
Abstract
Background:
There continues to be controversy regarding which clinicopathological features confer a higher risk of adverse outcome in papillary microcarcinomas (PMC). The aim of this study was to assess the prognostic value of a meticulous histologic examination in PMC.
Method:
All papillary thyroid carcinoma <1 cm in size without associated larger thyroid carcinomas, identified between 1977 and 2002, were categorized as PMC and subjected to a meticulous histopathologic examination by 2 thyroid pathologists.
Results:
148 PMC patients fulfilled the inclusion criteria. Within PMC, young age, male sex, tumor multicentricity, extrathyroidal extension, and infiltrative and larger tumor (≥0.5 cm) correlated with the presence of >1 cm metastatic node (MN) or >3 MN at presentation (p<0.05). With a median follow-up of 9.9 years, only 1 (0.7%) of 134 PMC patients died of thyroid carcinomas and 3 (2.2%) had recurrences in the neck. The patient who died had harbored a poorly differentiated carcinoma in his MN. The presence of MN and especially a large MN (>1 cm) correlated with worse recurrence-free survival (p=0.005 and p<0.0001, respectively). Except for one, all individuals with clinically adverse outcomes had >1 cm MN. Patients whose MNs were predominantly composed of poorly differentiated carcinoma or tall cell variant papillary thyroid carcinoma had a significant shorter recurrence-free survival (p<0.0001). Only 1 of 80 radioactive iodine–naïve PMC patients with absent or small MN (≤1 cm) had recurrence with a median follow-up of 9.2 years.
Conclusions:
(i) The size and histotype of the MN are predictors of outcome in PMC and should be recorded. (ii) The very rare PMC patients who suffer recurrence or even die of disease have usually aggressive histopathologic features at presentation. (iii) PMC patients with nodal disease that is small or absent at presentation are at a very low risk of recurrence and may be spared radioactive iodine therapy.
Introduction
S
There continues to be controversy regarding clinicopathological features that may confer a higher risk of adverse outcomes in PMC. Some (5 –8), but not all, studies (9,10) have shown that larger PMC (>5–7 mm) are associated with increased recurrence, increased lymph node metastasis, and/or higher risk of having extrathyroidal extension (ETE). ETE and multifocal disease were found to be associated with higher risk of recurrence and/or nodal metastasis at diagnosis in some (9,11,12), but not all, series (10). Some authors regard the mere presence of lymph node metastases as an indication for aggressive therapy (9,13), whereas others report no impact of small subclinical nodal metastases on survival (14). Despite the numerous studies dealing with the prognosis of PMC, certain histopathologic variables, such as tumor subtyping of the primary or the metastatic deposits in the lymph node, have been rarely or not evaluated at all. There is therefore a need to better prognosticate patients with PMC.
Toward that goal, we undertook a meticulous histopathologic examination of 148 PMC patients focusing on histologic tumor subtyping with the hope of identifying at presentation those patients at risk for adverse behavior.
Materials and Methods
Patient population and inclusion criteria
The institutional database was searched for all cases with a diagnosis of thyroid carcinomas treated at Memorial Sloan-Kettering Cancer Center between January 1977 and December 2002. The slides from the cases included in the study were examined by two head and neck pathologists with special interest in thyroid neoplasia (R.G. and M.R.). The pathologists were blinded to the clinical outcome of the patients. The thyroid carcinomas were classified according to the last World Health Organization classification of endocrine tumors except for papillary thyroid carcinoma (PTC), tall cell variant, and poorly differentiated thyroid carcinomas (15). The latter tumor was defined as a carcinoma displaying high mitotic activity (≥5 mitosis/10 high-power fields, 400×) and/or tumor necrosis, and showing follicular cell differentiation at the morphologic or immunohistochemical level. Tall cell variant was characterized as a papillary carcinoma composed of more than 50% of tall cells. The latter cell type was defined as having a height at least twice its width with an oncocytic cytoplasm. Patients were included in the study as PMC patients if they had only uni- or multicentric subcentimeter PTC as their primary tumor. Patients with PMC associated with larger thyroid carcinomas (≥1 cm) were not categorized as PMC patients. The study was approved by the Institutional Review Board of Memorial Sloan-Kettering Cancer Center.
