
Abstract
Background:
The management of Graves' disease (GD) in children is associated with a dilemma. Although the established initial treatment for GD in children is antithyroid drug (ATD) treatment, the remission rate in children is said to be lower than in adults, and severe propylthiouracil-induced adverse events (AEs) are an issue. Definitive treatments are effective, but they often result in permanent hypothyroidism and the need for lifelong T4 supplementation.
Objective:
The objective of this study was to investigate the outcome of ATD treatment, identify significant predictors of a remission, and evaluate the AEs of ATDs in a large pediatric population of GD patients.
Methods:
We retrospectively assessed the reports of 1138 children up to 18 years of age who had been newly diagnosed with GD at our institution between 1982 and 2006. Their median age at diagnosis was 16 years (range: 3–18 years), and there were 995 females and 143 males. All patients were initially treated with an ATD. Remission was defined as maintenance of euthyroidism for more than 12 months after discontinuing ATD treatment and the absence of any relapses during the follow-up period.
Results:
Of the 1138 patients, 723 continued on ATD treatment, 271 underwent surgery or radioactive iodine therapy, and 144 dropped out. Of the 723 patients who continued on ATD treatment, ATD treatment was subsequently ongoing in 84 and was discontinued in 639 (median duration of treatment: 3.8 years; range: 0.3–24.8 years). Of the 639 patients who discontinued ATD treatment, 334 (46.2%) achieved a remission, 247 (34.2%) experienced a relapse, and 58 (8.0%) dropped out. The cumulative remission rate increased with the duration of ATD treatment up until five years. No significant predictors of a remission were identified. The overall incidences of AEs associated with methimazole and propylthiouracil were 21.4% and 18.8% respectively. There were no fatal AEs in our population. While most AEs (91.6%) occurred within the first three months of ATD treatment, 2.7% developed more than two years after the start of ATD treatment. Seven of the eight late-onset AEs were induced by propylthiouracil.
Conclusion:
Long-term ATD treatment is a useful treatment option for GD in children.
Introduction
G
The management of GD in children is associated with a dilemma. The treatment options for hyperthyroidism in children include antithyroid drugs (ATDs), thyroidectomy, and radioactive iodine (RAI) therapy, the same as in adults. The first-line treatment for GD in children is ATD treatment. The GD remission rate in children treated with an ATD has been reported to be lower than in adults (15,19), and it is well known that ATDs give rise to adverse events (AE). The American Thyroid Association (ATA) and the American Association of Clinical Endocrinologists recently strongly recommended that methimazole (MMI) should be used to treat GD in children (20) because propylthiouracil (PTU) sometimes causes severe adverse events: liver failure and antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (21 –23). The definitive treatments—thyroidectomy and RAI therapy—are reliably effective, but they often result in permanent hypothyroidism and the need for lifelong thyroid hormone replacement therapy. Although the ATA has considered RAI therapy for children five years of age and over, the Japan Thyroid Association (JTA) and the Japanese Society of Pediatric Endocrinology have adopted a more cautious stance and do not recommend RAI therapy for children under 18 years of age because of concerns about RAI-associated carcinogenesis in the thyroid or other organs (24). Thus, there are fewer treatment options for GD in children in Japan, and it is necessary to depend on long-term ATD treatment.
The results of a meta-analysis of studies conducted in adult populations suggested that the optimal duration of ATD treatment is 12–18 months, and that if a remission is not achieved in 12–18 months, definitive therapy should be pursued (25). On the other hand, some studies have shown that remission rates increase over multiple years of treatment with ATD in children (2,4,17), and it remains uncertain whether the approach to the treatment of GD in adults described above is suitable in pediatric populations (26).
In this paper, we report a retrospective study of ATD treatment of GD in a large population of children (n=1138) up to 18 years of age who were treated at a single institution and followed for a long period of time.
