
Abstract
Background:
With an observed general rise in papillary thyroid carcinoma incidence, papillary microcarcinoma (PMC) is accordingly found more frequently and often incidentally by histological examination of surgical specimens from presumed benign thyroid disease. Only a few studies have specifically addressed the prognosis of incidentally found PMC, and they have been limited to retrospective single-center studies.
Methods:
This was a national, unselected, prospective cohort study of 406 papillary thyroid microcarcinoma patients diagnosed in Denmark from 1996 to 2008.
Objective:
The aim of this study was to evaluate incidence, outcome, and extent of necessary treatment, with special attention given to incidentally detected PMC.
Results:
Age-standardized ratios were found to increase from 0.35 per 100,000 per year in 1996 to 0.74 per 100,000 per year in 2008. A total of 240 out of 406 cases were found incidentally, and a significant rise in incidence was only found for the incidental cases. Median follow-up was 7.6 years for the incidental cases, and in this time span, five cases of recurrence and no deaths from thyroid cancer occurred. The five-year recurrence-free survival was 98.1%, and only occurrence of lymph-node metastasis was found to affect the recurrence rate. A total of 160 incidental cases were initially treated with lobectomy, and the incidence of recurrence was not significantly different in the cases receiving completion thyroidectomy.
Conclusion:
The rising incidence of PMC in Denmark is explained by incidental cases. When the carcinoma is not the index tumor for surgery, this study implies that completion thyroidectomy does not improve prognosis.
Introduction
PMC is often found incidentally by histological examination of surgical specimens from presumed benign thyroid disease (9), and although it has been suggested that no further surgery is warranted (10), some differences in management exist. The choice of optimal strategy after detection of incidental PMC might still be a dilemma for the surgeon. Factors such as multifocality and lymph-node metastases at presentation are believed to be indicators of worse prognosis (11). Only a few studies have specifically addressed the prognosis of incidentally found PMC (IPMC), and they have been limited to retrospective single-center studies (12 –14).
In this study, we present a national, unselected, prospective series of papillary thyroid microcarcinomas in order to evaluate incidence, outcome, and extent of necessary treatment, with special attention paid to incidentally detected tumors.
Materials and Methods
The DATHYRCA database is situated within the Danish Head and Neck Cancer study group (DAHANCA). The database prospectively registers clinical, surgical, histopathological, and follow-up data from Danish thyroid cancer patients on a national scale. To secure completeness at the patient level, the DATHYRCA database was cross-checked with three national governmental databases: the Danish Cancer Registry, the Danish Pathology Registry, and the Danish Patient Registry. All cancers in Denmark are reported to the Danish Cancer Registry, and since 1987, reporting of data has been mandatory. The Danish Pathology Registry is a national database that includes all histological and cytological reports in Denmark. The Danish Patient Registry includes codes for clinical diagnoses and surgical procedures for all hospitalizations in Denmark. Due to a unique 10-digit personal identification number (CPR-number), it is possible to trace an individual patient throughout all of the governmental registries.
CPR-number lists from the DATHYRCA database were compared to lists from the National Patient Registry and the National Cancer Registry according to the ICD thyroid cancer code (DC73.9), and patients missing in the DATHYRCA database were identified. Furthermore, a cross-reference based on topological and morphological codes was made to the Danish Pathology Database. Medical records were reviewed for patients missing in the DATHYRCA database and, as a result of the overall cross-check procedure, 182 thyroid cancer patients were retrospectively included. This strategy does not ascertain completeness at the variable level, and some information may still be missing in the database. In general, diagnostic procedures were taken into consideration and were also registered if they had been performed in an outpatient setting. As a main principle, data were analyzed as reported. The follow-up period ended on March 1, 2012, and patients were censored in the event of death or emigration from Denmark (lost to follow-up).
This study was based on data available from the DATHYRCA database on May 21, 2012. The inclusion criteria were as follows: histologically verified papillary thyroid carcinoma, diagnosed between January 1, 1996, and December 31, 2008, largest diameter ≤10 mm, no prior history of thyroid cancer, and alive at the time of diagnosis.
