
Abstract
Background:
The forkhead transcription factor FoxP3 plays an important role in regulatory T cell (Treg) functions. Tregs are critical in maintaining immunologic tolerance. It has been shown that vaccination against FoxP3-expressing cells is associated with enhancement of tumor immunity. Tregs appear to be increased in blood and in the tumor microenvironment of patients with different cancer types. Tumor cells themselves can express FoxP3. The present study investigates the possible role of FoxP3 expression in a series of human papillary thyroid cancers with a mean follow-up time of 15 years.
Methods:
One hundred five cases of papillary thyroid carcinoma (PTC) were investigated, and FoxP3 expression was evaluated in both tumor cells and tumor-associated infiltrates. For all patients, clinical/pathologic features were considered and the results analyzed by statistical tests.
Results:
Of the 105 PTC cases, 45 (43%) scored FoxP3-positive and 60 (57%) were negative. FoxP3 staining was localized predominantly in the cytoplasm of tumor cells. In some cases, both nuclear and cytoplasmic staining was seen in infiltrating cells. FoxP3 expression in tumor cells was correlated with the presence of extrathyroid invasion (p=0.04) and distant metastasis (p=0.04), but not with overall survival. Interestingly, FoxP3 expression in neoplastic cells was significantly associated with a resistance phenotype to radioiodine treatment (p=0.041).
Conclusions:
The data show an association of FoxP3 expression with features of PTC that seem to have a specific impact on radioiodine sensitivity.
Introduction
F
A strong correlation has been demonstrated between papillary thyroid cancer (PTC) and inflammatory infiltration, particularly infiltration of lymphocytes, macrophages, and dendritic cells. It is also known that thyroid autoimmunity is associated with a higher than normal incidence of PTC (19 –22). Recent results of our group indicate that expression of CXCR4 together with the BRAF mutation status is associated with more aggressive PTC phenotypes and with an enhanced spread of tumor cells outside the thyroid capsule (23). In the present study, we investigated 105 consecutive PTC cases (mean follow-up time of 15 years) to assess the possible prognostic value of FoxP3 expression in epithelial thyroid cells.
Patients and Methods
Study group and clinicopathological features
The study included 105 patients who underwent total thyroidectomy at the Department of Surgery of the University of Pisa, Italy, from 1985 to 1992. A presurgical cytological diagnosis of PTC was available for all patients. The clinical follow-up of patients was performed at the Department of Endocrinology, University of Pisa. Institutional approval from the local Ethics Committee was obtained for this study. Surviving patients gave written informed consent to the use of their tissue specimens for present and future investigations.
Hematoxylin-eosin–stained sections of 105 patients from the archives of the section of Pathology of the University of Pisa were re-evaluated independently by two pathologists (CU, FB). A diagnostic concordance rate of 98% was achieved between the two investigators. Rare discordant cases were discussed with a third pathologist (AP). Tumors were reclassified according to the World Health Organization 2004 histopathological criteria (24). Histopathological re-evaluation at the time of diagnosis included, whenever possible, histotype, presence of capsule infiltrating tumor cells, infiltration of extrathyroidal tissue, and the presence and number of metastatic lymph nodes.
For the majority of patients (not for all) clinical/pathologic parameters were also re-evaluated (i.e., age, sex, tumor size, development of node metastasis, detection of distant metastases, number of doses and total dose [mCi] of radioiodine administered). Clinical/pathologic features are summarized in Table 1.
Clinical outcome
At the time of the study, 105 PTC patients had a mean follow-up period of 15 years (range 1 to 24 years; median±SD, 18±6.18). In agreement with current guidelines for the diagnosis and management of thyroid cancer (25,26), patients were considered cured when neck ultrasound plus whole-body scans gave negative results, and when serum thyroglobulin and anti-thyroglobulin antibodies were undetectable after thyroid hormone withdrawal or after thyrotropin stimulation. Patients who died of causes unrelated to PTC were considered cured or not cured according to the clinical status at the time of death.