Patients and Methods
Patient population
In this retrospective study, we reviewed the medical records of 1138 patients up to 18 years of age who were newly diagnosed with GD between 1982 and 2006 at Ito Hospital and who had been followed up for more than one year. The diagnosis of GD was based on high serum free thyroxine (fT4) and free triiodothyronine (fT3) levels and suppressed serum thyrotropin (TSH) level together with positive TSH receptor antibody (TRAb), positive TSH stimulating antibody (TSAb) test, or elevated and diffuse thyroid radioactive iodine uptake (RAIU). All patients were initially treated with an ATD. In most patients, the initial doses of MMI and PTU were 30 mg/day and 300 mg/day respectively, and in the others, the initial doses were based on the initial thyroid hormone level. The ATD dose was gradually reduced in a titration regimen. The ATD was discontinued if euthyroidism was maintained at a low dose (MMI 2.5–5 mg/day or PTU 25–50 mg/day) for more than six months and the TRAb level or TSAb level was near or within the normal range. Remission was defined as maintenance of euthyroidism for more than 12 months after discontinuing ATD treatment and the absence of any relapses during the follow-up period. Relapse was defined as elevated serum fT4 and fT3 levels together with suppressed TSH level and elevated TRAb/TSAb level or high RAIU.
We collected information about the following from the patients' medical records: age at diagnosis, sex, body mass index (BMI) score, body height and body weight standard deviation scores (SDS) at diagnosis, family history of autoimmune thyroid disease (AITD), Graves' ophthalmopathy diagnosed clinically, goiter size at diagnosis, interval until the fT4 and TRAb levels became normal, ATD-associated adverse events, and duration of ATD treatment. Goiter size was calculated by tracing the outline of the thyroid on tracing paper and using the Ohkubo formula (27), which is a modified version of the Allen–Goodwin formula. The following laboratory data were also collected: serum fT4, fT3, TSH, and TRAb levels at diagnosis.
Thyroid hormone and TRAb measurements were performed using different assay kits, depending on the time when the measurements were made. Although different reference ranges were obtained with each assay kit, the data were combined for use in the analyses because the differences were insignificant.
Statistical analysis
All statistical analyses were performed using JMP software (v8.0.1; SAS Institute, Cary, NC). The results for categorical variables are expressed as percentages, and the results for continuous variables are expressed as medians (25th–75th percentiles).
Univariate analysis
The characteristics of different groups were tested for statistically significant differences by Student's t-test when the values were for continuous variables, and by the chi-square test or Fisher's exact test when the values were for categorical variables.
Multivariate analysis
Multivariate model selection was based on a stepwise procedure, and a logistic regression analysis was used to identify the significant predictors of a remission. The variables used in the analysis were age at diagnosis, sex, duration of ATD treatment, family history of AITD, Graves' ophthalmopathy, BMI score at diagnosis, height and weight SDSs at diagnosis, goiter size at diagnosis, interval until the TRAb became normal, interval until fT4 level became normal, initial fT4 level, initial fT3 level, initial fT3/fT4 ratio, TRAb level at diagnosis, TRAb level at the end of ATD treatment, and the proportion of patients treated with PTU long term.
Results
The 1138 patients consisted of 995 (87.4%) females and 143 (12.6%) males. Their median age at diagnosis was 16 years (range: 3–18 years). Age and sex distributions are shown in Figure 1, which also shows that the incidence of GD increased with the age groups. All patients were initially treated with an ATD: 1119 patients were treated with MMI (median initial dose: 30 mg/day; range: 5–45 mg/day), and 19 patients were treated with PTU (median initial dose: 300 mg/day; range: 100–300 mg/day). The median overall follow-up period of the patients as a whole was 10.8 years (range: 1–28.4 years).