In the basic DATHYRCA registration, no variable describes if the cancer is found incidentally or not, and in order to determine the initial indication for surgery, medical and histology reports were reviewed for all patients with PMC. To be categorized as incidental three criteria had to be met: (i) the PMC must not be the index tumor (the tumor for which surgical treatment was performed); (ii) a metastasis from thyroid cancer must not be the reason for the thyroid surgery resulting in detection of PMC; (iii) the histology of the surrounding specimen had to be benign (no malignancy except for the PMC must be found by histological examination of the thyroid specimen). Moreover, multifocal PMC were considered incidental if they fulfilled the mentioned criteria.
The database and analysis system Medlog was used for data registration, and STATA 11 was used for statistical analyses. Wilcoxon rank sum and chi-square tests were adopted to examine the relationship between variables, and Cuzick's test for trend was used to explore changes in incidence (15). p-Values of <0.05 were considered significant. All tests were two-sided. The Kaplan–Meier method and log-rank testing were used to estimate survival.
Age-adjusted incidences were calculated for the years from 1996 to 2008 according to the WHO World Standard Population (W) 2000–2025 (16). Data of the Danish population were retrieved from StatBank Denmark (17).
Results
A total of 406 patients met all the criteria for inclusion. Two patients were diagnosed at autopsy and were not included. The crude incidence rate (IR) for PMC in the period 1996–2008 was 0.57 cases per 100,000 per year. A rise in age-adjusted incidence rates is seen from 0.35 per 100,000 per year [95% confidence interval (CI) 0.27–0.43] in 1996 to 0.74 per 100,000 per year [CI 0.64–0.84] in 2008, and this was significant on a Cuzick's test for trend (p<0.01). Crude and age-adjusted incidence rates are shown in Figure 1.
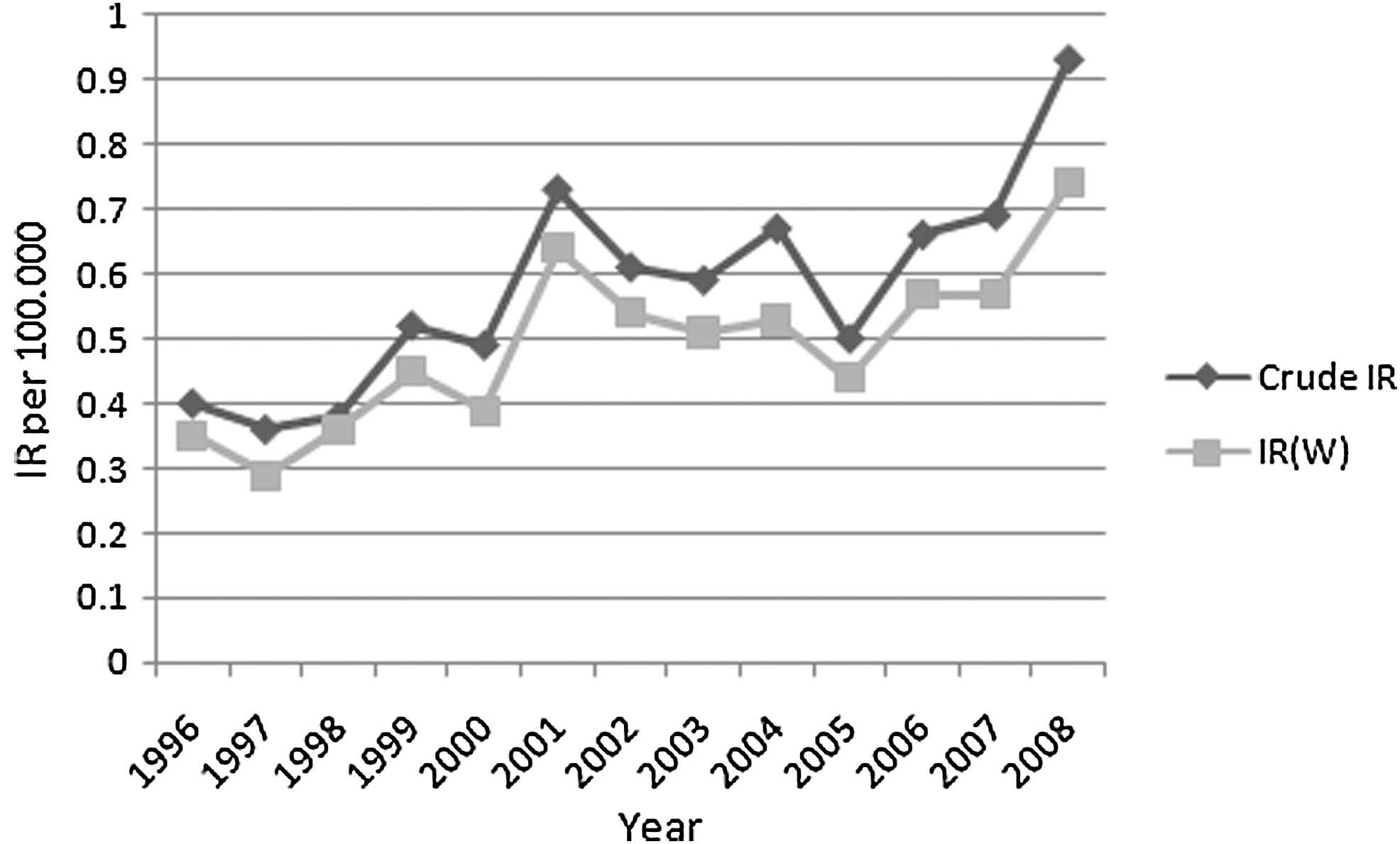
Crude and age-adjusted [IR(W)] incidence rates for papillary microcarcinomas in Denmark from 1996 to 2008.
Selected characteristics according to the way of detection (incidental vs. nonincidental) are shown in Table 1. A total of 250 cases (62%) were categorized as incidental. Larger tumor diameter, more frequent multifocality, extrathyroid extension, nodal and distant metastases, and a younger median age were found in the nonincidental group.
Histologically confirmed.
The yearly incidence of incidental and nonincidental tumors is shown in Figure 2, where an increased incidence of diagnosed IPMC seems to be present. A Cuzick's test for trend proved significant for this category (p<0.05), whereas no significant trend could be found for the incidence of nonincidental tumors (p=0.757).
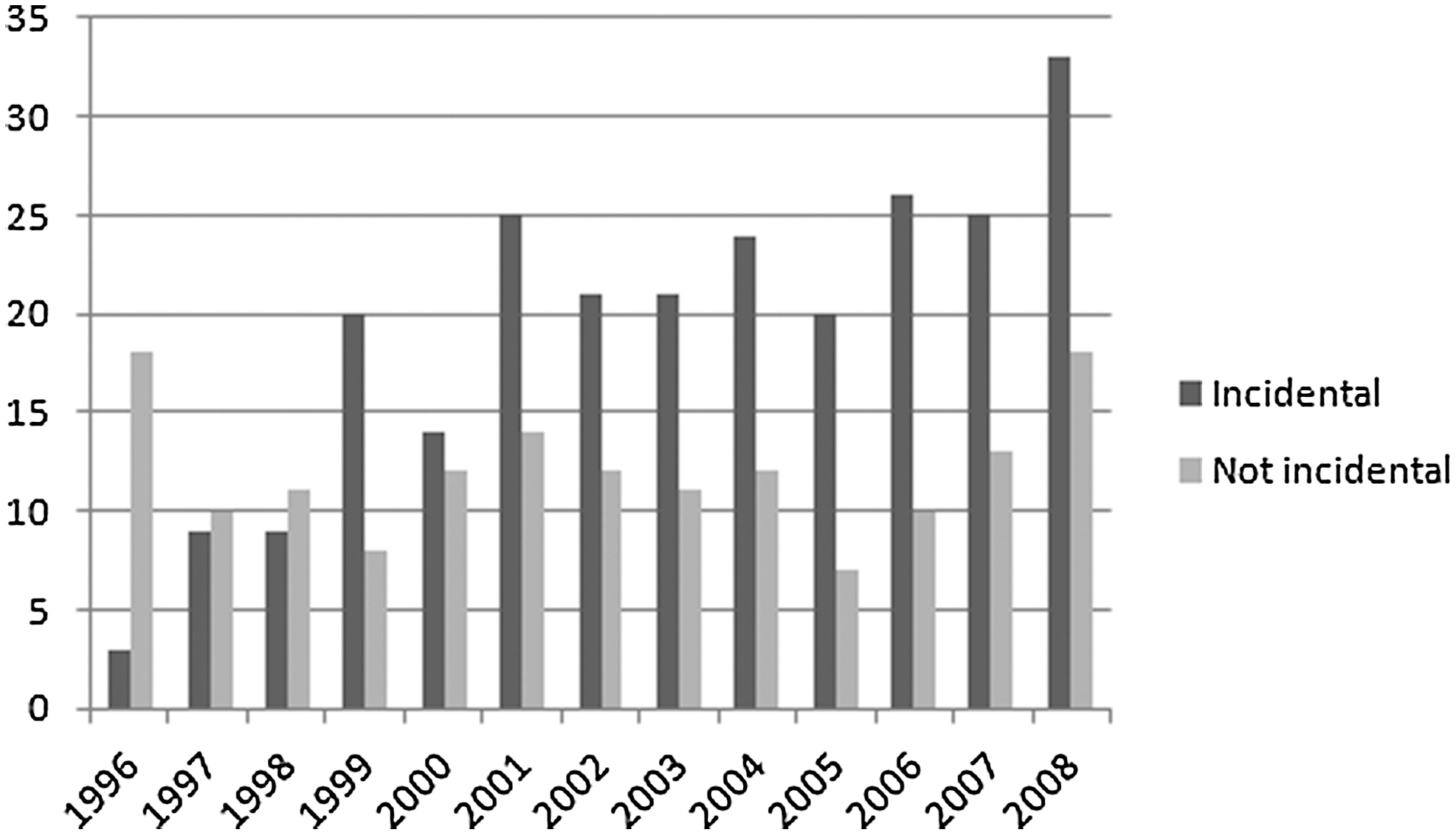
Cases of papillary microcarcinomas diagnosed yearly in Denmark from 1996 to 2008 divided according to the method of detection.
Treatment modalities and outcome