At the end of the study, 86 of 105 patients (81.9%) were cured. In contrast, 19 of 105 patients (18.1%) had persistent disease. Of these, 7 of 19 (36.8%) died of metastatic PTC.
As a standard procedure, all patients were treated with one or more doses of 131I (30–100 mCi per dose) to ablate postsurgical thyroid remnants. When required, cumulative amounts up to 1120 mCi 131I were used.
Staining for FoxP3
Immunohistochemical analysis of FoxP3 expression was performed on formalin-fixed, paraffin-embedded tumor sections using mouse monoclonal anti-human FoxP3 antibody (ab22510; Abcam, Cambridge, United Kingdom). Sections were stained using the Ventana automated slide stainer (Ventana Medical Systems, Tucson, AZ).
Expression of FoxP3 in epithelial tumor cells and lymphocytes was evaluated independently by two investigators (CU and FB) who were blinded to clinical-pathologic data. Discrepancies between the two observers were discussed with a third pathologist (AP). Cytoplasmic staining of ≥25% tumor cells was considered positive. The possible association of FoxP3 expression with clinical/pathologic features, BRAF status, and survival data were investigated by statistical analysis.
Moreover the authors evaluated the presence of FoxP3 expression in T lymphocytes collateral to the tumor, scoring as positive or negative in 10 high power fields. The intensity of the staining was evaluated as weak and strong.
As a control thyroid tissue from 20 normal glands underwent surgery for head and neck tumors was stained. All the cases were negative for FoxP3 stain.
BRAF mutational analysis
BRAF analysis was conducted in 74 cases of 105. Excluded cases were inadequate for mutational analysis because these were old specimens (before 1990) that were fixed in an inappropriate fixative.
In the samples amenable to analysis, detection of a BRAF mutation was performed by polymerase chain reaction single strand conformation polymorphism (PCR-SSCP) and direct DNA sequencing. PCR-SSCP screening of BRAF mutations was performed by amplifying exon 15 according to a standard procedure. DNA was used as a template in a 20 μL PCR mixture containing 10 mM Tris-HCl, 50 mM KCl, 1.5 mM MgCl2 (pH 8.3), 0.2 mM dNTPs, 8 pmol of amplimers, and 1.25 U of AmpliTaq Gold DNA Polymerase (Applied Biosystems, Foster City, CA). PCR primers for the BRAF exon 15 were as follows: 5′(F)-TCC TTT ACT TAC TAC ACC TCA GAT-3′ and 5′(R)-AGT GGA AAA ATA GCC TCA AT-3′. The amplicon size was 167 bp. Cycling conditions were as follows: initial denaturation (94°C, 5 minutes), then 35 cycles (denaturation, 94°C for 40 seconds; annealing, 55°C for 40 seconds; synthesis, 72°C for 40 seconds), followed by a final extension of 5 minutes at 72°C. All PCR products were visualized by electrophoresis in 2% agarose gels and purified using a PCR purification kit (Qiagen, Crawley, West Sussex, United Kingdom). Purified products were then diluted 1:1 with denaturing solution (1% xylene cyanol, 1% bromophenol blue, 0.1 mM EDTA, and 99% formamide), boiled for 5 minutes and immediately placed in ice to prevent the annealing of single-strand products. SSCP screening was carried out on the GenePhor Electrophoresis Unit using GeneGel Excel 12.5/24 (12.5% T, 2% C), according to manufacturer's instructions (GE Healthcare, Milano, Italy). Electrophoresis (600 V, 25 mA, 15 W) was performed at 18°C for 100 minutes. Gels were stained with PlusOne Silver Staining Kit (GE Healthcare), according to the manufacturer's instructions. Altered migration patterns in two or three independent PCR-SSCP runs were indicative of DNA mutations. Purified PCR products were then sequenced by a 3130 Genetic Analyzer (Applied Biosystem) automated sequencer using the Big Dye Terminator 3.1 (Applied Biosystem). DNA sequences were compared with the wild type exon 15 of the BRAF gene by using the Basic Alignment Search Tool (BLAST) software available at the National Center for Biotechnology Information.