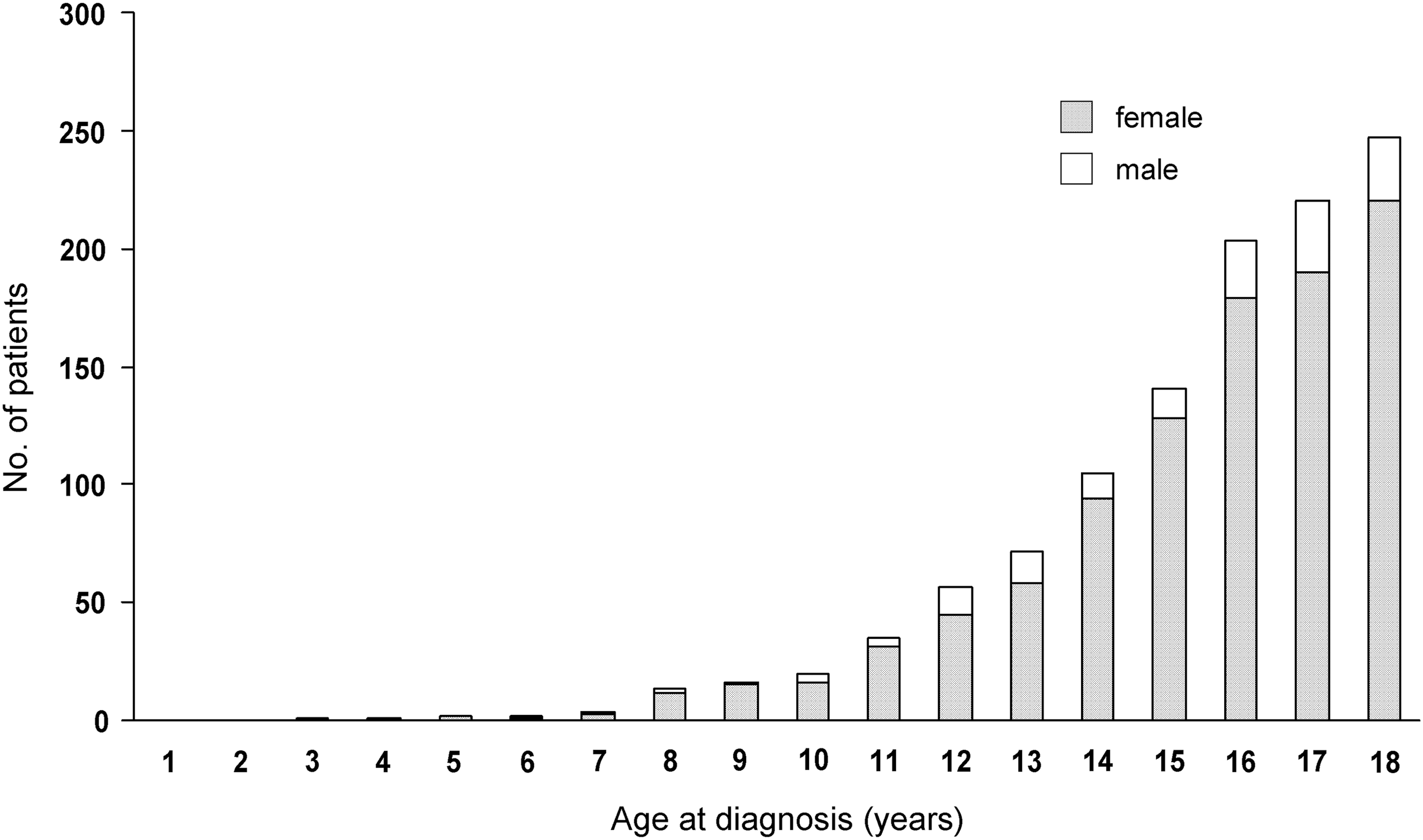
Distribution of children with Graves' disease (GD) according to age and sex at diagnosis. The 1138 patients consisted of 995 females and 143 males. Median age at diagnosis was 16 years (range: 3–18 years). The incidence of GD increased with the age group.
