
Abstract
Background:
Prophylactic central neck dissection (pCND) at the time of total thyroidectomy (TT) remains controversial in clinically node-negative (cN0) papillary thyroid carcinoma (PTC). Despite occult central lymph node metastases being common, it is unclear if removing these metastases initially would reduce future locoregional recurrence (LRR). This systematic review and meta-analysis aimed at comparing the short-term LRR between patients who underwent TT with pCND and those who underwent TT alone.
Methods:
A systematic review of the literature was performed to identify studies comparing LRR between patients with PTC who underwent TT+pCND (group A) and those who underwent TT alone (group B). Inclusion criteria were cN0 patients, with each comparative group containing >10 patients, and with the number of LRR and mean follow-up duration available. The pooled incidence rate ratio (IRR) was used for calculating the LRR rate between the two groups. Other parameters evaluated included postoperative radioiodine (RAI) ablation, surgically related complications, and overall morbidity. Meta-analysis was performed using a fixed-effects model.
Results:
Fourteen studies matched the selection criteria. Of the 3331 patients, 1592 (47.8%) belonged to group A, while 1739 (52.2%) belonged to group B. Relative to group B, group A was significantly more likely to have postoperative RAI ablation (71.7% vs. 53.1%; odds ratio [OR]=2.60 [95% confidence interval (CI)=2.12–3.18]), temporary hypocalcemia (26.0% vs. 10.8%; OR=2.56 [CI=2.04–3.21]), and overall morbidity (33.2% vs. 17.7%; OR=2.12 [CI=1.75–2.57]). When temporary hypocalcemia was excluded, overall morbidity was similar between the two groups (7.3% vs. 6.8%; OR=1.07 [CI=0.78–1.47]). Group A had a significantly lower risk of LRR than group B (4.7% vs. 8.6%; IRR=0.65 [CI=0.48–0.86]).
Conclusions:
Group A was more likely to have postoperative RAI ablation, temporary hypocalcemia, and overall morbidity than group B. Temporary hypocalcemia was the major surgical morbidity in pCND and, when excluded, the overall morbidity appeared similar between the two groups. Although our meta-analysis would suggest that those who undergo TT+pCND may have a 35% reduction in risk of LRR than those who undergo TT alone in the short term (<5 years), it remains unclear how much of this risk reduction is related to increased use of RAI ablation and potential selection bias in some of the studies examined.
Introduction
One of the main reasons for the lack of evidence is that studies so far comparing TT+pCND with TT alone have not had the statistical power to detect a difference in LRR. A recent study estimated more than 5000 patients would be required to have sufficient statistical power to demonstrate a 25% reduction in LRR with pCND in patients with cN0 (12). To our knowledge, three meta-analyses have compared the outcomes between TT+pCND and TT alone. Two were not strictly relevant because one included patients with benign disease, while the other included patients who underwent therapeutic CND (9,10). Zetoune et al. pooled together five relevant studies and found a similar overall LRR rate between TT+pCND and TT alone (2.02% vs. 3.92%; odds ratio [OR]=1.05 [95% confidence interval (CI)=0.44–3.91]) (11). However, this study did not account for the difference in follow-up duration between the two groups. With an increasing number of new publications on this controversial subject in recent years, we conducted a systematic review and meta-analysis to compare the risk of LRR between TT+pCND and TT alone by reviewing the current literature.
Methods
This systematic review and meta-analysis was conducted in accordance with the PRISMA statement (13).
Search strategy
Studies comparing the rate of LRR between patients who underwent TT+pCND and TT alone were retrieved from the Scopus, Medline (PubMed), and Cochrane Library electronic databases on January 30, 2013. We used the following free-text search terms in “All fields”: (i) “central neck dissection” or “level VI neck dissection” or “neck dissection”; (ii) “papillary thyroid carcinoma”; (iii) i and ii.
There was no language restriction and no methodological filters. The bibliographies of three previous meta-analyses were searched for other additional relevant references (9 –11).
Study selection
All titles identified by the search strategy were independently screened by three authors (B.H.L., S.H.N., and K.P.W.). Search results were compared, and disagreements were resolved by consensus. Abstracts of potentially relevant titles were then reviewed for eligibility, and full-length articles were selected for closer examination if there was a specific description on CND in patients with PTC. The criteria for eligibility were as follows. First, any prospective or retrospective studies on patients with PTC only were included. Studies that analyzed differentiated thyroid carcinoma were considered if results of PTC were separately reported. Second, studies with two arms comparing LRR between TT+pCND and TT alone were included. Third, each study arm had to have >10 patients. Fourth, patients in either arm had to be cN0 by preoperative imaging and intraoperative examination; patients with cN1 or distant metastasis (M1) were not included. Finally, the number of LRR and the mean follow-up (in months) in each study arm had to be available. The reason for obtaining the mean follow-up period was because, in order to work out the pooled incidence rate ratio (IRR) for TT+pCND and TT alone groups, we had to first calculate the number of person-years in each respective arm. Studies that specifically reported the number of LRR and follow-up period in TT+pCND and TT alone as subgroups were included. Patients who underwent hemithyroidectomy with pCND or underwent simultaneous pCND and prophylactic lateral neck dissection were excluded. For studies that only provided the number of LRR without the mean follow-up duration or provided only the median and not the mean follow-up duration, the corresponding author of those studies was individually contacted for further information. Multiple reports of the same data set were assessed, and the most updated report of a study was included.
