
Abstract


WEDNESDAY, SEPTEMBER 19, 2012
Registration Open 2:00 pm–8:30 pm
7:00 am–5:00 pm
Chairs: Susan Mandel and Robert Levine
(Separate registration required)
James A. Fagin, John C. Morris, Douglas Forrest, and Elizabeth N. Pearce
5:45 pm–7:30 pm
Chairs: Douglas Forrest and Elizabeth Pearce
Clinical Review Kathryn Schuff
Surgical Review Chris Holsinger
Basic Review Antonio Bianco
7:30 pm–9:00 pm
THURSDAY, SEPTEMBER 20, 2012
Registration Open 6:30 am–5:30 pm
Chair: Marilene Wang
Novel Therapeutics in Iodide Resistant Differentiated Thyroid Tumors Steven I. Sherman
Novel Therapeutic and Molecular Targets in Medullary Thyroid Carcinoma Matthew Ringel
Drug Resistance and Other Obstacles to Overcome for Effective Therapeutics for Iodide Resistant Thyroid Cancers Keith Bible
Introduction: Peter Kopp
Speaker: Nancy Carrasco
Chairs: Elizabeth Pearce and Douglas Forrest
Abstracts # 1, 2, 3, and 4
Introduction: Anthony Hollenberg
Speaker: Fredric Wondisford
Chair: Gregory Brent
Mouse Models for Thyroid Hormone Receptor Mutations Sheue-yann Cheng
New Mutations in Human THRA Gene Theo Visser
Update on Human THRB Mutations Samuel Refetoff
(for ATA Active members only)
FRIDAY, SEPTEMBER 21, 2012
Registration Open 6:30 am–5:30 pm
Chair: Naifa Busaidy
Detection, Conservative Management Douglas Ross
Molecular Genetics (Prognostic Role of BRAF) Marina Nikiforova
Surgical Management Taking into Account Molecular Data Martha Zeiger
Speaker and talk announced onsite
Introduction: Frances Carr
Speakers: Anne Cappola, James Fagin, Susan Mandel, and Carole Spencer
Introduction: Matthew Ringel
Speaker: Paul Ladenson
Introduction: Kenneth Burman
Speaker: Robert Smallridge
Chair: Ronald Cohen
Medullary Thyroid Cancer Rozita Bagheri-Yarmand
mtDNA Damage in Hurthle Cell Neoplasms: 3D Models Wen T. Shen
(Admission with ticket only)
SATURDAY, SEPTEMBER 22, 2012
Registration Open 6:30 am–5:30 pm
Chair: Stephen LaFranchi
Increasing Incidence of Congenital Hypothyroidism: Real or Artifact? Kenneth Pass
Increasing Incidence of Mild Cases: Do They Benefit from Early Detection and Treatment? Yves Giguère
Low Birth Weight/Preterm Infants with Delayed TSH Elevation: Natural History Rosalind Brown
Introduction: Graham Williams
Speaker: Krishna Chatterjee
Chairs: Julie Ann Sosa and Charles Emerson
Short Call Abstracts # 1, 2, 3, 4, 5, and 6
Introduction: Michael McDermott
Speaker: Bryan Haugen
Chair: Wilmar Wiersinga
Very Long-Term Treatment with ATD Peter Laurberg
TSH Receptor Monoclonal Antibodies B. Rees Smith
TSH Receptor Low-Molecular-Weight Antagonists Marvin Gershengorn
SUNDAY, SEPTEMBER 23, 2012
Registration Open 8:00 am–11:30 am
ATA Board of Directors Meeting 7:00 am–8:30 am
Introduction: Manisha Shah
Speaker: Robert Smallridge
Introduction: Jeffrey Garber
Speaker: James Hennessey
Moderator: R. Michael Tuttle
Surgeon Sanziana Roman
Pathologist Ronald Ghossein
Clinical Endocrinologists Bryan Haugen and Bryan McIver
Nuclear Medicine Anca Avram
Laboratory Medicine Carole Spencer
Oncology Lori Wirth
Thursday, September 20, 2012
Institute of Metabolic Science, University of Cambridge, Cambridge, United Kingdom
Disorders of Thyroid Function Thursday Oral Clinical 9:00 AM
Congenital central hypothyroidism occurs either as an isolated thyroid-stimulating hormone (TSH) deficiency or in conjunction with other pituitary hormone deficits. Undetected central hypothyroidism is associated with developmental delay in children and adverse cardiometabolic sequelae in adults. Hitherto, mutations in the thyrotropin-releasing hormone receptor (TRHR) or TSHβ subunit (TSHB) genes are the only known causes of isolated TSH deficiency.
Using whole-exome and candidate gene sequencing, we have studied 10 unrelated families with males exhibiting isolated TSH deficiency, testicular enlargement, and variably low serum prolactin levels.