Histopathologic analysis
The largest dimension of the carcinoma was based on review of the gross pathology report and direct microscopic measurement of the tumor on the slides. The mitotic rate of the tumor was determined by counting 10 contiguous high-power fields (400×) using an Olympus microscope (U-DO model BX-40; Olympus America Inc., Melville, NY). Using that microscope type, we found that these 10 high-power fields correspond to 2.4 mm2. Tumor necrosis was defined by a “comedo-like” appearance composed of degenerating cytoplasm and punctate, karyorrhectic nuclear debris. Vascular invasion was categorized as present or absent. Invasion of the tumor capsule defined as transcapsular penetration was recorded. A tumor was considered infiltrative if the carcinoma cells were present in between non-neoplastic thyroid follicles. ETE was defined as tumor cells invading beyond the thyroid capsule into peri-thyroid soft tissue or organs. ETE was subdivided into (i) none; (ii) focal (presence of 1–2 microscopic foci of ETE measuring ≤1 mm each); (iii) extensive (presence of >2 microscopic foci of ETE [≤1 mm in size each] or any foci >1 mm in size). The type of peri-thyroid tissue or organ invaded by the tumor was recorded (e.g., adipose tissue, skeletal muscle, recurrent nerve, trachea, and esophagus). Multicentricity was defined as the presence of two or more foci of carcinoma in the thyroid. The status of the resection margins was reported as positive (tumor present at the surgical margin) or negative (no tumor at surgical margin). The number of lymph nodes examined microscopically as well as the number of nodes with metastatic carcinoma were recorded. On the basis of gross and microscopic examination of the surgical specimen by the pathologist, the greatest diameter of the largest metastatic node (MN) was measured as well as the largest size of the largest metastatic tumor focus. Significant nodal disease was defined on the basis of the size of the largest MN and the number of nodes involved by tumor. The presence of >1 cm positive node was considered significant, while smaller MNs or absence of nodal metastases was classified as minimal nodal disease. With regard to the number of positive nodes, the finding of >3 MNs was categorized as significant, while the presence of a smaller number of positive nodes or absence of nodal metastases was defined as minimal nodal tumor burden. The most predominant histologic subtype of tumor in the lymph node was recorded. The most aggressive thyroid carcinoma subtype in lymph node was classified as poorly differentiated thyroid carcinoma, tall cell variant PTC, classical PTC, or follicular variant PTC. Extranodal extension was documented as present or absent.
Clinical parameters
The patients' electronic medical records were reviewed for the age at diagnosis, type of surgery, and adjuvant treatment including radioactive iodine (RAI) therapy. The type of cervical lymph node dissection/biopsy was recorded as central; lateral; central and lateral; or other. The latter category consists solely of peri-thyroidal lymph nodes removed with the thyroid specimen or superior mediastinal lymph nodes. The date of initial surgery and last date of follow-up were documented. The patient disease status at recurrence or follow-up was based on a combination of clinical and imaging assessments. These evaluations included history taking, physical examination, RAI scanning, cross-sectional imaging, and/or positron emission tomography scanning as well as serum thyroglobulin levels if the latter were available. The status at last follow-up was recorded as follows: no evidence of disease; alive with disease; or dead of other causes and dead of disease.
Statistical analysis
The two-tailed Fisher exact test was used to assess the relationship between categorical variables. Survival probabilities were estimated by the Kaplan–Meier method and compared using the log-rank test. A probability (p) value ≤0.05 was considered significant. Recurrence-free survival (RFS) was defined as the time interval between the date of initial surgery and the date of first recurrence. Disease-specific survival was defined as the presence or absence of dead of disease at the last follow-up. The time interval to dead of disease was calculated from the initial surgery to the last follow-up. This statistical analysis was carried out using commercially available software: SPSS for Windows, version 17.0 (SPSS Inc., Chicago, IL) and JMP version 4.0 (SAS Institute Inc., Cary, NC).
