
Abstract

We read Dr. Soelberg et al.'s article with great interest, as we have pursued this topic in our center over the years (1 –4). In fact, our 2007 article had the largest collection of patients with positron emission tomography (PET) data used in their analysis (1). We practice at a busy international multiple myeloma referral center, so we have a Nuclear Medicine/PET practice with abundant PET data. We agree with the authors that incidental focal thyroid lesions on PET-CT (computed tomography) should be taken seriously. They should be pursued as any thyroid nodule is when encountered clinically or incidentally, by ultrasound directed fine-needle aspiration biopsy and further expectant management based on cytology, adhering to current best practices or guidelines (5). If ambiguity persists after fine-needle aspiration, serious consideration should be given to open biopsy in the form of hemithyroidectomy due to 18F-fluorodeoxyglucose (FDG) avidity.
Diffuse thyroid uptake on PET-CT is usually not a concern for malignancy, and is indicative of inflammatory thyroid disease, which may ultimately require medical management (3,6). Although most acquired hypothyroidism in North America is from Hashimoto's thyroiditis, only a minority (<10%) of these patients have diffuse thyroid uptake noted in PET (7). Soelberg et al. started from the perspective of diffuse PET uptake in the thyroid, and not from the perspective of Hashimoto's thyroiditis, and eight of their reviewed studies reported a mean standardized uptake value (SUV) of 3.9.
With regard to focal thyroid uptake on PET-CT, our group has come to some slightly different conclusions regarding interpretation of the PET data (4). In our recent study, 23,384 PET and PET-CT scans performed between December 2001 and April 2011 were reviewed. Incidental thyroid uptake was noted in 1309 PET scans (5.17%), focal uptake in 690 (2.95%), and diffuse uptake in 619 (2.64%). Malignancy was identified in 27% of patients with focal uptake, 89% of which were primary thyroid malignancies. A significant difference between malignant SUVmax and benign SUVmax was found (mean±SD=7.04±7.88 for malignancies vs. 3.85±3.06 for benign tumors, p=0.0292). Receiver operating characteristics (ROC) curves were constructed on patients with PET data within three months of pathology diagnosis, and indicated that a SUVmax of 4.2 differentiated maximally between benign and malignant lesions (Fig. 1). This is a significantly higher value for SUV than the mean 2.0 reported by Soelberg et al. in their 22-series study group (1). Additional, we reported that serial SUV uptake measurements of thyroid lesions noted incidentally, for other oncologic surveillance and not removed because of benign cytology, had no significant change over time.
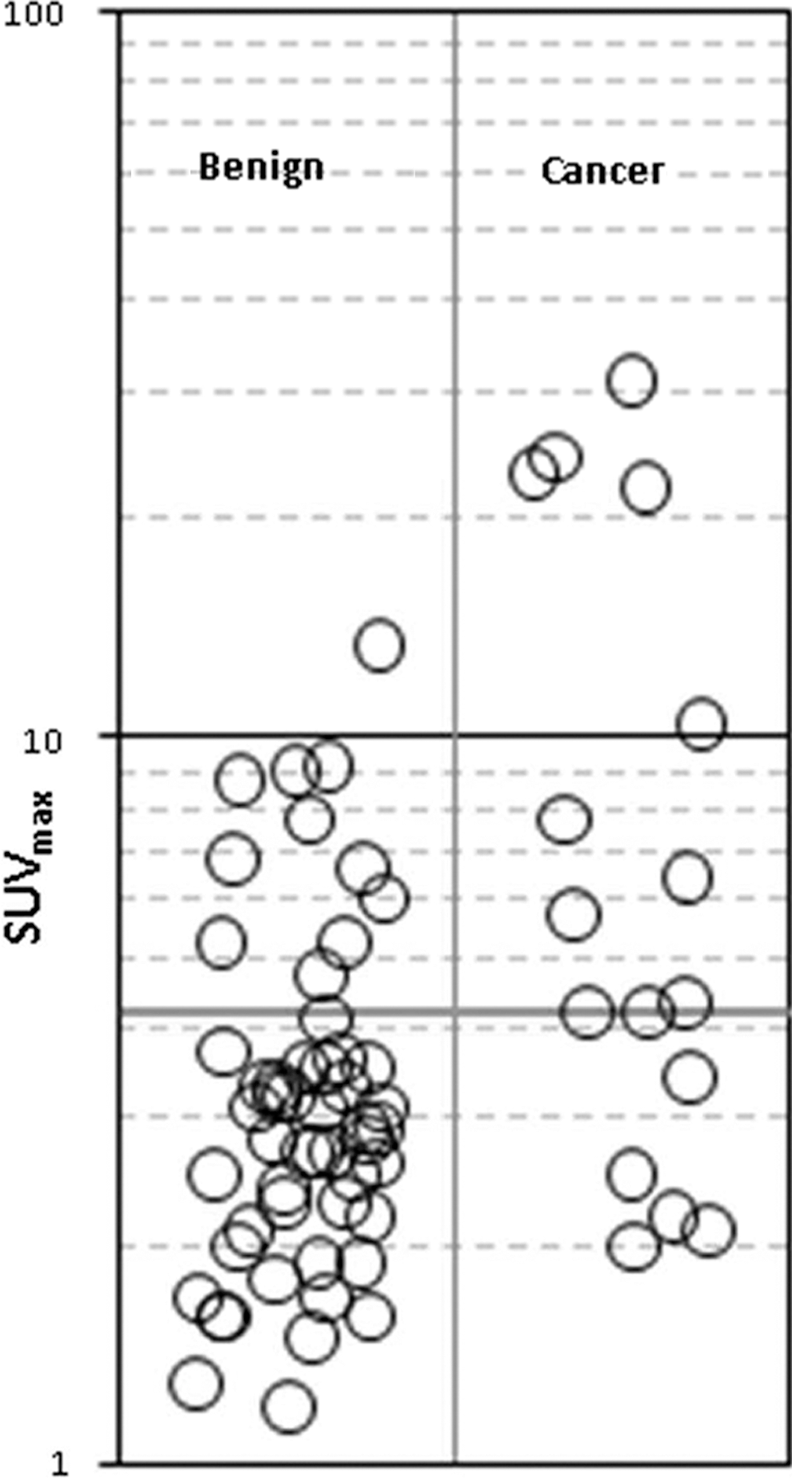
Modified from Boeckmann et al. (4). A standardized uptake value of 4.2 has maximal discrimination between benign and malignant.
Incidental focal thyroid uptake on PET-CT has the most clinical significance for possible malignancy of any other type of thyroid “incidentalomas” detected by other imaging modalities (CT, magnetic resonance imaging, and ultrasound) because it is a functional scan. These lesions should be approached according to best practices, as recommended by current guidelines on thyroid nodule evaluation.