Figure 2 shows the clinical course of the 1138 patients. Of the original 1138 patients, 723 patients continued ATD treatment, 271 patients underwent definitive therapy before ATD treatment discontinuation based on the criteria as mentioned above, and 144 patients were lost to follow-up. Of the 723 patients who had continued ATD treatment, ATD treatment was subsequently ongoing in 84 (11.6%), and was discontinued in 639 (88.4%) based on the criteria (median duration of treatment: 3.8 years; range: 0.3–24.8 years). Of 639 who discontinued ATD treatment, 334 (46.2%) achieved a remission, 247 (34.2%) experienced a relapse, and 58 (8.0%) were lost to follow-up. The median follow-up period after discontinuing ATD was 5.8 years (range: 1.0–24.8 years) in the group who achieved a remission, 10.8 years (range: 0.3–27.2 years) in the group who experienced a relapse, and 0.4 years (range: 0–0.9 years) in the group who dropped out. Of the 271 patients who underwent definitive treatment, 218 had surgery (median time to surgery: 1.3 years; range: 0.1–16.1 years) and 53 had RAI therapy (median time to RAI therapy: 6.0 years; range: 0.1–17.2 years). The reasons for pursuing definitive treatment were doctor's recommendation (n=148), patient's preference (n=73), adverse events (n=42), noncompliance with ATD (n=6), and thyroid cancer (n=2). The cumulative remission rate increased with the duration of ATD treatment up until five years (Fig. 3A). Of the 247 patients who experienced a relapse, the relapse occurred in 130 (52.6%) within one year after discontinuing ATD treatment and in 182 (73.7%) within two years (Fig. 3B). Of the 247 patients who experienced a relapse, 32 patients subsequently underwent definitive therapy shortly after resuming ATD treatment: 19 patients went to surgery, and the other 13 patients received RAI therapy. The remaining 215 patients continued ATD treatment (Fig. 2).
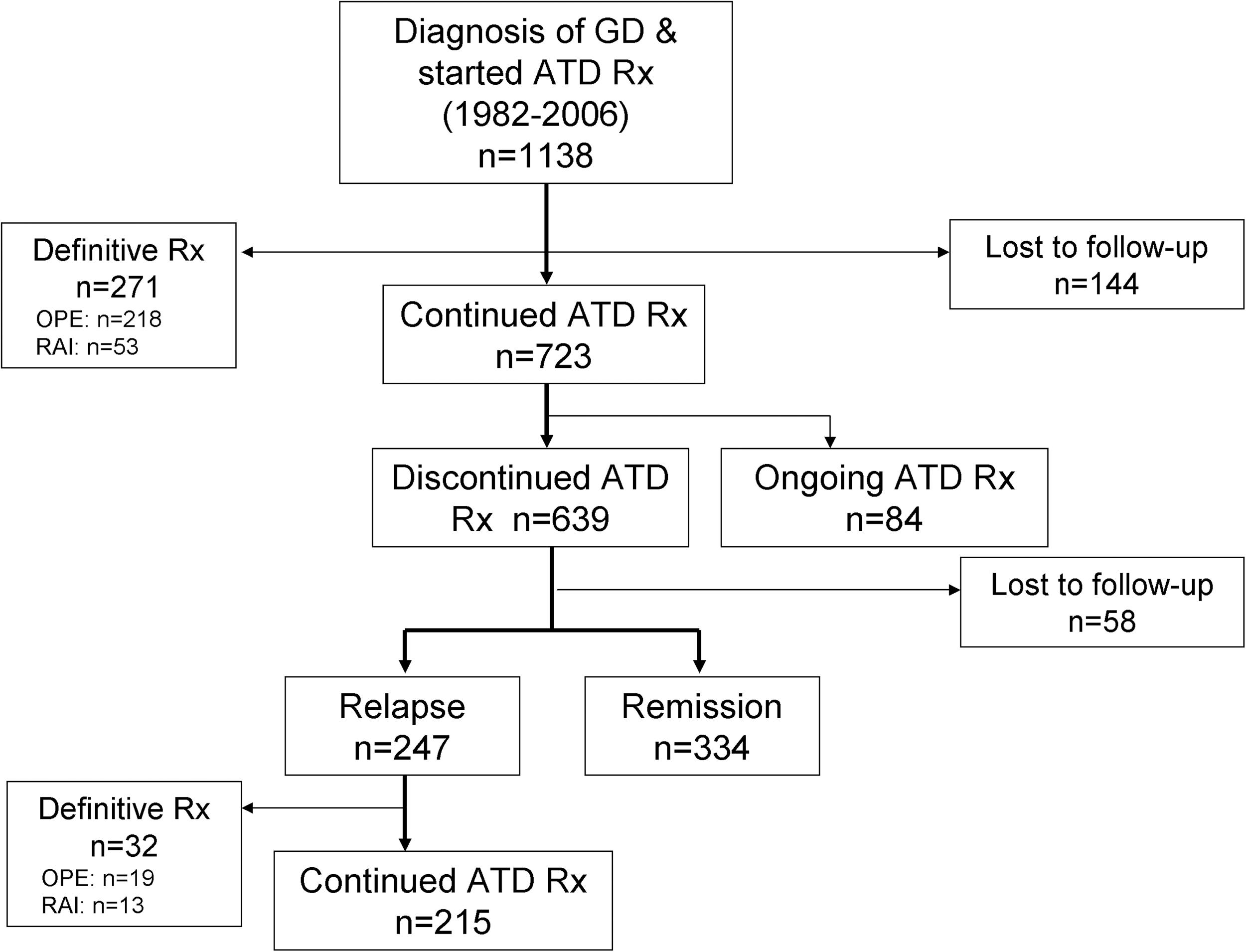
Clinical course of the 1138 pediatric patients initially treated with an antithyroid drug (ATD). Of the 1138 patients in the original population, 723 patients continued ATD treatment, 271 underwent definitive therapy before ATD treatment discontinuation based on the criteria, and 144 were lost to follow-up. Of the 723 who continued ATD treatment, ATD treatment was subsequently ongoing in 84 (11.6%) and was discontinued in 639 (88.4%). Of the 639 patients who discontinued ATD treatment, 334 (46.2%) achieved a remission, 247 (34.2%) experienced a relapse, and 58 (8.0%) were lost to follow-up. ATD, antithyroid drug; Rx, treatment; OPE, operation; RAI, radioactive iodine therapy.

