
Abstract
Background:
Energy-based hemostatic devices are increasingly being used in thyroid surgery. However, there are several limitations with regard to the existing evidence and a paucity of guidelines on the subject. The goal of this review is to employ the novel evidence synthesis technique of a network meta-analysis to assess the comparative effectiveness of surgical technologies in thyroid surgery and contribute to enhanced governance in the field of thyroid surgery.
Methods:
Articles published between January 2000 and June 2012 were identified from Embase, Medline, Cochrane Library, and PubMed databases. Randomized controlled trials of any size comparing the use of ultrasonic coagulation (harmonic scalpel) or Ligasure either head-to-head or against the “clamp-and-tie” technique were included. Two reviewers independently critically appraised and extracted the data from each study. The number of patients who experienced postoperative events was extracted in dichotomous format or continuous outcomes. Odds ratios were calculated by a Bayesian network meta-analysis, and metaregression was used for pair-wise comparisons. Indirect and direct comparisons were performed and inconsistency was assessed.
Results:
Thirty-five randomized controlled trials with 2856 patients were included. Ultrasonic coagulation ranked first (followed by Ligasure and then clamp-and-tie) with the lowest risk of postoperative hypoparathyroidism (odds ratio 1.43 [95% confidence interval (CI) 0.77–2.67] and 0.70 [CI 0.43–1.13], ultrasonic coagulation vs. Ligasure and ultrasonic coagulation vs. clamp-and-tie, respectively), least blood loss (−0.25 [CI −0.84 to −0.35] and −1.22 [CI −1.85 to −0.59]), and drain output (0.28 [CI −0.35 to −0.91] and −0.36 [CI −0.70 to −0.03]). From a health technology viewpoint, ultrasonic coagulation was associated with the shortest operative time (−0.66 [CI −1.17 to −0.14] and −1.29 [CI −1.59 to −1.00]) and hospital stay (−0.28 [CI −0.78 to 0.22] and −0.56 [CI −1.28 to 0.15]). The only exception occurs with the clinically important complication of recurrent laryngeal nerve paralysis, where the reverse trend applies (1.36 [CI 0.25–7.46] and 1.74 [CI 0.94–3.26]).
Conclusions:
The comparative effectiveness of ultrasonic coagulation in thyroid surgery outcomes seems superior to other techniques with the exception of recurrent laryngeal nerve injury. This network meta-analysis, one of a handful in a surgical field, offers preliminary and robust evidence to guide clinical decisions and policy makers to adopt safer thyroid operations.
Introduction
The initial “clamp-and-tie” technique, first standardized by Theodor Kocher in the 19th century, continues to the present era with several modifications, where surgeons apply ligatures, titanium vessel clips, or staples (3,4). With technological advancements, several new tools based on energy transmission (electricity and ultrasonic energy) have been introduced as techniques for hemostasis in thyroid surgery.
The two most widely used hemostatic tools are the ultrasound-based harmonic scalpel (Ethicon Endo-Surgery, Inc., Johnson & Johnson, Cincinnati, OH) and Ligasure system (Valleylab, Covidien, Boulder, CO). These work on the principles of delivering ultrasonic energy and the combination of pressure and energy to the vessel wall, respectively, to achieve hemostasis. As each hemostatic modality demonstrates several characteristics in terms of hemostatic efficacy and side effects, we aimed to assess all the available evidence comparing these technologies. This is particularly relevant in the field of thyroid surgery, where there is a paucity of guidelines and recommendations.
When there are several interventions available for the same condition, as is the case with hemostatic modalities in thyroid surgery, decisions about optimal care and policy making rely on evidence-based evaluation of the different interventions (5). In real practice, there is frequently a paucity of adequately powered randomized controlled trials (RCTs). By integrating the data derived from several RCTs, meta-analyses may be useful in identifying gaps and discrepancies in the existing randomized evidence and aid in the planning of future RCTs. However, traditional meta-analyses have several limitations (6). These include the inability to compare more than two interventions at one time and to calculate the relative efficacy of two (or more) interventions if they have not been directly compared in a trial (7).
A new and promising extension of meta-analysis, network meta-analysis, is becoming increasingly popular. Through the sophisticated modeling that it employs (which includes Bayesian approaches and specialized software), network meta-analysis overcomes many of the limitations of traditional meta-analysis (5,8). Network meta-analysis permits comparisons between interventions that have never been directly compared (indirect comparisons), thus allowing the comprehensive use of all available data (direct and indirect evidence). In this way, network meta-analysis not only achieves an improved precision for each comparison but also allows the ranking of many interventions for the same condition by estimating the probability of each treatment to be the best (9). This ranking is of particular importance for policy makers (6). Moreover, through the synthesis of indirect evidence, network meta-analysis can address certain biases, such as sponsorship bias, which is not possible to address in traditional meta-analysis (10,11). Sponsorship bias may be of particular relevance when comparing surgical technologies designed by different manufacturers. This study represents one of a handful of network meta-analyses in surgery.
