
Abstract
Background:
The cytopathologic description of atypia of undetermined significance (AUS)/follicular lesion of undetermined significance (FLUS) includes nine different criteria in The Bethesda System, and the risk of malignancy in this category shows a wide range. The objectives of the present study were to determine whether ultrasound (US)-guided core-needle biopsy (CNB) indicates a different malignant risk, and to identify management recommendations, malignant US findings, and distribution of CNB readings in subcategories of AUS/FLUS category, as seen on previous thyroid fine-needle aspiration readings.
Methods:
From October 2008 to July 2011, 191 thyroid nodules of 191 patients who had previously been diagnosed with nuclear atypia (Group AUS; n=84) and microfollicular architecture (Group FLUS; n=107) were enrolled in our retrospective study. Final diagnoses were obtained in 142 nodules after surgery and clinico-radiological follow-up. We compared the malignancy risk, management recommendation, malignant US findings, and distribution of CNB readings between the two groups and calculated the diagnostic value of CNB.
Results:
With CNB, the final malignancy results were greater in Group AUS (65%, 33/51) than Group FLUS (14.3%, 13/91; p<0.001), and there were more surgical candidates in Group AUS (57.8%, 46/84) than Group FLUS (19.6%, 21/107; p<0.001). CNB showed 95.8% diagnostic accuracy for identifying malignancies and 19.4% inconclusive readings. Malignant US findings were seen more frequently in Group AUS (76.5%, 39/51) than Group FLUS (52.7%, 48/91; p=0.007). Malignant CNB readings were statistically more frequent in Group AUS (49.2%, 41/84) than Group FLUS (9.4%, 10/107; p<0.001), and benign readings were statistically more frequent in Group FLUS (58.9%, 63/107) than Group AUS (28.6%, 24/84; p<0.001).
Conclusions:
US-guided CNB demonstrated that Group AUS showed a higher risk of malignancy, of becoming surgical candidates, of having malignant US findings, and of having malignant CNB readings than Group FLUS. Further management guidelines for Group AUS should differ from Group FLUS.
Introduction
A
Materials and Methods
Patient and study design
This retrospective study was approved by the institutional review board at the Asan Medical Center, and informed consent was waived for evaluation of data. Written informed consent for the routine CNB protocol was obtained from all patients before each procedure.
We reviewed the medical records and US images of the patients who underwent US-guided CNB for thyroid nodules at our institution between October 2008 and July 2011. A total of 600 consecutive core-needle biopsy results were identified in 587 patients. Of them, 191 thyroid nodules (mean size=1.8 cm; size range=0.3–7.7 cm) from 191 patients (mean age=51.1 years; age range=19–85 years) who had thyroid nodules identified on previous AUS/FLUS FNA readings were included in this study. During the same period, the prevalence of AUS/FLUS FNA readings at our institution was 16 % (3338/20,805). Regarding the AUS/FLUS FNA readings before CNB, eight patients had three, 18 patients had two, and 165 patients had a single prior AUS/FLUS FNA reading. The exclusion criteria were as follows: (i) patients with a tendency to bleed or patients receiving anticoagulation therapy; (ii) patients with nodules that would not allow a technically feasible successful CNB procedure; and (iii) patients with cystic thyroid nodules (cystic portion >90%).
We divided the 191 nodules into two groups—Group AUS (n=84) and Group FLUS (n=107)—using the cytological features according to the previous studies (10,13,15,19). Repeat FNAs were performed in some patients 6–12 months after CNB. Final diagnoses were obtained in 142 nodules (Group AUS: n=51, mean size=1.34 cm; Group FLUS: n=91, mean size=2.21 cm) from 142 patients (22 men and 120 women; mean age=51.1 years). For malignant nodules (n=46), the final diagnosis was based on the histopathological readings after surgical resection. For benign nodules (n=96), the final diagnosis was based on histopathological readings after surgical resection (n=15, 16%) or on a concordant benign reading of the FNA and the CNB (n=24, 25%) or benign readings of the CNB or FNA with a stable size during the one-year follow-up period (n=57, 59%; Fig. 1). In all patients with a concordant benign reading of the FNA and the CNB (n=24), benign CNB results were followed by benign FNA readings.