Results
Incidence of PMC
Out of the 670 PTC patients reviewed microscopically in the study period, there were 148 (22%) PMC patients as defined in
Clinicopathologic features at presentation of PMC
Table 1 displays the clinicopathologic features of the 148 patients with PMC identified for this study. Patients presenting with palpable adenopathy comprised 18% of the study cohort and were significantly younger (median 33.5 vs. 48 years), more often males (50% vs. 16%), had larger PMC (median 0.65 vs. 0.4 cm), and had more infiltrative tumors (100% vs. 74%) than the remainder of the patient population (p<0.05). Thirty-nine patients (26%) were administered RAI therapy, while 104 (70%) of individuals did not receive it. RAI therapy status was not available for five patients. Of the 69 patients whose surgical specimen contained lymph nodes, the type and site of lymph node dissection/biopsy were as follows: central compartment, 16 (23%); lateral compartment, 28 (40.5%); central and lateral compartments, 9 (13%); other, 15 (22%); site not specified, 1 (1.5%).
In one case, the tumor could not be subtyped.
Extrathyroid extension could not be evaluated in three patients.
Margin status was not assessable in one case.
In one patient, the size of the largest metastatic node could not be accurately assessed.
In two cases, the histotype could not be evaluated in the lymph node because of inadequate lymph node material.
In two patients, extranodal extension was equivocal or could not be assessed because of inadequate material.
Multicentricity defined as >1 focus of carcinoma could not be accurately evaluated in two cases.
In one instance, the extent of surgery was not clear.
FVPTC, follicular variant of papillary thyroid carcinoma; PTC, papillary thyroid carcinoma; TT, total thyroidectomy.
Clinicopathologic correlates of significant nodal metastatic disease at presentation in PMC
Tables 2 and 3 show the clinicopathologic correlates for significant nodal disease at presentation. When defined by size, significant nodal disease occurred more often in young individuals and male patients (p=0.004 and 0.026, respectively). A similar correlation was also found with infiltrative tumor (p=0.045). It is, however, tumor multicentricity and ETE that correlated very strongly with the presence of significant nodal disease (measured by MN size) (p=0.0001).
Absence means no positive nodes or largest positive node ≤1 cm. Significant metastatic disease largest positive node >1 cm.
One case was not included in this table since the exact size of the metastatic node could not be accurately assessed.
One tumor could not be subtyped since the slides were misplaced at the time of subclassfication.
Others were cribriform-morular, columnar, and solid variant.
Extrathyroid extension could not be evaluated in three patients.
Margin status was not assessable in one case.
In one patient, the exact nature of the surgery was not clear.
One tumor could not be subtyped since the slides were misplaced at the time of subclassfication.
Other were cribriform-morular, columnar and solid variant.
Extrathyroid extension could not be evaluated in three patients.
Margin status was not assessable in one case.
In one case, the extent of surgery was not clear.
In regard to the number of involved nodes, younger patients had a much higher incidence of significant nodal disease (p=0.0045), while sex did not affect the number of MNs (p=0.1165). Primary tumors with the largest focus ≥0.5 cm and infiltrative microcarcinomas had a larger number of MNs (p=0.047 and 0.016, respectively). As was found with MN size, tumor multicentricity and ETE correlated very strongly with significant nodal disease (defined as >3 positive nodes) at presentation (p=0.0001).
Clinicopathologic correlates of multicentricity in PMC
Younger patients had a much higher incidence of multicentric PMC (i.e., >1 primary tumor focus) (p=0.0025). Multicentric tumors were more often infiltrative, displayed more frequently ETE, and harbored larger primary tumors than their unicentric counterparts (p<0.01). As mentioned above, there was a very strong correlation between multicentricity and the presence of significant nodal disease whether defined on the basis of tumor size or number of positive nodes (p=0.0001). Patients with multicentric PMC were more often subjected to total thyroidectomy (p=0.0001) than those with unifocal tumors.