Data extraction
All data were extracted onto a standardized form. The primary data extracted from each article included type or design of study, first authorship, country of origin, year of publication, patient demographics, preoperative nodal assessment, method of selection for pCND, tumor characteristics, number of patients who underwent TT+pCND or TT alone, extent of pCND (unilateral vs. bilateral), number of normal and metastatic central LNs harvested, mean follow-up period, radioiodine (RAI) ablation given or not, number of LRR, operating time, volume of blood loss, and any surgically related morbidities. LRR was defined as a recurrence occurring in the thyroid bed, central and/or lateral compartments. A patient found to have distant recurrence only (i.e., without concomitant LRR) was not counted as a LRR, while a patient with concomitant LRR and distant recurrence was counted as a LRR. The percentage of recurrent laryngeal nerve (RLN) injury was calculated based on the number of patients. The overall morbidity rate was calculated by dividing the total number of patients who suffered one or more perioperative morbidity over the total number of patients. If a patient suffered from two or more morbidities, it was counted as one.
Statistical analysis
All the individual outcomes were integrated with the meta-analysis software Review Manager Software 5.0 (Cochrane Collaborative, Oxford, United Kingdom). LRR was assessed by IRR according to person-year of follow-up, and ORs were examined for the other surgical outcomes. All results were aggregated and analyzed using a fixed-effects model. A subgroup analysis of overall morbidity was performed excluding temporary postoperative hypocalcemia. Publication bias was estimated by Begg's rank correlation test and Egger's regression test (14,15). The meta-analyses in this study were conducted using R version 2.15.1 (R Foundation for Statistical Computing, Vienna, Austria) and the metafor package (16).
Results
Figure 1 shows the flowchart of studies retrieved and excluded. Of the 1822 titles initially identified from the database search, 41 full-length articles were assessed for inclusion, of which 27 were excluded and 14 studies were determined to be eligible and were included in this systematic review (7,17 –29). Appendix Table A1 lists these 27 articles (6,8,30 –54) and the reason for their exclusion. No additional study was found from our search of the three bibliographies in previous meta-analyses (9 –11). One study (8) was excluded, as it analyzed a subset of study subjects that were later recruited in a multicenter cohort study (25).
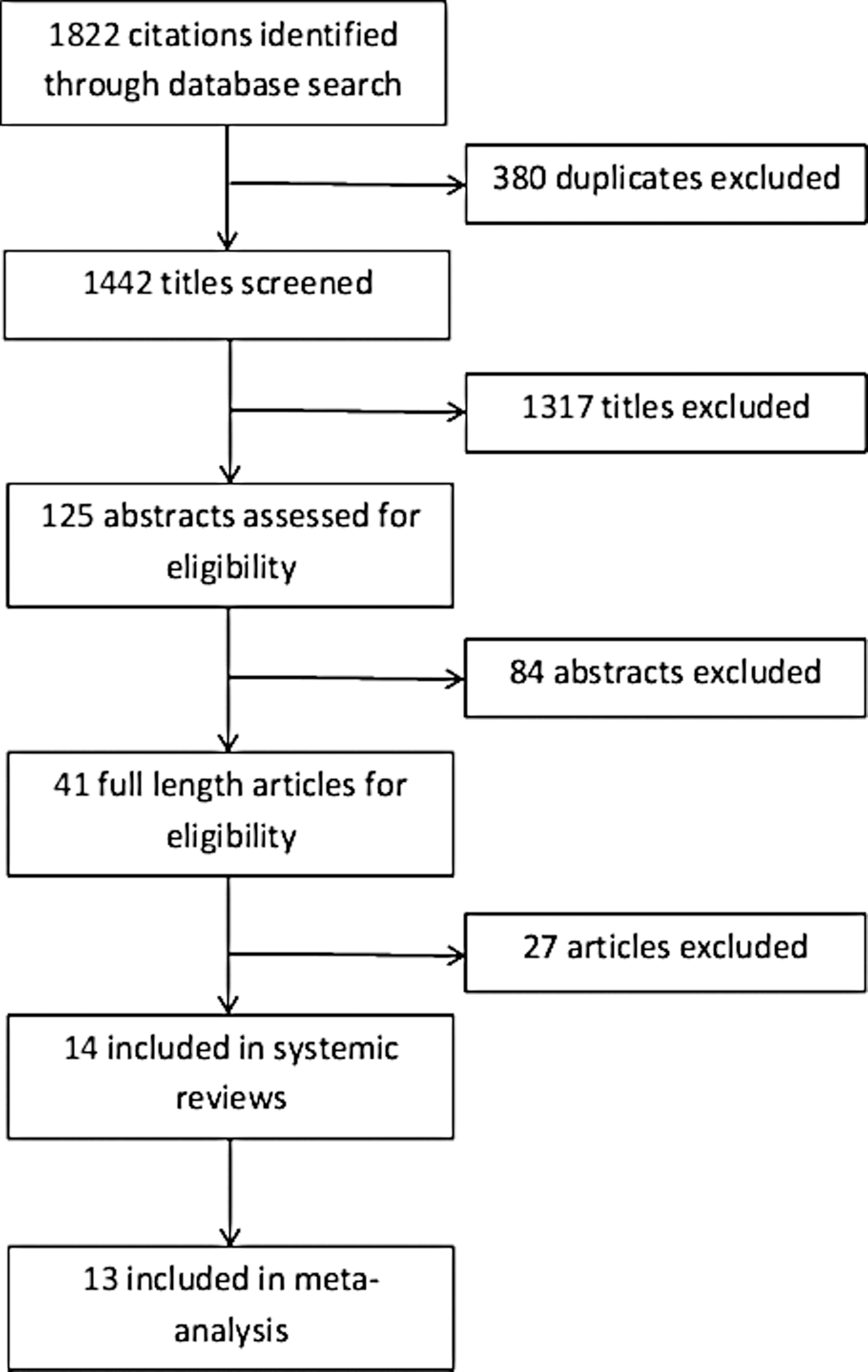
Flow diagram for study selection.