Statistical methods
Overall survival (OS) was defined as the time elapsed from the date of surgery to the date of death or the date of the last follow-up. The disease-free survival (DFS) time was defined as the time elapsed from the date of surgery to the date of local recurrence or metastasis. The chi-square test was used to analyze the correlation of clinical and pathological data with FoxP3 expression. The population survival curve from a sample was analyzed with Kaplan–Meier analysis. Statistical significance was assessed using the log-rank test. The Statistica 6.0 software (StatSoft, Inc. Tulsa, OK) was used, and p values <0.05 were considered statistically significant.
Results
Expression of FoxP3 in PTC cells and infiltrating lymphoid cells
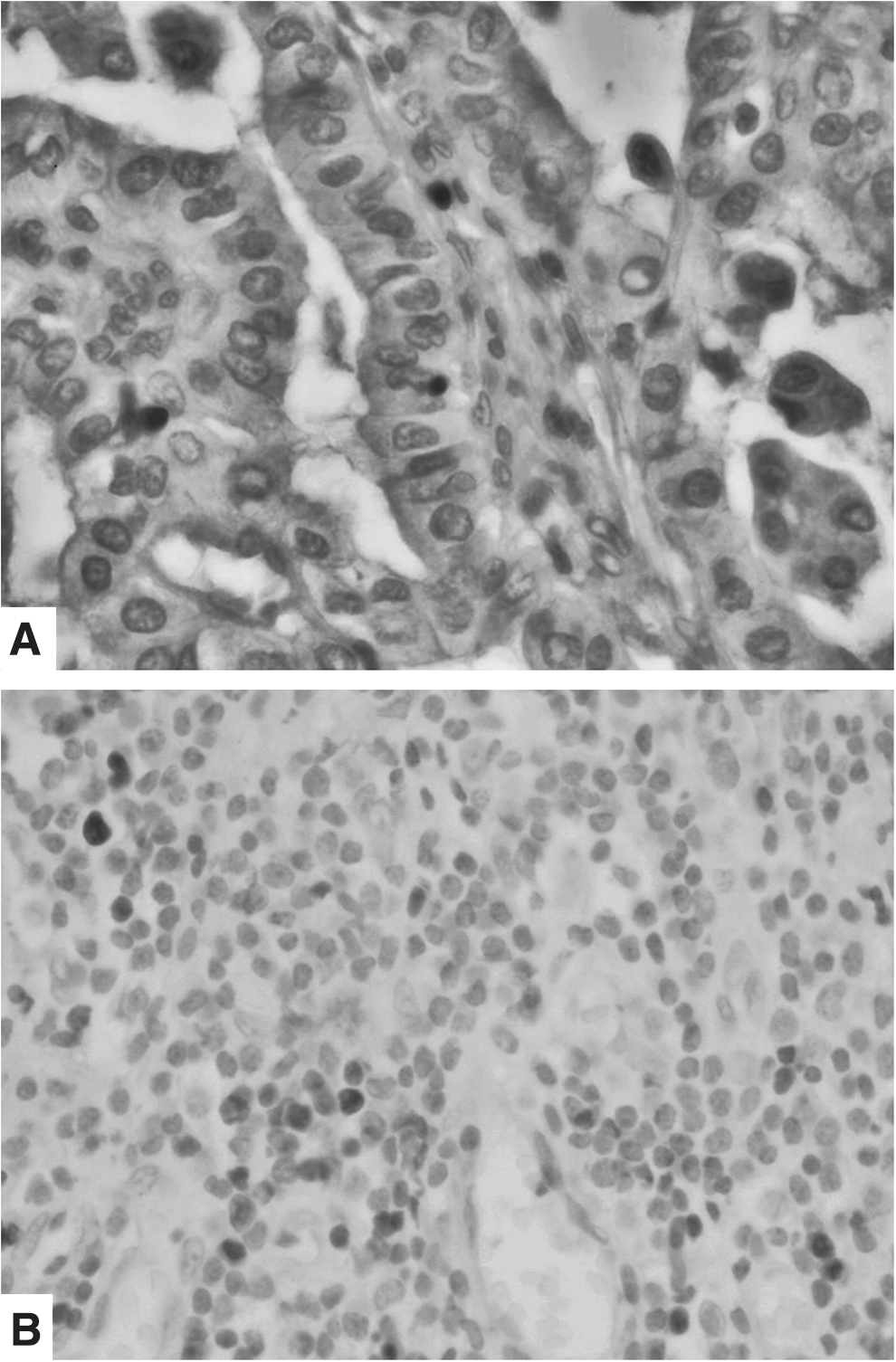
Among the tumor specimens that were immunostained for FoxP3, 45 of 105 (42.9%) scored positive, whereas 60 of 105 (57.1%) were negative. FoxP3 staining was localized predominantly in the cytoplasm of tumor cells. In a few specimens, both cytoplasmic and nuclear staining was observed. The intensity of staining was weak for all samples, with the exception of sporadic infiltrating cells. Of 105 tumor specimens immunostained for FOXP3, 29 (28%) were scored as positive in lymphocytes collateral to the tumors, and 76 (72%) as negative (Fig. 1A, 1B).
Expression of FoxP3 in epithelial cells of tall cell papillary thyroid carcinoma
Expression of FoxP3 and clinical/pathologic data