Outcome analysis
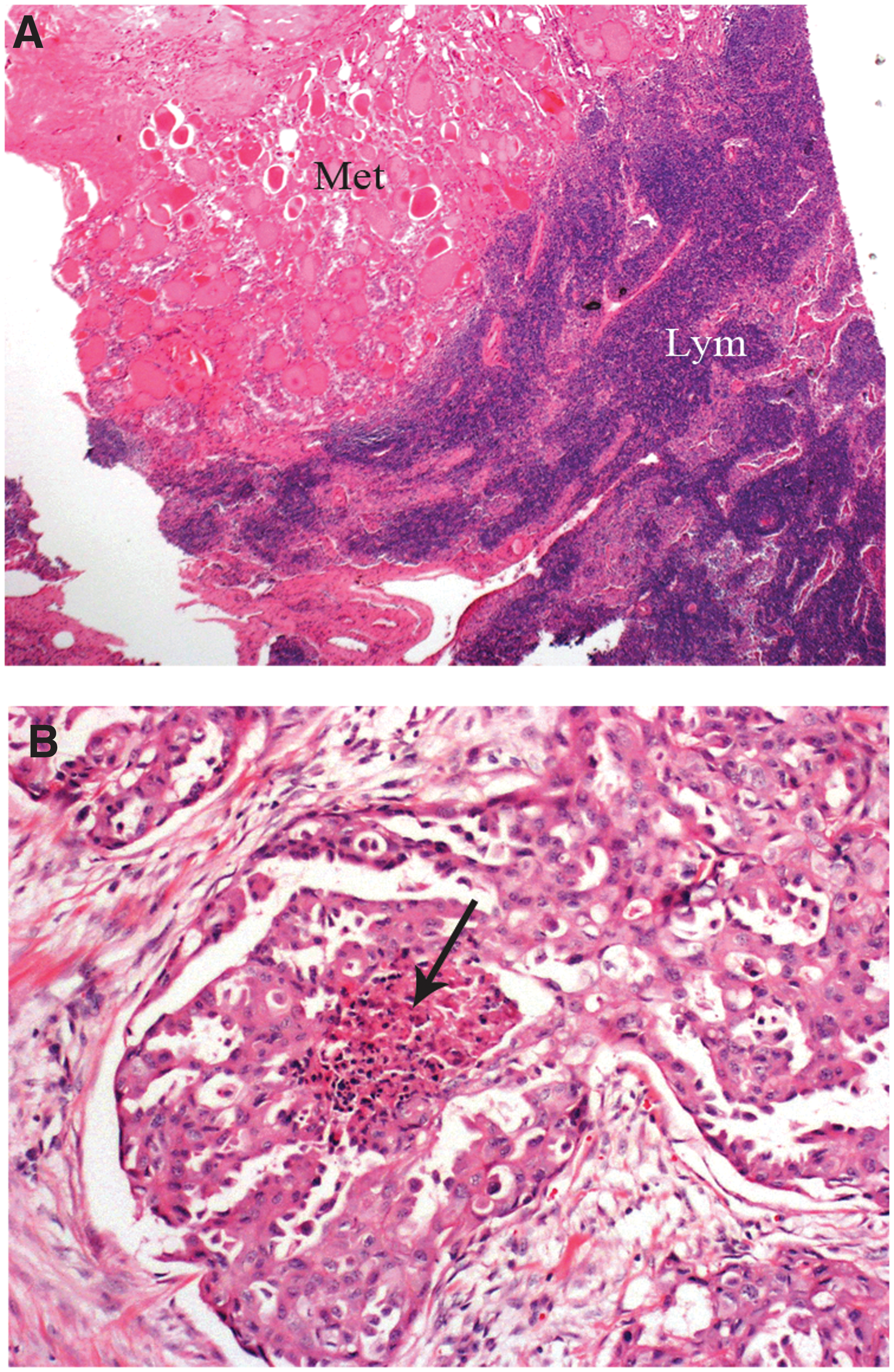
Follow-up data were available on 134 patients. The median follow-up was 9.9 years (range 0.2–28 years). Only one (0.7%) of the patients died of thyroid carcinoma. This 57-year-old man presented with a left neck mass and underwent left lobectomy and left neck dissection. The specimen revealed six foci of PMC ranging from <0.1 to 0.3 cm in size (Fig. 1). Five of those microcarcinomas were growing as infiltrative follicular variant of PTC and 1 as an infiltrative classical PTC. He had 8 MNs (1.5 cm largest positive node) containing metastatic poorly differentiated thyroid carcinoma (Fig. 2). He was treated by completion thyroidectomy and RAI therapy but developed metastatic carcinoma in the neck nodes 10 months after diagnosis. A computerized tomography scan revealed lung metastases 1 year after diagnosis. Of note, no computerized tomography scan was performed at presentation. Three years after presentation, he died of extensive metastatic disease in lung, right neck, and intrathoracic nodes.
