
Abstract
Background:
Even though the presence of antithyroglobulin antibodies (TgAbs) represents a significant problem in the follow-up of patients with differentiated thyroid cancer (DTC), the current guidelines on the management of DTC that have been published in recent years contain no text concerning the methods to be used for detecting such antibody-related interference in thyroglobulin (Tg) measurement or how to manage TgAb-positive patients in whom Tg cannot be used reliably as a tumor marker.
Aim:
An international group of experts from the European Thyroid Association Cancer Research Network who are involved in the care of DTC patients met twice to form a consensus opinion on how to proceed with treatment and follow-up in TgAb-positive DTC patients based on the available evidence in the literature. Here we will report on the consensus opinions that were reached regarding technical and clinical issues.
Results:
This clinical opinion article provides an overview of the available evidence and the resulting consensus recommendations. The current literature does not provide sufficient data for giving evidence-based answers to many questions arising in the care of TgAb-positive DTC patients. Where insufficient evidence was available, a thorough discussion by a group of physician-scientists, all of whom have a distinguished track record in thyroid cancer care, was held to arrive at a consensus expert opinion. The questions and answers discussed were then summarized into an algorithm for the management of TgAb-positive patients.
Conclusion:
We were able to define 26 consensus expert recommendations and a resulting algorithm for the care of TgAb-positive DTC patients.
Introduction
Although the presence of TgAbs represents a significant problem in the follow-up of DTC patients (7 –10), the various reviews on this subject (10) and guidelines on the management of DTC that have been published in recent years contain no text concerning the methods to be used for detecting such antibody-related interference in Tg measurement (11 –15). Furthermore, present guidelines lack clear recommendations on the management of TgAb-positive patients in whom Tg cannot be used reliably as a tumor marker.
An international group of experts (in endocrinology, nuclear medicine, and laboratory medicine) who are involved in the care of DTC patients therefore assembled for a conference in Berlin, Germany (November 6, 2011) and in Pisa, Italy (September 9, 2012) to form a consensus opinion on how to proceed with treatment and follow-up in DTC patients who are TgAb-positive. Further discussion was carried out via electronic communication. The consensus group also included one representative from an assay manufacturer and one from thyroid cancer patient organizations. In this article, we report on the agreements reached during these meetings.
This consensus statement was explicitly not intended as a guideline since little or no solid scientific evidence exists in the literature to answer many of the questions that we frequently confront, which compelled us to focus on expert opinion. Whenever possible, physicians should first refer to the relevant guidelines. Should no help be forthcoming there, it is our hope that this document can provide some inspiration or even a sense of direction on how to proceed. Nonetheless, since this document does not constitute a guideline as such, DTC patients with circulating TgAbs will require individualized management and follow-up, both of which demand the skill and experience of an interdisciplinary team of experts in endocrinology, nuclear medicine, and laboratory medicine.
Methods
Before the consensus meeting, a review of the literature up to and including August 2012 was performed by the participants, and a series of questions were posed: 1. Questions concerning the methodology of measurement of Tg, TgAbs, and HAbs 1.1 Which method should be used for the detection of TgAbs? 1.2 How to define a “positive” TgAb level in DTC patients? 1.3 Are there methods to eliminate TgAb interference in Tg measurement? 1.4 Which method should be used for the detection of HAbs and when? 2. Questions regarding the clinical assessment of patients with TgAbs 2.1 When should serum TgAb levels be measured? 2.2 Can serum TgAb levels be used as a surrogate tumor marker? 2.3 Are there clinically useful alternatives to serum Tg and serum TgAb measurement that can be used as tumor marker in TgAb-positive DTC patients? 2.4 What type of follow-up is appropriate for patients with TgAbs? 2.5 Which imaging methods are appropriate in DTC patients with TgAbs?
During the consensus meeting these questions and the corresponding evidence available in the literature were discussed. A consensus answer was reached for each question. In the process, the evidence in the literature for each question was graded using the same system used for the Revised American Thyroid Association Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer (11), which in turn was adapted from the U.S. Preventive Services Task Force, Agency for Healthcare Research and Quality (16). This grading system is summarized in Table 1. Based on the consensus opinions, a management algorithm for use in clinical practice was formulated.
The definitions used in grading these recommendations are identical to those used by Cooper et al. (11) in the American Thyroid Association Guidelines.
Results
1. Technical Issues in Tg and TgAb Measurement
1.1. Which method should be used for the detection of TgAbs?
There are basically two methods for the detection of TgAbs: either the direct measurement of the antibodies or the determination of recovery rates in Tg testing. Whereas the former method will, depending on the assay used, detect most TgAb-positive patients, the latter method will, due to its relatively wide reference range, predominantly show strong interferences when using a conventional recovery buffer containing 40–50 μg/L Tg (17). On the other hand, not all patients with positive TgAbs will show interference in recovery measurement (17 –19). Sometimes, seemingly low levels of TgAbs may be associated with strong interference, whereas some patients with high levels of TgAbs show no signs whatsoever of interference in the Tg measurement (7,18 –28). Nonetheless, in all such cases a faster biological clearance of TgAb-bound Tg, resulting in lower blood levels of Tg, cannot be excluded, thus causing an unreliable Tg measurement (29 –31).
Immunometric and competitive assays
The presence of TgAbs usually results in reduced or undetectable levels of Tg in widely used immunometric assay (IMA) methods (i.e., immunoradiometric assays [IRMAs], immunochemiluminometric assays) regardless of the serum concentrations of either Tg or TgAbs (10,19,32 –37), although newer assays appear to be more resistant to the influence of TgAbs than older generation ones (38).