Baseline characteristics
Table 1 shows a comparison of the baseline characteristics between the 14 eligible studies. There was no randomized trial. Thirteen studies were retrospective, while one was prospective. Of the 3331 patients included, 1592 (47.8%) underwent TT+pCND (group A), while 1739 (52.2%) underwent TT only (group B). In terms of preoperative nodal assessment, ultrasonography (US) was used as the standard imaging modality in all studies, but only two studies specifically mentioned that both bilateral central and lateral neck compartments were examined (25,27).
Matching: 1=age; 2=sex ratio; 3=tumor size; 4=extrathyroidal extension; 5=tumor multifocality.
s, significantly different (p<0.05) between groups A and B; ns, not significantly different between groups A and B; na, not available or specified; LN, lymph node; LNM, lymph node metastasis; ETE, extrathyroidal extension.
In terms of selection for pCND, seven studies were based on individual surgeon's preference (7,18,22,24,25,27,28), while four studies did not specify their method of selection (17,19,23,26). Three studies used historical controls (TT alone) for comparison (20,21,29). Only 11 of 14 studies statistically compared age, sex ratio, tumor size, extrathyroidal extension, and tumor multifocality between the two groups (7,17,18,21 –26,28,29). Of these, two studies found age to be significantly older in group B (21,25), and three studies found tumor size to be significantly different (7,21,23). Two studies found tumor size to be significantly larger in group A (7,21), while one study found tumor size to be significantly smaller in group A (23). Three of nine studies found the rate of extrathyroidal extension to be significantly higher in group A (7,22,24), and two of nine studies found the rate of tumor multifocality to be significantly higher in group A (22,26). Bilateral pCND was performed in eight studies (17,18,22 –24,26,28,29), while the other six studies performed either unilateral or a combination of unilateral and bilateral pCND (7,19,20,21,25,27). Among the eight studies reporting bilateral pCND (17,18,22 –24,26,28,29), the mean number of central lymph nodes harvested ranged between 5.6 and 9.6, while the one study reporting unilateral pCND harvested a median of five (7). The incidence of central LNM in group A ranged from 23.5% to 82.4%, while in group B it ranged from 0.9% to 9.7% with 9 of 14 studies not reporting the incidence of central LNM in group B.
Surgical outcomes
Table 2 shows a comparison of outcomes between the two groups. Only 9 of the 14 studies reported whether RAI ablation was given after surgery (7,18,21 –24,26,27,29). Their dose ranged from 2.78 to 5.55 GBq. One study empirically gave the same dose of RAI, irrespective of the extent of LNM (7). The mean frequency of postoperative RAI ablation in groups A and B were 746/1041 (71.7%) and 498/937 (53.1%). Group A was significantly more likely to receive RAI ablation than group B (OR=2.60 [CI=2.12–3.18]). This was expected because of the higher incidence of central LNM (or N1a) in group A leading to tumor group upstaging in patients older than 45 years (28). Only 1 of 14 studies compared operating time between the two groups and found group B to have a significantly shorter operating time than group A (28).
The sum of all complications; same patient with more than two complications was counted as one.
Including two chyle leaks.
Figure 2 shows the forest plot for temporary hypocalcemia. Of the 14 studies, 11 studies compared temporary postoperative hypocalcemia between the two groups, while 10 studies compared permanent postoperative hypocalcemia in the two groups. In eight studies, permanent hypocalcemia was defined as persistent hypocalcemia and/or need for calcium supplements for more than six months (7,20,23 –28), while two studies defined it as more than 12 months (18,29). If one assumed all studies utilized a similar definition for temporary and permanent hypocalcemia, the overall temporary hypocalcaemia rate in group A was significantly higher than that in B (336/1294 (26.0%) and 144/1330 (10.8%), respectively; OR=2.56 [CI=2.04–3.21]) while the overall permanent hypocalcaemia was also similar between the group A and B (25/1254 (2.0%) and 15/1257 (1.2%), respectively; OR=1.74 [CI=0.87–3.50]).