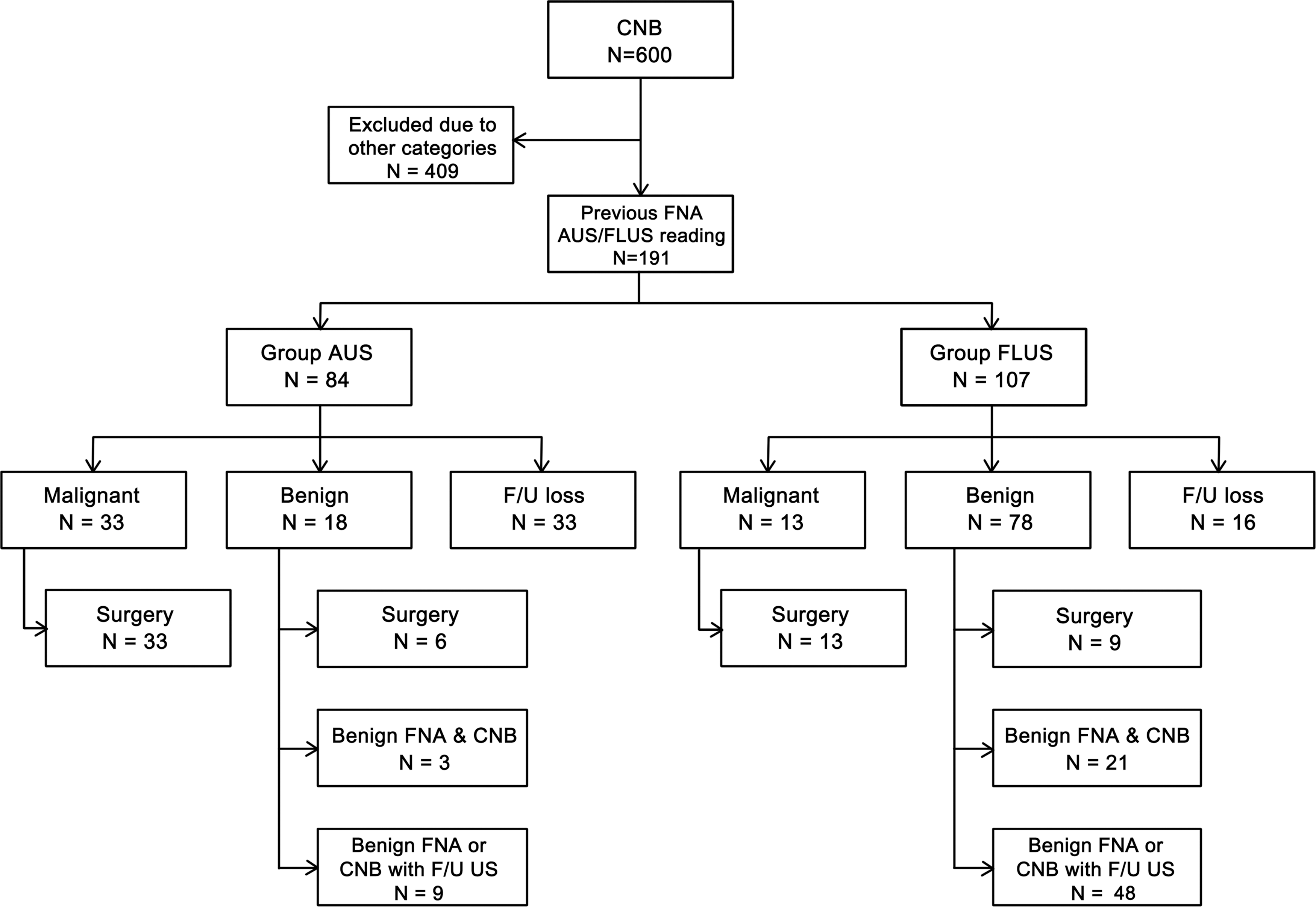
Flow chart of the study group. CNB, core-needle biopsy; FNA, fine-needle aspiration; AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; F/U, follow-up; US, ultrasound.