The competitive radioimmunoassays (RIAs) are reported to be more resistant to TgAb interference (7,18,19,39,40). However, TgAb interference may falsely increase Tg levels in some RIAs (7 –9,18,19,39 –42). Additionally, these methods are less sensitive than IMAs and, in turn, they cannot detect the low Tg levels typically found in (nearly) cured DTC patients. An important issue is the heterogeneity of TgAb assays, which differ with regard to the recognized TgAb epitope (19). In addition, this issue is further complicated by the fact that in autoimmune thyroid disease, TgAbs target a multitude of different epitopes, which differ from those targeted by TgAbs in DTC patients (21,26). As a consequence, these assays display different sensitivities for the detection of TgAbs, and they also differ with regard to the absolute levels of measured antibodies. Since different Tg assays also measure different Tg epitopes (19,43), using a TgAb assay that most likely recognizes TgAb interference in that particular Tg assay should be encouraged. In practice it is often assumed that this TgAb assay is most likely an assay from the same manufacturer, although there is no evidence in the literature to support this assumption.
Even though most TgAb assays on the market are claimed to have been standardized against the first International Reference Preparation 65/93 standard, wide interassay variability between different TgAb assays is observed (10,19,24,25,27,44). Even different laboratories using the same assay may produce considerably different results. As is also stated in recommendation 43 of the ATA guidelines from 2009, like Tg levels, TgAb levels are therefore best measured longitudinally using the same assay in the same laboratory. This is especially important when the use of TgAb levels as a surrogate tumor marker (see section 2.2) is considered. Should a change of assays occur, the TgAb measurement should be performed simultaneously at least once with both assays in each individual patient in order to establish an individual baseline level with the new assay.
■
TgAb levels, like Tg levels, are best assessed using an immunometric assay.
■
For the detection of serum TgAbs, it is recommended to use an assay that is standardized against the International Reference Preparation 65/93 standard.
■
In order to assess the presence of TgAb interference when using a given Tg assay, a TgAb assay from the same manufacturer is preferable.
■
For longitudinal consistency of clinical care, consecutive measurements of TgAb levels should be performed in the same laboratory using the same assay every time.
Recovery testing
Although recovery testing most likely will not suffice to rule out TgAb interference in Tg measurement due to the aforementioned in vitro and in vivo biological considerations (7,17,19,29 –31,42), a sensitive recovery test would represent an easy and low-cost alternative for the detection of potential TgAb or HAb interference.
Conventional recovery testing with serum buffers containing 40–50 μg/L of Tg is considered undisturbed by most manufacturers if recovery rates are >70%; that is, a concentration of 15 μg/L Tg can be missed without finding a pathologic recovery. Several studies in the literature indicate that the lower limit of the reference range is approximately 80% (7,45,46), which would still allow an obfuscation of 10 μg/L Tg. Given such a wide reference range, only strong interferences will be shown when using a conventional recovery buffer containing 40–50 μg/L Tg. In earlier days, when the lower detection limit of Tg assays was approximately 5 μg/L, this low sensitivity of recovery measurement might have been adequate. In modern clinical practice, a level of 1 μg/L is considered relevant (11 –15); as a consequence, conventional recovery testing is no longer adequate. Data in the literature also show that in patients with circulating TgAbs, the measured Tg levels are significantly lower than in controls, even when recovery rates are still within the reference range. Furthermore, even in patients who are positive for the presence of TgAbs but show no interference in a recovery measurement, a faster biological clearance of TgAb-bound Tg cannot be excluded (29 –31). A faster clearance would result in lower blood levels of Tg and thus clinically unreliable Tg results.
A new development in recovery testing is the introduction of the so-called “mini-recovery,” in which recovery measurement is performed by adding serum with a low (i.e., 1–5 μg/L) Tg concentration (46). The performance of this mini-recovery has not yet been investigated extensively in DTC patients. Theoretically, however, this mini-recovery test should be able to identify a detection loss of about 1 μg/L Tg, which, as already described, represents a clinically relevant limit according to current international guidelines. Further investigations on the value of this mini-recovery test appear warranted (46), but currently there is not enough evidence to recommend either in favor of or against this method (recommendation grade I).
In clinical practice, all of us occasionally encounter patients who, while having clear foci of disease or thyroid remnants, nonetheless have undetectable serum Tg levels in spite of negative TgAb tests (47 –49). Undetectable pre-ablation Tg levels in the presence of negative TgAbs may suggest a thoroughly complete total thyroidectomy. However, it may also occur when TgAbs are not measured properly, the spatial conformation of Tg is changed leading to a decreased immunoreactivity, the thyroid cancer has lost its ability to secrete Tg, or when HAbs are present.
Erroneous undetectable pre-ablation Tg levels might be suspected in cases in which patients have an advanced TNM stage, a high risk of recurrence, and/or thyroiditis is found in the pathological analysis of the surgery specimen, and/or presence of metastases or a large thyroid remnant (with an 131I uptake usually >2%) on post therapeutic whole-body scintigraphy (WBS). Especially in the case of metastasized disease, the possibility of a non–Tg-secreting tumor should be considered.
Such findings always raise the question of whether the measurement of Tg is reliable (indicating that the tumor no longer produces Tg), whether a sufficiently sensitive and specific TgAb assay has been used, or whether one of the other previously mentioned factors is present (4,6,50). Different approaches such as measuring Tg with different IMAs or comparing results of Tg IMA and RIA methods, retesting for TgAbs using different assays, performing recovery tests, or screening for HAb interferences should be available in this setting. However, the problem is complex and the care required in interpretation of the results is exemplified in a recent study of 288 consecutive DTC patients, 47 of whom were found to have an undetectable serum pre-ablation Tg by a particular IMA but had residual 131I uptake on postablation whole-body scanning (48). In order to investigate the possibility of antibody interference, the authors measured TgAbs with two different assays, performed Tg recovery experiments, pretreated samples with HAb blocking tubes and measured Tg using two further IMAs. Of the 47 patients, 10 were found to have TgAbs and one had HAbs causing a negative interference in Tg measurement. Of the remaining 36 patients, 18 had a detectable Tg by a second IMA and 18 a detectable Tg by a third IMA. Thus, after extensive laboratory investigation, only 9 of the original 47 patients with an initially undetectable serum Tg with residual 131I uptake were confirmed to have an undetectable serum Tg and no evidence of assay interference (48).