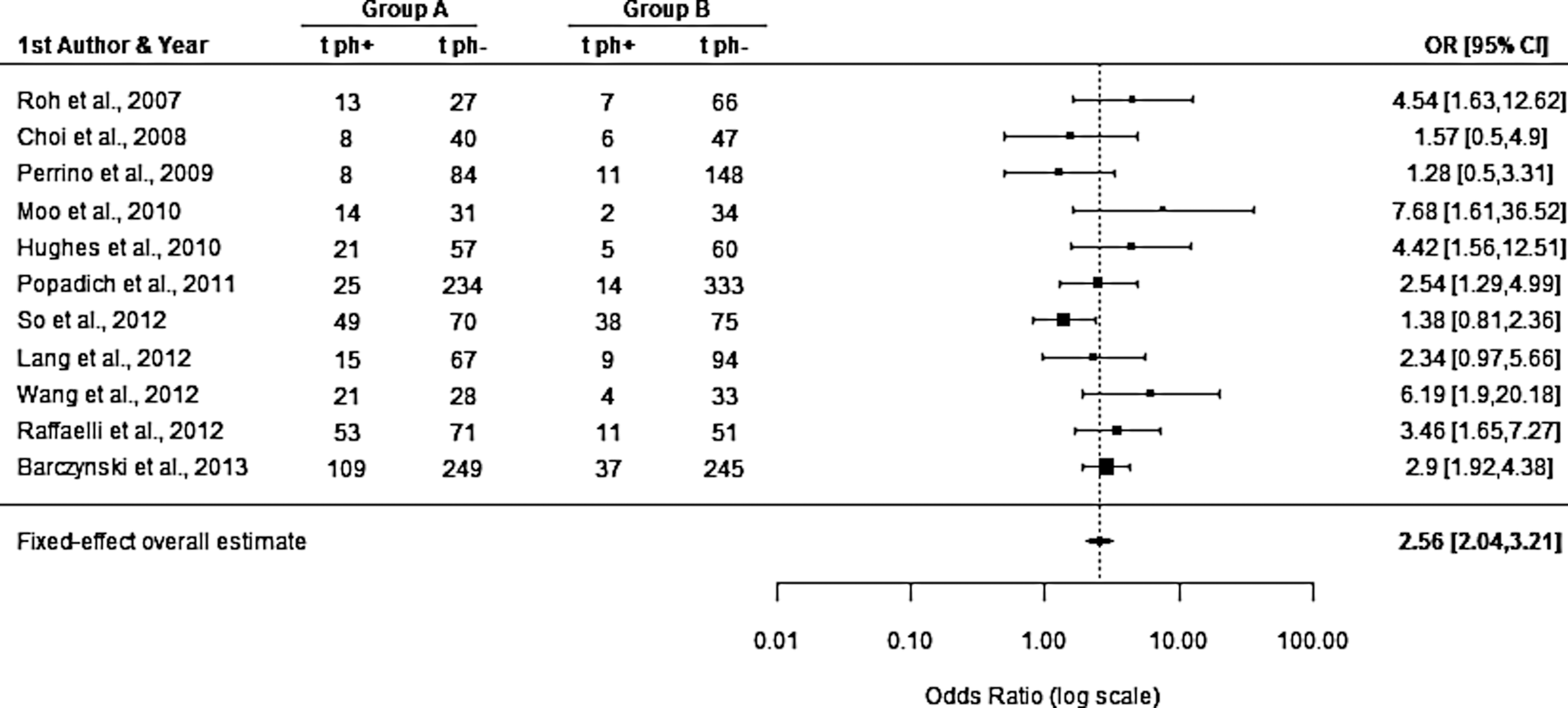
Forest plot for temporary hypocalcemia (tph). OR, odds ratio; CI, confidence interval.
Similar to hypocalcemia, the definition for temporary and permanent RLN injury varied between studies. Routine perioperative DL was performed in five studies (7,25,26,28,29), and persistent impairment in vocal cord function for more than six months was defined as permanent RLN injury in seven studies (19,23 –27). The cumulative temporary RLN palsy was comparable between group A and B (42/1294 (3.2%) and 41/1330 (3.1%), respectively; OR=1.02 [CI=0.64–1.64]). The cumulative permanent RLN palsy was also comparable between groups A and B (14/1197 (1.2%) and 21/1240 (1.7%), respectively; OR=0.75 [CI=0.37–1.55]).