Table 1 compares the clinical and biochemical parameters of four groups: the remission (REM) group, the relapse (REL) group, the ongoing ATD treatment (OAT) group, and the definitive treatment (DT) group. The proportion of males, TRAb level at diagnosis, initial fT3 level, and initial fT3/fT4 ratio were significantly higher in the OAT group than in the REM group and REL group, and the intervals until the fT4 and TRAb levels became normal were significantly longer in the OAT group than in the REM group. The only significant differences in the parameters between the REM group and the REL group were a lower proportion of patients treated with PTU and larger goiter size at diagnosis in the REM group. There were significant differences between the DT group and the other three groups because more than half of the patients in the DT group had been “selected” by their physicians to undergo definitive treatment shortly after the start of ATD treatment based on the presence of findings such as a large goiter, high thyroid hormone level, or persistent high TRAb level. In the DT group, the proportion of males and BMI score at diagnosis were significantly higher than in the REM group and REL group, and the age at diagnosis was significantly older than in the REL group.
p<0.05, ** p<0.01 vs. remission group; ‡ p<0.05, ‡‡ p<0.01 vs. relapse group; ¶ p<0.05, ¶¶ p<0.01 vs. continued group.
AITD, autoimmune thyroid disease; BMI, body mass index; SDS, standard deviation scores; TRAb, thyrotropin receptor antibody; PTU, propylthiouracil; ATD, antithyroid drug; fT3, free triiodothyronine; fT4, free thyroxine; ND, no data.
No significant predictors of remission were identified after adjustment for the other variables in the multivariate logistic regression analysis comparing the REM group to the REL group and OAT group (Table 2). Although the p-value for the difference in initial goiter size was 0.04, the differences were judged not to be highly significant because the 95% confidence interval included 1.00.
OR, odds ratio; CI, 95% confidence interval.