In order to overcome this problem, we would like to draw the attention to a proposed “in vivo” recovery test (34): Tg and TgAb measurement can be performed preoperatively in any patient with suspected DTC who is referred for thyroidectomy (49). In patients with nodular thyroid disease or a malignant tumor, it is expected that Tg will be detectable before surgery, even though “normal” Tg levels generally have no clinically reliable meaning with regard to, for example, the presence of metastases (11); very high Tg levels in the absence of a thyroiditis may however suggest metastatic spread. This strategy will provide a “baseline” Tg and TgAb situation, which, as the National Association of Clinical Biochemistry (NACB) guidelines state (34), will allow assessment of the reliability of Tg and TgAb measurements in the same patient after thyroidectomy.
Patients in whom lymphocytic thyroiditis is diagnosed postoperatively (i.e., identified in the pathological analysis of thyroidectomy specimens) have a very high likelihood of TgAb positivity (51). The Tg epitope recognition pattern of TgAbs in patients with lymphocytic thyroiditis surrounding a thyroid cancer is similar to that of other patients with autoimmune thyroid disease (26). Should lymphocytic thyroiditis be described in a TgAb-negative patient, it is most likely worthwhile checking for the presence of TgAbs using multiple assays (17,18,43,51) if the routine TgAb assay produces a negative result.
■
Conventional recovery testing for the detection of TgAb interference is not accurate enough for use with modern Tg assays in the care of DTC patients.
■
Although the measurement of Tg and TgAbs before thyroidectomy for a suspected or proven DTC is not recommended for clinical purposes, a prethyroidectomy Tg and TgAb measurement might be used as an in vivo recovery test in order to assess the reliability of Tg for use as a postoperative tumor marker.
1.2. How to define a “positive” TgAb level in DTC patients?
Currently there is no consensus in the literature on how to define a positive test for TgAbs in DTC patients. Recently, it has been suggested that in modern quantitative TgAb assays up to 20% of samples may be misclassified if the manufacturer-recommended cut-off levels (MCOs) are used to define a positive test for TgAbs (18,20). The MCOs are calculated for use in the diagnosis of autoimmune thyroid disease, a condition in which TgAb levels are generally higher than in most DTC patients and a potential interference in Tg testing is not at the forefront (52). However, low concentrations of TgAbs, which are still considered “normal” when using the MCO, may already cause clinically significant interference in the Tg measurement employed in DTC patients.
In 2011 articles, Spencer (10) and Spencer et al. (18) postulated that the limit of detection (LoD) for a given assay should represent the cut-off for TgAb positivity. The LoD is defined as the lowest concentration of an analyte that can be detected with a stated uncertainty (i.e., the concentration corresponding to a signal 2 or 3 standard deviations above the mean for a calibrator free of analyte). LoD and MCO for several assays that are currently on the market are given in Table 2. In the study by Spencer et al. (18), 20% of DTC patients had TgAb levels between the LoD and the MCO.
LoD, limit of detection; LoQ, limit of quantification; MCO, manufacturer cut-off level; TgAb, antithyroglobulin antibody.
The postulate of using the LoD was based on a comparison between the results of TgAb tests and an IRMA-to-RIA ratio for Tg measurement, in which the RIA was used as the gold standard (18). However, employing this IRMA-to-RIA ratio is controversial because this method has not been independently validated as an accurate index of clinically relevant interference in Tg measurement. Therefore, the percentage of misleading results, which in the study by Spencer et al. (18) was as high as 50%, was probably (considerably) overestimated and would at least require further confirmation.
An alternative to the LoD, the limit of quantification (LoQ), also known as the functional sensitivity, has been proposed. LoQ is the level of the analyte at which the assay is able to reproduce the results with an interassay coefficient of variation not exceeding 20%. Using the LoQ instead of the LoD as a lower limit for TgAb detection would provide a higher degree of certainty that the measured TgAb level does indeed represent a potentially relevant interference in the individual patient, although further study is needed to confirm this.
As a technical note, it should be emphasized that for any assay used in the care of thyroid patients both reference ranges and the LoD as well as the LoQ should be determined in-house, as recommended by the guidelines from the National Association of Clinical Biochemistry (34). Manufacturers are encouraged to evaluate and state the LoQ of TgAb assays for diagnostic use. However, although these data can be used as a guide, they cannot substitute independent in-house assay evaluations. For accurate diagnostics in DTC patients, it may furthermore be necessary to create assay standards that approach the LoQ of the TgAb assay. As such standards are not usually included in assay packages, for now laboratories are encouraged to create their own standard materials in this setting.
■
In DTC patients, the LoQ of a given TgAb assay should be regarded as the upper normal limit for the presence of TgAbs.
■
Thyroid laboratories should report two reference ranges for TgAbs: one based on the presence of TgAbs in a population free of thyroid disease, which should be used for the diagnosis of autoimmune thyroid disorders, and the LoQ which should be used as the upper normal limit in DTC patients.
■
Laboratories should verify the LoD, LoQ, and reference range in their own patient population.
1.3. Are there methods to overcome TgAb interference in Tg measurement?
To the best of our knowledge there are no validated methods for completely eliminating the interfering effects of TgAbs.
Some laboratories have adopted a policy of switching to an RIA for Tg measurement once the presence of TgAbs has been recognized (18). Although in some cases this may reduce the interference of TgAbs in the measurement of Tg, the use of RIAs in large parts of the world is not feasible due to the limited availability of such assays. Furthermore, conventional RIAs are not sensitive enough (9) to detect the very low levels of Tg which, with modern immunometric assays, are used to define the difference between a disease-free patient and one with persistent disease.