Figure 3 shows the extent of surgery on the thyroid gland, including both initial and completion procedures, according to incidental and nonincidental subtypes. Total thyroidectomy was performed significantly more often in the nonincidental group (p<0.001). For the IPMC, total thyroidectomy was carried out in 99 patients (40%), and in 50 of these (51%), the procedure was performed as the initial surgery. This procedure was used significantly more often as the primary surgical procedure (p<0.005) in the period after July 1, 2002. Comparing the tumor size of patients undergoing total thyroidectomy with those who underwent less extensive surgery as their primary surgical procedure showed no significant difference (p=0.19). To evaluate the need for further surgical treatment after diagnosis, the initial thyroid procedure of 250 IPMC cases were reviewed. Isthmus resection was performed in one patient, uni- or bilateral resection in seven patients, and subtotal or total thyroidectomy in 82 patients, leaving 160 patients with a lobectomy eligible for the analysis. In 39 of these cases, a subsequent completion thyroidectomy was performed. Five had histologically confirmed metastases to the lymph nodes at diagnosis and were excluded from the analysis, since this parameter has previously been shown to affect outcome. The results, presented in Table 2, show no difference in recurrence or survival between patients treated with lobectomy alone and those having supplementary surgery and in some cases radioiodine. Four recurrences were detected, and they were all situated in the thyroid bed (T-site). Three were found in the lobectomy group, and none of these were multifocal cases.