The rate of hematoma was reported in eight studies. The cumulative hematoma rate was comparable between groups A and B (8/842 (1.0%) and 7/975 (0.9%), respectively; OR=1.33 [CI=0.53–3.35]). The wound infection/seroma rate was also similar between groups A and B (3/842 (0.4%) and 7/975 (0.9%), respectively; OR=0.78 [CI=0.28–2.07]). Figure 3 shows the forest plot for overall morbidity. The overall morbidity rate ranged between 14.3% and 53.8% in group A, while in group B it ranged between 11.0% and 40.7%. The overall morbidity after thyroid surgery in group A was significantly higher than in group B (430/1294 (33.2%) vs. 235/1330 (17.7%); OR=2.12 [CI=1.75–2.57]). However, after excluding temporary hypocalcemia, the overall morbidity in group A was not significantly different from group B (94/1294 (7.3%) vs. 90/1330 (6.8%); OR=1.07 [CI=0.78–1.47]). Figure 4 shows the forest plot for overall morbidity after excluding temporary hypocalcemia. The potential publication bias did not appear significant, as confirmed by the Begg analysis (Kendall's tau=−0.1636, p=0.5423) and the Egger regression test (z=−0.8921, p=0.4167).
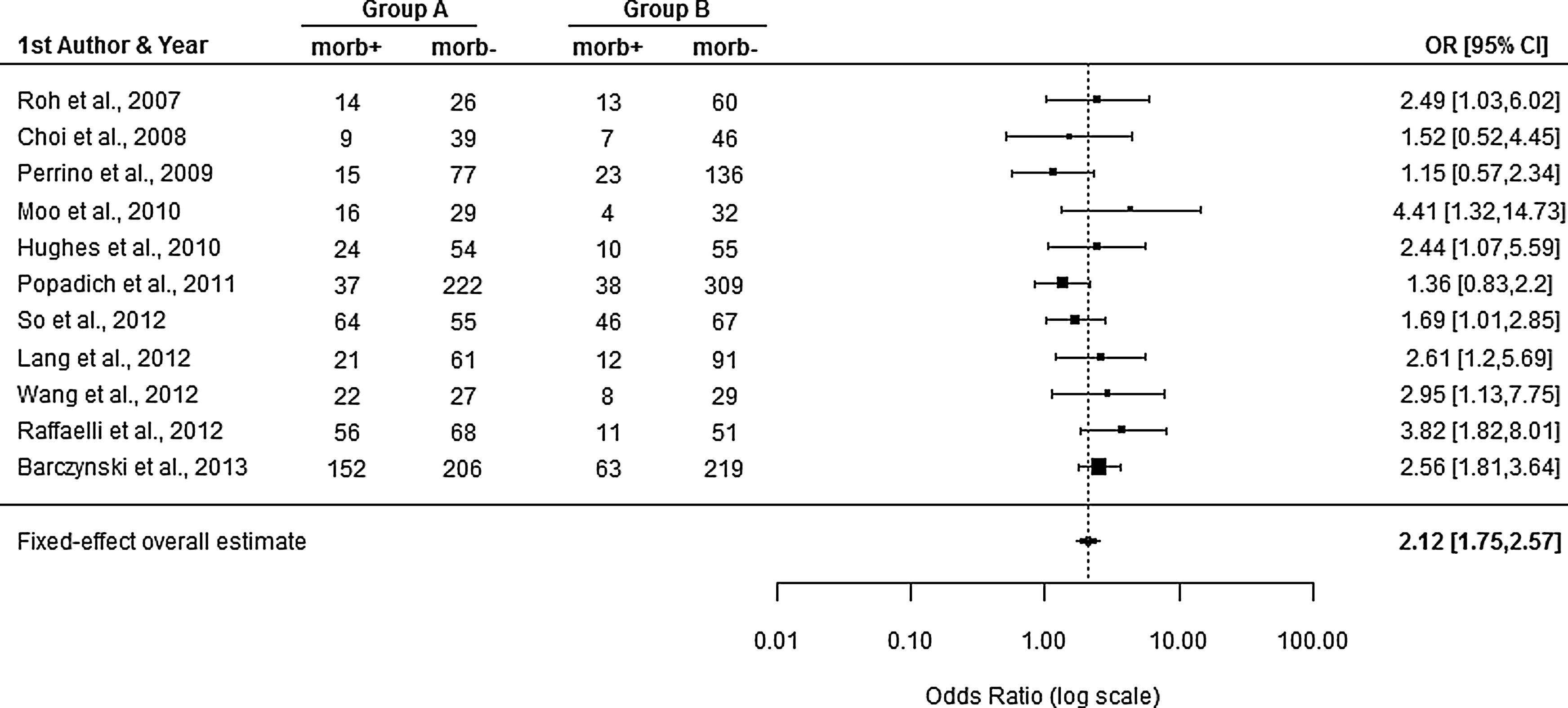
Forest plot for overall morbidity (morb).