Materials and Methods
Identification of studies
A literature search was performed using Embase, Medline, Cochrane Library, and PubMed databases on all RCTs published between January 1, 2000, and June 1, 2012, reporting on the different hemostatic instruments used in thyroid surgery (harmonic scalpel and Ligasure system) and comparing these to each other and/or to conventional clamp-and-tie thyroidectomy. Different combinations of expanded medical subject headings were used, as shown in Appendix A. The “related articles” function was used to broaden the search, and all abstracts, studies, and citations were reviewed. No language restrictions were made.
Study selection
The inclusion criteria for this network meta-analysis were RCTs of any size comparing the use of ultrasonic coagulation or the Ligasure system in thyroid surgery either against each other or against the traditional clamp-and-tie technique. They had to report on at least one of the outcome measures (mentioned below) and contain a previously unreported group. When two or more RCTs were reported by the same institution, either the one of better quality or the most recent publication was included in the analysis. Studies that were not randomized or prospective in their design were excluded from our analysis. Similarly, studies that used no controls or that used historical controls were excluded, as were studies in which the outcomes of interest (mentioned below) were not reported or it was impossible to calculate these from the published results. Finally, studies that involved patients not undergoing thyroid surgery or involved animal subjects were excluded. The PRISMA statement flow diagram illustrating the search strategy is shown in Figure 1.
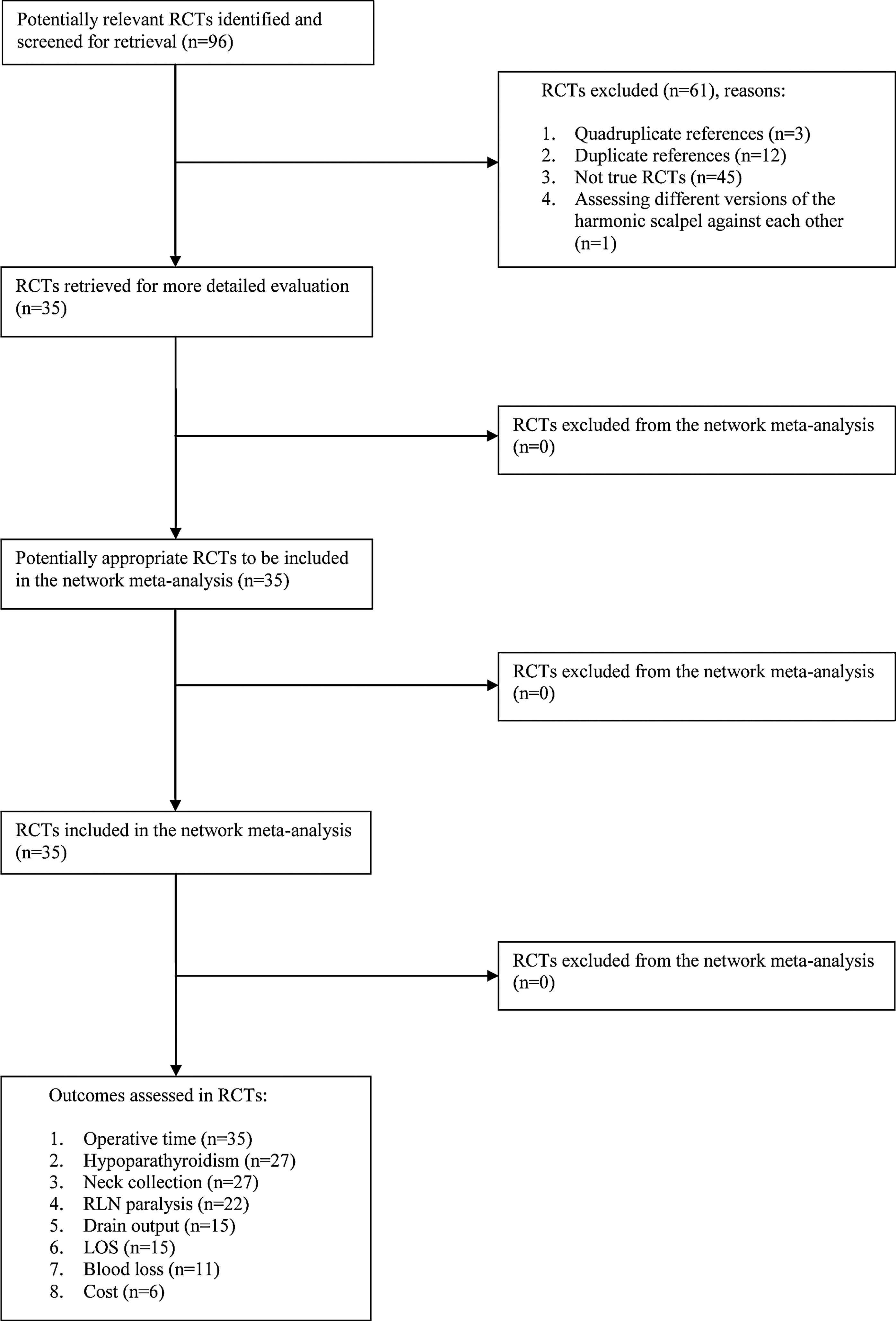
PRISMA statement flow diagram illustrating the search strategy used for the network meta-analysis.
