
Abstract
Background:
Helicobacter pylori infection is reportedly associated with extradigestive diseases such as immune thrombocytopenic purpura and coronary heart disease. The risk factors for autoimmune thyroid diseases (ATDs) remain largely unknown, and whether H. pylori infection is associated with ATDs is still controversial. The aim of this meta-analysis was to determine the association between H. pylori infection and ATDs.
Methods:
Studies comparing the prevalence rate of H. pylori infection in patients with ATDs and healthy controls, published in English, were identified through a systematic search in MEDLINE and EMBAS up to June 2012. Serological or nonserological tests were used to confirm H. pylori infection and the presence of cytotoxin-associated gene A (CagA) antigens. The odds ratios (OR) and associated 95% confidence intervals [CI] were obtained.
Results:
Seven studies involving a total of 862 patients met the inclusion criteria and thus were included in our meta-analysis. Overall, H. pylori infection was associated with ATDs (OR 1.92 [CI 1.41–2.61]); the association was significant for Graves' disease (OR 4.35 [CI 2.48–7.64]) but not for Hashimoto's thyroiditis (OR 1.45 [CI 0.92–2.26], p=0.11). No association was observed in the subanalysis of studies using only enzyme-linked immunosorbent assay to detect H. pylori infection (OR 1.38 [CI 0.86–2.19], p=0.18). Five of the seven articles reported the association of CagA seroprevalence and ATDs. CagA seropositivity significantly increased the risk for ATDs by 2.24-fold [CI 1.06–4.75].
Conclusions:
Both the prevalence of H. pylori infection and the seroprevalence of CagA-positive strains are associated with ATDs. These findings suggest that H. pylori infection potentially plays a part in the development of ATDs.
Introduction
Autoimmune thyroid diseases (ATDs) include Graves' disease (GD), Hashimoto's thyroiditis (HT), and atrophic thyroiditis, all of which are characterized pathologically by infiltration of thyroid tissue by T- and B-cells that are reactive to thyroid antigens biochemically by the production of thyroid autoantibodies and clinically by abnormal thyroid functions (8). They are complex diseases that are postulated to be caused by the combined effects of multiple susceptibility genes and environmental triggers (9,10). Autoantibodies against thyroid antigens, such as antithyroglobulin antibodies (TgAbs), thyroid peroxidase antibodies (TPOAbs), and antithyrotropin-receptor antibodies are the typical markers of ATDs (11). Concerning the nosogenesis, there has been serological evidence for the role of bacterial infections in the pathogenesis of thyroid diseases; however, the exact pathogens have never been identified (12).
In the past 15 years, a number of studies have been published on the association between H. pylori infection and ATDs. Although several studies have shown a significantly increased H. pylori prevalence in patients with ATDs compared with those in the control group, other studies have produced insignificant results. Therefore, the present meta-analysis of relevant clinical studies was performed to determine the association between H. pylori infection and ATDs in order to provide evidence-based knowledge on the potential etiological role of H. pylori infection in the development of ATDs.
Materials and Methods
Literature search
To identify the literature for this meta-analysis, a systematic search of all studies published in English in MEDLINE and EMBASE up to June 2012 was conducted. The following medical subject headings or keywords were used: Helicobacter pylori or H. pylori or HP, autoimmune thyroid disease, and autoimmune thyroiditis. The literature search was conducted independently by two reviewers. We also reviewed references cited by the relevant articles and major gastroenterology and endocrinology conference abstracts. Articles were subsequently identified by extensive review of titles or abstracts.
Inclusion and exclusion criteria
Observational (case–control, cohort, and cross-sectional) studies were included if the following criteria were met: 1. Studies were conducted in humans. 2. The diagnosis of GD was based on the presence of hyperthyroidism (suppressed thyrotrophin and elevated free triiodothyronine and free thyroxine), diffuse goiter on thyroid tissue together with positive titers of antibodies (TPOAbs, TgAbs, and antithyrotropin-receptor antibodies). The diagnostic criteria of HT included hypothyroidism (elevated thyrotrophin and low free triiodothyronine and free thyroxine), positive titers of antibodies (TPOAbs and TgAbs), typical ultrasonographic aspects of the thyroid gland, or fine-needle aspiration biopsy and cytology. Atrophic thyroiditis was defined by the presence of clinical and biochemical hypothyroidism, positive antithyroid antibodies, and thyroid atrophy on ultrasonography examination. 3. H. pylori infection was diagnosed by serological tests, including antigen-specific enzyme-linked immunosorbent assay (ELISA) and Western blotting, or nonserological tests, including rapid urease test, 13C-urea breath test (UBT), and stool antigen test (SAT). 4. A control group was included. Studies with insufficient information on the association between H. pylori and ATDs, or with an inversed study strategy were excluded. In addition, for studies with data published twice or more, only the article with an adequate study strategy and larger case number was selected.