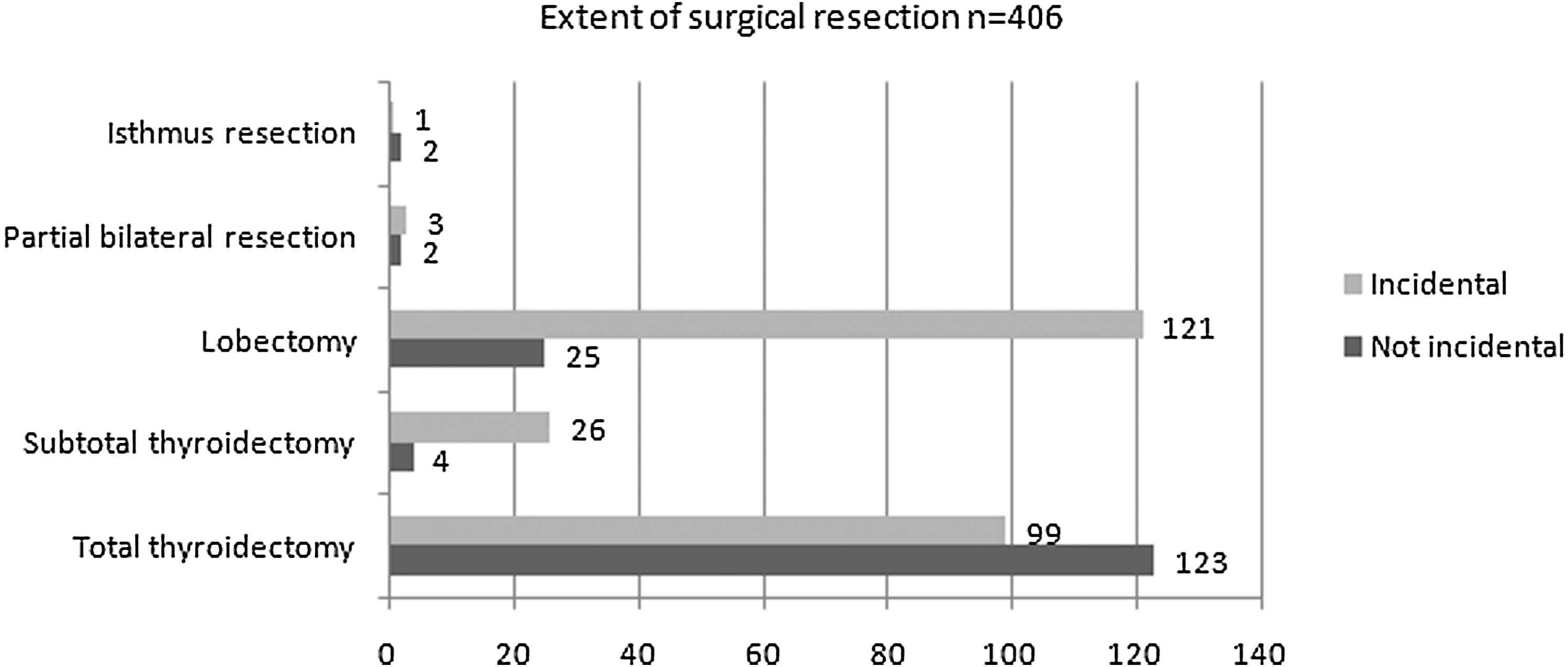
Extent of surgical resection of the thyroid gland in 250 patients with incidental papillary microcarcinomas and 156 with nonincidental papillary microcarcinomas in Denmark from 1996 to 2008.
NS, not significant.
In 53 patients (21%), radioiodine ablation was applied in the IPMC group, while this modality was used in 108 patients (69%) in the nonincidental group. Nodal surgery, either extirpation or neck dissection, was carried out in 31 patients (12%) in the IPMC group and 99 patients (63%) in the nonincidental group.