Outcomes of interest
Given the low mortality after thyroidectomy and the importance of postoperative functional outcomes, we decided to use as primary endpoints the following functional outcomes: hypoparathyroidism and RLN paralysis (both permanent). Secondary endpoints were considered the following intraoperative outcomes such as operation time, blood loss, and postoperative outcomes such as drain output, neck collection, length of hospital stay (LOS), and cost.
Data extraction
Two reviewers (G.G. and H.A.) independently critically appraised and extracted the data from each study: first author, institution, country of origin, year of publication, study design, study population characteristics, hemostatic methods compared, number of subjects operated on with each technique, and outcome measures. We extracted the number of patients who experienced postoperative events in dichotomous format or continuous outcomes. Any discrepancies were resolved by consensus. Jadad scores were calculated for all included studies (12,13). Appraisal of all studies to determine their risk of bias was also performed using a recently introduced tool for evaluating the rigor of surgical RCTs, and a composite quality score was computed for each study taking into account the Jadad and risk-of-bias scores (14). A composite quality score of ≥3 was defined as a threshold of rigor (14). Again, any discrepancies were resolved by consensus. This study was written based on the PRISMA guidelines (15).
Statistical analysis
In all statistical methods used, differences in follow-up between different RCTs were controlled for by incorporating the length of follow-up as a variable in the regression analysis.
Pair-wise comparison
Effect sizes for pair-wise comparisons were calculated with the DerSimonian and Laird random effects methods (16). We calculated odds ratio (OR) for dichotomous data and standardized mean difference (SMD) with 95% confidence interval (CI). Statistical heterogeneity was evaluated using the I 2 statistic, where values above 50% are considered to represent high between-study heterogeneity, values of 25–50% as modest heterogeneity, and values below 25% are considered as low heterogeneity. To identify the source of heterogeneity, metaregression analyses were performed using study-specific variables, such as year of publication and the Jadad score.
Bayesian network meta-analysis
We performed a random-effects network meta-analysis applying a Bayesian framework using Markov chain Monte Carlo methods (17,18). This technique combines pair-wise and indirect evidence for any given pair of interventions (6). We utilized a vague prior in this analysis applying previously established models (17,18). Iteration number and the burn-in value were set to 20,000 and 100,000, respectively. We defined p-values less than 0.05 as significant and calculated the range of 95% credible intervals. We also estimated the ranking of each intervention for our outcomes of interest based on the surface under the cumulative ranking curve (SUCRA) (18,19) to quantify the efficacy of interventions in the network meta-analysis. SUCRA scores represent cumulative ranking probabilities so that an intervention that consistently ranks first when compared with other treatments will derive a SUCRA score of 1, and if it always ranks last it will derive a SUCRA score of 0.
We performed the network meta-analysis based on the assumption that our network maintains an equivalent coherence between direct and indirect evidence when considering the same outcomes. Incoherence was calculated using the difference of log odds ratio (log OR) or the difference in SMD between indirect and direct evidence whenever indirect evidence was available according to one common comparator. Our definition of incoherence was based on a CI that did not include the value 1. Bayesian framework meta-analyses were performed by WinBUGS 1.4 (MRC Biostatistics Unit, Cambridge, United Kingdom), while all other analyses were carried out by R version 2.15.2 (Bell Laboratories, Berkeley Heights, NJ).
Results
Overview of the studies included
An initial literature search performed using Embase, Medline, Cochrane Library, and PubMed databases with entrance of the Mesh search headings listed in Appendix A revealed 1020 articles. The abstracts were screened yielding a total of 96 potentially relevant publications that were retrieved for more detailed evaluation. After thorough assessment, 35 RCTs were filtered, which form the basis of our network meta-analysis, with a total number of 2856 patients (1 –4,8,20 –50). The characteristics of included studies are listed in Table 1. The median Jadad score was 2 (range 1–3). Of these, 24 compared ultrasonic coagulation with clamp-and-tie (1 –3,20 –24,26,28,29,31,33,34,36,37,40 –44,46 –48,50), 11 compared Ligasure with clamp-and-tie (1,4,23,25,27,30,32,35,39,40,49), and 5 compared ultrasonic coagulation with Ligasure (1,23,38,40,45). Of the 35 RCTs, 3 were sponsored by the manufacturers of the harmonic scalpel (Ethicon Endo-Surgery, Inc.) (22,33,42) and one by the manufacturer of Ligasure (Valleylab) (38). In the remainder, the authors did not report any conflicts of interest or sponsoring.
Individual score definitions are provided in Appendix B.