We evaluated the difference in risk of malignancy, distribution of CNB readings, and the management recommendations between the two groups, based on the results of the surgery or follow-up and CNB. Since there have been no management recommendation systems for thyroid CNB, we applied the recommended clinical management of The Bethesda System (1). The management recommendations were classified into three categories: (i) clinical follow-up for benign readings; (ii) repeat biopsy for inconclusive readings (nondiagnostic or AUS/FLUS readings); and (iii) surgery performed for follicular neoplasm/suspicious for a follicular neoplasm, suspicious for malignancy, and malignant readings. We also evaluated the risk of malignancy in the two groups in conjunction with the previous FNA results and US findings. We assessed the diagnostic value of CNB for determining malignancy. The reference standard was pathologic results after surgery. We specified this for two groups of CNB results: malignant and suspicious for malignant. We measured its accuracy, sensitivity, specificity, and positive and negative predictive values.
US-guided CNB procedures
For all patients, the CNB procedures were performed on an outpatient basis. US examinations were performed using one of three US systems: an iU22 unit or HDI-5000 (Philips Healthcare, Bothell, WA), or an EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear, high-frequency probe (5–14 MHz). All US examinations and CNBs were performed by four clinically experienced radiologists specializing in the thyroid (J.H.B., J.H.L., E.J.H, and H.K.L) with 16, 11, 7, and 7 years of thyroid US experience respectively.
We evaluated the thyroid nodules for their size, location, composition, and vascularity, as well as the vascular structures around the thyroid gland by US. US-guided CNBs were performed with a 1.1-cm or a 1.6-cm excursion, disposable, 18-gauge, double-action, spring-activated needle (TSK Ace-cut; Create Medic, Yokohama, Japan) after administering local anesthesia using 1% lidocaine. Using a freehand technique, the core needle was approached from the isthmus directed toward the solid element of a partially solid nodule and the wall of a predominantly cystic nodule (>50% of the cystic portion and ≤90% of the cystic portion). After the tip of the biopsy needle was advanced into the edge or within the nodule, the stylet and cutting cannula of the needle were sequentially fired. To prevent hemorrhage, the vessels along the approach route were carefully evaluated by power Doppler US before and during the procedure (Fig. 2). In all patients, targeting of thyroid nodules was possible, and the biopsy procedures were well tolerated. Additional CNB was performed when the lesion was considered inaccurately targeted in the case of small nodules, or when an adequate tissue core was not obtained by visual inspection. Tissue cores were placed in 10% buffered formalin immediately after the procedure and were then conventionally processed. Following the biopsy, each patient was treated using firm, local compression of the biopsy site for 10–20 minutes. If a patient complained of pain or neck swelling, a repeat US examination was performed in order to evaluate possible complications.