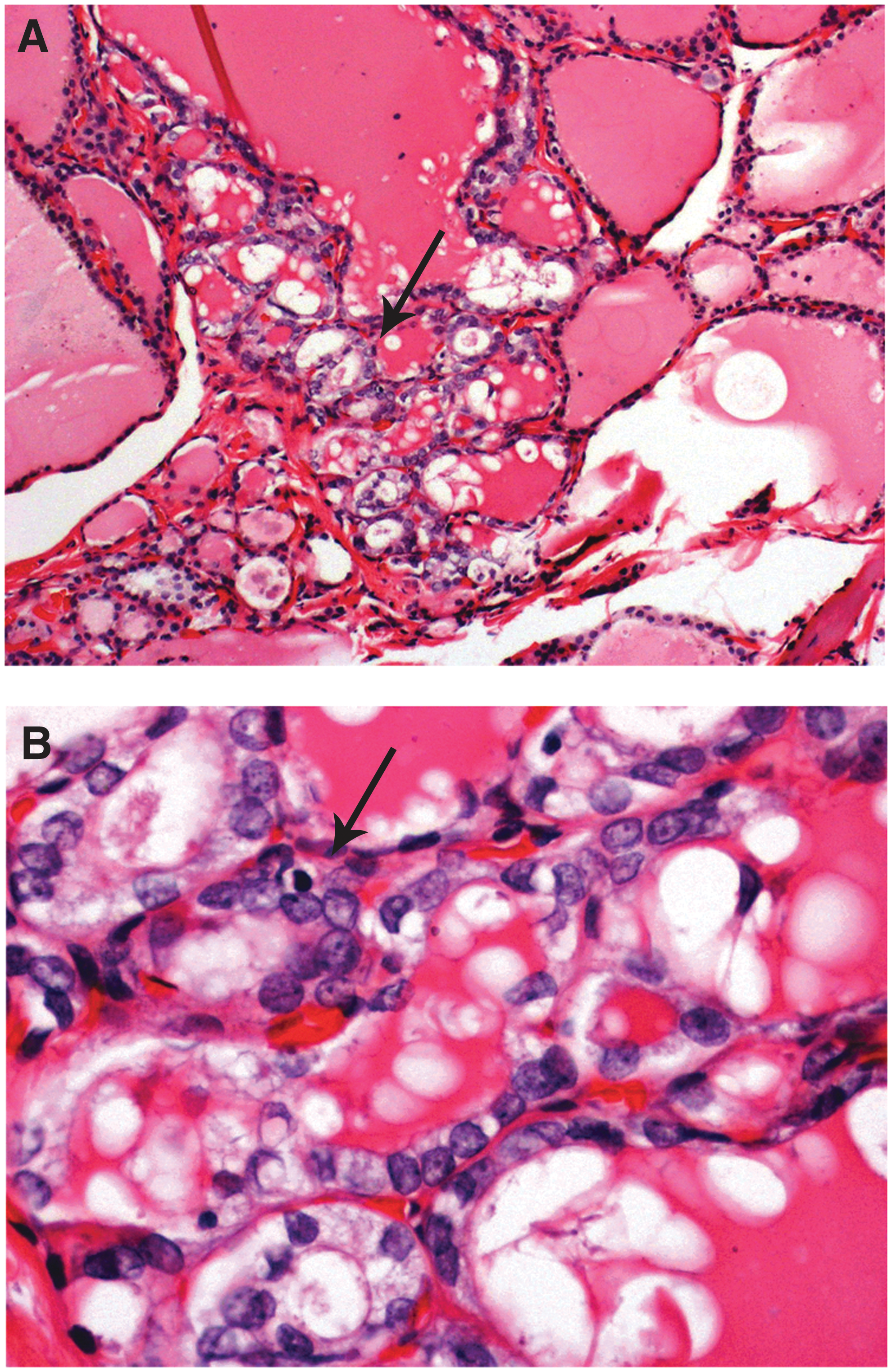
A 57-year-old man with six foci of papillary microcarcinomas who died of thyroid carcinoma 3 years after presentation.