Identification of studies
After initial computer and manual search, articles were subsequently assessed by review of titles and abstracts by two reviewers. Full texts were browsed after primary screening. Disagreements were resolved through discussion. Final article selection was conducted by both reviewers.
Data extraction and quality appraisal
Data extraction from each article was carried out independently by the two reviewers. Our research strategy was to obtain a positive rate of H. pylori infection in each group. The following data were extracted: authors, year of publication, study design, characteristics and number of cases and controls, diagnostic methods for H. pylori infection, CagA status and ATDs, proportion of patients infected with H. pylori, and CagA antibody–positive strains.
Two reviewers independently assessed the quality of every study included in this meta-analysis by using the criteria from the guidelines for reading case–control studies proposed by Lichtenstein et al. (13). The contents of this guideline mainly included validation of methods for selecting participants, credibility of controls and representativeness of cases, and age, sex, and socioeconomic status matching techniques between the two groups. The quality levels were graded as good (A), fair (B), and poor (C).
Statistical analysis
In this study, heterogeneity was tested by the I 2 statistic (values <50% were considered to represent no significant heterogeneity). The fixed effect model was used when there was no significant heterogeneity (I 2<50%); otherwise, the random effect model was used. p-Values of <0.05 were regarded as statistically significant for all included studies. Dichotomous variables were calculated using the odds ratios (OR) with the 95% confidence interval [CI] as the summary statistic. The Mantel–Haenszel method was used to combine ORs for the outcome parameters. Statistical analyses of data were undertaken using the Statistical Software Package (STATA) version 7.0 (STATA Corporation, College Station, TX) and Review Manager version 4.2 (The Cochrane Collaboration, Oxford, United Kingdom).
Results
Literature search and selection