Median follow-up time was 8 years—7.6 years for the 250 IPMC cases (range 0.06–16 years) and 8.6 years for the nonincidental group (range 0.8–16.1 years). During this period, 15 recurrences were detected, with one third occurring in the IPMC cases. Thus, the relative risk of recurrence is 3.2 times higher in the nonincidental group (p<0.05). Six recurrences (40%) were found in the thyroid bed, seven (47%) in regional lymph nodes (N-site), and two (13%) had distant metastases (M-site). Four T-site and one N-site recurrences were in the incidental group. Figure 4 shows a Kaplan–Meier plot of recurrence free survival (RFS) in the incidental and nonincidental group. Log rank testing was applied to investigate if histologically confirmed lymph-node metastases, sex, multifocality, age >45 years at diagnosis, tumor size >5 mm, or extrathyroid extension were predictors of recurrence. Only the presence of lymph-node metastases was a significant factor (p<0.05).
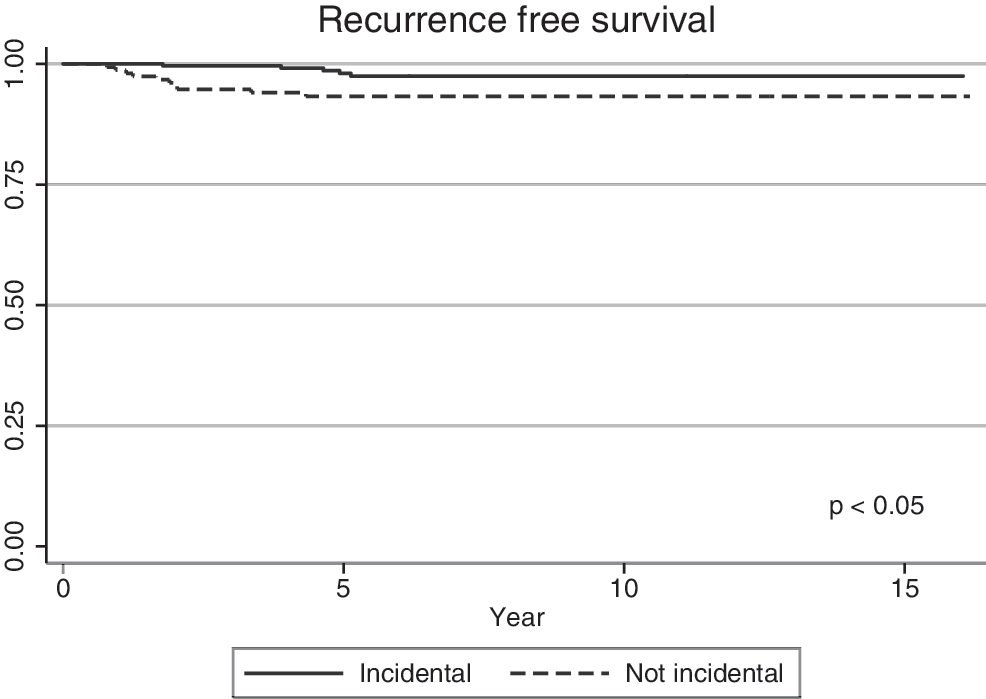
Plot of recurrence-free survival in 250 patients with incidental papillary microcarcinoma and 156 patients with nonincidental papillary microcarcinomas in Denmark from 1996 to 2008.
The five-year RFS was 98.1% [CI 94.9–99.3], and the 10-year RFS was 97.5% [CI 94.0–99.0] in the incidental group, and 93.3% [CI 87.9–96.3] for both 5 and 10 years RFS in the nonincidental group. This difference has been proven to be significant by log rank testing (p<0.05).
During the follow-up period, two patients died from nonincidental PMCs, and 40 patients died of other causes. Among these, 14 died from another cancer, 21 died from other diseases, two committed suicide, and in three cases, the cause of death could not be determined. Five-year cause-specific and crude survival was 100% and 92.6% [CI 88.4–95.4] respectively, and 10-year cause-specific and crude survival was 100% and 92% [CI 87.5–94.9] for the IPMC group, while five-year cause-specific and crude survival was 98.5% [CI 93.9–99.6] and 94.6% [CI 89.5–97.3], and 10-year cause-specific and crude survival was 98.5% [CI 93.9–99.6] and 86.5% [CI 78.9–91.4] in the nonincidental group. Significance in cause-specific survival could not be proven by log rank testing (p=0.08). The cause-specific survival is shown in Figure 5.