Pair-wise comparisons
The summary of effects sizes is demonstrated in Table 2. Pair-wise comparisons were identified in 27 studies identifying hypoparathyroidism (1 –4,20 –24,27 –30,32 –35,37,40 –42,44 –48,50), 22 on RLN paralysis (1,3,20,22 –24,26,28,29,31,32,36,39 –42,45 –50), 35 on operative time (1 –4,20 –51), 11 on blood loss (1,20 –22,24,28,29,40,42,44,48), 15 on drain output (1 –3,22,28,29,32,33,37,41,42,45,46,48,50), 27 on neck collection (2,4,20,22,23,26 –41,43,45,47 –50), 15 on LOS (3,20,21,23,27,29,30,32,37,39,41,45 –47,50), and 6 on cost (1,3,4,21,36,38). The comparison of ultrasonic coagulation with clamp-and-tie identified a significant difference in operation time (SMD −1.29 [CI−1.59 to −1.00], p<0.01), blood loss (SMD −1.22 [CI−1.85 to −0.59], p<0.01), and cost (SMD −0.57 [CI−1.07 to −0.07], p=0.03). The comparison of Ligasure with clamp-and-tie identified a significant difference in operation time (SMD −1.08 [CI−2.08 to −0.09], p=0.03), while there were no significant differences between harmonic scalpel and Ligasure. More than moderate heterogeneity between included studies was, however, observed in several pair-wise comparisons. To explore the source of heterogeneity, metaregression analyses were performed (Table 3). The year of publication was significantly associated with operation time in the comparison between Ligasure versus clamp-and-tie [coefficient 0.64 (0.02–1.26), p=0.04] and cost in the comparison between ultrasonic coagulation versus clamp-and-tie [coefficient 0.22 (0.12–0.31), p<0.01], while the Jadad score was significantly associated with blood loss [coefficient 1.00 (0.29–1.71), p=0.01] and drain output [coefficient 0.65 (0.07–1.24), p=0.03] in the comparison between ultrasonic coagulation versus clamp-and-tie, and LOS in the comparison between Ligasure versus clamp-and-tie [coefficient 2.56 (1.74–3.37), p<0.01].
The numbers following the group comparison in the left-hand column denote the number of pair-wise comparisons in the literature. Boldface denotes significance.
H, harmonic scalpel; C, clamp-and-tie; L, Ligasure; OR, odds ratio; CI, 95% confidence interval; RLN, recurrent laryngeal nerve; SMD, standardized mean difference; LOS, length of stay; NA, not assessed.
The numbers following the group comparison in the left-hand column denote the number of pair-wise comparisons in the literature. Boldface denotes significance. aNumerical values indicate coefficient (range) values.
Bayesian framework network meta-analysis
Bayesian framework network meta-analyses were applied for all our outcomes of interest (Table 4). The comparison of ultrasonic coagulation with clamp-and-tie revealed a significant difference in RLN paralysis (OR 1.93 [CI1.00−3.57], p=0.05) and operation time (SMD −1.41 [CI−1.84 to −0.97], p<0.01). The comparison of Ligasure with clamp-and-tie identified a significant difference in operation time (SMD −1.07 [CI−1.65 to −0.50], p<0.01), while there was no significant difference between the harmonic scalpel and Ligasure. Assessment of the coherence of synthesized effects sizes between direct and indirect comparisons was performed within a network loop of the three hemostatic devices, where we calculated the incoherence in each surgical outcome (Fig. 2). There was no significant incoherence in all surgical outcomes, indicating the adequacy of calculating synthesized effects sizes by the Bayesian framework network meta-analysis in all our outcomes of interest. To represent the ranking of each device on all our outcomes of interest, we constructed a heatmap representing the efficacy of surgical instruments on our outcomes of interest based on SUCRA scores.
