
Abstract
Background:
Recent data from a population-based study in children and adolescents suggest that serum thyrotropin (TSH) levels are associated with arterial blood pressure and hypertension. These results are in agreement with some but not all population-based studies in adults. Discrepancies in results might be explained by drug intake, different iodine supplies, and sizes of populations investigated. In addition, it is not clear whether an association between TSH and hypertension exists longitudinally or only cross-sectionally. Thus, our aim was to investigate cross-sectional and longitudinal associations between thyroid function and arterial blood pressure in a large consortium of cohort studies in adults.
Methods:
Data from five population-based studies were pooled resulting in 17,023 individuals being available for cross-sectional and 10,048 individuals for longitudinal analyses. Associations of baseline TSH with baseline blood pressure or hypertension were analyzed by multivariable median or logistic regression models. Multivariable median or Poisson regression models were used to investigate associations of baseline TSH with five-year change in arterial blood pressure or incident hypertension.
Results:
There was a cross-sectional positive association of TSH with arterial blood pressure (p<0.001) and hypertension (odds ratio [OR]=1.76 [confidence interval (CI) 1.24–2.50], p=0.002). Likewise, hypothyroidism was associated with systolic (β=1.1 [CI 0.1–2.1], p=0.040) and diastolic blood pressure (β=1.4 [CI 0.7–2.0], p<0.001). TSH, however, was not consistently associated with a five-year change in blood pressure or incident hypertension.
Conclusions:
High serum TSH levels were associated with current hypertension and blood pressure but not with a five-year change in blood pressure and incident hypertension. This argues for only a short-term effect of thyroid hormone levels on arterial blood pressure or a spurious association that needs further evaluation in population-based studies.
Introduction
Thus, current evidence for an association between serum TSH levels and arterial blood pressure is inconsistent, and previous studies might have been hampered by small sample sizes (3 –8), selection bias (2,8), and misclassification of antihypertensive drug intake (2 –8). Associations between serum TSH levels and arterial blood pressure might also depend on the iodine supply of the respective study region (9). Therefore we aimed to analyze the association between serum TSH levels and arterial blood pressure in a pooled population taken from five large population-based European studies conducted in regions with formerly mild to moderate iodine deficiency (10,11) comprising more than 17,000 individuals in total (12 –16).
While cross-sectional studies may reveal statistical associations between different parameters, the capacity of these studies to identify cause-and-effect relationships between parameters under investigation is limited. Unfortunately, studies investigating the association between thyroid function and blood pressure in a longitudinal design are scarce (17). A recent longitudinal study (17) including approximately 3000 adults failed to show an association between thyroid function and blood pressure. We opted to reinvestigate the prospective association between thyroid function and blood pressure in a larger study population using a longitudinal design with data from four out of the five studies that were used for our cross-sectional analyses. For the longitudinal analyses, more than 10,000 adult individuals were available.
Materials and Methods
Study population
Data from four population-based cohort studies and one population-based cross-sectional study were used for the present analyses: Study of Health in Pomerania (SHIP) (16), the Rotterdam Study (13), INTER99 (14), Cardiovascular disease, Living and Ageing in Halle (CARLA) (12), and Kooperative Gesundheitsforschung in der Region Augsburg (KORA) F4 (15).
Study characteristics are summarized in Table 1. In all studies, the adult participants gave informed written consent. All studies followed the recommendations of the Declaration of Helsinki and were approved by the local Ethics Committees.
SHIP, Study of Health in Pomerania; CARLA, Cardiovascular disease, Living and Ageing in Halle; KORA, Kooperative Gesundheitforschung der Region Augsburg; TSH, thyrotropin.
Exclusion criteria
From each study, we excluded all participants with missing data on any of the considered outcome, exposure, or confounder variables. For the cross-sectional analyses, the number of excluded subjects were 94 in SHIP, 6181 in the Rotterdam Study, 490 in INTER99, 66 in CARLA, and 98 in KORA. For the longitudinal analyses, the number of excluded subjects were 72 in SHIP, 3549 in the Rotterdam Study, 317 in INTER99, and 34 in CARLA. The large number of subjects excluded from the Rotterdam Study was because serum TSH levels were only measured in a randomly selected subset of the total population. The total number of subjects included from each study is given in Tables 1, 2, and 4.