Adverse events were identified in 241 (21.4%) of the 1124 patients treated with MMI; they consisted of the 1119 patients initially treated with MMI and the five patients who were switched to MMI after initial treatment with PTU. Adverse events were found in 55 (18.8%) of the 292 patients treated with PTU; they included the 19 patients initially treated with PTU and the 273 patients who were switched to PTU after initial treatment with MMI (Fig. 4). Fortunately, none of the patients in this study experienced a fatal adverse event. The incidence of cutaneous reactions was significantly higher among the patients treated with MMI than among the patients treated with PTU (p<0.01). The incidences of liver dysfunction, neutropenia, and ANCA positivity were significantly higher among the patients treated with PTU than among the patients treated with MMI (p<0.01). There were no significant differences in the incidence of agranulocytosis or joint pain between the MMI group and the PTU group (Fig. 4). Liver dysfunction was induced by MMI and PTU in 22 patients, and it was mild and transient. The median levels of AST, ALT, and total bilirubin were 106 IU/L (range: 50–308 IU/L; reference range: 8–35), 187 IU/L (range: 94–620 IU/L; reference range: 5–40), and 0.55 mg/dL (range: 0.3–1.4 mg/dL; reference range: 0.2–1.2), respectively. There were no differences in liver enzyme levels or the intervals until liver dysfunction developed between the MMI group and the PTU group. The liver dysfunction improved after discontinuing ATD treatment, and no other clear cause of liver dysfunction besides the ATDs was identified. Of the five patients who became ANCA positive under PTU treatment, three had joint pain, one had both joint pain and subcutaneous nodes, and the other was asymptomatic. Only one of the five patients (the patient with both joint pain and subcutaneous nodes) required corticosteroid treatment, and the joint pain in the other three patients spontaneously resolved after discontinuing PTU. Of the 296 adverse events induced by MMI and PTU, 271 (91.6%) occurred within the first three months of ATD treatment. There were eight late-onset adverse events (2.7%), which developed more than two years after the start of ATD treatment (agranulocytosis, n=2; neutropenia, n=1; mild liver dysfunction, n=1; and ANCA positivity, n=4). Of these eight adverse events, seven were in patients treated with PTU. For MMI specially, 95.0% of the adverse events occurred within the first three months (Fig. 4).
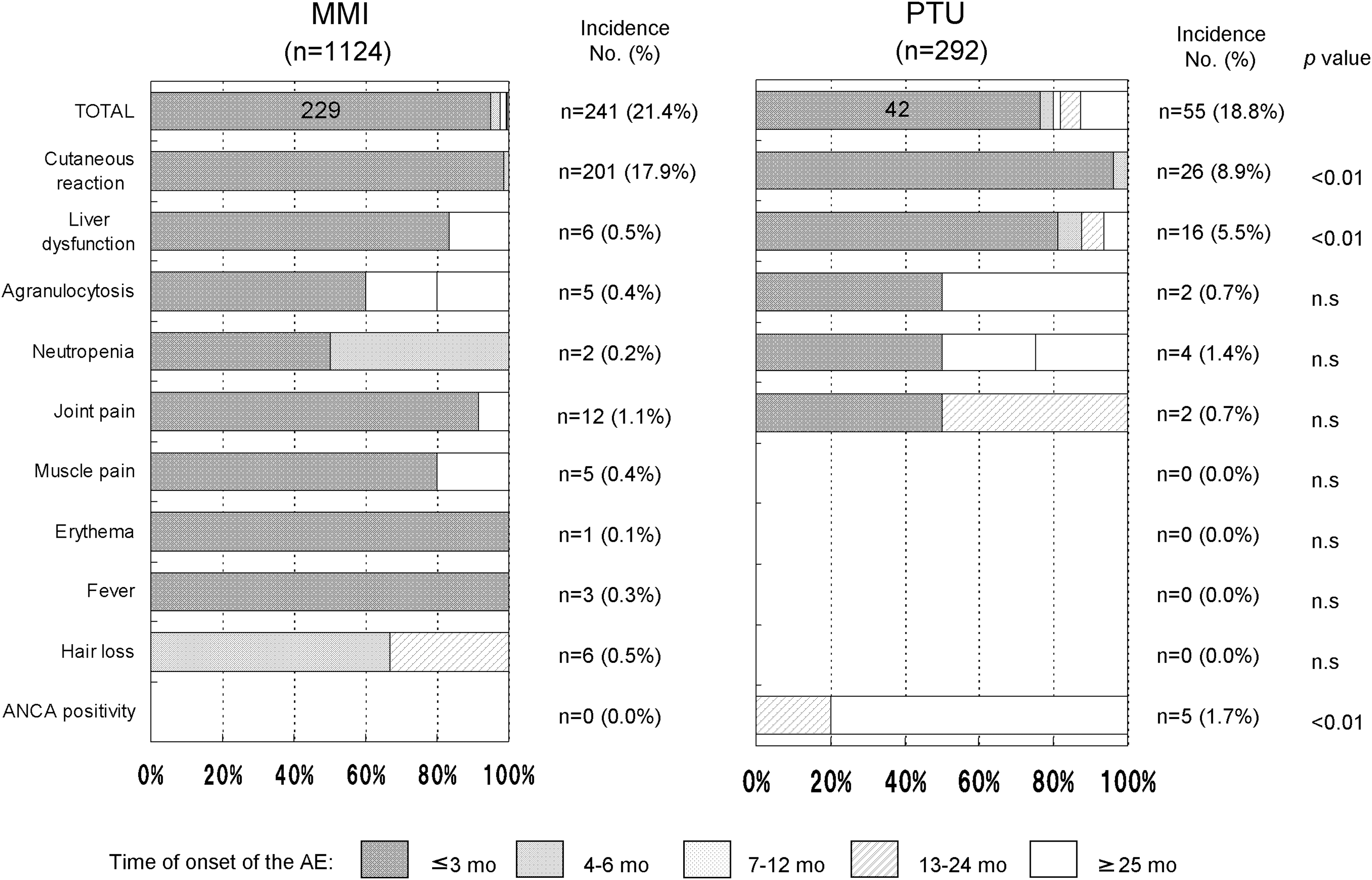