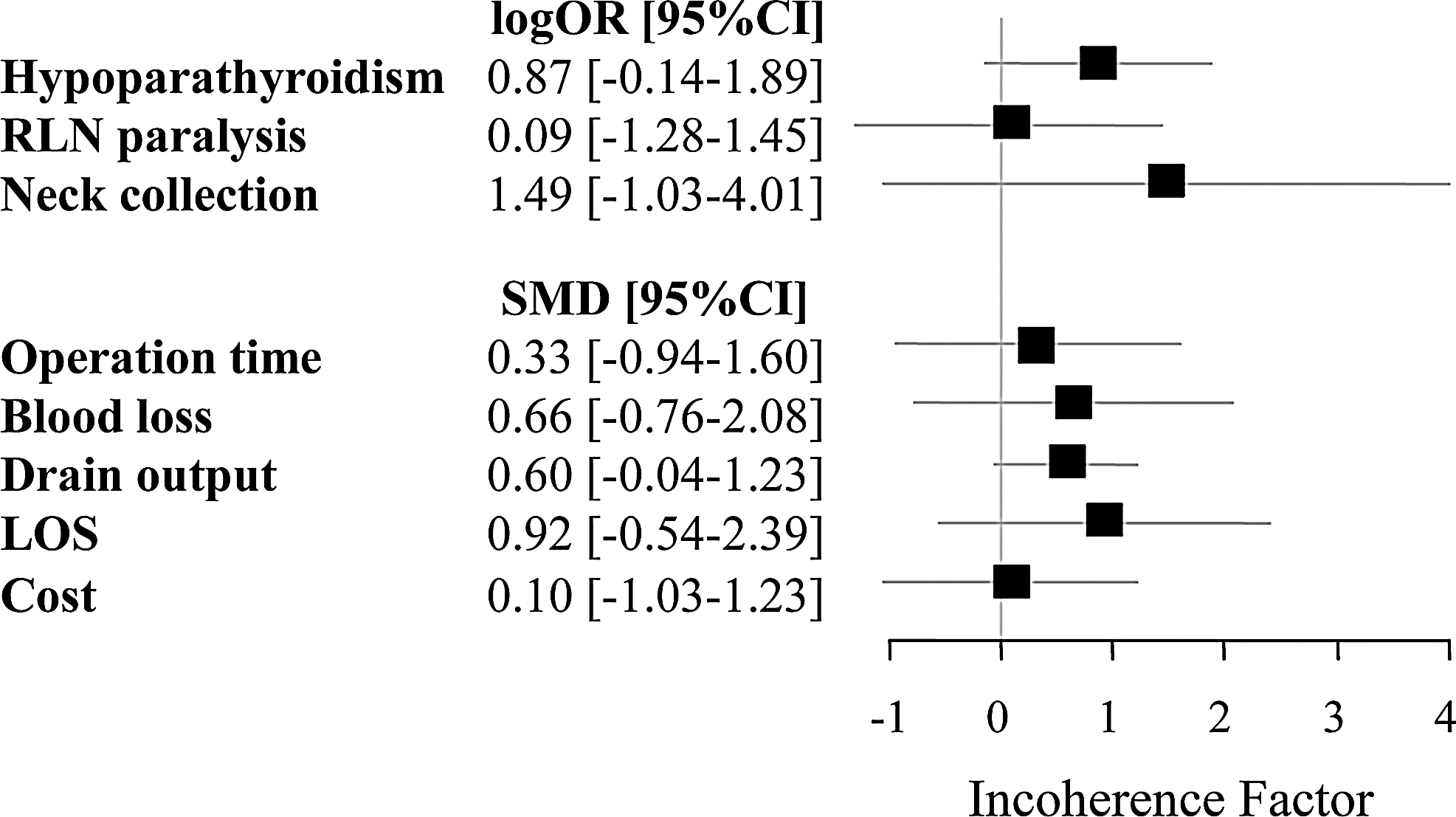
Forest plot illustrating calculation of incoherence in each surgical outcome. Assessment of the coherence of synthesized effects sizes between direct and indirect comparisons was performed within a network loop of the three hemostatic devices.
Boldface denotes significance.
As the year of publication and the Jadad score had a potential influence on some pair-wise comparisons, we evaluated the effect of these covariates on ORs calculated by Bayesian framework network meta-analyses using metaregression analyses (Table 5). The year of publication was significantly associated with operation time [coefficient −2.81 (−4.74 to 0.97), p<0.01], while the Jadad score was significantly associated with LOS [coefficient 0.42 (0.15–0.69), p<0.01].
Values in parentheses indicate ranges.
Discussion
This study demonstrates that there are significant differences in clinical outcomes between the hemostatic modalities in modern thyroid surgery. Between the three modalities available (ultrasonic coagulation, Ligasure, and clamp-and-tie), ultrasonic coagulation demonstrates the best profile in terms of the majority of clinical outcomes (operative time, hypoparathyroidism, blood loss, drain output, and cost), followed by Ligasure and then clamp-and-tie. Conversely, ultrasonic coagulation demonstrated the highest risk for RLN paralysis, whereas clamp-and-tie offered the lowest cumulative probability of this complication. For LOS and neck collection, ultrasonic coagulation again demonstrates the best profile but is then followed by clamp-and-tie and finally Ligasure. These results carry significant clinical implications and can contribute to healthcare decisions and policy to establish guidelines for thyroid surgery.
Despite a large volume of evidence on the use of hemostatic agents in thyroidectomy, there is an absence of guidance on comparative effectiveness for hemostatic modalities in thyroidectomy from the relevant international bodies or associations. This may reflect the high cost of these devices and the limitations associated with the published RCTs and their inclusion in meta-analyses. As a result, skepticism may be expressed regarding the objectivity and bias of thyroidectomy studies, and there are several reasons why the existing evidence is constrained and potentially biased. First, a significant proportion of the relevant RCTs have been sponsored by device manufacturers. Second, previous meta-analyses that have been published to date possess several limitations (52 –55). They are all based on small numbers of RCTs (52 –55), noninclusion of articles from the past 24 months, and data from nonrandomized studies (55). Others have been sponsored by the manufacturer of the harmonic scalpel (53) or the authors have failed to disclose competing interests (54). Third, they have restricted their search strategy to English or German articles (53). Our study aimed to minimize some of these biases by incorporating the data from 29 RCTs published in English (1 –4,20,22,25,26,28,29,33,34,36 –50), 4 in Italian (23,24,31,32), 1 in French (21), and 1 in German (35). Finally, the main setback of these meta-analyses is that they have focused on pair-wise, direct comparisons of these hemostatic devices against each other or the clamp-and-tie technique. As a matter of fact, this represents the main limitation of (conventional) meta-analyses in general (9). Conventional meta-analyses are restricted to addressing only one intervention (pair-wise) comparison for one outcome, which can lead to a constrained view of the evidence (9), thus limiting the ability of identifying or ranking the best treatments (5). To overcome the limitations of pair-wise comparisons, we used the most robust evidence synthesis technique to conduct a multiple treatments comparison meta-analysis (also known as a network meta-analysis). We used Bayesian statistics to calculate the ranked probabilities of best outcomes for each hemostatic modality (5). Bayesian statistics were used because they make it easier to account for correlations induced by multi-arm trials, and the estimation of predictive intervals and ranking probabilities is comparatively clear-cut (see Materials and Methods) (56).