After the initial literature search, 109 citations, all published in English, were identified. One additional study was identified by reviewing the references of an article. Among these citations, 95 were excluded through review of the titles and abstracts due to duplicated publication (n=11), being not case–control, cohort, or cross-sectional studies (n=55), or unavailability of information on the association between H. pylori infection and ATDs (n=24), or raw data (n=2), or being a report involving animal subjects (n=3). Then, the full text of the remaining 15 studies was retrieved and carefully reviewed. Of these, five articles were excluded due to the lack of evaluating the presence of H. pylori infection and two were excluded because of their inversed study strategy. An additional article was excluded due to lack of a control group. Therefore, a total of seven observational studies (14 –20) met our inclusion criteria (Fig. 1).
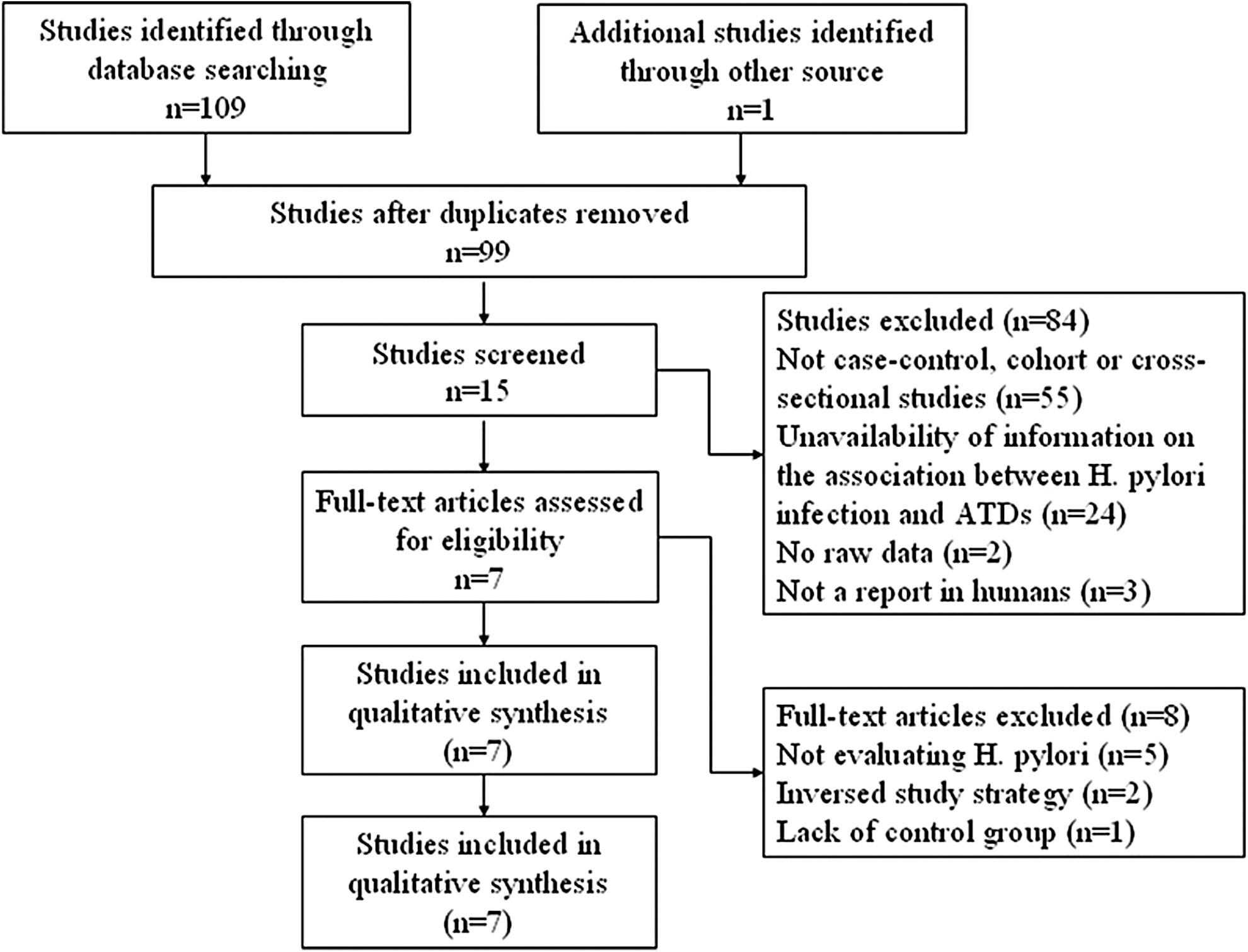
Literature search and selection.
Characteristics of individual studies
The characteristics of the included articles are summarized in Table 1. All studies were published between 1998 and 2012. The first article by de Luis et al. (14) was published in 1998. All of the included studies had a case–control design. The number of study subjects ranged from 36 to 212, with a combined number of 862. All of the articles were age- and sex-matched. The proportion of females ranged from 66.7% to 100%. Regarding the methods used to assess H. pylori infection status, four studies used serologic methods (ELISA or Western blotting), two used nonserologic tests (13C-UBT or SAT), and one used both methods. Five of the seven studies reported the CagA status in cases (Table 1).
ATDs, autoimmune thyroid diseases; ELISA, enzyme-linked immunosorbent assay; F, female; Hp-Po, Helicobacter pylori positive; M, male; NR, not reported; SAT, stool antigen test; UBT, 13C-urea breath test; WB, Western blotting.
Meta-analysis results
Among the seven studies, four showed a significant difference of the H. pylori prevalence rate in ATDs and controls (14,15,18,19). No association was observed from the remaining three studies (16,17,20). The overall prevalence rate of H. pylori infection was 54.3% (253 of 466) in ATDs and 45.2% (179 of 396) in controls. Our meta-analysis of all the included studies showed a significant association between H. pylori positivity and ATDs. The fixed effect model was used. The summary OR was 1.92 ([CI 1.41–2.61], test for overall effect: Z=4.19, p<0.0001). No significant statistical heterogeneity was seen (I 2=39.9%) (Fig. 2). The funnel plot did not show significant publication bias (Fig. 3).