Same patient as in Figure 1.
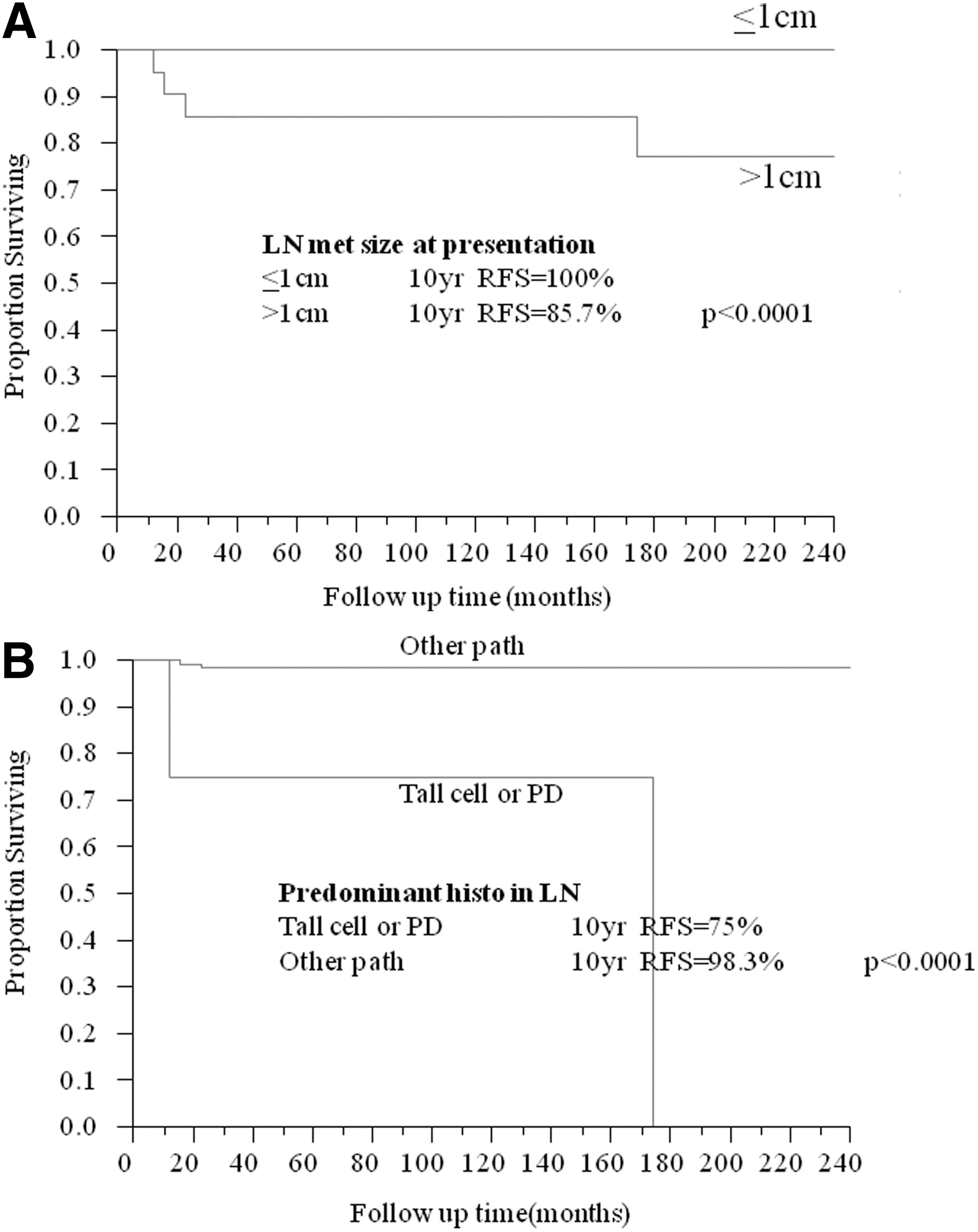
Three (2.2%) of the patients had histologically confirmed recurrences in the neck 1.2, 2, and 14 years after diagnosis but were alive at the last follow-up. The clinicopathologic features at presentation of all four patients who recurred or died are shown in Table 4. Except for one patient, all individuals with clinically adverse outcomes had significant nodal disease (>1 cm positive node measured microscopically) at presentation. Only one of these three patients with large positive nodes and adverse behavior had palpable adenopathy at presentation. In the whole patient population, the presence of nodal metastatic disease and especially a large MN (>1 cm) correlated with worse RFS (p=0.005 and p<0.0001, respectively) (Fig. 3A). Patients whose predominant histotype in the MN was poorly differentiated carcinoma or tall cell variant PTC had a significantly shorter RFS (75% at 10 years) than those whose predominant histotype consisted of classic and follicular variant PTC (98% at 10 years) (p<0.0001) (Fig. 3B). The mere presence of poorly differentiated carcinoma or tall cell variant PTC in the MN correlated also with decreased RFS (p=0.04). Age, sex, tumor infiltration, size of the largest primary tumor focus, tumor multicentricity, extrathyroid extension, the number of MNs, and extranodal extension did not affect RFS (p>0.05). Eighty patients with absent or small nodal metastases (≤1 cm in size) did not receive RAI therapy. Table 5 shows the clinicopathologic features and outcome in this subset of individuals. Only one (1%) of those 80 patients recurred with a median follow-up of 9.2 years.
Lung metastasis found one year after diagnosis.
DM, distant metastasis; DOD, death of disease; ENE, extranodal extension; F, female; FVPTC, follicular variant of papillary thyroid carcinoma; LN, lymph node; M, male; Met, metastasis; neg, negative; PD, poorly differentiated thyroid carcinoma; pos, positive; RAI, radioactive iodine; Rec, recurrence; TCV, tall cell variant of papillary thyroid carcinoma; TT, total thyroidectomy.
In two cases, the extrathyroid extension status could not be accurately assessed.
Discussion
