence of lateral cervical lymph node metastasis (N1b) was a significant prognostic maker to predict recurrence of PTC in multivariate analysis (Models 2 and 3). As a comparison between Model 3 of Table 3 and Model 3 of Table 4, the presence of lateral cervical lymph node metastasis (N1b) was a stronger prognostic marker to predict recurrence (HR=12.17, p=0.001) than XIAP negativity (HR=3.97, p=0.029). However, the presence of central cervical lymph node metastasis (N1a) was not significant and was a weaker prognostic marker (HR=3.38, p=0.08) than XIAP negativity.
Values are unadjusted or adjusted HR [CI]. p-Values were calculated by using the Cox proportional hazards model.
Model 1 was unadjusted. Model 2 was adjusted for age and sex. Model 3 was adjusted as for Model 2 with additional adjustments for tumor size, multifocality, and extrathyroidal extension.
Discussion
XIAP is one of the IAP proteins, a family of signal transducers that perform a diverse array of functions, which impinge on many signaling pathways and elicit multiple cellular responses in the cells (10). XIAP binds and functionally inhibits caspase-3, -7, and -9 (16 –18). Abnormal expression of XIAP is reported in the pathology of many human cancers. However, only a few large-scale studies provide translational evidence of an association between XIAP expression and clinical outcomes (9,10,19 –21).
To our knowledge, this is the first study to evaluate the prognostic value of XIAP expression in combination with BRAFV600E mutational status in PTC. The BRAFV600E mutation is a promising prognostic biomarker for patients with PTC, as a number of previous studies have shown that it has a high predictive power in the prognosis of PTC (4 –6,13). This prognostic value may allow BRAFV600E mutational status to guide clinical decision making. However, the BRAFV600E mutation has limited value in clinical decision making in areas in which the BRAFV600E mutation is extremely prevalent, such as Korea. The present study was designed to evaluate whether XIAP expression has prognostic value when combined with BRAFV600E mutational status in PTC. Among patients with BRAFV600E -mutant PTC, 18% were negative for XIAP expression, and the HR for recurrent PTC was significantly increased in this subgroup of patients. Therefore, XIAP expression could be a novel biomarker to assist decision making in patients with BRAFV600E -mutant PTC during clinical follow-up after initial treatment.
In our previous study, we found that XIAP expression was higher in thyroid cancer, particularly in classical PTC, compared to benign thyroid nodules such as nodular hyperplasia and follicular adenoma (12). These findings are consistent with other studies, suggesting that XIAP contributes to tumor cell survival as an apoptosis inhibitor. The expression of XIAP was negatively associated with the risk of lateral neck lymph node metastasis in our study (12). There was also a significant correlation between BRAFV600E -mutated PTCs and increased XIAP expression. However, in Chinese patients, XIAP expression was positively associated with lymph node metastasis (22), and there was no correlation between BRAFV600E mutational status and XIAP expression (23). Differences in the prevalence of the BRAFV600E mutation and dietary iodine intake in the Korean and Chinese populations may explain this discrepancy. Dietary iodine intake in Korea is considerably higher than in China. Many Korean groups showed that the prevalence of the BRAFV600E mutation is very high (around 70–80%) in Korea compared to other parts of the world (13,24). It is possible that regional differences in dietary iodine intake and the prevalence of the BRAF mutation in PTC could explain this discrepancy regarding the association between XIAP expression and the clinical and molecular biological features of PTC. It is widely accepted that IHC staining of tissue for the quantification of target proteins is subject to a great deal of variability, both in the staining procedure and in the interpretation of the IHC results. Therefore, quality-control processes will be necessary before our results can be applied to clinical practice.
In the present study, PTCs with the BRAFV600E mutation had increased XIAP expression. The MAPK pathway (RAS→RAF→MEK→MAPK/ERK) plays a central role in the regulation of cell growth, division, and proliferation (25). BRAFV600E is the major cause of aberrant activation of the MAPK/ERK pathway in human cancers (26). The phosphoinositide-3 kinase (PI3K)/AKT signaling pathway also regulates various biological processes, such as cell proliferation, growth, and apoptosis (27). The RAS/RAF/ERK and the PI3K/AKT pathways interact on multiple levels (28), and some studies suggest that enhanced RAS/RAF/ERK signaling affects PI3K/AKT activation (29,30). However, the influence of XIAP on the PI3K/AKT or MAPK signaling pathways has not been completely elucidated. Recently, it was shown that AKT and RAF-1 could activate XIAP via phosphorylation of XIAP and inhibition of XIAP degradation (31,32). Therefore, the BRAFV600E mutation may result in XIAP activation through constitutive activation of MAPK and PI3K/AKT signaling pathways.
The anti-apoptotic activity of XIAP is regulated by SMAC/DIABLO (33), and this could be a possible explanation for the association between decreased XIAP expression and clinical recurrence and lateral lymph node metastasis in PTC. SMAC/DIABLO is normally localized to the mitochondria and released into the cytosol during the early stages of apoptosis, where it promotes caspase activity by inhibiting XIAP. Recent studies revealed that the relative proportion of XIAP to SMAC/DIABLO, rather than the absolute level of XIAP expression, may determine cancer cell survival (33,34). However, the present investigation focused on XIAP expression only. Therefore, follow-up studies are required to investigate the role of XIAP and SMAC/DIABLO in carcinogenesis and metastasis of PTC.
In conclusion, negative XIAP expression was significantly associated with lateral neck lymph node metastases in PTC. Patients with tumors positive for the BRAFV600E mutation and negative for XIAP expression had a significantly higher risk of recurrence. The evaluation of the XIAP expression by IHC in combination with BRAFV600E mutation analysis may be useful for the prediction of prognosis in PTC patients in BRAFV600E -prevalent areas.
Footnotes
Acknowledgment
This study was supported by the Research Grant Number NRF-2012R1A1A2038383 from the National Research Foundation (NRF) of Korea.
Author Disclosure Statement
The authors have no competing interests to disclose.