In our network meta-analysis, for the majority of the outcomes assessed, ultrasonic coagulation was consistently ranked first, with Ligasure second and clamp-and-tie third best. There were three exceptions, however: those relating to RLN paralysis, neck collection, and the LOS. A summary of these rankings on outcomes of interest among ultrasonic coagulation, Ligasure, and clamp-and-tie is presented in the form of a heatmap as the surface under the cumulative step function (SUCRA) in Figure 3. SUCRA=1 corresponds to an intervention that always ranks first and SUCRA=0 to an intervention that always ranks last. This ranking is extremely valuable for policy makers.
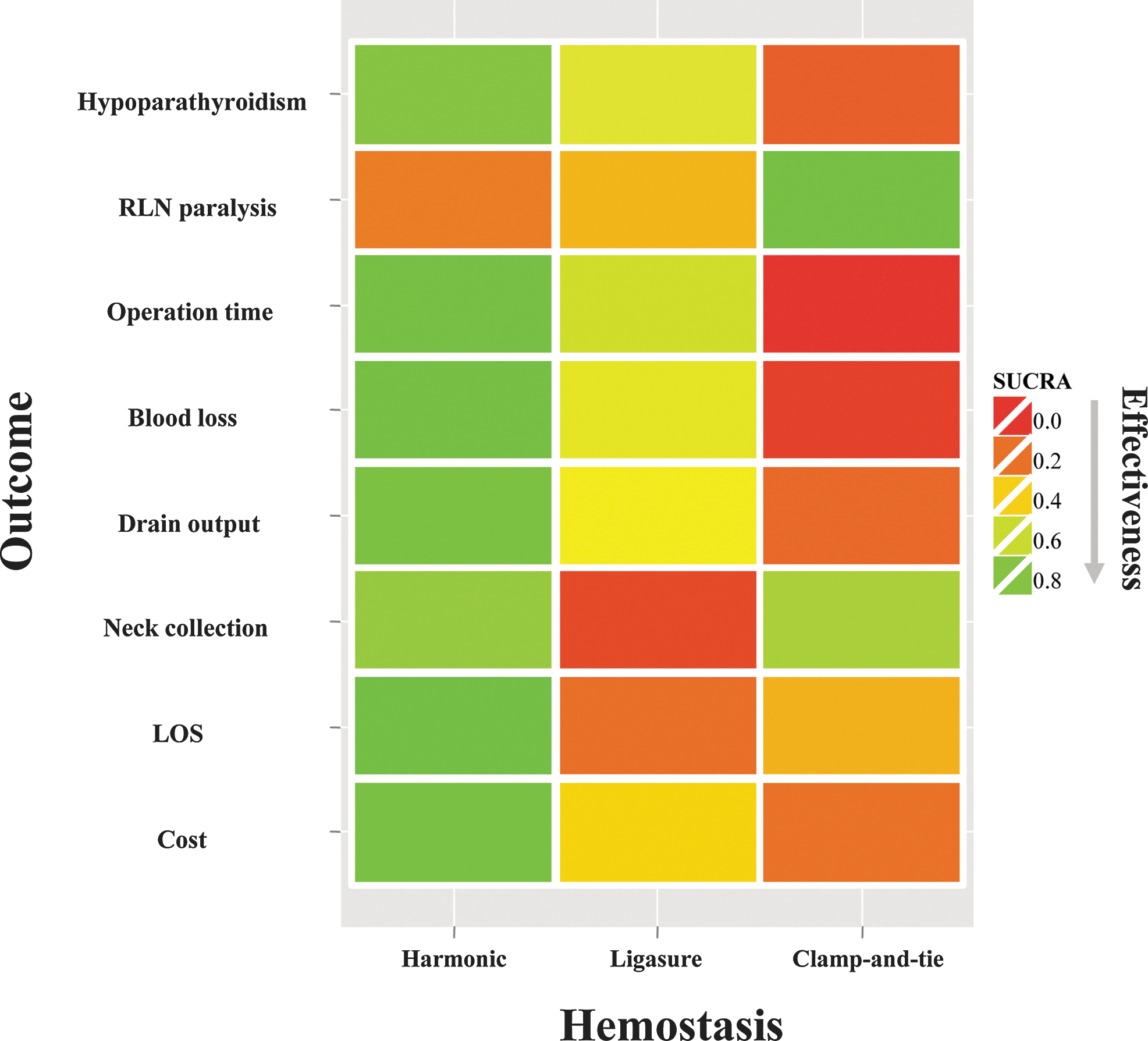
Ranking of hemostatic devices on all outcomes of interest represented in the form of a heatmap as the surface under the cumulative ranking curve (SUCRA). The heatmap represents the efficacy of surgical devices on all outcomes of interest based on SUCRA scores. SUCRA=1 corresponds to an intervention that always ranks first and SUCRA=0 to an intervention that always ranks last. Similarly, green represents the best device and red represents the worst for each individual outcome in a qualitative approach. Color images available online at
With regard to hypoparathyroidism (permanent), this was shown to be much less prevalent postoperatively when using ultrasonic coagulation compared with both Ligasure and clamp-and-tie. These effects on the parathyroid glands may be explained by the physics underpinning the functioning of these instruments (22), as the temperatures reached by ultrasonic coagulation are significantly lower (50–100°C) than those reached by bipolar electrocoagulation (150–400°C) (44). Moreover, the lateral thermal spread of ultrasonic coagulation (1–3 mm wide) is approximately half that of bipolar systems (42). In terms of RLN paralysis (permanent), our network meta-analysis conversely demonstrated clamp-and-tie to be the safest hemostatic modality followed by Ligasure and then ultrasonic coagulation. RCTs reporting RLN paralysis were only included in the network meta-analysis when RLN function was objectively assessed with pre- and postoperative laryngoscopy. RLNs are larger structures with a more predictable anatomic position than the parathyroid glands, making it easier to identify and preserve them (by avoiding using any heat-delivering device when in proximity). The concept of RLN injury following thyroid surgery is of particular importance as it constitutes the number one cause of malpractice litigation in thyroid surgery (57,58). Despite national guidelines for the RLNs in thyroid surgery (59)—both in the United States (60) and United Kingdom (61)—these mainly focus on the use of intraoperative nerve monitoring (62). There are no accepted policies on the use of hemostatic modalities to prevent RLN injury. The results of this network meta-analysis suggest that the superior safety profile of the clamp-and-tie technique can contribute to future international thyroidectomy guidelines.