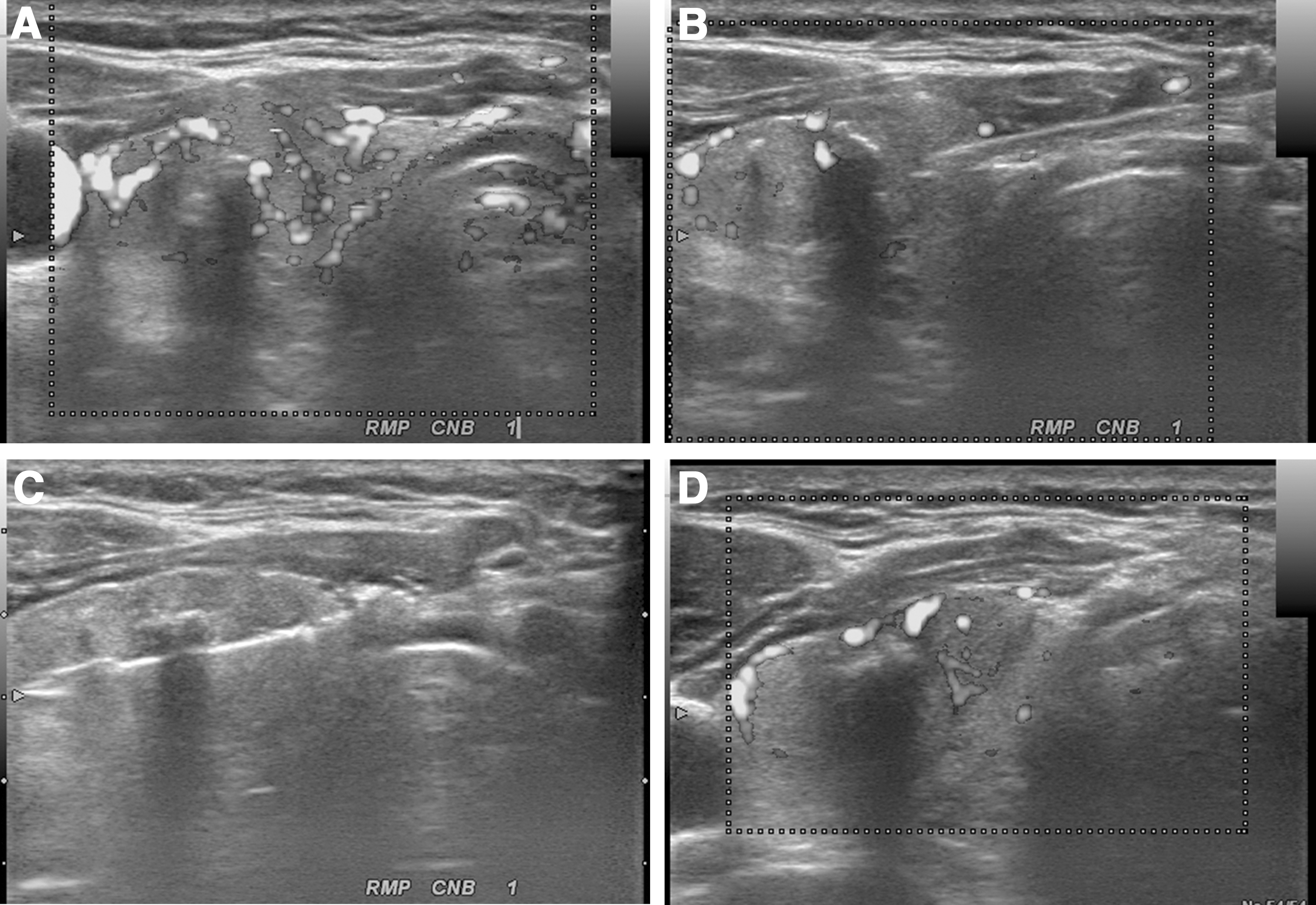
US-guided CNB for a thyroid nodule located in the right thyroid gland.
Cytohistology analysis
CNB specimens were reviewed by our staff histopathologists, although the diagnostic criteria for CNB have not yet been standardized for thyroid nodules. For this study, histology diagnoses were categorized into the same six categories as The Bethesda System—nondiagnostic, benign, AUS/FLUS, follicular neoplasm/suspicious for a follicular neoplasm, suspicious for malignancy, and malignant—according to the histopathology results of the CNB. A nondiagnostic CNB reading included the absence of follicular thyroid tissue, the presence of only a normal thyroid gland, and tissue containing only a few follicular cells and therefore insufficient for diagnosis. The AUS/FLUS reading for the CNB included nodules in which some atypical cells were present but were not diagnostic of suspicious malignancy or malignancy, and included cellular follicular nodules in which a distinction between follicular neoplasm and hypercellular hyperplastic nodule was not possible. Cases of AUS/FLUS were subclassified according to the morphologic features noted in the cytopathology reports (10,13,15,19). Group AUS was used for the cases that demonstrated nuclear atypia, such as the presence of occasional nuclear grooves, an abnormal chromatin pattern, or nuclear overlapping and crowding, those being anomalous findings within individual cells. These findings are concerning for the presence of a papillary thyroid carcinoma. Group FLUS was used for the cases that showed low cellularity with a predominantly microfollicular pattern and no or minimal colloid, which is concerning for a follicular neoplasm. Nodules with histology features favoring follicular neoplasm were categorized as ‘suspicious for follicular neoplasm or follicular neoplasm. We also analyzed the type of malignancy after surgery.
Analysis of the US findings
US images were independently reviewed retrospectively by two radiologists (J.H.B. and E.J.H.). Neither reviewer had any information regarding a patient's clinical history, previous imaging results, or histologic results. Any diagnostic discrepancies between the two reviewers were resolved by consensus. The US findings of the nodules were evaluated for the following features: size (maximal diameter); shape (oval-to-round, irregular, or taller than wide); margins (well defined, ill defined, or spiculated); echogenicity (hyperechoic, isoechoic, hypoechoic, or markedly hypoechoic); the presence of echogenic dots suggesting microcalcifications; and the presence of macrocalcifications. The US criteria for malignant nodules were a taller-than-wide shape, spiculated margin, marked hypoechogenicity, and the presence of micro- or macrocalcifications (20,21).