Incidence and time to onset of ATD-induced adverse events. The incidences of adverse events induced by methimazole (MMI) and propylthiouracil (PTU) were 21.4% and 18.8% respectively, and 91.5% (n=271) of the adverse events developed within the first three months after the start of ATD treatment and 2.7% (n=8) were late-onset cases that developed more than two years after the start of ATD treatment. Of the eight cases of late-onset adverse events, seven were induced by PTU. AE, adverse event; ANCA, antineutrophil cytoplasmic antibody; mo, month; n.s., not significant.
Discussion
Pediatric GD patients treated with an ATD are said to be less likely to achieve a remission than adults. The generally accepted GD remission rate in response to ATD treatment is 30% in children and 50% in adults (15). Retrospective studies have reported GD remission rates in response to ATD treatment in the 17%–40% range in children and adolescents (1 –3,5 –14), and four prospective studies have reported rates in the 29%–49% range (15 –18), whereas the rates reported in adult studies have been in the 39.5%–85% range (28 –32). Although the ATA recommends definitive treatment for children if a remission is not achieved after one to two years of MMI treatment (20), some studies have shown that long-term ATD treatment improved the outcome of pediatric GD. Leger et al. found that the remission rate was 49% in response to three two-year consecutive cycles of ATD treatment in cases in which hyperthyroidism relapsed after discontinuing ATD treatment (17). Lippe et al. reported an approximately 25% increase in remission rate for every two years that ATD treatment was continued (2). Our remission rate of 46.2% after a median duration of 3.8 years of ATD treatment (range: 0.3–24.8 years) was higher than in previous retrospective studies. The exclusion of the 271 patients who underwent definitive treatments from the calculation of the overall remission rate may have affected the overall remission rate, but they had to be excluded because it was impossible to know whether they would have achieved remission if they had continued ATD treatment. The cumulative number of remissions in our study increased with the duration of ATD treatment up until five years. Although definitive treatments are effective, they often result in permanent hypothyroidism and require lifelong T4 treatment. In addition, thyroidectomy is associated with a higher complication rate in children than in adults (20,33). In view of the fact that long-term ATD treatment of GD in children results in a high remission rate, it is not necessarily imperative that all children should undergo definitive therapy if a remission is not achieved after a one- to two-year period of ATD treatment.