Another strategy that has been pursued in the last few years is to switch to tandem mass spectrometry for the measurement of serum Tg in the presence of TgAbs. Although Hoofnagle et al. (53) were able to show that in principle this method is feasible, the analytical sensitivity of tandem mass spectrometry is currently not sufficient for clinical use (53,54). However, further research into this technique, especially on how to improve analytical sensitivity, is desirable.
Furthermore, both these alternative strategies still cannot overcome the possibility that circulating TgAbs might lead to a faster clearance of antibody-bound Tg, which in turn results in an inappropriately low serum level of Tg even before blood is drawn.
■
Currently there are no methods for overcoming TgAb interference that result both in sufficient accuracy and sufficient sensitivity of Tg measurement for clinical use.
1.4. Which method should be used for the detection of HAbs and when?
Fortunately, HAb interference, not to be confused with TgAb interference, in Tg measurement is rare and often does not significantly affect Tg measurement. The prevalence of HAb interference in DTC patients is reported to be variable. Although in their study Preissner et al. (5) suspected HAb interference in as much as 13% of DTC patients, most other studies report a significant, but clinically irrelevant interference in less than 2% of patients (4,6,50,55).
In clinical practice, several methods are available for the detection of HAb interference. Just using the Tg IMA, HAb interference may be detected either by recovery measurement or by measurement of Tg in serially diluted sera (provided Tg levels are high enough). An additional method, which is more specifically geared towards HAb interference, is only pretreating serum with proprietary HAb blocking tubes and subsequently comparing the result of Tg measurement with the one obtained in serum that was not pretreated. Whether the (potentially considerable) additional costs of any such strategies can be justified considering the low incidence of HAb interference in the general population of DTC patients (<2%) (4,6,50,55) has not been studied. HAb testing or, alternatively, recovery test or serum serial dilution should be performed, however, in patients with discordant clinical findings (e.g., positive imaging, undetectable serum Tg in the absence of TgAbs) and/or unusual clinical courses of Tg levels or Tg recovery. In patients with an unusual clinical course of Tg levels (e.g., detectable serum Tg levels which hardly change over time and do not increase after thyrotropin [TSH] stimulation), HAb interference should also be suspected.
■
Considering the low prevalence of HAb interference, routine testing for the presence of HAbs is not recommended.
■
In the event of clinical suspicion of HAb interference, testing for the presence of HAbs can be performed using proprietary, commercially available heterophilic antibody blocking tubes. Recovery testing and/or serial serum dilution measurement of Tg can be considered as alternatives for the use of blocking tubes.
Clinical considerations
TgAbs are more frequently present in female than in male DTC patients (7), and they are much more prevalent in DTC patients than in the general population (2,7).
The presence of TgAbs is usually an expression of the presence of an autoimmune thyroid disease, such as chronic autoimmune thyroiditis (even focal) or Graves' disease. The removal of all thyroid tissue through thyroidectomy and 131I ablation of thyroid remnants should, at least in theory, eliminate all antigens eliciting the autoimmune response. This in turn would lead to the disappearance of the autoimmune process along with circulating TgAbs (1,56,57). Conversely, persisting or rising serum TgAbs could indicate the presence of remaining or recurring thyroid (cancer) tissue. Chiovato et al. (1) demonstrated that, after initial treatment with thyroidectomy and 131I ablation, it took a median of 3 years following treatment for TgAbs to disappear (i.e., after 3 years, 50% of the original group of TgAb-positive patients were still positive for TgAbs!) in a large population of DTC patients with TgAbs.
2. Clinical Assessment of Patients with TgAbs
2.1. When should serum TgAb levels be measured?
In light of the identified considerations, TgAb measurements must be considered mandatory in the follow-up of all patients with DTC who were initially TgAb-positive.
There is still an open debate on whether it is useful to measure TgAbs in patients who never had circulating TgAbs, provided the same assay was used for every measurement during follow-up.
Although there is some evidence of cases in which an elevation of TgAbs was the biochemical sign of recurrence (7,32,36,58 –60), such cases concern patients who were TgAb-positive at diagnosis. Therefore, there is no evidence that the repeated measurement of TgAbs is useful in patients who were never positive for TgAbs. Nonetheless, in adherence to existing guidelines we would advise to err on the side of caution until more solid evidence is available to select those patients in whom the presence of TgAbs should be measured perpetually. This caution implies measuring TgAbs concomitantly with any Tg assessment. This is also suggested in the American Thyroid Association guidelines of 2009 in recommendation 43 (11).
When using the longitudinal measurement of serum TgAb levels as a surrogate tumor marker, the effects of any immune system modulating drug should be considered. Many drugs, of which interferons are a good example, either stimulate or suppress the immune system and may thus temporarily lead to falsely elevated or decreased serum TgAb levels, or may even induce TgAbs (61). As there is no clear evidence in the literature regarding the duration of the effects of such modulating drugs, we propose waiting a longer rather than a shorter interval after cessation of the medication before resuming longitudinal monitoring of TgAb levels —a period of 6 months appears to be the minimum appropriate waiting period.
A similar waiting period should be addressed after each 131I treatment course, because the radiation-induced damage to thyrocytes can cause a temporary and transient flare-up of the autoimmune process underlying the presence of TgAbs (58,62 –65). Here too, a minimum waiting period of 6 months seems to be appropriate before considering an increase in TgAbs to indicate potentially progressive disease. Should TgAb levels decrease in the months after 131I therapy, however, we feel this can nonetheless be interpreted as a sign of remission of disease.
■
The presence of TgAbs should be assessed quantitatively in concurrence with every Tg measurement during the treatment and follow-up of differentiated thyroid cancer patients.
■
After the administration of immune system modulating drugs or 131I treatment, an interval of at least 6 months after cessation of the drug should elapse before TgAb levels can be interpreted and compared reliably with pretherapy levels in the longitudinal follow-up of patients with DTC.
