
Abstract
Objective:
To investigate whether elevated and sequential changes in serum antithyroglobulin antibody (TgAb) levels are indicators of recurrence or persistence of papillary thyroid cancer (PTC) in patients with undetectable thyroglobulin.
Methods:
In 56 patients followed for more than 7 years, we recorded all serum TgAb levels (except the ones determined within one year after 131I therapy or diagnostic scans) and evaluated their disease status. All patients had undergone total thyroidectomy and remnant ablation by 131I, and they were positive for TgAb and had undetectable thyroglobulin during follow-up. The sequential changes of TgAb were defined as persistently high, increasing, persistently medium, decreasing, and decreasing to negative. Recurrence or persistence of PTC was defined as active disease as assessed by 131I scanning, 18F-fluorodeoxyglucose positron emission tomography, ultrasonography, computed tomography, or surgical examination.
Results:
Of the 56 patients enrolled, 10 patients had persistent PTC and 12 patients had recurrent PTC at more than 1 year after total thyroidectomy and 131I therapy. TgAb was persistently high in 4 patients (3 with active PTC), increasing in 6 patients (4 with active PTC), persistently medium in 16 patients (12 with active PTC), decreasing in 5 patients (none with active PTC), and decreased to negative in 25 patients (3 with active PTC). According to the trend, the patients with persistently high TgAb, increasing TgAb, and persistently medium TgAb had active disease more often (p<0.001). In the multivariable regression analyses, the trend of TgAb change was a strong predictor of PTC activity (p<0.001, R 2=−0.501). The most common diagnostic procedures performed for active disease were neck ultrasonography (21 patients) followed by 18F-fluorodeoxyglucose positron emission tomography (11 patients). The patients with autoimmune thyroid disease had better prognoses than did the patients without autoimmune thyroid disease (18% active PTC vs. 53% active PTC, p=0.02).
Conclusion:
The presence of TgAb is indicative of an active tumor. Sequential TgAb change is a good predictor of disease prognosis and is helpful for clinical decision making.
Introduction
T
Subjects and Methods
Subjects
In this retrospective study, we enrolled 56 patients (49 women and 7 men, mean age 54.0±13.6 years, mean age at diagnosis 42.9±12.0 years) found to have PTC who underwent total thyroidectomy and neck lymph node sampling, followed by immediate 131I remnant ablation at the Endocrinology and Metabolism outpatient clinics of Kaohsiung Chang Gung Memorial Hospital from January 1990 to December 2005. More than 15 sequential measures of Tg antibody were done for each patient. TgAb ≥50 IU/mL was defined as TgAb positive, and TgAb <50 IU/mL was defined as TgAb negative. After total thyroidectomy and neck lymph node sampling, Tg and TgAb measurements were performed in all patients every three months. They were all positive for TgAb one year after surgery and had an undetectable Tg for more than seven years. We excluded the TgAb measurements performed within one year after 131I therapy or a 131I diagnostic scan to avoid inclusion of transient positive TgAb. Patients with anaplastic carcinoma or with poorly differentiated thyroid cancer (such as the insular, tall cell variant) were excluded. We also excluded 62 patients with detectable Tg and positive TgAb after 1 year of surgery. All the 56 enrolled patients underwent 18F-fluorodeoxyglucose positron emission tomography (18F-FDG PET), neck ultrasonography, 131I whole-body scan, and computed tomography (CT), or magnetic resonance imaging (MRI), or both during follow-up. This study was conducted according to the guidelines outlined in the declaration of Helsinki, and the protocol of this study was approved by the Ethics Committee of Chang Gung Memorial Hospital.
A Tg antibody titer of >500 IU/mL was considered persistently high, 100–500 IU/mL was considered persistently medium, and 50–100 IU/mL was considered low.
TgAb trend definitions
1. Persistently high TgAb: >500 IU/mL, even with fluctuation.
2. Increasing TgAb: from low to medium, medium to high, or from low to high level. The slopes of TgAb changes were positive in all periods.
3. Persistently medium TgAb: ≥100 and ≤500 IU/mL, excluding the increasing and decreasing TgAb patterns.
4. Decreasing TgAb: from high to medium, from high to low, or from medium to low. The slopes of TgAb changes were negative in all periods.