The incidence of PMC (22%) in our PTC population is very close to the frequency reported in large studies (9,16). The age at presentation (median 46 years), the male:female ratio, and the nodal metastatic rate (31%) were also similar to the values previously published in these large series (9,16). The frequency of ETE (20%) in our patient cohort is in congruence with some (9), but not all, studies (16,17). This discrepancy could be related to the fact that the microscopic diagnosis of minimal ETE is subject to significant interobserver variability between pathologists. The higher incidence of infiltrative follicular variant PTC in the PMC (17%) compared with their frequency in PTC in general (reported as extremely rare to 4%) is intriguing (18,19). The infiltrative follicular variant of PTC was shown to be different from encapsulated FVPTC in regard to its metastatic spread, behavior, and molecular profile (20). The presence of a relatively high number of small infiltrative FVPTC in PMC is another argument in favor of this subgroup of FVPTC being different from encapsulated FVPTC. Indeed, if these two subtypes of follicular variant PTC were related, one would expect a tumor to start as encapsulated and appear infiltrative at a later stage in its evolution.
While the mere presence of nodal metastasis was shown to increase recurrences in PMC by some authors (9), worse outcome was restricted to only patients with palpable nodal disease rather than microscopic metastasis in other publications (21). It is therefore important to identify the features of the primary microcarcinoma that correlate with significant nodal disease. There is very little data on the subject in the literature (21). We found that young age, male sex, infiltrative and large PMC (≥0.5 cm) correlate with significant nodal disease. However, tumor multicentricity and ETE correlated most strongly with the presence of a significant nodal tumor burden whether defined by the size of MN (>1 cm) or the number of nodal metastases (>3) (p=0.0001). These findings may have important clinical implications. For example, the presence of multicentricity and ETE in a young male patient with PMC may prompt more regular neck ultrasonography examination in search for clinically relevant nodal disease. It remains to be seen whether molecular analysis of the primary PMC helps predict significant nodal disease in view of a recent article reporting a correlation between BRAFV600E and the mere presence of nodal metastases (22).