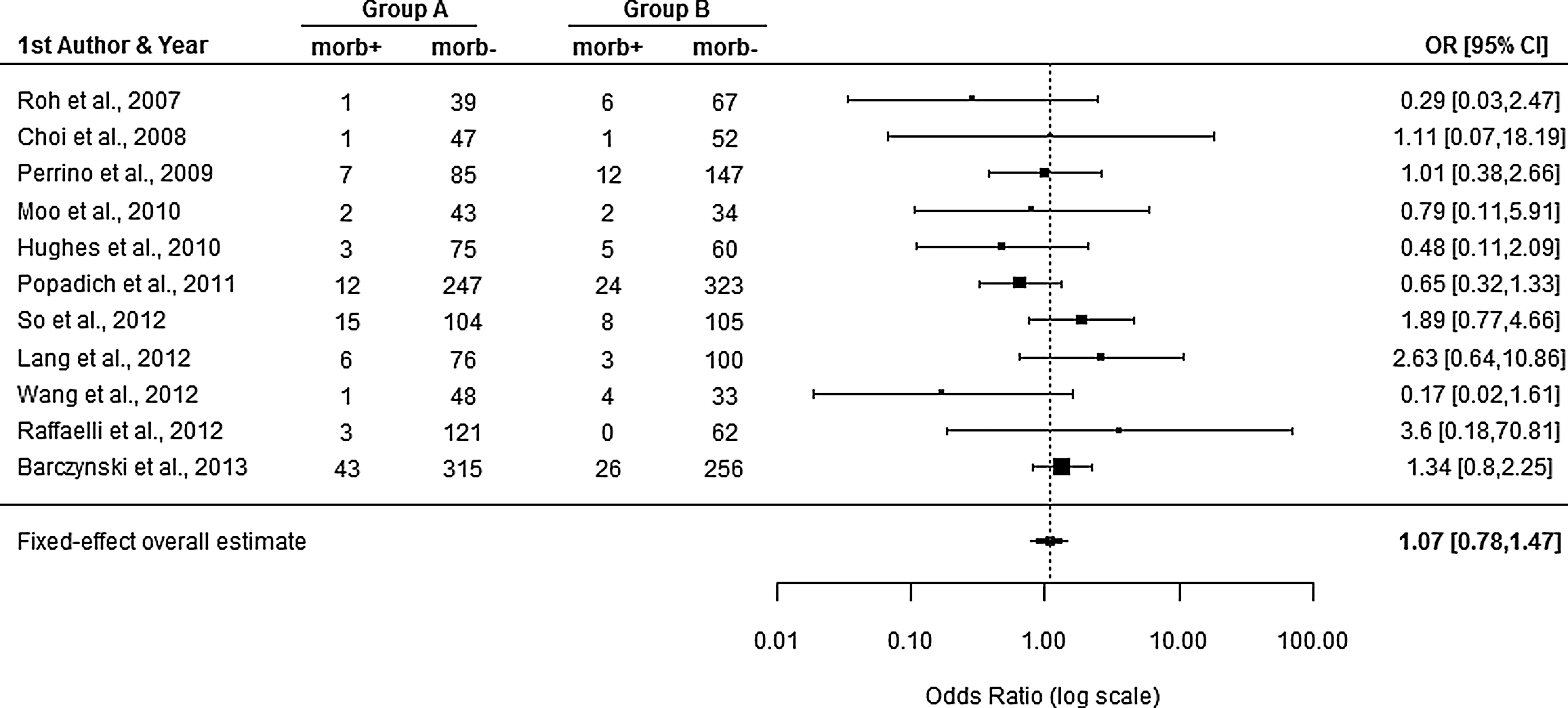
Forest plot for overall morbidity after excluding temporary hypocalcemia.
LRR
Table 3 compares the LRR rate between the two groups. One study was excluded in the IRR calculation because the mean duration of follow-up was not available (19). Figure 5 shows the forest plot for LRR. The pooled mean follow-up in groups A and B were 45.2 and 50.8 months, respectively, while the pooled mean number of person-years in groups A and B were 598.9 and 662.3, respectively. Group A had significantly lower LRR than group B (75/1592 (4.7%) vs. 149/1739 (8.6%); IRR=0.65 [CI=0.48–0.86]). The potential publication bias was not significant, as confirmed by Begg analysis (Kendall's tau=−0.1677, p=0.4268) and the Egger regression test (z=0.0984, p=0.9216).

Forest plot for locoregional recurrence (LRR).
Only medians were provided and therefore incidence rate ratio could not be calculated.
LRR, locoregional recurrence.
Discussion
To our knowledge, this is to date one of the largest meta-analyses evaluating the impact of pCND on LRR in patients with clinically nodal negative PTC or cN0. With significantly more patients being included than in previous meta-analyses, our data suggest that those who undergo TT+pCND have a 35% reduction in risk of LRR than those who undergo TT alone. Although no significant publication bias was found in our meta-analysis, as shown by the Begg's rank correlation test and Egger's regression test, it is worth nothing that there was one particular large recent study that could have had a profound impact on the overall IRR (29). In fact, its number of person-years in groups A and B were almost two to three times of that of the next largest study (25). Nevertheless, on the funnel plot (data not shown), this particular study was just on the margin of the funnel, and therefore it was not excluded from the final meta-analysis.