Statistical analysis
Statistical analysis was performed using SPSS for Windows v19.0 (IBM Corp., Armonk, NY). We compared the demographic data between Group AUS and Group FLUS, and performed the chi-square test and the unpaired Student's t-test to demonstrate differences in patient sex, age, nodule size, and CNB number.
The chi-square test or Fisher's exact test was used to compare the categorical variables, that is, the six categories of The Bethesda System, including the malignancy risk and type, management recommendations, malignant US findings, and distribution of CNB readings between Group AUS and Group FLUS.
For both groups, we calculated the diagnostic value of CNB for the diagnosis of thyroid malignancy. A statistical difference was defined as p<0.05.
Results
Demographic data
Table 1 shows the comparison of the demographic data between Group AUS and Group FLUS. The nodule size was larger in Group FLUS (mean=22.2 mm; range=3–70 mm) than in Group AUS (mean=13.2 mm; range=4–35 mm; p=0.005). The mean number of CNB procedures was significantly higher in Group AUS (mean±SD=1.26±0.49; range=1–2) than in Group FLUS (mean±SD=1.14±0.36; range=1–2; p=0.002).
AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; CNB, core-needle biopsy.
Comparison of malignancy risk and type
Final diagnoses were obtained in 142 nodules (Group AUS, n=51; Group FLUS, n=91) after surgical and clinico-radiological follow-up. Figure 1 shows the numbers of surgical and clinic-radiological follow-up in each group. The CNB results and follow-up showed that the malignancy risk of Group AUS/FLUS was 32.4% (46/142), and Group AUS (65%, 33/51) was significantly higher than that of Group FLUS (14.3%, 13/91; p<0.001; Table 2). Among the patients with malignancy, the occurrence of papillary thyroid carcinoma was significantly higher in Group AUS (96.7%, 32/33) than in Group FLUS (69.2%, 9/13; p=0.018). All papillary thyroid carcinomas were classical papillary thyroid carcinomas. Follicular carcinoma was seen more frequently in Group FLUS (30.8%, 4/13) than in Group AUS (3.3%, 1/33; p=0.018). However, benign results were significantly higher in Group FLUS than in Group AUS (85.7%, 78/91 vs. 35.3, 18/51%; p<0.001). When we just compared distribution of CNB readings between Group AUS and Group FLUS regardless of follow-up (n=191), malignant readings (suspicious for malignancy: 8.3%, 7/84 vs. 1.9%, 2/107; and malignant: 40.5%, 34/84 vs. 7.5%, 8/107) were significantly higher in Group AUS than in Group FLUS (p<0.001), and benign readings (58.9%, 63/107 vs. 28.6%, 24/84) were significantly higher in Group FLUS than in Group AUS (p<0.001).
Data are expressed as n (%).
Comparison of the final diagnosis between Group AUS and Group FLUS.
FN, follicular neoplasm; SFN, suspicious of follicular neoplasm.
Comparison of the management recommendations
Table 3 compares the management recommendations of Groups AUS and Group FLUS. Surgery was recommended more often in Group AUS than in Group FLUS (57.8%, 46/84 vs. 19.6%, 21/107; p<0.001). In contrast, clinical follow-up was recommended more frequently in Group FLUS than in Group AUS (58.9%, 63/109 vs. 28.6%, 24/84; p<0.001).
Data are expressed as n (%).
Inconclusive diagnoses of CNB, including nondiagnostic and AUS/FLUS readings, were found in 19.4% (n=37). In Group AUS, 16.7% (n=14) of the CNB readings were inconclusive, and in Group FLUS, 21.5% (n=23) of the CNB readings were inconclusive. There was no statistically difference in the inconclusive rate between Group AUS and Group FLUS patients (p=0.463).
Comparison of malignant US findings
Malignant US findings were statistically more frequent in Group AUS (76.5%, 39/51) compared to Group FLUS (52.7%, 48/91; p=0.007; Fig. 3). Each malignant US finding was significantly more common in Group AUS than in Group FLUS, that is, spiculated margin (39.2% vs. 8.8%; p<0.001), marked hypoechogenicity (47.1% vs. 26.4%; p=0.016), and micro- or macrocalcifiation (60.8% vs. 41.8 %; p=0.036), except for that of a taller-than-wide shape (15.7% vs. 8.8%; p=0.270).