5. Decreased to negative: TgAb decreased to <50 IU/mL during follow-up or low-grade fluctuation occurred, with TgAb levels between 100 and <50 IU/mL. The slopes of TgAb changes were negative in all periods.
We grouped the patients of trends 1, 2, and 3 together as the nondecreasing TgAb group and patients of trends 4 and 5 as the decreasing TgAb group.
Definition of persistent or recurrent disease
Active disease was defined as recurrence or persistence of PTC as assessed by 131I scan, 18F-FDG PET, CT, MRI, neck ultrasonography with cytological study, or surgical pathology.
Persistent disease was defined as the reappearance of disease within one year after complete ablation confirmed by neck ultrasonography with positive cytological or surgical histopathological findings or extracervical 131I uptake on whole-body scanning, 18F-FDG PET, MRI, or CT.
Recurrence was defined as the reappearance of disease one year after complete ablation of thyroid remnants confirmed by neck ultrasonography with positive cytology or histopathological findings or extracervical 131I uptake on whole-body scanning, 18F-FDG PET, MRI and CT. All patients were without evidence of disease at the first one-year follow-up period and underwent more than one instance of surgery or 131I ablation therapy after active PTC was revealed. The patients with autoimmune thyroid disease had serum thyrotropin-binding inhibitor immunoglobulin >15% or serum antimicrosomal antibodies >1:100.
Methods
Serum Tg, TgAb, and thyrotropin (TSH) were measured every three months during thyroxine supplementation. Serum Tg measurements were performed by radioimmunoassay (Tg IRMA; CIS-Bio International, Bagnols-sur-Cèze, France). The interassay coefficients of variation were 14.6%, 4.6%, and 6.2% at low, medium, and high concentrations, respectively. The intra-assay coefficients of variation were 7%, 2.4%, and 1.8% at low, medium, and high concentrations, respectively. The detection limit was 0.2 ng/mL. TgAbs were measured by a competitive radioimmunoassay (TgAb RIA CT; Biocode, Liége, Belgium). The sensitivity was 15 IU/mL, and <50 IU/mL was considered a negative finding. TSH was also measured by radioimmunoassay (RIA-gnost h-TSH; CIS-Bio International). The functional sensitivity was 0.2 μIU/mL, with a normal range of 0.25–4.0 μIU/mL.
Statistical analysis
Differences between the groups were analyzed using the Mantel–Haenszel χ 2-test. Multiple regression models were used to investigate the influence of disease activity. A probability value of <0.05 was regarded as significant. All statistical operations were performed using the SPSS for Windows (Version 11.5; SPSS, Chicago, IL).
Results
Comparison of disease activity
Of the 56 people enrolled in the study, only four patients had persistently high TgAb levels (one with inactive and three with active PTC). Only six patients had increasing TgAb levels (two with inactive and four with active PTC). Sixteen patients had persistently medium TgAb levels (4 with inactive and 12 active PTC [75%]). We grouped the patients within these three groups together as the nondecreasing TgAb group. Patients with decreasing TgAb (5 with inactive and none with active PTC) and patients whose TgAb decreased to negative (22 with inactive and 3 with active PTC [12%]) were grouped together as the TgAb decreasing group. Their clinical characteristics are given in Table 1. In the TgAb nondecreasing group, 27% of patients had inactive PTC, while 73% of patients had active PTC. In the decreasing TgAb group, only 10% of patients had active PTC, while 90% of patients had inactive PTC. The nondecreasing TgAb group had a significantly higher risk of persistence or recurrence of PTC (p<0.001, χ 2-test).
ATD (H/G), autoimmune thyroid disease (Hashimoto's thyroiditis/Graves' disease); P, persistence of papillary thyroid cancer; R, recurrence of papillary thyroid cancer; TgAb, antithyroglobulin antibody.
In the trend in which TgAb decreased to negative, the time lag between positive detection and the disappearance of TgAb was 1.7±1.3 years. Additionally, there were still 3 of 25 patients (12%) with persistently active PTC. They all had lung metastasis revealed by PET, but not by 131I uptake on whole-body scanning, after further 131I therapy, even when TgAbs were less than 50 IU/mL.