Data are expressed as median and interquartile range (continuous data), or as number and percentage (categorical data).
Defined as diastolic blood pressure ≥90 mmHg, systolic blood pressure ≥140 mmHg, or intake of antihypertensive medication.
Assessments
Pulse pressure was defined as the difference between systolic and diastolic blood pressure. Hypertension was defined as systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg or use of antihypertensive medication. Use of antihypertensive medication was assumed in subjects answering “yes” to the question, “Was medication against high blood pressure prescribed by a physician during the last year?” Smoking status was categorized into the three categories: current smokers, former smokers, and never smokers. Former smokers were individuals who had smoked during their lifetime but not in the 12 months prior to the time of the baseline examination. Height and weight were measured for the calculation of the body mass index (BMI): weight (kg)/height (m2). The TSH reference range was defined as 0.3–<3.0 mIU/L (18). Low serum TSH levels were defined as serum TSH levels <0.3 mIU/L, and high serum TSH levels as serum TSH levels ≥3.0 mIU/L.
Statistical analyses
Data on quantitative characteristics are expressed as median and interquartile range; data on qualitative characteristics are expressed as percentages and absolute numbers. Associations between baseline serum TSH levels and blood pressure at baseline were assessed using multivariable median (continuous outcomes) and logistic regression models (dichotomous outcomes) adjusted for age, sex, smoking status, and BMI. Associations between baseline serum TSH levels and the change in blood pressure between baseline and follow-up were assessed by multivariable median regression (continuous outcomes) and multivariable Poisson regression with robust standard errors (dichotomous outcomes) adjusted for baseline values of age, sex, smoking status, BMI, and time between baseline and follow-up.
To assess the sensitivity of our longitudinal results for loss to follow-up, we calculated inverse probability weights for each of the single studies and used those weights in the regression models. The aim of this approach is to give more weight to subjects whose propensity to drop out of the study is high (19). The weights accounted for loss to follow-up are based on sociodemographic and health-related variables. In the analyses with categorized TSH (hyper- and hypothyroidism), serum TSH levels within the reference range are the reference.
All regression models were calculated separately for each individual study and again for the pooled population. Pooled analyses were additionally adjusted for the included studies. In all analyses with continuous exposure variables, fractional polynomials were applied to explore and graph nonlinear associations (20). The dose–response relation was found using fractional polynomials up to degree 2 with all possible combinations of powers selected from the set (−2, −1, −0.5, 0, 0.5, 1, 2, 3) and by comparing them using the log likelihood to determine the best-fitting model. If none of the fractional polynomials models fitted the data significantly better than the one with the untransformed exposure variable, calculations were done using the untransformed exposure variable. Interaction terms between serum TSH levels and all confounders were tested in the regression models. For all multivariable analyses, TSH was transformed by a power transformation to reduce the effects of outliers on the fractional polynomials (20). Statistical significance was set at p<0.05. All analyses were performed using Stata 12.0 (Stata Corporation, College Station, TX).
Results
Cross-sectional analyses
Baseline values of the single populations differed according to age, blood pressure, and serum TSH levels (Table 2). Participants of the Rotterdam Study and CARLA were the oldest, and those of INTER99 were the youngest. Most measures of blood pressure, including systolic and diastolic blood pressure, hypertension, and intake of antihypertensive medication, were higher or more common in CARLA than in the other studies, whereas hypertension and use of antihypertensive medication were least common in INTER99. Serum TSH levels were higher in INTER99, KORA, and the Rotterdam Study than in SHIP and CARLA.
In the pooled cross-sectional analyses using data from all five populations, serum TSH levels were positively associated with systolic blood pressure (Fig. 1), diastolic blood pressure (Fig. 2), and hypertension (Fig. 3) after adjusting for age, sex, smoking status, and BMI. There was no association with pulse pressure (Table 3). Interaction terms of serum TSH levels with age, sex, BMI, or smoking status were not associated with any of the outcomes.