We have identified nine distinct mutations in the X-linked immunoglobulin superfamily member 1 (IGSF1) gene in affected males. IGSF1 encodes a pituitary-enriched plasma membrane glycoprotein; disease-associated mutations block trafficking of IGSF1 from the endoplasmic reticulum to the membrane, consistent with the loss-of-protein function. We have also characterized IGSF1-deficient mice. Adult male IGSF1 null mice show decreased pituitary TSH content and circulating T4 levels, together with increased body weight and fat mass, recapitulating features of the human disorder. Decreased TRHR mRNA levels in pituitaries from null mice, together with reduced TSH bioactivity in patients with IGSF1 mutations, suggest that impaired TRH signaling may be the basis for hypothyroidism.
Collectively, our observations delineate a novel X-linked syndrome in which loss-of-function mutations in IGSF1 cause central hypothyroidism, testicular enlargement, and variable prolactin deficiency, and identify a previously unsuspected role for IGSF1 in hypothalamic–pituitary control of thyroid and testicular function.
Leibniz Institute for Age Research/Fritz Lipmann Institute, Jena, Germany
Thyroid Hormone Metabolism & Regulation Thursday Oral Basic 9:15 AM
Inactivating mutations in the thyroid hormone (TH) transporter MCT8 cause a severe form of psychomotor retardation. In mice, Mct8 deficiency results in an impaired transport of T3, but not of T4 into the brain, and it is not associated with any neurological impairments. We speculated that in mice, TH uptake into the CNS is facilitated by Mct8 and by Oatp1c1, a T4-specific TH transporter localized at the blood–brain barrier.
To define the role of Mct8 and Oatp1c1 in brain TH transport, we generated Mct8/Oatp1c1 double knockout (dko) mice and analyzed them by determining T4 transport, brain TH content, deiodinase activities, and expression levels of TH-regulated gene products in wild type, the respective single and double mutant animals. Immunohistochemical stainings were performed to determine neuronal differentiation and myelination at different postnatal time-points. Animals were also subjected to extensive behavioral studies.
In contrast to Mct8 ko and Oatp1c1 ko mice, Mct8/Oatp1c1 dko mice exhibited a strongly diminished uptake of T4 into the CNS. Hence, brain T4 and T3 content was pronouncedly reduced, while type 2 deiodinase activities were found to be highly elevated. Determination of T3-regulated gene products indicated a severe hypothyroid state of the brain in the absence of both transporters. As a consequence, differentiation of inhibitory neurons in the cerebral cortex, as well as myelination, was strongly impaired. Finally, behavior tests revealed coordination and locomotor deficits in Mct8/Oatp1c1 dko mice.
Our data point to a critical function of Mct8 and Oatp1c1 in the transport of TH into the brain. Since Oatp1c1 is only weakly expressed in the human CNS, Mct8/Oatp1c1 dko mice may be considered as an animal model for human MCT8 deficiency.
Medicine, Mount Sinai School of Medicine, New York, NY
Disorders of Thyroid Function Thursday Oral Basic 9:30 AM
Autoimmune thyroid diseases (AITDs) result from interactions between genetic and environmental factors. Several AITD susceptibility loci have been identified through genome-wide association studies, but the causal variants remain undefined. Recent evidence suggests that epigenetic mechanisms modulate the complex interplay between genes and intra- and extracellular factors to trigger pathological autoimmune responses. Since cytokines are key mediators of tissue inflammation and infiltration, we tested the hypothesis that inflammatory cytokines promote thyroid cell dysfunction through epigenetic modifications of AITD genes. One prime cytokine in the etiology of AITD is interferon-alpha (IFNa), which has also been shown to precipitate AITD when used as therapeutic agent. We have previously shown that IFNa increases mRNA expression of major AITD susceptibility genes in both cell lines and a mouse model of IFNa thyroid expression.
We mapped modifications of histone patterns [histone H3 mono- and trimethylated at Lys-4 (H3K4me1 and H3K4me3)] induced by IFNa at these loci using ChIP-seq in human thyroid cells. ChIP-seq data were integrated with RNA-seq and bioinformatic analyses.
Integration of ChIP-seq and RNA-seq data showed that significantly upregulated pathways included genes characterized by H3K4me3 enrichment in the 5′-regions, demonstrating a correlation between H3K4me3 and pathway activation by IFNa. Most upregulated genes/pathways participate in innate immunity and host defense response. IFNa induced enrichment of H3K4me1 mostly in noncoding gene regions. We next used the potential of H3K4me1 to mark regulatory regions to identify functional AITD-associated single-nucleotide polymorphisms (SNPs). An AITD-associated SNPs, in thyroglobulin (TG) gene was marked by enrichment of H3K4me1. This same SNP was previously shown by us through bioinformatic analyses followed by ChIP, luciferase reporter, and siRNA assays to bind interferon regulatory factor-1 (IRF1) and to modulate TG promoter activity in an allele-dependent manner.
Our results demonstrate that an unbiased genome-wide epigenomic screening can pinpoint the disease-associated variants and identify novel genetic–epigenetic interactions.