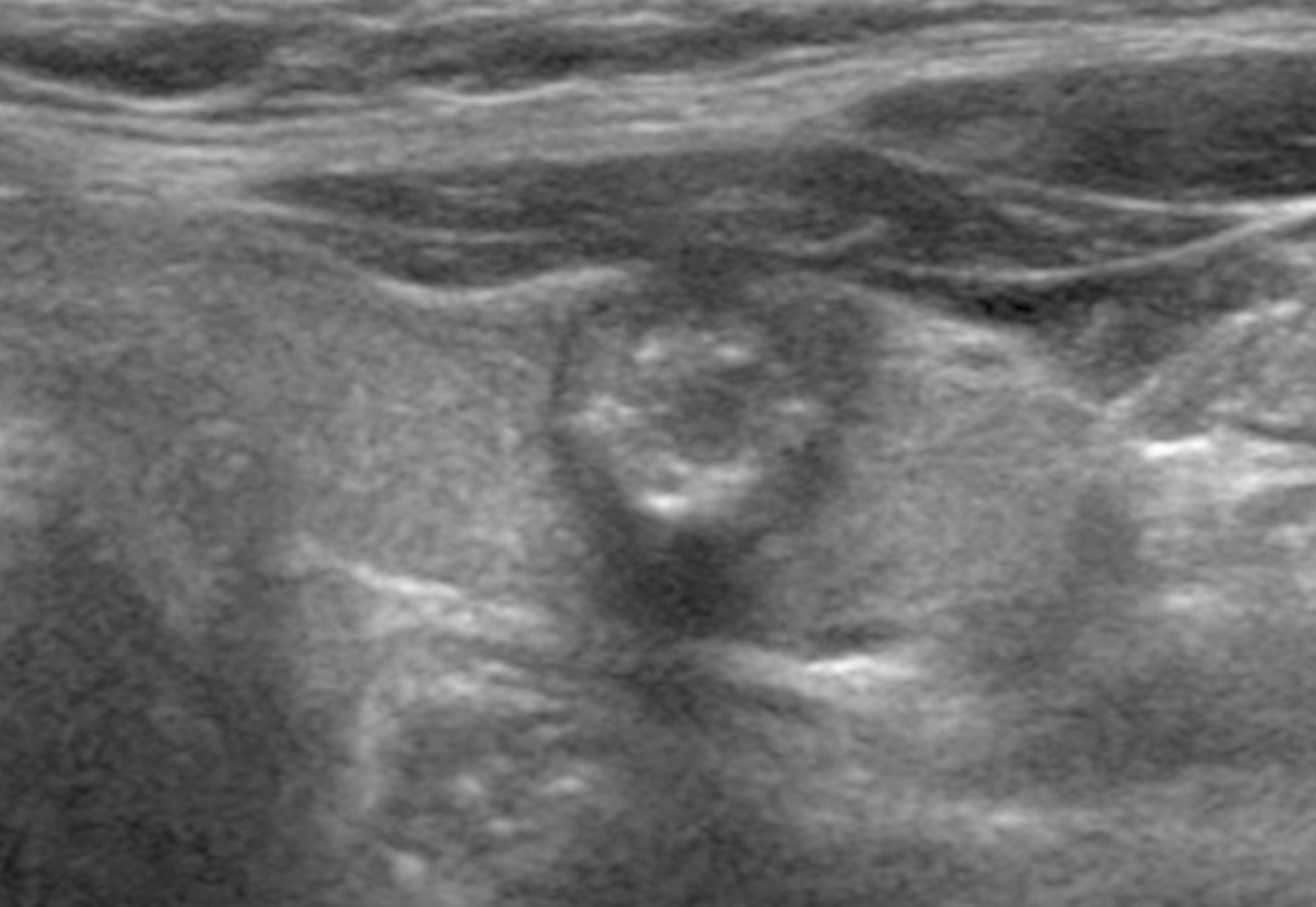
US findings of Group AUS in a 49-year-old woman. Transverse US image of the thyroid nodule shows malignant findings, including microcalcification and spiculation. US-guided CNB histology and surgical pathology revealed a papillary thyroid carcinoma.