Active disease was not associated with age at diagnosis (p=0.22). In the active PTC group, 10 patients had persistent PTC and 12 patients had recurrent PTC (Table 2). The patients with recurrent PTC all belonged to the nondecreasing TgAb group; of them, three had increasing TgAb levels and nine had persistently medium TgAb levels. The most frequently used diagnostic procedures were neck ultrasonography (21 patients), followed by 18F-FDG PET (11 patients).
Papillary thyroid cancer persistent or recurrent after first surgery.
CT, computed tomography; MRI, magnetic resonance imaging; PET, 18F-fluorodeoxyglucose positron emission tomography; t1, persistently high; t2, increasing; t3, persistently medium; t4, decreasing; t5, decreasing to negative; U, ultrasonography; WBS, whole-body scan.
Comparison of PTC activity by initial TgAb titer
The initial TgAb titers (one year after 131I scan) were low in 13 patients (3 with active PTC and 10 with inactive PTC), medium in 31 patients (11 with active and 20 with inactive PTC), and high in 12 patients (8 with active and 4 with inactive PTC). The initial TgAb levels were higher in the nondecreasing TgAb group (p=0.02, χ 2-test; Fig. 1A) and were also higher in the patient group of persistent/recurrent PTC (p=0.05, χ 2-test; Fig. 1B).
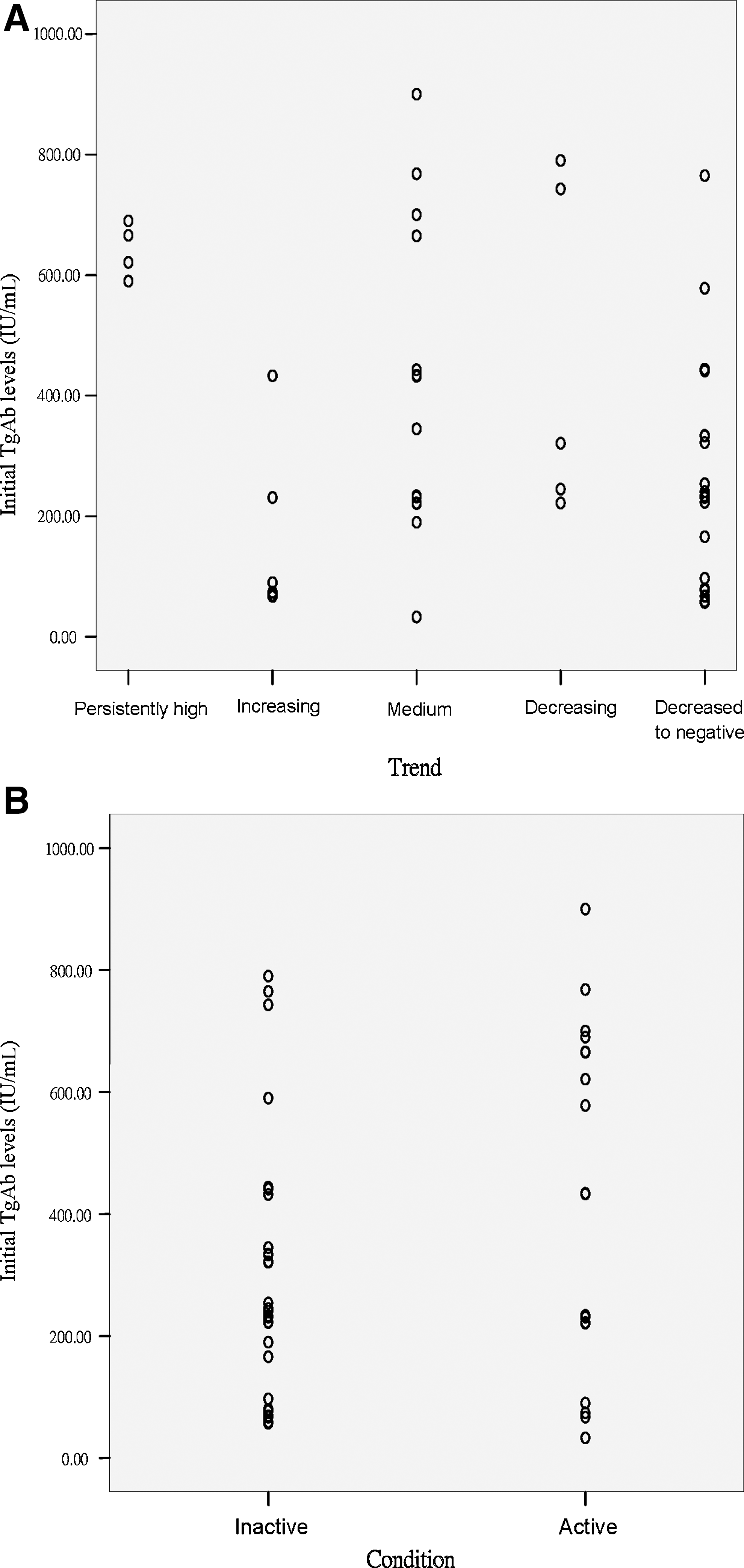
Initial TgAb levels for different TgAb trends by PTC activity. The initial TgAb levels are higher for persistently high TgAb levels (trend 1) and lowest for decreasing to negative (trend 5). The initial TgAb levels were higher in the nondecreasing TgAb group
Comparison of PTC activity by initial stage
According to AJCC 7th edition Tumor–Node–Metastasis (TNM) staging (10), of the 56 patients, 10 had stage 1 PTC (2 with active and 8 with inactive PTC; 2 in the nondecreasing TgAb group and 8 in the decreasing TgAb group), 16 patients had stage 2 PTC (5 with active and 11 with inactive PTC; 6 in the nondecreasing TgAb group and 10 in the decreasing TgAb group), 17 patients had stage 3 PTC (8 with active and 9 with inactive PTC; 10 in the nondecreasing TgAb group and 7 in the decreasing TgAb group), and 13 patients had stage 4 PTC (7 with active and 6 with inactive PTC; 8 in the nondecreasing TgAb group and 5 in the decreasing TgAb group). The initial tumor stage was higher in the nondecreasing TgAb group (p=0.02) and in the patient group of persistent/recurrent PTC (p=0.04).