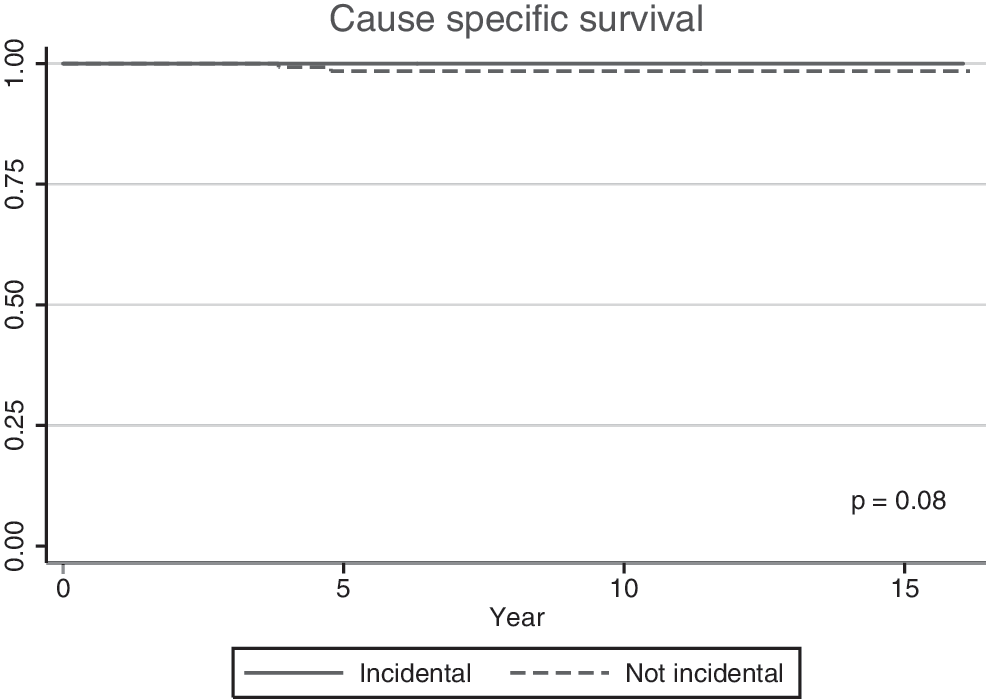
Plot of cause-specific survival in 250 patients with incidental papillary microcarcinomas and 156 patients with nonincidental papillary microcarcinomas in Denmark from 1996 to 2008.
Discussion
In accordance with known literature, this national study provides further evidence that PMC is more frequently detected, and we have been able to demonstrate that the increase is caused by incidental cases. Furthermore, it seems that the outcome is not improved by completion thyroidectomy in the case of IPMC.
As this study is built on national data, where the prospective registration has been carried out at six different referral centers, some inconsistency may exist. Patients who were diagnosed outside these centers may have been missed at the initial registration. For this reason, a cross-reference to the Danish Patient Registry was carried out, and missing patients were retrospectively included. Denmark has a system of public health insurance, and the hospital payment for treatment depends on the diagnosis reported to the patient registry. Therefore it is considered very accurate. By cross-checking with these two registries, including the Danish Cancer Registry, it is certain that a very high degree of completeness has been achieved. This reduces or even eliminates the risk of selection bias.
To our knowledge, this is the first national study on the outcome of IPMC. However, the strength of the design is debatable, since it is only an observational study. A randomized design of IPMC patients to either no further surgery or completion thyroidectomy and perhaps radioiodine would have been a better way to address the question about the optimal treatment level for this patient category. However, several studies have already shown very high survival rates for IPMC patients that are comparable to the background population, and a design including randomization to further surgery with increased risk of complications might not be preferable for ethical and economic reasons.
Previous studies have investigated the proportion of IPMC among patient with PMC, and frequencies between 21% and 99% have been published (14,18). This reflects that no uniform definition has been established, but also institutional selection and differences in diagnostic work-up strategies play a role. In our study of unselected cases, the proportion of IPMC was 62%, which is comparable to the 58% found in the study by Dunki-Jacobs et al. in the setting of a community hospital (19), and with definitions that are very similar to ours.