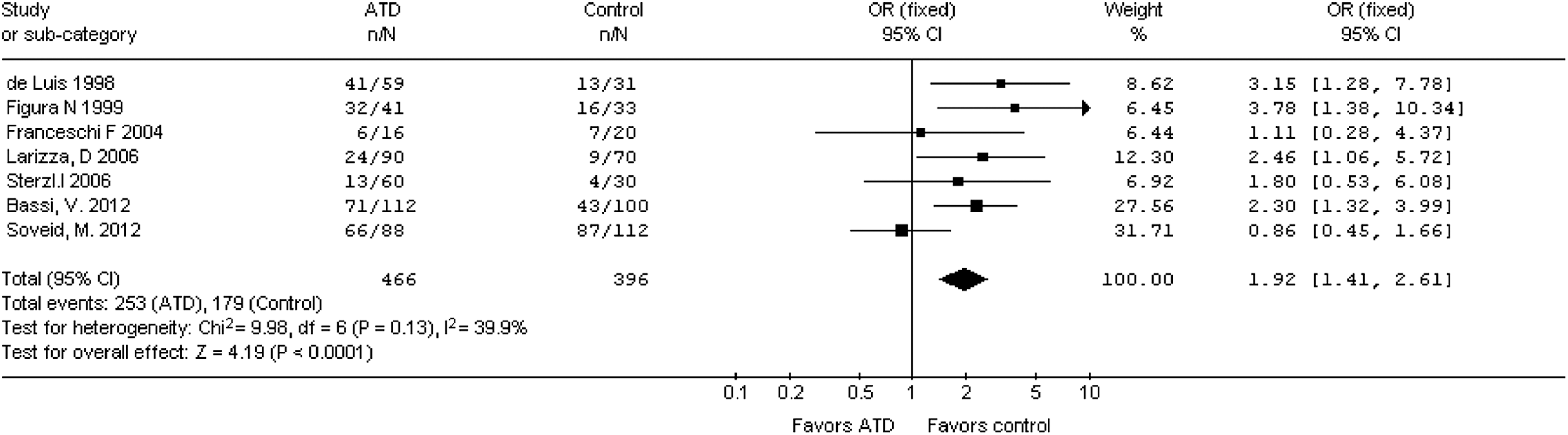
Association between Helicobacter pylori infection and autoimmune thyroid diseases. The squares represent individual studies and the size of the square represents the weight given to each study in the meta-analysis. The diamond represents the combined results. OR, odds ratio; CI, confidence interval.
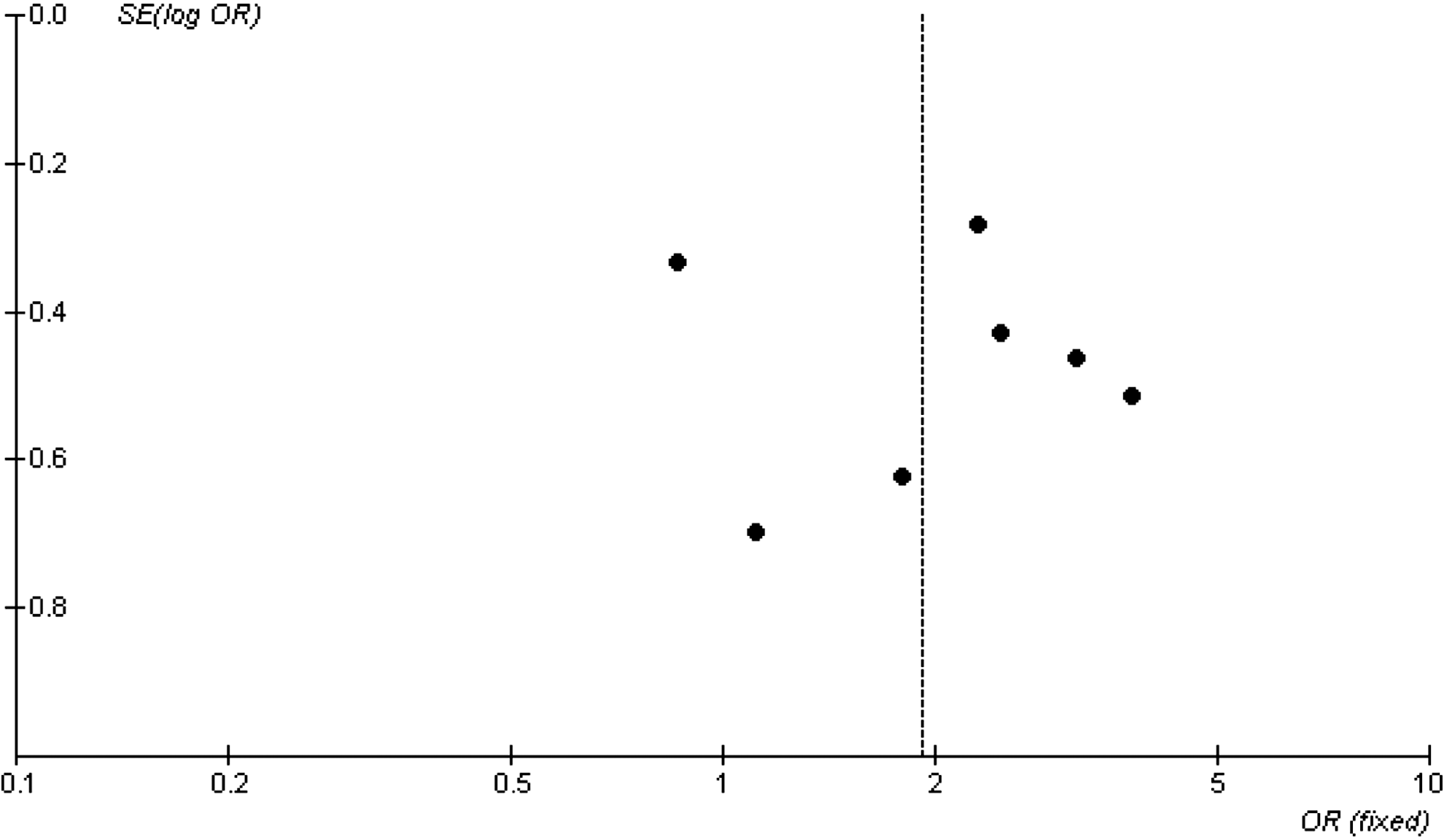
Funnel plot analysis of H. pylori infection and autoimmune thyroid diseases.
Concerning the different criteria used in the detection of H. pylori infection in the different studies, we performed a subanalysis in the studies using ELISA as the diagnostic criteria. The prevalence rate of H. pylori infection was 43.3% (103 of 238) in ATDs and 47.2% (100 of 212) in controls (OR 1.38 [CI 0.86–2.19], test for overall effect: Z=1.34, p=0.18).
In some selected studies, there were opposite results between GD and HT concerning the prevalence rate of H. pylori. Therefore, we performed a subanalysis for GD and HT, respectively. The prevalence rate of H. pylori infection was 66% (64 of 97) in GD and 32.3% (65 of 201) in controls (OR 4.35 [CI 2.48–7.64], test for overall effect: Z=5.12, p<0.0001) (Fig. 4A). In addition, the prevalence rate of H. pylori infection was 37.7% (60 of 159) in HT and 32.5% (72 of 221) in controls (OR 1.45 [CI 0.92–2.26], test for overall effect: Z=1.62, p=0.11) (Fig. 4B).

Three out of five articles that provided data on CagA antibody seroprevalence showed a statistical association between ATDs and CagA seropositivity (15,19,20), while the other two did not (16,17). The overall CagA seroprevalence in ATDs was significantly higher than that observed in controls—42.6% (135 of 317) versus 22.4% (66 of 295). The meta-analysis result showed a significant difference in CagA seropositivity between ATDs and controls, yielding an OR of 2.24 ([CI 1.06–4.75], test for overall effect: Z=2.11, p=0.03). However, there was a significant heterogeneity (I 2=69.9%; Fig. 5).