Comparison of PTC activity among patients with autoimmune thyroid diseases
Thirteen patients had Hashimoto's thyroiditis (1 patient with persistently medium TgAb levels and 1 patient with decreasing levels, both of whom had active PTC, and 11 patients with conversion to negative TgAb levels, all who had inactive PTC). Nine patients had Graves' disease (one patient with persistently medium TgAb levels and one patient with decreasing TgAb levels, both of whom had active PTC, while the remaining seven patients had inactive PTC). The remaining 34 patients did not have autoimmune thyroid disease (18 had active PTC and 16 had inactive PTC). The patients with autoimmune thyroid disease had less persistent and recurrent PTC than did the patients without autoimmune thyroid disease (18% with active PTC vs. 53% active PTC, p=0.02). However, the prognoses did not differ between patients with Graves' disease and patients with Hashimoto's thyroiditis, (22% active PTC vs. 15% active PTC, p=0.10).
Multivariate analysis
To assess the effects of different predictive factors on PTC activity, we performed multiple linear regression analyses. The predictive markers included the TgAb trend, initial TgAb titer, and initial TNM stage. A change in TgAb trend was a strong predictor of PTC activity (p<0.001, R 2=−0.501; Table 3).
Dependent variable: activity of papillary thyroid cancer.
Discussion
We present the results of a longitudinal study in which we used a sensitive, direct radioligand assay for measurement of TgAb. We found that the change in TgAb trend significantly correlated with the prognosis of patients with PTC and undetectable Tg. Persistently high TgAb levels, increased TgAb levels, and persistently medium TgAb levels predicted poor PTC prognoses. The persistence of low TgAb concentrations years after the initial surgery and 131I ablation therapy was predictive of remission in the disease, especially when TgAb levels presented a declining trend and decrease to less than 50 IU/mL. One laboratory medicine practice guideline suggested that all specimens sent for Tg measurement require adjunctive TgAb testing because TgAb status can change from positive to negative or negative to positive, especially in patients with undetectable Tg (11). In the study by Soyluk et al. (12), patients with PTC and low recurrence risk still had high recurrence rates during long-term follow-up when they had positive TgAb tests.