2.2. Can serum TgAb levels be used as a surrogate tumor marker?
In their study on the course of TgAbs after treatment of DTC, Chiovato et al. (1) noted a significant correlation between the levels of TgAbs and the disappearance of thyroid tissue. This observation confirms the theoretical model that was just described. Therefore, it can be suggested that TgAbs can be used as a surrogate tumor marker: patients in whom TgAb levels decrease are likely to be at much lower risk of recurrence or persistent disease than those with stable or rising serum TgAb levels. In recent years an increasing body of evidence has emerged supporting this proposition.
Pacini et al. (2) in 1988 already described a correlation between the clinical course of DTC and the changes in TgAb levels: in most patients without recurrent or persistent disease, the serum TgAb levels decreased considerably or disappeared altogether; only a few patients without persistent or recurrent disease showed stable or increasing serum TgAb levels. In contrast, the majority of DTC patients with persistent disease showed unchanged or increasing serum TgAb levels. Similar observations were reported by Rubello et al. (66) in 1992 and by Spencer et al. (7) in 1998. Chung et al. (32) in 2002 showed that a clear difference exists between TgAb-positive and TgAb-negative patients with regard to DTC recurrence rates (49% and 3.4%, respectively). Kim et al. (60) published an interesting study in 2008 showing that serum TgAb levels 6–12 months postablation have a remarkable prognostic significance: TgAb-negative DTC patients had a disease-free survival rate of more than 95% over the course of 160 months, while TgAb-positive patients had a disease-free survival rate below 80%. In fact, based on a comparison of TgAb levels 6–12 months after ablation to TgAb levels immediately before ablation, three groups emerged in the Kaplan-Meier analyses. Those patients in whom postablation serum TgAb levels had dropped to less than 50% of the baseline value had a good prognosis with none of them showing recurrence. Those patients in whom serum TgAb levels had dropped less than 50%, but had not increased, had a disease-free survival of approximately 80%. Those in whom TgAb levels 6–12 months after ablation had increased compared to baseline only had a 55% disease-free survival during the subsequent follow-up (67).
In patients in whom serum TgAb levels disappear during the follow-up, the problem of TgAb interference is solved and serum Tg assays can be used reliably. For the management of such patients we invite the reader to consult one of the many guidelines on the treatment of DTC that are available in the literature.
As just described, it is more important to evaluate the trend in serum TgAb levels rather than the absolute values when using serum TgAb levels as a surrogate tumor marker. Hence, a patient showing a decrease in TgAb levels from 3000 to 1000 U/L within 1 year is likely to be better off than the patient who shows an increase from 200 to 400 U/L. In this respect, it therefore invites the question of how to define a change in Tg levels. Assuming a normal distribution of analytical and biological variability, the minimal critical change (Δc) for two measurements can be defined as Z×21/2×(bCV2+aCV2)1/2, where Z is the Z-score for a given significance level, and bCV and aCV are the biological and analytical coefficient of variation, respectively (24,68).
In order to calculate a practical rule of thumb for the quick use of the formula, we will assume a biological coefficient of variation (CV) for TgAbs of 8.5% (69). For the analytical CV of TgAb measurement we assume 20% (i.e., the functional sensitivity proposed as threshold for positivity). This allows for obtaining a method-independent value for the critical difference: 2.77×[(8.52+202)]1/2=53%. This value nicely correlates with the 50% drop used as the criterion in the article by Kim et al. (60). This formula can also be applied to specific TgAb assays, however, when the analytical coefficient of variation for a given level is known.
Based on the considerations described above, the use of serum levels of TgAbs as a “surrogate tumor marker” has been mentioned in the literature (10,70), using this perhaps somewhat misleading term. Indeed, TgAbs cannot be considered a tumor marker, because the serum levels of TgAbs are not correlated with the tumor load of the patient, but rather indicate the activity of the immune system. Moreover, unlike Tg, the sensitivity of TgAbs as a surrogate tumor marker cannot be improved by intensive TSH stimulation (71). Furthermore the mere presence of TgAbs in serum has thus far not been conclusively shown to correlate with a worse or better overall prognosis (72 –76).
■
TgAb levels do not correlate with the tumor load. Changes in serum TgAb levels can be used as an imprecise surrogate marker of residual benign or malignant thyroid tissue.
■
When using TgAbs as a surrogate marker, the trend is more important than the absolute level. A consistent reduction in serum TgAb levels is an indication that the patient is likely free of disease. In contrast, a consistent rise of serum TgAb levels should raise the suspicion of recurrence. Unchanged serum TgAb levels must be regarded as indeterminate, although the risk of persistent disease or recurrence is higher in these patients than in those with decreasing TgAb levels.
2.3. Are there clinically useful alternatives to serum Tg and serum TgAb measurement that can be used as tumor marker in TgAb-positive DTC patients?
In the effort to establish alternative methods for the follow-up in TgAb-positive DTC patients, attempts have been made to identify circulating thyrocytes through measurement of thyroid-specific mRNA fragments, such as Tg mRNA, TSH-receptor mRNA, or thyroid peroxidase mRNA, in the mononuclear layer of centrifuged venous blood (77 –84). However, in the majority of studies, it proved impossible to define a cut-off with sufficient sensitivity and specificity for clinical use because Tg mRNA measurement is plagued by problems such as, for example, the so-called “illegitimate” transcription (85).
More recently, Boldarine et al. (86) reported the development of a quantitative Tg mRNA assay based on the use of RNA primers that are specific for regions of Tg mRNA not affected by alternative splicing. Using this assay, the authors were able to accurately distinguish patients with persistent or recurrent disease from the disease-free ones. Although such results are definitely encouraging, independent confirmation is required before this assay can be recommended.