As shown in Table 2, the correlation of FoxP3 expression with clinical/pathologic characteristics was significant only for the presence of extrathyroid invasion (p=0.04) and the presence of distant metastasis (p=0.04). No significant association was observed among FOXP3 expression in lymphocytes and clinico-pathological features analyzed.
NS, not significant.
No association was detected between FoxP3 expression and age, sex, tumor size, presence of tumor capsule, multifocality, lymph node metastasis, or histotype.
Comparing the survival patient cohort with the clinical/pathologic characteristics (Table 3), only one feature was significantly correlated with poor survival rates: presence of extrathyroid invasion (p=0.03). Other parameters were not significantly correlated.
Expression of FoxP3 and overall survival time and disease-free survival time
No correlation was found between expression of FoxP3 and OS or DFS. Similarly, FoxP3 positivity scores failed to correlate with OS or DFS. Moreover, no correlation was found between the FOXP3 expression in lymphocytes and OS and DFS or with radioactive iodine therapy.
Expression of FoxP3 and radioiodine therapy
As shown in Fig. 2A, expression of FoxP3 in PTC cells was significantly associated with the total dose of 131I that had been used for each case (p=0.041), not with the number of doses administered to each patient (p>0.1; Table 2). No significant correlation was detected between expression of FoxP3 in infiltrating lymphoid cells and the total dose of 131I used for each patient (Fig. 2B).