Association between cytotoxin-associated gene A seropositivity and autoimmune thyroid diseases. The squares represent individual studies and the size of the square represents the weight given to each study in the meta-analysis. The diamond represents the combined results.
Discussion
Human autoimmune thyroiditis is characterized by infiltration of thyroid tissue by lymphocytes, gradual destruction of the gland associated with cytotoxic T cells, and production of various secondary polyclonal thyroid autoantibodies, notably TPOAbs and TgAbs (21). The three ATDs mentioned above have a similar etiology, as well as common pathological, biochemical, and clinical characteristics. Hence, it is justifiable to put them together in this meta-analysis. Both genetic and environmental factors have been implicated in the pathogenesis of the disease (22). Besides H. pylori, many bacteria and viruses have been implicated in the pathogenesis of ATDs, such as Yersinia enterocolitica (23,24) and the hepatitis C virus (25,26).
Infectious agents may induce thyroid autoimmunity by a variety of diverse mechanisms, such as inducing modifications of self-antigens, mimicking self-molecules, inducing polyclonal T-cell activation (e.g., by superantigens), altering the idiotypic network, forming immune complexes, and inducing expression of major histocompatibility complex molecules on thyroid epithelial cells (12). However, more investigation is needed to elucidate the underlying molecular mechanisms.