Furthermore, alternative strategies based on known mutations have been tried, such as detection of the BRAF 1799T> mutation in peripheral blood of patients with these mutations (87). However, such other concurrent diseases such as melanomas (88) may cause false-positive results, and the detection of such mutations in circulation is limited to patients who have the particular mutation. Furthermore, thus far the detection of mutations in peripheral blood is currently not sufficiently sensitive for clinical use. Nonetheless, further research into the detection of known tumor-related mutations in the circulation of patients seems warranted and may be expanded to include other mutations such as the various RET/PTC mutations.
Alternatively, several techniques from other domains of oncology which have until now been insufficiently tested in DTC may be adapted for use in DTC patients such as the detection of circulating tumor cells (89 –91), detection of specific micro-RNA fragments (92 –98), or analysis of cancer cell exosomes (99,100).
■
Currently, there are no alternatives to Tg or TgAb measurement with both sufficient sensitivity and specificity for clinical use. Further development of alternative methods (e.g., by solving the problems affecting Tg mRNA measurement such as illegitimate transcription) is desirable, however.
2.4. What type of follow-up is appropriate for patients with TgAbs?
Based on the literature, it seems appropriate to differentiate follow-up based on the course of serum TgAb levels. As in any other DTC patient, appropriate follow-up during the first year consists of frequent visits (once every 3–6 months), and a high standard of assessment must be adhered to (11 –15). This involves measurement of concentrations of thyroid hormones, Tg levels, and TgAbs in addition to cervical ultrasound. Whether diagnostic radioiodine whole-body scintigraphy (dxWBS) should be performed to verify the complete ablation of thyroid tissue is a matter of discussion. Whereas according to some studies dxWBS is a prognostically and diagnostically useful procedure (101), other studies regard this procedure as superfluous (102,103). Ultimately, however, performing a dxWBS is a matter of physician preference until the responsible professional societies will deliver appropriate, evidence-based guidelines on this issue.
Decreasing TgAb levels
In patients in whom serum TgAb levels decrease strongly after ablation, a remission can be assumed and the follow-up may be less aggressive. In these patients, the indication for dxWBS would be similar to that of a patient with undetectable Tg and a negative TgAb test that is, the dxWBS should be performed no more than once, if not pathologic. Once TgAb levels have disappeared completely, further follow-up can take place in accordance with the guidelines.
Although rare, the reappearance of TgAbs during follow-up in such patients should prompt a strong suspicion of recurrence requiring an appropriate clinical work-up, which may include ultrasound of the neck, dxWBS and, if negative, additional imaging procedures.
A further relatively rare scenario that may nonetheless occur in clinical practice concerns the patient who shows decreasing TgAb levels that stabilize at some point during follow-up. In such patients the question arises whether this should be regarded as a sign of recurrence, or rather as a sign of a constitutive immune system activity. Here we would advocate that these patients be followed as any patient with TgAb levels that have a decrease from baseline; that is, after one negative dxWBS, these patients should be followed clinically by measurement of TgAbs and cervical ultrasound, as long as TgAb levels remain stable. Should they rise, however, this should then prompt the suspicion of recurrence and appropriate diagnostic measures should be taken.
Unchanged TgAb levels
In patients in whom serum TgAb levels neither rise nor fall considerably (<50%), the disease status is uncertain because the persistence of TgAbs may or may not indicate persistent disease. Therefore, a more intensive follow-up has to be considered. Since serum TgAb levels do not provide a sense of direction in these patients and serum Tg measurement cannot be used reliably, periodic dxWBS may well be the only method to ascertain the disease-free status, at least for tumor localizations outside of the neck. Considering the slow course of DTC and the burden that the procedure places on patients, it appears unreasonable to perform a dxWBS more often than once every 3 years and in most patients this interval can be considerably longer; individual factors such as age, sex, histology, and initial stage of disease should be considered when choosing the interval. Furthermore, it is questionable whether further dxWBS is useful once dxWBS is negative and no further indications of persistent or recurrent disease, such as an increase in TgAbs or pathologic findings on cervical ultrasound, are present.
Rising TgAb levels
In patients in whom serum TgAb levels rise after 131I ablation or therapy, progressive disease is likely. In addition to the routine cervical ultrasound in these patients, other diagnostic procedures, including radioiodine dxWBS and, if negative, further imaging methods, should be undertaken to identify the location of the tumor tissue. If a focus can be identified, appropriate therapeutic measures are warranted.
TgAb-positive patients with a differentiated microcarcinoma of the thyroid
In patients with a microcarcinoma (<1 cm) and TgAbs, additional difficulties are present. In these patients metastases are fortunately rare and, lacking evidence to the contrary, the prognosis for the whole group with regard to survival must be regarded as good as for microcarcinoma patients without TgAbs. According to various guidelines, these patients only require a resection of the affected thyroid lobe, without total thyroidectomy or 131I ablation (11 –15). Therefore, these patients will have a considerable thyroid remnant, making follow-up by Tg levels difficult even in patients without TgAbs, although a stable TG level in such a patient, in combination with formal neck ultrasound, is helpful in assessing whether there is concern for recurrent or progressive disease. However, in patients who are positive for TgAbs, Tg levels cannot be used reliably, and because there is still a thyroid lobe in place, the course of TgAb levels cannot be used either. Furthermore, radioiodine scanning will not yield any meaningful results because most radioiodine will be taken up by the remaining thyroid tissue, thereby obscuring any smaller lesions in its vicinity on a whole-body scan. Since there is no evidence in the literature that patients with TgAbs and a microcarcinoma of the thyroid have a poorer prognosis, there is no medical justification for a more elaborate or additional treatment than in those without TgAbs. However, for the follow-up of these patients, there currently remains no other option than to perform regular cervical ultrasound and, in case of a suspicion of metastasis, secure the diagnosis through a biopsy.