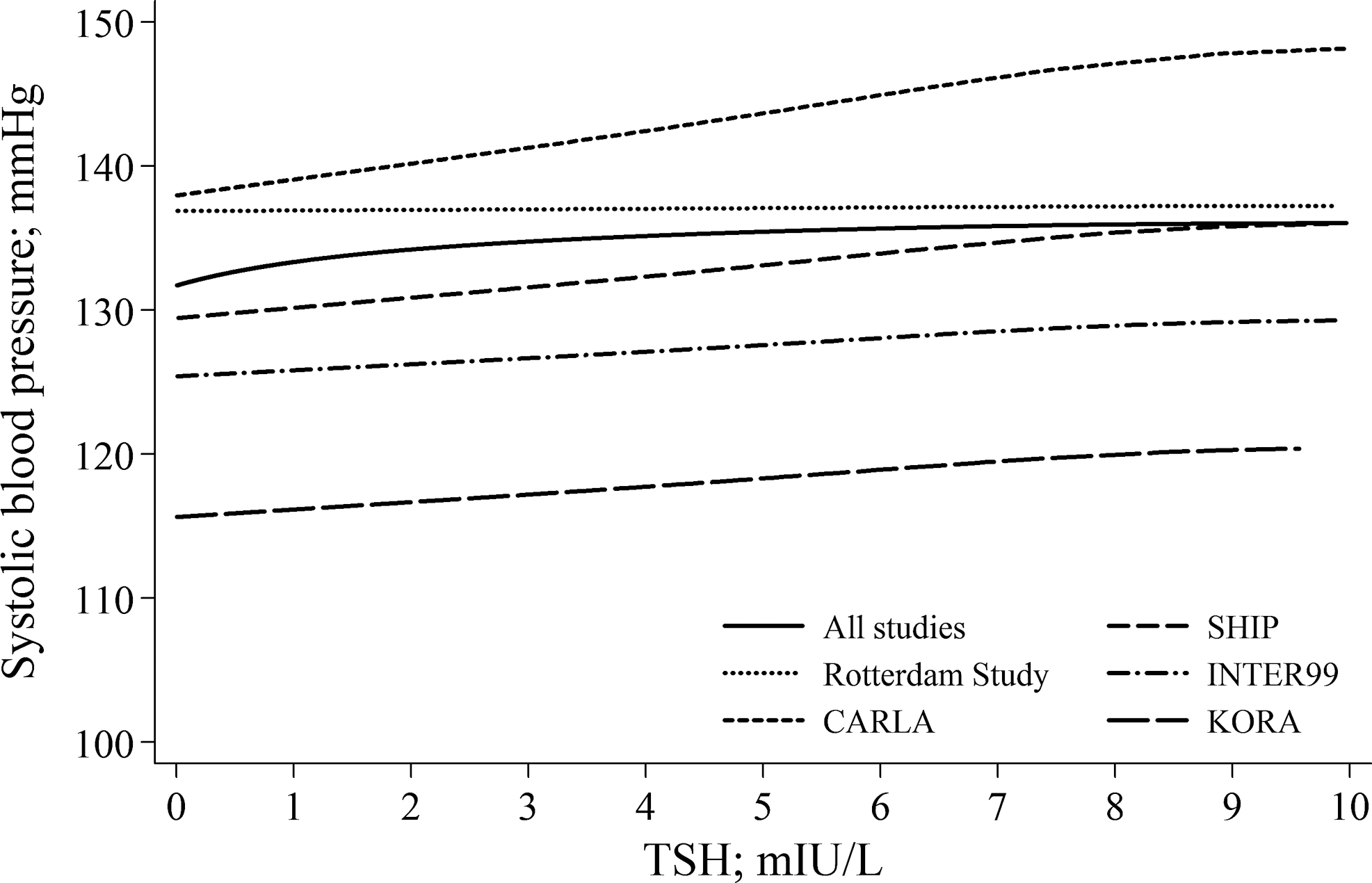
Adjusted regression curves for the association between baseline serum thyrotropin (TSH) levels over the full range and baseline systolic blood pressure in the single studies and the pooled population.