The TNM stage at initial treatment is very important in estimating the prognoses for all cancers (10). In our present study, the nondecreasing TgAb group had higher initial TgAb levels and TNM stages. Nonetheless, among our patients with negative Tg combined with positive TgAb, the initial titer of TgAb and TNM stage seemed less important in predicting the prognosis of PTC because, after multivariable regression, only the TgAb trend was a statistically strong predictor of PTC activity. TgAb trends are suggested to be a more reliable surrogate DTC tumor marker than Tg, when TgAb concentrations are high and serum Tg concentrations (measured by RIA) are low (13). Therefore, sequential changes in serum TgAb levels rather than the initial TgAb titer or tumor staging are useful for prediction of clinical recurrence/persistence in Tg-negative patients with PTC.
In patients with autoimmune diseases, thyroid antibody production primarily arises in intrathyroidal lymphocytes. Persistence or increase in TgAb for a long period after thyroidectomy and 131I ablation therapy can reflect the persistence of Tg-producing tissue. TgAb may persist for many years without clear evidence of persistent disease. The half-life of TgAb after thyroidectomy is about 10 weeks and serum TgAb levels could be falsely high for more than 6 months after 131I therapy (4,14). We excluded TgAb data within one year after 131I treatment to exclude this possibility. However, we still found a few patients with initially positive TgAb, which persisted for about three years and then turned negative, as similarly reported by Chiovato et al. (6). The relationship between PTC and Hashimoto's thyroiditis has been investigated previously, and histopathological studies have shown that there is a higher prevalence of coexisting lymphocytic thyroiditis or Graves' disease in DTC patients. In the absence of lymphocytic thyroiditis, the presence of TgAb is rare (15 –17). Compared with the general population, in patients with DTC, especially PTC, the incidence of both TgAb and thyroid peroxidase antibodies is about twofold higher (2,18). Histological lymphocytic infiltration or serological detection of TgAb resulted in an almost threefold increased risk of PTC, but was associated with a favorable prognosis (14). Lymphocytic thyroiditis in PTC frequently causes mistakenly low or undetectable Tg. Therefore, in Tg-negative patients with PTC and lymphocytic thyroiditis, it is essential to determine TgAb. Nonetheless, in a retrospective study, a positive serum TgAb test was an independent predictor for thyroid malignancy in thyroid nodules, along with serum TSH levels, regardless of the presence of autoimmune thyroid disease (19). In the present study, we found that 39% of patients had autoimmune thyroid disease (23% with Hashimoto's thyroiditis), which is compatible with a previous report of 8–46% (14). Inactive PTC was more prevalent in patients with autoimmune thyroid disease, especially Hashimoto's thyroiditis.
18F-FDG PET is a good method to detect recurrent disease in patients with DTC who have increased TgAb levels with undetectable Tg levels and negative 131I whole-body scans (20). Periodic cervical ultrasonography is still a very important imaging modality in patients with PTC traditionally categorized as low risk and should be more frequent in patients who have positive TgAb tests (13). In our study, the detection rate with ultrasonography was higher than that of PET. The consensus statement from the American Society of Radiologists (21) reflects current technological improvements in neck ultrasonography used for the detection of thyroid nodules and assessment of lymph node chains and the thyroid bed. According to the European consensus for the management of patients with DTC, patients with undetectable Tg and positive TgAb tests should be monitored with periodic 131I diagnostic whole-body scanning and neck ultrasonography. CT, MRI, and 18F-FDG PET should be performed whenever there is suspicion of distant metastasis. This consensus also suggests that the disappearance of TgAb during follow-up may be considered as evidence of remission (22).
We conclude that sequential changes in TgAb are surrogate tumor markers in Tg-negative patients with PTC and more helpful for clinical decision making than initial TgAb levels. Nondecreased TgAb indicates active tumor existence and should be interpreted as evidence of PTC persistence or recurrence. Frequent clinical and imaging studies are indicated. Cervical ultrasonography may be a cost-effective monitoring procedure. Clinicians should be aware that the strongest indication for PTC relapse occurs with persistently elevated TgAb or progressively increasing TgAb levels measured over the long-term.
Footnotes
Author Disclosure Statement
No competing financial interests exist.