TSH stimulation testing
The goal of measuring Tg after stimulation through an elevated TSH is to maximize the sensitivity of Tg measurements for the presence of persistent or recurrent disease in a qualitative sense. Therefore, if Tg is detectable despite the presence of TgAbs (assuming that the TgAbs have not falsely increased Tg levels, which, as already described, is rare in modern IRMAs), TSH stimulation of Tg is unnecessary. In patients with undetectable Tg in the presence of TgAbs, the result of Tg stimulation testing is not reliable, as a negative stimulation test in the presence of TgAbs remains unreliable. Therefore, in TgAb-positive patients, there is no indication for TSH-stimulated Tg measurement. When TSH stimulation is performed for dxWBS or 131I therapy, stimulated Tg can be measured simultaneously but the physician should be aware of the restrictions on its reliability and usefulness.
■
In TgAb-positive patients, follow-up should be stratified according to the trend of serum TgAb levels.
■
In patients showing a strong decrease in serum TgAb levels, cervical ultrasound and regular measurements of TgAbs suffice.
■
In patients with persistent or increasing serum TgAb levels, dxWBS should be performed at periodic intervals during follow-up.
■
There is currently no evidence that patients with TgAbs and a microcarcinoma have a poorer prognosis and therefore would require more extensive treatment than those without TgAbs. Follow-up in these patients should therefore rely primarily on cervical ultrasound without radioiodine treatment or scanning.
■
In TgAb-positive patients, there is no indication for isolated TSH-stimulated Tg measurement.
2.5. Which imaging methods are appropriate for use in DTC patients with TgAbs?
As in DTC patients without TgAbs, cervical ultrasound is the primary imaging method of choice in DTC patients with TgAbs (11 –15). In patients without TgAbs, the combination of Tg and ultrasound may be sufficient for follow-up in most patients. Although neck ultrasound in expert hands is able to detect cervical lymph node metastases or local recurrences, it is unable to detect distant metastases in the lungs or elsewhere in the body.
Should cervical ultrasound reveal a suspicious lymph node, the usual procedure is to perform a fine-needle aspiration biopsy of this lesion. Some authors have also advocated measuring Tg in the aspirate to assist in the diagnostic process (104 –110). The latter procedure can also be performed without problems in TgAb-positive patients, because locally produced Tg levels in metastases are manifold higher than in the peripheral blood and usually exceed the blocking capability of antibodies. Moreover, in these measurements the exact level is not as important as the relative Tg level in comparison with peripheral blood.
Other diagnostic imaging modalities are able to identify larger, nodular metastases, but not the diffuse, miliary lung metastases often seen in papillary thyroid carcinoma. The latter can best be detected by means of dxWBS or post 131I therapy whole body scanning (rxWBS). Consequently, we believe that there is still a role for a dxWBS in the work-up of TgAb-positive patients. In many DTC patients without TgAbs the use of dxWBS is disputed (102,111,112), especially in low-risk patients. Indeed, in most DTC patients, the combination of sensitive Tg measurement and cervical ultrasound suffices. This is not possible in patients who are positive for TgAbs, however, because Tg is unreliable and ultrasound alone is not able to exclude extracervical disease. Therefore, as already detailed previously, we advocate performing a dxWBS at regular intervals as well as when a suspicion of recurrent disease arises. What exactly constitutes a “negative” dxWBS (e.g., whether uptake in the thyroid bed is pathologic or not) is a matter of discussion, which we leave to guidelines from the responsible professional societies. In patients who have a negative dxWBS but in whom the attending physician nonetheless has a strong suspicion of recurrence, it is accepted nuclear medicine practice to give a so-called “blind therapeutic activity” (113) in order to perform a rxWBS, because it is a well-established fact that rxWBS has a considerably higher sensitivity than dxWBS (113,114). The precise activity to be used for rxWBS lies in the hands of the attending nuclear medicine physician and should be chosen in accordance with the relevant guidelines of the responsible professional societies.
For those who prefer or have access to other radionuclides, dxWBS can also be performed using the gamma-emitter 123I (115 –117) or the positron emitter 124I (118,119), although both are more costly and, especially in the case of 124I, more difficult to come by than 131I.
[18F]fluoro-2-deoxyglucose (FDG) positron emission tomography combined with computed X-ray tomography (PET/CT) was recently shown to be useful for the detection of recurrences in patients with TgAbs by Seo et al. (36): in a number of patients, recurrences were detected in the neck, which had been missed by cervical ultrasound. In patients with persistent or increasing TgAb levels without a clear focus on dxWBS or rxWBS, the emergence of iodine-negative tumor foci should be assumed. A manifestation of the so-called “flip-flop” phenomenon has been described according to which iodine-negative DTC lesions are usually positive on FDG-PET/CT and vice versa (120 –124). As a consequence FDG-PET/CT is the imaging method of choice in 131I negative DTC patients, especially when TgAb levels increase and a recurrence is suspected. However, the considerable costs associated with FDG-PET/CT imply that it should be used as a secondary imaging modality in DTC patients after other modalities have yielded insufficient results. For the follow-up of known distant metastases, a less expensive conventional CT scan may suffice.
■
Cervical ultrasound is the primary imaging method of choice in patients with DTC, therefore this is also the case in those with TgAbs.
■
Sonographically suspicious lesions should be further analyzed by fine-needle aspiration biopsy. In TgAb-positive patients with DTC, it is still helpful to analyze the aspiration fluid for the presence of Tg.
■
In patients with persistent or increasing TgAbs, 131I dxWBS/rxWBS is the imaging method of choice for identifying persistent or recurrent disease. If available, dxWBS can also be performed using 123I or 124I.
■
In patients with persistent or increasing serum TgAb levels and negative radioiodine dxWBS/rxWBS, FDG-PET/CT is the imaging method of choice to identify radioiodine-negative tumor foci.