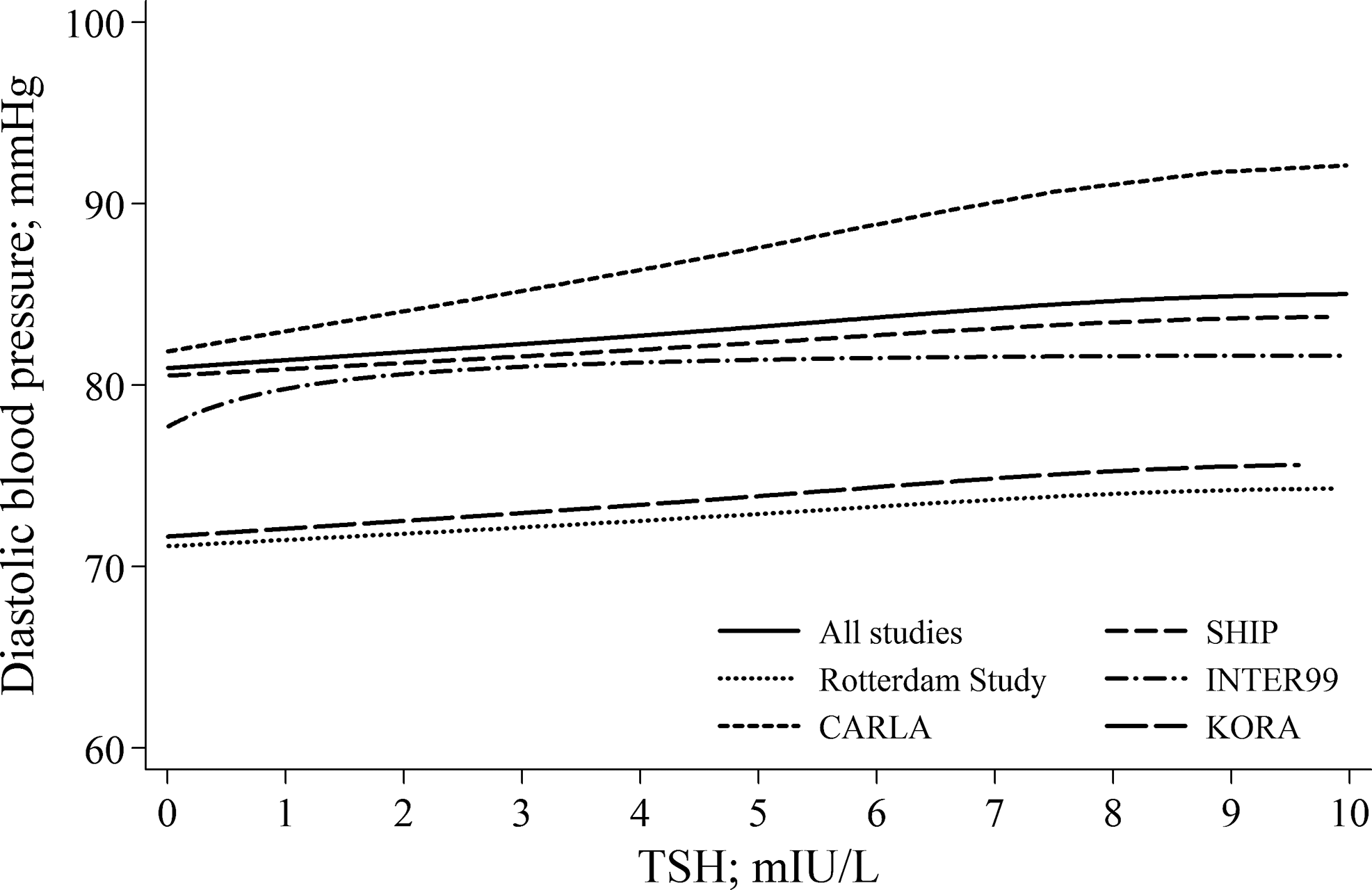
Adjusted regression curves for the association between baseline serum TSH levels over the full range and baseline diastolic blood pressure in the single studies and the pooled population.

Association between power-transformed serum TSH levels and baseline hypertension in the single populations and in the pooled population.
n=17,023; n=14,896 for analyses regarding TSH in the reference range. Median regression for continuous outcomes, logistic regression for dichotomous outcomes; all models adjusted for age, sex, body mass index, and smoking status. Pooled data analysis additionally adjusted for study. Fractional polynomials were applied to test for a nonlinear relationship between serum TSH levels and the respective outcome.
Compared to serum TSH levels within the reference range (0.3–3.0).