In our study, 73.7% of relapses occurred within two years after discontinuing ATD, which is similar to a prospective study showing a relapse rate of 59% at one year after discontinuing carbimazole, and 68% at two years (15). These results suggested that hyperthyroidism recurs relatively soon after discontinuing ATD treatment, so regular checkups, particularly in the first one to two years after discontinuing treatment with an ATD, are important.
The factors predicting remission identified in previous retrospective studies of GD in children have been variable. A study by Glaser et al. identified a high BMI score and small goiter size at diagnosis as predictors of a remission (9), whereas a study by Mussa et al. identified low TRAb levels at diagnosis and duration of ATD treatment as predictors (4). The prognostic factors identified in prospective studies have also varied. Graser et al. reported a low fT3 level at diagnosis and normalization of thyroid function within three months as predictors of a remission (16). Kaguelidou et al. identified younger age, disease severity at diagnosis, and non-Caucasian as predictors of a relapse (15). Thus, no consistent predictors of a remission across populations have ever been identified. Moreover, the factors predicting remission identified by two studies conducted on the identical population were different, even though the only difference between the two studies was the duration of ATD treatment (15,17). There were differences among the studies in populaton size, analysis methods, and parameters measured, and those differences may have been responsible for the variety of the factors predicting remission identified. GD is generally thought of as a multifactorial disease, and the onset of GD is thought to depend on complex interactions among multiple genetic, environmental, and endogenous factors (34 –36). Similarly, the factors associated with remission may also vary from individual to individual.
No significant predictor of a remission was identified in our study population. One reason for the failure to identify any predictors of a remission may have been the limitations on data collection because it was a retrospective study. Deciding to switch to definitive treatment requires not only taking into account the various prognostic factors that have been identified, but also thoroughly considering the balance between the risks and benefits for the individual patient based on their background and clinical course.
The overall incidences of adverse events associated with MMI and PTU in this study were 21.4% and 18.8% respectively. These rates were similar to those reported in other studies in pediatric populations (5.1%–35%) (1,5 –8,10,13 –16,37), and they were not higher than in the Japanese adult population (13.9%–51.9%) (38,39). Most of the ATD-induced adverse events (91.6%) in our study developed within the first three months of ATD treatment, which is consistent with other studies that have also reported that most adverse events induced by ATD developed within the first six months (21,37). The JTA recommends a physical and biochemical checkup every two to three weeks in the first three months (40), and the frequent examinations may have resulted in overdiagnosis of noncritical transient ATD-induced changes as adverse events. However, it is important to make an effort to detect adverse events early, especially within the first several months.
In this study, PTU was found to be associated with a significantly higher incidence of liver dysfunction (p<0.01) and ANCA positivity (p<0.01) than MMI, but none of the adverse events was fatal. In children, the risk of PTU-induced liver failure requiring liver transplantation is about 1 in 2000–4000 (41). The patients treated with PTU were in the minority (n=292) because we have been preferentially prescribing MMI for children, as it is more effective than PTU in rapidly reducing thyroid hormone levels to the normal range (38,42). The small number of patients treated with PTU may be the reason for the absence of cases with serious liver failure in our population. The incidence of late-onset adverse events in this study was low (2.7%), and since most of the late-onset adverse events were induced by PTU, MMI is preferable for long-term treatment. Because the ATA recommends avoiding PTU as a treatment for GD in children (20), prescription of MMI for the treatment of GD in pediatric patients is expected to increase. Continuing careful monitoring of patients treated with MMI and persistent efforts to detect ATD-induced adverse events early, such as by regular checkups and educating patients and their guardians about adverse events, are imperative.
In conclusion, long-term ATD treatment is a useful treatment option for GD in children because our study shows that it results in a high remission rate (46.2%) and that the number of remissions increases with the duration of ATD treatment up until five years. However, vigilance is needed concerning ATD-associated adverse events throughout the ATD treatment period, and MMI is a preferable ATD for long-term treatment of GD in children.
Author Disclosure Statement
None of the authors has any conflicts of interest to disclose.