Directions for Future Research
During the discussion. and writing of this consensus statement, we were often forced to conclude that too little evidence is available to answer most technical and clinical questions surrounding the care of DTC patients with TgAbs. Further studies will be required to be able to come to “evidence-based” recommendations. Major questions for future research on the one hand concern technical matters, including the improvement of immunoassays to the point that TgAbs no longer interfere with measurements. However, on the other hand, because TgAbs may still cause a faster clearance of Tg, it is also imperative to research alternative follow-up measurements for DTC patients based on the detection of circulating cells, mRNA transcripts, or known mutations. Only the future will tell which method will eventually emerge as most promising replacement for Tg in patients with TgAbs.
Many clinical matters need to be researched as well. The prognostic value of TgAbs has a body of evidence supporting it, this evidence is retrospective, however, and therefore would require prospective validation. Prospective studies of TgAb-positive patients will also allow a better evaluation of the biochemical and imaging methods to be used during follow-up. As with all prospective studies in DTC, the inherently favorable prognosis in most patients will, however, make the organization of such studies very difficult because of the long time span needed.
Conclusion
The current literature does not provide sufficient data for the provision of definite and conclusive answers and recommendations in the care of TgAb-positive DTC patients. This consensus statement does, however, provide an overview of the available evidence. The resulting consensus expert opinion and the 26 clinical recommendations are soundly based on a meticulous discussion of this evidence by a group of experts.
The questions and answers discussed have been summarized in an algorithm for the management of TgAb-positive patients. This algorithm is presented in Figure 1.
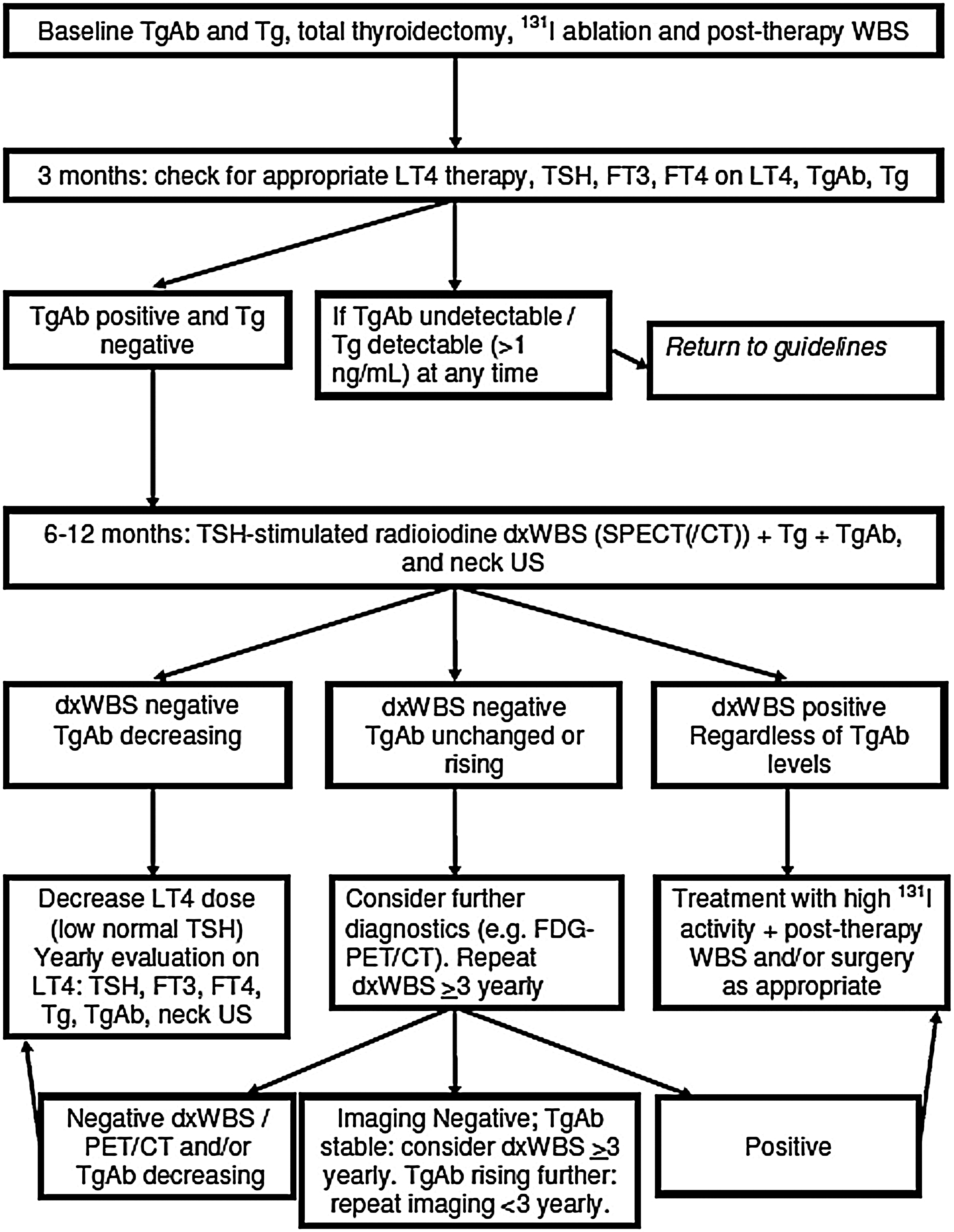
Proposed algorithm for treatment and follow-up in antithyroglobulin antibody–positive differentiated thyroid cancer patients. WBS, whole-body scintigraphy; LT4, levothyroxine; TSH, thyroglobulin; FT3, free triiodothyronine; FT4, free thyroxine; TgAb, antithyroglobulin antibody; Tg, thyroglobulin; dxWBS, diagnostic radioiodine whole-body scintigraphy; US, ultrasound; PET/CT, positron emission tomography combined with computed X-ray tomography.
Footnotes
Author Disclosure Statement
The Berlin meeting of experts described in this article was supported financially in part by Thermo Fisher Scientific Inc.; C.T. is an employee of B·R·A·H·M·S GmbH, Thermo Fisher Scientific Inc.