PTSH was transformed to PTSH−1, since otherwise PTSH remained untransformed.
Defined as diastolic blood pressure ≥90 mmHg, systolic blood pressure ≥140 mmHg, or intake of antihypertensive medication.
p<0.05; ** p<0.001.
We detected a significant association between serum TSH levels and systolic blood pressure in the INTER99 study (Fig. 1) but not in any of the other studies. Moreover, serum TSH levels were positively associated with diastolic blood pressure in INTER99, CARLA, KORA, and the Rotterdam Study (Fig. 2) but not in SHIP. Serum TSH levels were cross-sectionally associated with an increased risk of hypertension in INTER99 and KORA (Fig. 3).
High serum TSH levels were cross-sectionally associated with systolic and diastolic blood pressure in the pooled population (Table 3). Likewise, serum TSH levels within the reference range were significantly associated with systolic and diastolic blood pressure, pulse pressure, and hypertension. There was no association between low serum TSH levels and blood pressure.
Excluding all participants with intake of antihypertensive drugs revealed only one substantial difference compared to those of the main results listed in Table 3: low serum TSH levels were not associated with systolic blood pressure in the pooled population free of antihypertensive drug intake (β=0.9 [CI −0.3, 2.2], p=0.149).
Longitudinal analyses
Blood-pressure values changed differently between baseline and follow-up in the different populations (Table 4). Systolic and diastolic blood pressures decreased in SHIP and CARLA between baseline and follow-up, whereas there was an increase in systolic blood pressure and pulse pressure in the Rotterdam Study, and no change in INTER99. Incidence of antihypertensive drug intake was highest in CARLA and lowest in INTER99. Regression of baseline antihypertensive drug intake was highest in SHIP and lowest in CARLA. Incidence of hypertension was highest in the Rotterdam Study and lowest in INTER99, while regression of baseline hypertension was most common in INTER99 and least common in the Rotterdam Study.
Data are expressed as median and interquartile range (continuous data), or as number and percentage (categorical data). Changes are those between baseline and follow-up, standardized for a five-year follow-up.
Defined as diastolic blood pressure ≥90 mmHg, systolic blood pressure ≥140 mmHg, or intake of antihypertensive medication.
In the pooled population, we detected only one longitudinal association between serum TSH levels and blood pressure (Table 5). In the model including the whole range of serum TSH levels, there was an inverse association of TSH and the change in diastolic blood pressure. Interaction terms of baseline serum TSH levels with baseline values of age, sex, BMI, or smoking status were not associated with any of the longitudinal outcomes. Among the single populations, there were significant associations between baseline serum TSH levels and follow-up blood pressure variables only in the Rotterdam Study and CARLA. Serum TSH levels over the full range were significantly associated with incident hypertension (relative risk [RR]=1.98 [CI 1.14, 3.43], p=0.015), and high serum TSH levels were associated with the change in pulse pressure (β=4.3 [CI 0.9, 7.8], p=0.015) and with incident hypertension (RR=1.34 [CI 1.06, 1.69], p=0.015) in the Rotterdam Study, while serum TSH levels within the reference range were significantly associated with a change in diastolic blood pressure in CARLA (β=−1.9 [CI −3.7, −0.1], p=0.040).
n=10,048; n=8734 for analyses regarding TSH in the reference range. Median regression for continuous outcomes, Poisson regression for dichotomous outcomes; all models adjusted for baseline values of age, sex, body mass index, smoking status, and study. Fractional polynomials were applied to test for a nonlinear relationship between serum TSH levels and the respective outcome. Inverse probability weights were used to account for loss to follow-up.
Compared to serum TSH levels within the reference range (0.3–3.0).
Defined as diastolic blood pressure ≥90 mmHg, systolic blood pressure ≥140 mmHg, or intake of antihypertensive medication.
p<0.05.
After exclusion of individuals taking antihypertensive drugs at baseline and follow-up, serum TSH levels over the full range were no longer associated with diastolic blood pressure in the pooled population (β=−1.9 [CI −4.2, −0.4], p=0.109).
Discussion
We demonstrate a positive association of serum TSH levels over the full range and within the reference range with arterial blood pressure in our cross-sectional analyses of pooled data from five population-based studies in adults. Furthermore, serum TSH levels were positively related to prevalent hypertension. In contrast, we did not detect a consistent association of serum TSH levels with a five-year change in blood pressure and incident hypertension.