As previously stated, the incidence of papillary thyroid carcinoma has been rising in several countries, and this seems to be especially true for PMC (1). Much debate has focused on the reason for this rising incidence. This study clearly demonstrates that the proportion of incidental cases is the main reason for the rising incidence in PMC, which points to increased pathological detection as the explanatory variable. Grodski et al. (20) and Neuhold et al. (14) have previously shown that the rising incidence of IPMC was associated with increased sampling of resected specimens by pathologists. If more thyroid surgery on a national scale has been exerted in the period, this may also explain the increase, but our group has previously examined this question without finding any significant impact of this aspect (21). In the current study, however, it was found that total thyroidectomy is more often used in diagnosed cases in the recent period, indicating that a change in surgical practice also plays a role.
The outcome for patients with IPMC in this series is excellent and similar to what is reported elsewhere for PMC (3,4,14). This is highlighted by the fact that no patients died from IPMC during a median follow-up of 7.6 years. No significant difference was found in survival between incidental and nonincidental cases. However, our cohort of 406 cases has not been followed long enough to draw conclusions regarding this particular point.
By log rank testing, lymph-node metastasis was the only factor that significantly affected RFS, and this factor seems to be the main explanation for the difference in outcome between IPMC and nonincidental cases.
Of the IPMC cases, five patients (2%) had histologically confirmed lymph-node metastases. It is possible that some metastases were missed because not all patients underwent lymph-node surgery. Indeed, the incidence of metastases in our study is not high compared to previous studies, in which incidences from 22% to 69% have been reported (22,23). The figures seem to depend on the use of neck dissection and the histopathological examination of the lymph-node specimens. In 2002, Qubain et al. (24) examined the distribution of micrometastases in N0 patients, and 26% were positive when cytokeratin immunohistochemistry was utilized. With this in mind, it is interesting that no IPMC without histologically confirmed metastases developed recurrence in the lymph nodes. Similar results were found by Neuholdt et al. (14), confirming that lymph-node dissection should be reserved for patients with clinical signs of metastasis or histologically confirmed metastases.
With the rising incidence of IPMC reported in this study and previously for PMC, the question of optimal treatment for PMC has formerly been addressed. On one hand, authors advocate that observation is sufficient (25), while others advocate that microcarcinomas should be treated as any other papillary carcinoma, meaning total thyroidectomy with possible radioiodine ablation (26,27). When a papillary microcarcinoma is incidentally found, our results indicate that total thyroidectomy does not improve the prognosis. However, it has to be stated that the study is limited in terms of conclusions about optimal treatment because of the observational nature, since different treatment modalities have been used.
Even in patients with multifocal disease, the prognosis was not significantly different in this study. This is in contrast to previous studies (3,5) where multifocality has been identified as a risk factor. Moreover, in a comprehensive meta-analysis study by Roti et al. (28), multifocality was shown to be highly significantly associated with recurrence. Our study is limited by the number of patients and the observation time, which could explain our failure to show a significant impact on survival.
With the excellent prognosis of a five-year RFS exceeding 98% and no cause-specific mortality for IPMC and similar outcomes between groups undergoing only lobectomy and completion thyroidectomy, these results are in accordance with current European guidelines (10), recommending that completion surgery is not warranted in this group of patients. Other retrospective studies of outcome from IPMC have reached similar conclusions (12 –14).
Conclusion
The rising incidence of PMC in Denmark is explained by incidental cases. When the carcinoma is not the index tumor for surgery, this study implies that completion thyroidectomy does not improve prognosis. However, longer follow-up is needed to evaluate survival.
Footnotes
Acknowledgments
We thank the Odense University Hospital, University of Southern Denmark, DAHANCA, Becket-Fonden, and Else og Mogens Wedell-Wedellsborgs Fond. This study has been approved by the Danish Regional Ethics Committee and by the Danish Data Protection Agency.
Author Disclosure Statement
No competing financial interests exist. No writing assistance used.