This network meta-analysis demonstrated ultrasonic coagulation to be the most time-efficient hemostatic device in thyroid surgery. When ultrasonic coagulation and Ligasure were compared against each other with regard to operative time (both directly and indirectly), there was a trend favoring ultrasonic coagulation though the results were not shown to be statistically significant. The faster trend associated with ultrasonic coagulation compared with Ligasure can be explained by the fact that ultrasonic coagulation allows simultaneous sealing and division of vessels, while Ligasure only seals vessels that have to be subsequently cut with scissors after withdrawal of the device (20,63). This adds to the operative time and accounts for Ligasure being slower than ultrasonic coagulation. More recently, a newer version of Ligasure (Ligasure™ LF1212A) has been developed with an integrated cutting blade into the instrument, which overcomes this limitation with the one RCT assessing this new modification, revealing no significant difference between the modified Ligasure and ultrasonic coagulation on thyroidectomy operative times (45).
This important advantage that both ultrasonic coagulation and Ligasure possess over clamp-and-tie with regard to the significantly reduced operative time outweighs their significantly increased costs. Both the harmonic scalpel and Ligasure are non-reusable devices (64) [Harmonic: $255 (42) and Ligasure: $387 (4)] that operate with an electrical supply derived through a reusable generator [Harmonic: $21,698 (42) and Ligasure: $15,000 (4)]. Despite these financial overheads, this network meta-analysis demonstrated that ultrasonic coagulation may be the most cost-effective hemostatic tool for thyroid surgery (followed by Ligasure and then clamp-and-tie) in view of the reduced operative time and LOS it is associated with. A formal cost-effectiveness analysis may be more accurate to assess cost effectiveness.
As evident from the SUCRA heatmap, the trend for blood loss and drain output closely followed that for operative time (i.e., ultrasonic coagulation superior, followed by Ligasure and then clamp-and-tie). This is not surprising, as decreased operative field blood can lead to easier identification of fine and delicate structures such as the RLNs and parathyroid glands, making surgery faster but, more importantly, safer. Similarly, ultrasonic coagulation was the hemostatic device with the smallest risk of developing a neck collection (followed by clamp-and-tie and then Ligasure), further reinforcing its safety profile.
This network meta-analysis carries some limitations that require consideration before the results can be applied into clinical practice. Our analysis was based on the assumption that all the data were similar enough to be analyzed together or that their dissimilarity could be accounted for during the analysis (9). To deal with this limitation, we assessed RCT similarity by examining for heterogeneity among all included RCTs. We did so by performing a subgroup analysis and metaregression not only to assess, but also to improve, the similarity among RCTs before performing (adjusted) indirect comparisons (65).