It has been shown that subclinical hypothyroidism is associated with increased arterial stiffness (21,22) and a higher prevalence of endothelial dysfunction (23,24), both of which might be intermediate pathophysiological stages between hypothyroidism and hypertension. Indeed, in our cross-sectional analyses, individuals with high serum TSH levels had significantly higher blood pressure values than euthyroid individuals. This finding corresponds well with our previously reported results in children and adolescents (1), but partly disagrees with those of the HUNT study from Norway (2). In that large population-based study (2), high serum TSH levels were associated with arterial blood pressure only in women but not in men. The failure to find a significant association between high serum TSH levels and arterial blood pressure in men may have been due to a selection bias because serum TSH levels were measured in only 50% of the male study population but in 100% of the female population. In our study, no statistically significant interactions between serum TSH and sex were found, which indicates that there were no relevant sex-related differences in the association between thyroid function and blood pressure.
Two smaller studies (5,6) found a cross-sectional association between subclinical hypothyroidism and blood pressure. In contrast, three other studies (3,7,8) failed to demonstrate such an association. However, in the studies (3,7,8) that did not show significant associations between subclinical hypothyroidism and blood pressure, the adjusted mean values of systolic and diastolic blood pressure were also approximately 2 mmHg higher in subclinical hypothyroidism than in euthyroidism (3,7,8), which is comparable to the estimates found in our study.
Arterial blood pressure hypothetically mediates the association of subclinical hyperthyroidism with atrial fibrillation (25), left ventricular hypertrophy (26), and carotid atherosclerosis (27,28). However, in agreement with our results, most of the previous studies on this issue (2,3,7,8,17,29) did not demonstrate an association between low serum TSH levels and arterial blood pressure (2,3,7,17,29), with the exception of just one study (8). However, in that study, serum TSH levels were available in only 50% of the study population, which might have introduced selection bias. Thus, associations of overt hyperthyroidism with increased systemic vascular resistance and arterial blood pressure (30) should not be expanded to subclinical hyperthyroidism. Of note, in all previous studies, the associations of subclinical hyperthyroidism with atrial fibrillation (25), left ventricular hypertrophy (26), and carotid atherosclerosis (27,28) were independent of blood pressure-related variables, which indicates either direct effects of subclinical thyroid overfunction on these outcomes or yet unknown pathophysiological mechanisms connecting subclinical hyperthyroidism and cardiovascular disorders.
In agreement with our findings in children and adolescents (1) and with results from the HUNT study (2), but contrary to the results of two other studies (5,7), we detected a positive relation between serum TSH levels within the reference range and blood pressure. The TSH reference range depends on the iodine supply in the study region (9). The studies that did not find an association between serum TSH levels in the reference range and blood pressure were conducted in Far East Asia (5,7), a region that is characterized by iodine excess. Consequently, the upper limit of the serum TSH reference range was higher in that studies (5,7) than in the present one and in the HUNT study (2). Former iodine supply slightly differed between the studies included in the present analyses and the HUNT study (2). While the studies included in the present analyses are from regions with former mild to moderate iodine deficiency (10,11), iodine supply was sufficient in Norway in the past (10). Thus, serum TSH levels within the reference range might be associated with blood pressure in regions with mild to moderate iodine deficiency or sufficient iodine supply, but not in regions with iodine excess. On the other hand, discrepancies between results from Europe and Far East Asia might also be explained by a higher prevalence of hypertension in Far East Asia than in Europe due to substantial differences in lifestyle factors and in approaches used for the screening, prevention, and treatment of hypertension and cardiovascular disease (31).
In our cross-sectional analyses, associations between serum TSH levels and arterial blood pressure remained statistically significant after exclusion of all subjects taking antihypertensive medication. Although drug intake was carefully and thoroughly assessed in our studies, we cannot rule out some misclassification of drug use. However, such misclassification is probably negligible and will usually lead to conservative estimates. Furthermore, our results are similar to those from our study in children and adolescents (1) in which antihypertensive drug intake was minimal.