Despite this important positive finding, we remain cautious in our conclusions, as there are a number of potential limitations. First, the mean follow-up period was relatively short in one study, having a mean follow-up period of only 10 months. In fact, the overall mean follow-up duration for groups A and B was only 45.2 and 50.8 months, respectively, and hence both groups had a mean follow-up of less than five years. Given the fact that PTC is a relatively slow-growing, indolent tumor, patients may not develop detectable LRR until many years after the initial operation. Therefore, a significant longer follow-up duration would be necessary to assess fully whether pCND could significantly reduce LRR at least in the medium to long term (12). Apart from this, 13 of 14 studies were retrospective analyses, and so they were subject to selection bias. Surgeon's preference or discretion was mentioned in 7 of 14 studies as their method of selecting pCND, while four studies did not clearly describe their method of selection. Three studies actually used historical controls for outcome comparison (20,21,29). These selection biases were evident by the fact that only one of the five baseline characteristics (i.e., sex ratio) was consistently comparable in all studies. The other baseline characteristics such as age, tumor size, presence of extrathyroidal extension, and tumor multifocality were not consistently comparable, and since some of these could also potentially influence the risk of LRR, it was difficult to assess the real impact of pCND on LRR. Accounting for these factors in the multivariate analysis may help, but not all these characteristics were readily available for analysis. Perhaps the best way to resolve this would be to conduct a prospective randomized trial in the future. Although all studies did mention using US as a method for preoperative nodal assessment, it was difficult to assess the quality and the comprehensiveness of the assessment. This issue was particularly relevant in the three studies where historical controls were analyzed because quality of imaging tended to change with time. Furthermore, it was unclear from these studies what US criteria were used for deciding on fine needle aspiration or surgery.
In terms of other outcomes, similar to previous studies (7,24,27), we found the rate of postoperative RAI ablation was significantly higher in group A than B (71.7% vs. 53.1%, respectively; OR=2.60 [CI=2.12–3.18]). This can likely be attributed to the higher incidence of central LNM in group A relative to B. However, it is interesting to note that the incidence of central LNM varied widely from 23.5% to 82.4% between studies. Perhaps this is also a reflection of the quality of preoperative US assessment, and might also be a result of differences in the extent of the pCND and quality of the histological examination between studies (5,55,56). Moreover, similar to previous meta-analyses (9 –11), we found temporary hypocalcemia to be significantly higher in group A than B (26.0% vs. 10.8%, respectively; OR=2.56 [CI=2.04–3.21]). This would suggest that patients undergoing pCND during TT are 2.6 times more likely to develop temporary hypocalcemia than those undergoing TT alone. This is undoubtedly related to increased extent of surgical dissection leading to devascularization of parathyroid glands and/or inadvertent removal of parathyroid glands (7,17 –27). However, it is worth noting that the rate of permanent hypocalcemia, temporary and permanent RLN injury, hematoma, and wound infection/seroma were not similar between the two groups. In addition, even though the overall morbidity was significantly higher in group A than B (OR=2.12 [CI=1.75–2.57]), when this analysis was repeated with temporary hypocalcemia excluded, the overall morbidity was similar between group A and B (OR=1.07 [CI=0.78–1.47]). This finding implied that the majority of morbidity arising from pCND was actually related to temporary hypocalcemia rather than other surgically related complications.
Conclusion
The addition of pCND to TT resulted in a greater likelihood of administering postoperative RAI ablation, temporary hypocalcemia, and overall morbidity. However, since temporary hypocalcemia accounted for the majority of overall morbidity in patients undergoing pCND, when temporary hypocalcemia was excluded from overall morbidity, it was similar between the two groups. Although our meta-analysis would suggest that those who undergo TT+pCND may have a 35% reduction in risk of LRR than those who undergo TT alone in the short term (<5 years), it remains unclear how much of this risk reduction is related to increased use of RAI ablation and potential selection bias in some of the studies examined.
Footnotes
Author Disclosure Statement
All authors had nothing to disclose. No competing financial interests exist.