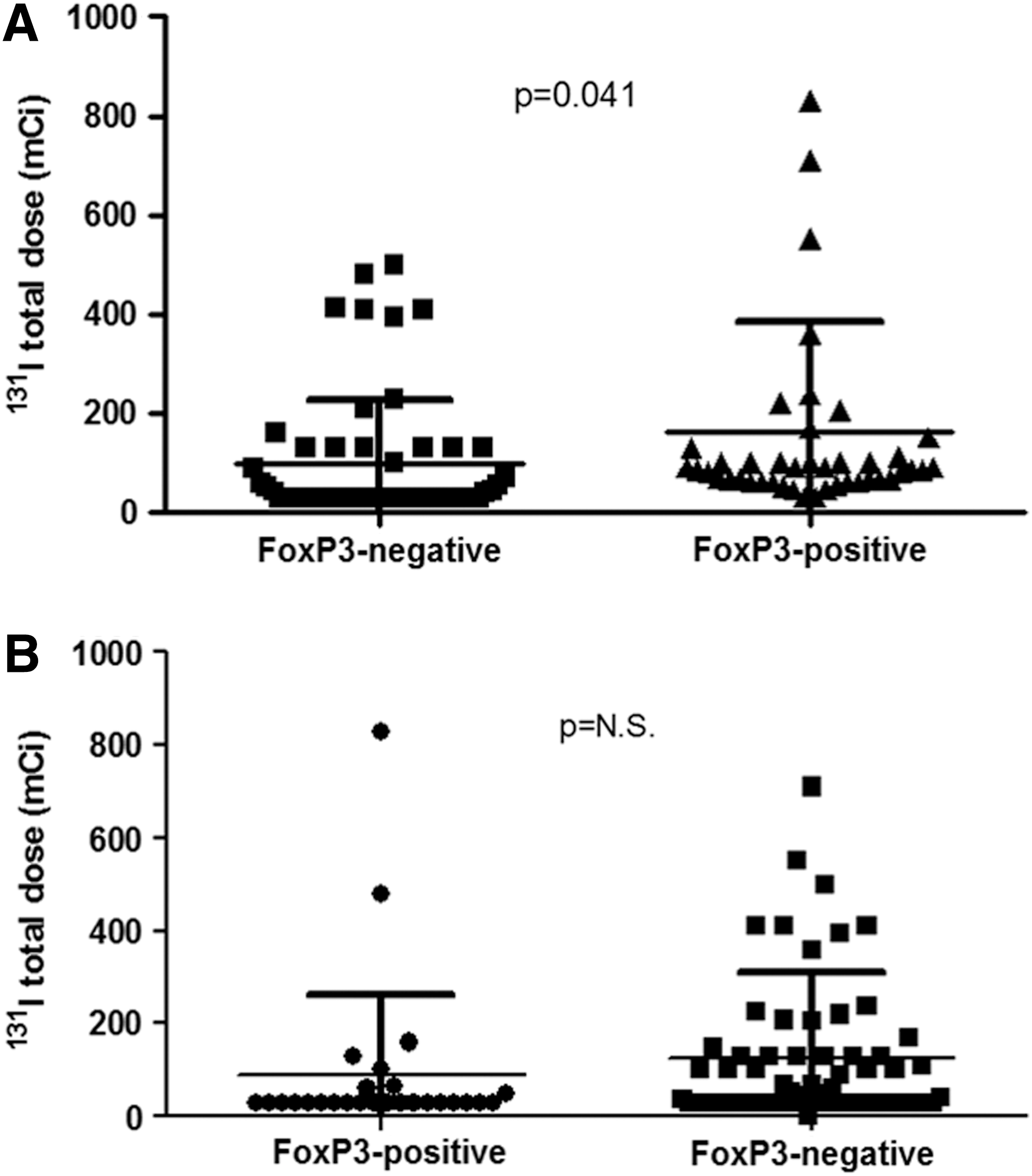
Expression of FoxP3 in papillary thyroid carcinoma cells was significantly associated with the cumulative dose of 131I that had been used for each case
Expression of FoxP3 and BRAF status
Forty-four (62%) of the 72 cases analyzed were wild-type for BRAF and 27 (38%) harbored the V600E mutation. No correlation was found between expression and positivity of FoxP3 and BRAF status.
Discussion
In general, PTC has a good prognosis with high survival rates and a high cure rate. Only 10%–15% of cases are not cured by combined surgical and radioiodine treatments. The latter cases usually require more aggressive treatments that often fail to reach a definitive cure (27).