Previous research on the association between thyroid function and incident hypertension or change in arterial blood pressure is scarce. There is only one population-based cohort that investigated this topic (17) and it was integrated into our pooled analysis. Our pooled analyses do not indicate any consistent association of serum TSH levels with change in blood pressure or incident hypertension. These results suggest that the association between thyroid function and blood pressure might be time-dependent and that current thyroid function does not predict future hypertension. Nevertheless, further studies with longer periods of follow up and in alternative geographical locations are required.
There are some strengths and limitations of our study. The large number of individuals included is a major strength. Furthermore, blood pressure measurements followed the same protocol in SHIP, CARLA, and KORA. A limitation of our study is that blood samples were taken from fasting subjects in INTER99, KORA, and the Rotterdam Study, whereas in SHIP and CARLA, blood samples were taken in nonfasting subjects. In consequence, serum TSH levels were lower in SHIP and CARLA than in the other three studies. Reasons for the difference in serum TSH levels between the studies might arise from a real difference of serum TSH levels between the studies, from an effect of fasting versus nonfasting sample taking, or from the circadian rhythm of serum TSH levels (32). A further limitation is that serum TSH levels were measured only once in our study, so that variations in serum TSH levels could not be considered. In addition, no data on free triiodothyronine and free thyroxine levels were available in our study. Possible effects of free thyroxine on arterial blood pressure have to be investigated in the future, since recent studies have shown significant associations between free thyroxine levels and various cardiovascular relevant phenotypes, including coronary artery calcification (33), left ventricular mass (34), and fatty liver (35). Finally, our data are derived solely from European populations, which challenges the extrapolation of our findings to populations from other geographical locations and with different ethnicities and iodine levels.
We conclude that high serum TSH levels associated with current hypertension and blood pressure, but not with five-year change in blood pressure and incident hypertension. This argues for only a short-term effect of thyroid hormone levels on arterial blood pressure, which needs to be further evaluated in additional population-based studies within different ethnicities, geographical locations, and perhaps with a longer follow-up period, in which a mid- and long-term effect of thyroid function could be addressed.
Footnotes
Acknowledgments
SHIP is part of the Community Medicine Net (
INTER99 was financially supported by The Danish Medical Research Council, The Danish Centre for Health Technology Assessment, Novo Nordic, Research Foundation of Copenhagen County, Ministry of Internal Affairs and Health, The Danish Heart Foundation, The Danish Pharmaceutical Association, The Augustinus Foundation, The Ib Henriksen Foundation, and The Becket Foundation. The Inter99 study was initiated by Torben Jørgensen (PI), Knut Borch-Johnsen (co-PI), Troels Thomsen, and Hans Ibsen. The present steering group comprises the former two and Charlotta Pisinger.
The KORA research platform and the KORA Augsburg studies are financed by the Helmholtz Zentrum München, German Research Center for Environmental Health (GmbH), which is funded by the German Federal Ministry of Education, Science, Research, and Technology and by the State of Bavaria. Thyroid examinations were additionally funded by Sanofi-Aventis in the framework of the Papillon Initiative.
The CARLA Study was founded by a grant from the German Research Foundation (DFG) as part of the Collaborative Research Center 598 “Heart failure in the elderly—cellular mechanisms and therapy” at the Medical Faculty of the Martin-Luther-University Halle-Wittenberg, by a grant of the Wilhelm-Roux Programme of the Martin-Luther-University Halle-Wittenberg; by the Ministry of Education and Cultural Affairs of Saxony-Anhalt; and by the Federal Employment Office.
The Rotterdam Study is funded by Erasmus Medical Center and Erasmus University, Rotterdam; Netherlands Organization for the Health Research and Development (ZonMw); the Research Institute for Diseases in the Elderly (RIDE); the Ministry of Education, Culture and Science; the Ministry for Health, Welfare and Sports; the European Commission (DG XII); and the Municipality of Rotterdam. The generation and management of GWAS genotype data for the Rotterdam Study is supported by the Netherlands Organization of Scientific Research NWO Investments (#175.010.2005.011, 911-03-012). This study is funded by the Research Institute for Diseases in the Elderly (014-93-015; RIDE2), and the Netherlands Genomics Initiative (NGI)/Netherlands Organization for Scientific Research (NWO) project #050-060-810.
Author Disclosure Statement
No competing financial interests exist.