Our updated meta-analysis of seven studies evaluated a total of 862 patients, and found a significant association between H. pylori infection and ATDs. In addition to the seven studies included in our meta-analysis, many studies probed into the potential role of H. pylori in the development of ATDs by other study strategies. Sterzl et al. (27) found a higher occurrence of anti-TPO and anti-GPC in H. pylori seropositive persons compared with seronegative ones, irrespective of age and sex. Bertalot et al. (28) found that thyroid autoantibodies decreased after eradication of H. pylori infection. The findings of Centanni et al. (29) indicated that patients with multinodular goiter required an increase in the dose of thyroxine if they had concomitant atrophic gastritis, chronic H. pylori infection, or both. Substantial data suggested that in several conditions (30) unusually large doses of thyroxine are required. The findings led to the hypothesis that gastric acid secretion is necessary for the effective absorption of oral thyroxine (29). H. pylori infection affects gastric acid secretion. This has been attributed to the release of inhibitory cytokines (31), the production of fatty acids inhibiting H+/K+–ATPase activity (32), impaired feedback between gastrin and acid secretion (33), and damage to the mucosa of the gastric body (34). H. pylori infection has also been shown to cause atrophic gastritis and plays an important part in the progression of atrophic gastritis. Ito et al. (35) found that, in H. pylori–positive patients, the antiparietal cell antibody level was significantly higher in the patients with moderate to severe atrophic gastritis than in those with mild atrophic gastritis. Elisei et al. (36) found a homologous 11-residue peptide in both gastric parietal cell antigen and TPO. These findings suggest the existence of an epitope common to both of the two antigens. Thus, we hypothesize that H. pylori infection may play a role in the development of ATDs. However, the role of antiparietal cell antibody and antiperoxidase antibodies in the pathogenesis of ATDs is yet to be elucidated.
Subanalysis of the studies using ELISA only for the detection of H. pylori infection showed no significant association between H. pylori infection and ATDs, suggesting that a possible bias may exist. It is known that most ELISA methods detect both past and current H. pylori infections, whereas other detection methods such as UBT and SAT detect current infection. Theoretically, UBT and SAT are more accurate than ELISA for the detection of H. pylori infection and should be used in the studies that evaluate the association between H. pylori infection and ATDs.
CagA is a marker for the cag pathogenicity island, which includes genes necessary for the enhanced inflammation induced by pathogenic strains (37). Infection with H. pylori strains possessing CagA is associated with an increased risk of developing peptic ulcer and gastric cancer (5). In the metaanalysis presented here, we found a significant association between CagA positivity and ATDs (OR 3.4 [CI 2.50–4.64]). We speculate that there is a possible cross reaction between antibodies produced during H. pylori infection and thyroid antigens leading to potential development of ATDs. Also, the data support the role of molecular mimicry in the pathogenesis of thyroid autoimmunity (38). In addition, the development in immune responses may also contribute. On one hand, T helper (Th) cells can be categorized as Th1 or Th2, identified by different patterns of cytokine production and effector function (39); Wang et al. (40) found that polarization of Th cell immune responses occurred in patients with CagA-positive H. pylori infection, which was associated with the stage and severity of gastric pathology during the progression of gastric carcinogenesis. On the other hand, the mixed pattern of cytokine production (41,42) indicates that both the Th1 and Th2 responses are involved in all types of ATDs. It is now clear that secretion of chemokines and cytokines within thyroid tissue accounts for the accumulation and expansion of the intrathyroidal lymphocyte pool (43). Therefore, we suppose that Th cells play an important role in the association between H. pylori infection and ATDs. More and further studies are needed to test our hypothesis.
We also realize that our study has several limitations. First, only seven studies met the criteria and were included, which is a major limitation of our meta-analysis. Second, among the included studies, one used SAT and the other used the 13C-UBT to detect H. pylori infection. Five studies used a serological test, which detected past and current infections. Serological tests detected more positive cases than the nonserological tests, causing bias. Second, although there was no significant publication bias in the meta-analysis of H. pylori positivity and ATDs, a publication bias existed for the meta-analysis of CagA and ATDs. Thus, more large-sample, multicenter, randomized, and controlled studies are needed.
In conclusion, both the overall prevalence of H. pylori infection and the seroprevalence of CagA-positive strains are associated with ATDs. These findings suggest that H. pylori potentially plays a part in the development of ATDs; however, further studies are needed to confirm our findings and to explore the underlying mechanisms.
Footnotes
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No. 81072032 and 81270476). The authors thank Medjaden Bioscience Limited for assisting in proofreading the manuscript.
Author Disclosure Statement
No competing financial interests exist.