In this study, clinical/pathologic and prognostic features of a large series of cases were correlated with FoxP3 expression in tumor and infiltrating cells as a potential prognostic biomarker. Recently, FoxP3 expression, both in epithelial tumor cells and in collateral lymphocytes, has been correlated with the outcome of a variety of tumors. Hinz et al. (10) suggested that FoxP3 expression in epithelial pancreatic cancer cells could represent an example of molecular mimicry and could reveal a hidden mechanism of immune evasion by cancer cells. However, the function of FoxP3 in tumor cells could be extremely subtle since it has been reported that FoxP3 may down-regulate intracellular PDE3B (cyclic nucleotide phosphodiesterase 3B) in Tregs (28). PDE3B, in turn, is associated with the increased expression of metabolic fitness genes, better survival, and reduced apoptosis of tumor cells (29). Merlo et al. (12) reported that FoxP3 expression in breast cancer is associated with the survival rate, but not with local relapse. They hypothesized that expression of this marker was related to metastatic potential, not only to the suppression of the local immune response. Thus, FoxP3 was believed to influence the development of distant metastasis in breast cancer. In thyroid cancer, detection of infiltrating Tregs correlates with aggressive disease. Patients with tumor-associated lymphocytes (particularly FoxP3-positive cells in tumor-involved lymph nodes) exhibit disease progression and increased incidence of invasion and metastasis (30).
FoxP3 binds to the transcriptional start site of the chemokine receptors CXCR4 and CCR7 (31). CCR7 is a critical signal that determines T cell exit from peripheral tissue and is supposed to play a role in cancer invasion and metastasis (32). The CXCR4 receptor and its ligand CXCL12 are expressed widely in human cancers. Both are associated with disease progression at the levels of tumor cell proliferation, invasion, and angiogenesis. Righi et al. (33) showed that therapy with a selective CXCR4 antagonist in ovarian cancer resulted in increased tumor apoptosis and necrosis, reduction in intraperitoneal dissemination, and selective reduction of tumor-infiltrating FoxP3-positive T cells.
Recent evidence indicates that interactions between chemokine receptors and their ligands may also have critical roles in the development of PTC, including stimulating growth, progression, and metastasis. In particular, a strong association between CXCR4 expression, mutation of BRAF (serine/threonine-protein kinase B-Raf), and the degree of neoplastic infiltration has been reported (23). These data indicate that the CXCR4 expression associated with oncogenic activation may represent a determinant of the local aggressiveness of neoplastic cells. It has been hypothesized that, also in PTC, CXCR4 expression and BRAF mutation status may cooperate in conferring a particularly aggressive tumor phenotype (23). One possibility is the direct involvement of inflammatory cells (e.g., T lymphocytes and Tregs). Our data show that expression of FoxP3 can be detected not only in tumor-infiltrating T cells, but also in epithelial neoplastic cells. Expression of this marker appears associated with two negative prognostic factors (i.e., extrathyroidal tumor invasion and distant metastasis). More importantly, FoxP3 expression in neoplastic cells is associated with a resistance phenotype to radioiodine treatment. Here, it should be recalled that BRAF mutations are frequent in PTC and may be associated with loss of the sodium/iodide symporter (NIS). This event is associated with radioiodine-refractory disease (34).
In the investigated cohort, expression of FoxP3 was not associated with overall survival. The very nature of PTC may explain these seemingly contradictory data. In fact, PTC is characterized by a good prognosis with high survival rates of over 20 years (27). In our series of 105 patients, only 9% died of the disease.
In conclusion, the data show an association of FoxP3 expression with features of PTC that seem to have a specific impact on radioiodine sensitivity.
Footnotes
Acknowledgments
This study has been supported by grants from Associazione Italiana per la Ricerca sul Cancro (AIRC, Milan, Italy); Istituto Toscano Tumori (Florence, Italy); Ministero dell'Istruzione, dell'Università e della Ricerca (MIUR, Rome, Italy).
Author Disclosure Statement
The authors declare no conflicts of interest.