| First author | Journal | Year, country | Title | Main reason(s) for excluding from analysis |
|---|---|---|---|---|
| Henry (32) | Langenbeck's Archives of Surgery | 1998, France | Morbidity of prophylactic lymph node dissection in the central neck area in patients with papillary thyroid carcinoma | The TT alone group had patients with benign thyroid disease |
| Steinmuller (33) | Langenbeck's Archives of Surgery | 1999, Germany | Complications associated with different surgical approaches to differentiated thyroid carcinoma | Unable to separate some patients with follicular thyroid carcinoma and some who had therapeutic LND |
| Wada (34) | Annals of Surgery | 2003, Japan | Lymph node metastasis from 259 papillary thyroid microcarcinomas: frequency, pattern of occurrence and recurrence, and optimal strategy for neck dissection | Unable to separate some patients who underwent therapeutic CND |
| Gemsenjäger (35) | Journal of the American College of Surgeons | 2003, Switzerland | Lymph node surgery in papillary thyroid carcinoma | Unable to separate patients with therapeutic LND and lobectomy |
| Sywak (8) | Surgery | 2006, Australia | Routine ipsilateral level VI lymphadenectomy reduces postoperative thyroglobulin levels in papillary thyroid cancer | Data from this study were included in a later study (25) |
| Palestini (36) | Langenbeck's Archives of Surgery | 2008, Italy | Is central neck dissection a safe procedure in the treatment of papillary thyroid cancer? Our experience | Unable to exclude some patients with cN1; also no follow-up and recurrence data were available |
| Davidson (37) | Laryngoscope | 2008, United States | Papillary thyroid cancer: controversies in the management of neck metastasis | Unable to separate patients who had nodal plucking, therapeutic CND, LND, or combination |
| Hu (38) | Chinese Journal of Cancer | 2008, China | Application of central lymph node dissection to surgical operation for clinical stage N0 papillary thyroid carcinoma | No follow-up or recurrence data were reported |
| Sadowski (39) | Surgery | 2009, United States | Routine bilateral central lymph node clearance for papillary thyroid cancer | All patients who underwent CND had cN1 |
| Besic (40) | Annals of Surgical Oncology | 2009, Slovenia | Extent of thyroidectomy and lymphadenectomy in 254 patients with papillary thyroid microcarcinoma: a single institution experience | Too few (i.e., <10) patients in the prophylactic arm |
| Rosenbaum (41) | Archives of Otorhinolaryngology Head Neck Surgery | 2009, United States | Central neck dissection for papillary thyroid cancer | Unable to exclude patients with cN1 |
| Giles (42) | Surgery | 2009, Turkey | The long term outcome of papillary thyroid carcinoma patients without primary central lymph node dissection: expected improvement of routine dissection | Only included patients who underwent TT without CND |
| Bonnet (43) | Journal of Clinical and Endocrinology Metabolism | 2009, France | Prophylactic lymph node dissection for papillary thyroid cancer less than 2cm: implications for radioiodine treatment | Prophylactic LND were included; also no TT alone group was available for comparison |
| Lim (44) | British Journal of Surgery | 2009, Korea | Central lymph node metastases in unilateral papillary thyroid microcarcinoma | No TT alone group was available for comparison |
| Shen (45) | Surgery | 2010, United States | Central neck lymph node dissection for papillary thyroid cancer: the reliability of surgeon judgment in predicting which patients will benefit | All patients had therapeutic CND |
| Chung (46) | Journal of the Korean Surgical Society | 2010, Korea | Is central lymph node dissection mandatory in 2 cm or less sized papillary thyroid cancer? | All patients had lobectomy |
| Shindo (47) | Archives of Otorhinolaryngology Head Neck Surgery | 2010, United States | Total thyroidectomy with and without selective central compartment dissection | The TT alone group had benign thyroid disease |
| Bozec (48) | European Archives of Otorhinolaryngology | 2011, France | Clinical impact of cervical lymph node involvement and central neck dissection in patients with papillary thyroid carcinoma: a retrospective analysis of 368 cases | TT alone group was not available; also some patients had therapeutic CND or LND |
| Forest (49) | Annals of Surgery | 2011, Australia | Central compartment dissection in thyroid papillary carcinoma | No TT alone group was available for comparison |
| Mitra (50) | Journal of Laryngology and Otology | 2011, United Kingdom | Effect of central compartment neck dissection on hypocalcaemia incidence after total thyroidectomy for carcinoma | No follow-up or recurrence data reported |
| Teixeira (6) | Surgery | 2011, Brazil | The incidence of central neck micrometastatic disease in patients with papillary thyroid cancer staged preoperatively and intraoperatively as N0 | No TT alone group for comparison |
| Kutler (51) | Head and Neck | 2012, United States | Routine central compartment lymph node dissection for patients with papillary thyroid carcinoma | Unable to exclude patients who had hemithyroidectomy and CND; also some therapeutic LND were included |
| Hyun (52) | Annals of Surgical Oncology | 2012, Korea | Impact of combined prophylactic unilateral central neck dissection and hemithyroidectomy in patients with papillary thyroid microcarcinoma | All patients underwent hemithyroidectomy |
| Zhang (53) | Journal of Clinical Endocrinology and Metabolism | 2012, China | Risk factors for neck nodal metastasis in papillary thyroid microcarcinoma: a study of 1066 patients | All patients underwent hemithyroidectomy |
| Hartl (54) | Annals of Surgery | 2012, France | Optimization of staging of the neck with prophylactic central and lateral neck dissection for papillary thyroid carcinoma | All patients routinely underwent prophylactic CND and ipsilateral LND |
| Yoo (55) | World Journal of Surgery | 2012, United States | Level VI lymph node dissection does not decrease radioiodine uptake in patients undergoing radioiodine ablation for differentiated thyroid cancer | Unable to separate some patients who underwent therapeutic CND |
| Giordano (56) | Thyroid | 2012, Italy | Complications of central neck dissection in patents with papillary thyroid carcinoma: results of a study on 1087 patients and review of the literature | No follow-up or recurrence data reported |
TT, total thyroidectomy; cN1, clinically involved lymph node metastases; LND, lateral neck dissection; CND, central neck dissection.