Comparison of malignancy risk with adjunctive, malignant US findings
Table 4 lists the comparison of the malignancy risk with adjunctive, malignant US findings between Group AUS and Group FLUS patients. The malignancy rate was 76.9% if thyroid nodules in Group AUS patients had malignant US findings, although there was no malignancy detected in the final diagnosis in Group FLUS patients without malignant US findings (Fig. 4).
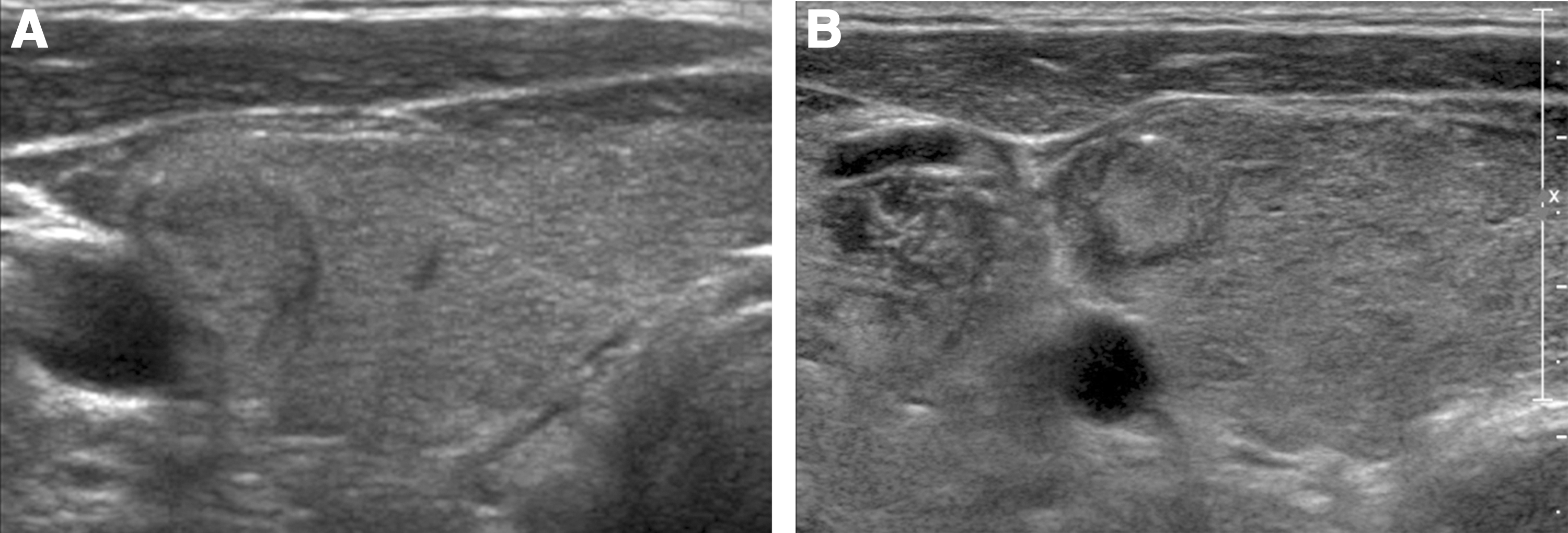
US findings of Group FLUS in a 52-year-old woman. Transverse US image of the thyroid nodule shows an isoechoic solid mass
Diagnostic value of CNB for detecting malignancy
Using the criteria of The Bethesda System category suspicious for malignancy and malignant, the diagnostic accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of CNB for detecting thyroid malignancy were 95.8%, 87%, 100%, 100%, and 94.1% respectively. There was no case of a false-positive diagnosis, although there was one false-negative case that was diagnosed as AUS on CNB.
Complications
There were no serious complications requiring further intervention or patient hospitalization. In one (0.5%) patient, neck swelling, pain, and perithyroidal hematomas occurred. These symptoms were relieved following manual compression for one hour. There were no cases of needle-track metastases seen at follow-up.
Discussion
Our study demonstrates that Group AUS showed a significantly higher risk of malignancy as well as malignant US findings than Group FLUS. Regarding the management recommendations, surgery is recommended more frequently in Group AUS, and clinical follow-up is recommended more frequently in Group FLUS. US-guided CNB showed a 95.8% diagnostic accuracy for malignancy and 19.4% of inconclusive diagnoses in the thyroid nodules with previous AUS/FLUS FNA readings.