The death rate from PMC in this study was very low (<1%), similar to most previous publications that report a mortality rate of 0–2% (6,9,21,23 –26). The overall recurrence rate was also low (3%) in congruence with some, but not all, studies. Indeed, the recurrence rates from PMC in the literature vary widely, ranging from 1.6% to 25% (6,13,16,21,23 –27). These discrepant results may be due to (i) differences in the size criterion for PMC (some studies use 1.5 cm as a cutoff), (ii) more sensitive disease detection in series where the majority of patients had both thyroid lobes removed, and (iii) the inclusion of persistent disease in the estimation of the recurrence rate (26). It is noteworthy that 3 of the 4 patients who had recurrence, including the patient who died of PMC, harbored large MNs (>1 cm) at presentation. By the Kaplan–Meier analysis, patients with large (>1 cm) positive nodes had a significantly shorter RFS (87% at 10 years) than the rest of the study population (100% at 10 years, p<0.0001). These findings are in accordance with the study of Wada et al. (21), who found a higher recurrence rate in patients with palpable nodes compared with those with subclinical nodal disease. In regard to measurement of nodal disease, we used the size of the largest MN rather than the size of the largest metastatic tumor focus for our analysis since the former correlates much better with outcome as shown in a previous study from our group (28). The lack of correlation of the metastatic focus size could be due to the difficulty in assessing metastatic tumor burden in a lymph node using a unidimensional measurement of the largest metastatic deposit (28). A previously seldom investigated prognostic variable in PMC is the histotype of the lymph node metastases. We categorized the tumor histotype in the lymph nodes as aggressive (tall cell variant PTC, poorly differentiated) and indolent (follicular variant and classical PTC), and quantified each component. Individuals whose predominant histotype was tall cell variant PTC or poorly differentiated carcinoma had a much worse RFS (75% at 10 years) compared with those harboring indolent subtypes of PTC in their nodal disease (98.3% at 10 years, p<0.0001). This correlation remained significant (although to a lesser degree) when the aggressive histotype constituted a minor component of the lymph node metastasis (p=0.04). These results are in congruence with those of Piana et al. (29), who reported three fatal cases of PMC that all presented with massive lymph node metastases showing morphological evidence of tumor progression (tall cell features, poorly differentiated areas, and high-grade cytologic features).
It appears from the above data that the very rare PMC patients who suffer recurrence or die of the disease have aggressive histopathologic features at presentation (Table 4). The vast majority of these features can therefore be identified at presentation if the pathologist performs a meticulous histologic examination. The latter should include size measurement of the nodal metastases and subtyping of the metastatic deposits in the lymph node. It is also possible to define a subset of PMC at very low risk of recurrence, who may be spared RAI therapy. Indeed, this study population included 80 patients with absent or low-volume nodal metastases (≤1 cm in size) who did not receive RAI therapy. With a median follow-up of 9.2 years, only one of those patients suffered recurrence and was alive at the last follow-up.
Because of the extremely indolent behavior of PMC, an attempt at nonsurgical observation has been undertaken a few years ago by Japanese investigators (14). Patients were advised surveillance if they lacked clinically apparent lymphadenopathy (≥1 cm), distant metastasis, or extrathyroid or extranodal extension by imaging studies. No molecular analysis of the fine-needle aspiration was performed. The challenge for the future in PMC is to identify prognostic factors of adverse outcome in the preoperative setting that rely on the cytomorphologic and molecular analysis of the fine-needle aspirate. If this stratification can be achieved, then many patients with PMC will be offered active surveillance and spared unnecessary surgery with its side effects and costs.
Footnotes
Author Disclosure Statement
No competing financial interests exist.