Moreover, because the surgical technology developed by competing companies is evolving constantly to improve the performance of the device, the applicability of the data using older generations of instruments may be limited. To address this limitation and take into account the technological evolution of the devices, we made relevant adjustments for year when calculating ORs in both metaregression analyses for pair-wise comparisons (direct comparisons) and the Bayesian framework network meta-analysis (indirect comparisons). These year-adjusted models allowed assessment of the impact that year had on each outcome of interest.
Another limitation relates to the presence of incoherence. This refers to the situation where the results from the indirect comparisons contradicted those of the direct comparisons. Although direct comparisons are usually more reliable (9,66,67), this is by no means always the case (9,11,68,69). Through the use of treatment networks, confounding factors (e.g., sponsor agendas) were revealed and eliminated, leading to an increase in the objectivity of the evidence synthesized from our network meta-analysis. Nevertheless, given the retrospective nature of meta-analysis (including network meta-analysis), it is impossible to exclude the presence of publication bias or other sources of selective reporting bias from our study. However, the very nature of network meta-analysis and the complex statistical techniques it employs is aiming to do exactly that—that is, limiting all these biases significantly, more so than pair-wise meta-analytic techniques (70).
Furthermore, it was impossible to derive from the included RCTs any information about the completeness of oncologic resection for cancer cases to allow comparison of this outcome for the different hemostatic devices. This would have required comparative post-total thyroidectomy measurements of thyroglobulin and/or radioactive iodine scan findings. Finally, it is imperative to emphasize that the most important influence on outcome in thyroid surgery is the experience and volume of the surgeon (71,72); this has not been directly taken into account as RCTs did not have as a criterion for entering surgical experience or surgical volume.
This study illustrates significant differences between the technological tools available to facilitate thyroid surgery. Through the use of sophisticated statistical methodology, this network meta-analysis has allowed the objective, quantitative integration of both direct and indirect evidence for comparing hemostatic technologies in thyroid surgery. It is important to reiterate here that none of the authors has any conflict of interest making our evidence synthesis and interpretation of results impartial. Guidelines based on this network meta-analysis can contribute to enhanced governance in the field of thyroid surgery. This would result from the methodological robustness of this evidence synthesis, combined with a high-precision analysis and the consistency and directness of the evidence (73 –75).
Ultrasonic coagulation seems to possess certain advantages over Ligasure and clamp-and-tie. Ultrasonic coagulation was associated with the lowest risk of postoperative hypoparathyroidism, least blood loss and drain output, and, from a health technology assessment viewpoint, with the shortest operative time and hospital stay. In the ranking scale, Ligasure follows ultrasonic coagulation as second, with clamp-and-tie third. The only exception occurs with the clinically important complication of RLN paralysis, where the reverse trend applies. Surgeon experience and volume remain the most important determinators of outcome in thyroid surgery irrespective of the hemostatic method used.
These results offer clinically important implications on worldwide surgical decisions, policy making, and guideline formation with regard to the use of hemostatic devices in thyroid surgery. The comparative cost effectiveness of each device will, however, require formal cost-effectiveness studies. Our results fulfill a global need as there are no current national or international guidelines regarding the application of hemostatic agents in thyroid surgery.
Dedication
This article is dedicated to the memory of Professor Ioannis Garas, MD, PhD.
Footnotes
Author Disclosure Statement
No funding or sponsoring was received for this study, and none of the authors have any conflicting interests to report.
Appendix A. Mesh Search Headings Used
“Ligation” AND “Thyroidectomy” (52 studies), “Electrocoagulation” AND “Thyroidectomy” (37 studies), “Diathermy” AND “Thyroidectomy” (33 studies), “Haemostasis” AND “Thyroidectomy” (111 studies), “Haemorrhage” AND “Thyroidectomy” (244 studies), “Blood Loss, Surgical” AND “Thyroidectomy” (56 studies), “Postoperative Haemorrhage” AND “Thyroidectomy” (42 studies), “Hematoma” AND “Thyroidectomy” (63 studies), “Hypocalcemia” AND “Haemostasis, Surgical” AND “Thyroidectomy” (11 studies), “Hypoparathyroidism” AND “Haemostasis, Surgical” AND “Thyroidectomy” (5 studies), “Surgical Procedures, Minimally Invasive” AND “Haemostasis, Surgical” AND “Thyroidectomy” (6 studies), “Laryngeal Nerves” OR “Recurrent Laryngeal Nerve” OR “Vocal Cord Paralysis” AND “Haemostasis, Surgical” AND “Thyroidectomy” (3 studies), “Drainage” OR “Suction” AND “Thyroidectomy” (96 studies), “Pain Measurement” AND “Thyroidectomy” (30 studies). Searches were also performed under the terms “harmonic scalpel AND thyroidectomy” (53 studies), “Ligasure AND thyroidectomy” (53 studies), and “Clamp-and-tie AND thyroidectomy” (13 studies).