The Bethesda System for Reporting Thyroid Cytopathology suggested that the AUS/FLUS category was the optional group for FNA readings regarding thyroid nodules that were not clearly benign, suspicious, or malignant (4,22). Based on previous studies, the prevalence of this category is 3–20.5%, and the risk of malignancy was reported as 6–48% (3 –11). The wide range of both the prevalence and risk of malignancy may reflect heterogeneous histology results. Recently, several studies have classified the AUS/FLUS category into subcategories. Among these subcategories, the risk of malignancy for the nuclear atypia group (32.6–60%) was significantly higher than that for the microfollicular architecture group (7–34%) (9,12,13,15,23,24). By recognizing that the nuclear atypia group demonstrates a much higher risk of malignancy than that of the other AUS/FLUS subcategories, the need for reassessing the original clinical recommendations within The Bethesda System emerges (13). Our study shows a 32.4% of risk of malignancy in the AUS/FLUS category. However, Group AUS showed a significantly higher risk of malignancy, surgery rate, and malignant USG findings than did Group FLUS. There was also a statistical difference in the distribution of CNB histology results between Group AUS and Group FLUS. Malignant readings were significantly higher in Group AUS than in Group FLUS, and benign readings were significantly higher in Group FLUS than in Group AUS. In addition, as Group FLUS without malignant US findings showed no malignancy in the final diagnosis, we suggest that Group AUS should be followed more closely and the rebiopsy should be performed sooner than in Group FLUS patients. However, clinical follow-up may be adequate management for nodules found in Group FLUS patients in whom malignant US findings were not found in clinical practice. Moreover, we expect that the guidelines for the clinical management of the AUS/FLUS category may be further refined because of the different risk of malignancy, management recommendations, and malignant US findings between the two groups.
A recent study (18) prospectively compared CNB and repeat FNA in nodules with previous AUS/FLUS FNA readings and showed that CNB significantly reduced inconclusive—that is, nondiagnostic or AUS/FLUS—readings compared with repeat FNA (26.7% vs. 49.1%; p<0.001). Our larger data set (N=191) also suggests that CNB can effectively reduce inconclusive diagnoses (19.4%) compared with repeat FNA in nodules with previous AUS/FLUS FNA readings, as seen in published literature reports (20–49.1%) (6,16 –18). Based on these observations, CNB can reduce the frequency of repeat FNA or unnecessary diagnostic surgery. Our study also shows a high diagnostic rate similar to that seen in the previous results of Na et al. (18). In our study, the high diagnostic value of CNB for detecting thyroid malignancy, mostly papillary thyroid carcinomas, may be primarily explained by the lower rate of inconclusive results and the low rate of a false-negative diagnosis. This factor may be related to the advantages of CNB, which include larger tissue samples, less operator dependency if the needle successfully penetrates the nodule, and its ability to assess the histological architecture and relationship of a nodule to the adjacent thyroid tissue (18,25). Recently, several reports have also demonstrated that molecular tests for the detection of genetic alterations and differential gene expression may enhance the diagnostic value of FNA of thyroid lesions (26,27).
Our study has several limitations. First, our case evaluation was retrospective, and the high prevalence of malignancy in our study may be related to a bias in patient selection. Only a small percentage of AUS/FLUS patients (191/3338) was enrolled. Large-scale prospective studies will be needed to determine the different management plans required for Groups AUS and Group FLUS, as well as the usefulness of CNB. The second limitation consists in the loss of follow-up in 39% of Group AUS. Third, because many of the benign nodules were not confirmed by surgery, the number of thyroid nodules with a final diagnosis is limited. However, this limitation could be explained by the recommendations of The Bethesda System, in which clinical follow-up is recommended for benign FNA readings. Fourth, we did not compare between initial FNA versus a combination of CNB and FNA. Finally, the lack of diagnostic category standardization in the histological diagnosis of CNB requires further investigation.
In conclusion, US-guided CNB demonstrates that patients with previous nuclear atypia FNA readings (Group AUS) showed a higher risk of malignancy and a higher frequency of malignant CNB readings, were more often surgical candidates, and exhibited more malignant US findings than previous microfollicular architecture FNA readings (Group FLUS). Further management guidelines for patients with nuclear atypia readings (Group AUS) should therefore differ from those for patients with microfollicular architecture (Group FLUS).
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.