Head and Neck Surgery, Memorial Sloan Kettering Cancer Center, New York, NY
Thyroid Cancer Thursday Oral Clinical 9:45 AM
The American Thyroid Association guidelines on the management of well-differentiated thyroid cancer (WDTC) recommend the routine use of RAI in all T3 or greater primary tumors, and selective use in patients with intrathyroidal disease <1 cm, or evidence of nodal metastases. The guidelines recognize that there are conflicting and inadequate data to make firm recommendations for most patients. The aim of this study was to analyze our experience of the selective use of radioactive iodine (RAI) in the management (WDTC).
Retrospective review of 1129 patients who underwent total thyroidectomy in Memorial Sloan Kettering Cancer Center between 1986 and 2005: the median age was 46 years (range 11–91 years) with a man-to-woman ratio of 1:2.8. All patients were managed with total thyroidectomy and had no evidence of macroscopic residual disease after surgery or distant metastases. Four hundred ninety were pT1/T2N0, 193 pT1/T2N1, and 444 were pT3/T4. All patients were assessed using the GAMES risk stratification method. Select patients within each group did not receive RAI. Details on recurrence and disease-specific survival were recorded by the Kaplan–Meier method and compared using the log-rank test.
With a median follow-up of 63 months (range 1–282 months), select patients with early primary disease (pT1/T2) and low-volume metastatic disease in the neck (pT1/T2 N1) who were managed without RAI had excellent outcomes. In the group with advanced local disease (pT3/T4), select patients with pT3N0 disease were safely managed without RAI. The 5-year DSS and RFS in the pT1/T2N0, pT1/T2N1, and pT3/T4 were 100% and 92%, 100% and 92%, and 98% and 87%, respectively.
Our results justify the selective use of RAI following initial surgical treatment using a risk group stratification method. The place of RAI in the management of PTC should not be a blanket treatment for all. Instead clinicians must make the decision on whether to recommend adjuvant RAI on a case-by-case basis using a multidisciplinary team experienced in the management of thyroid cancer.
Descriptive Statistics of Whole Group and Stratification by RAI/No RAI
Thyroid Cancer Thursday Oral Clinical 1:40 PM
The long-term sequelae of RAI for DTC in pediatric and young adult patients are not well defined. Existing data are limited to case series with limited follow-up, which may underestimate the risk of SPM. Epidemiologic analyses of SPM risk have only been performed in the adult population. The objective of this study was to analyze the elevated risk of SPM attributable to RAI, among young patients with DTC.
Analysis of 3,850 pediatric and young adult patients (<25 years old) with DTC, who were followed in the NCI SEER cancer registry (1973–2008), equating to 38,605 person-years at risk (PYR). The excess risk of SPM was calculated relative to a reference population and expressed as standardized incidence ratio (SIR) and excess absolute risk (EAR) per 10,000 PYR. The excess risk was compared in RAI-treated and non-RAI-treated patients.
Thousand five hundred seventy-one patients (40%) received RAI. The percentage of patients treated with RAI increased over time, from 4% in 1973 to 62% in 2008 (p<0.001). Among patients who received RAI, 26 SPMs were observed, and 18.3 were expected. The relative risk of SPM at any site was significantly elevated (SIR 1.42, p=.05), corresponding to 4.4 excess cases per 10,000 PYR. The SPM risk was not elevated in the non-RAI-treated cohort (SIR 1.01, EAR=0). Patients treated with RAI were at a dramatically elevated risk for development of a salivary malignancy (SIR=34.12, p<0.001), corresponding to 1.7 excess cases per 10,000 PYR. The risk of leukemia in RAI-treated patients was elevated (SIR=3.98, p=0.31, EAR=0.9), but did not reach statistical significance. There was no elevated risk of salivary cancer or leukemia in the non-RAI-treated cohort.
Pediatric and young adult patients who receive RAI for DTC experience an elevated risk of SPM, mainly salivary gland cancer. Excess absolute risk estimates indicate that over a decade, ∼1 in 227 RAI-treated patients will develop an SPM, and 1 in 588 RAI-treated patients will develop a salivary cancer, attributable to RAI. Because the expected survival time for young DTC patients is long, it is critical to carefully weigh the benefits of RAI against the small, but real, increase in the SPM risk.

Use of radioactive iodine in patients <25 years old with DTC over time.
Iodine Uptake & Metabolism Thursday Oral Clinical 1:55 PM
The developing fetus is reliant on maternal iodine for thyroid hormone production, which is required for normal neurodevelopment. Perchlorate (ClO4) is a competitive inhibitor of the sodium/iodide symporter (NIS) and is ubiquitous at low levels in the environment. Thiocyanate (SCN), from cigarette smoke and the diet, is a weaker NIS inhibitor. Environmental ClO4 and SCN exposures during pregnancy could potentially decrease thyroidal iodine uptake in the mother and/or her fetus and subsequent thyroid hormone synthesis. The objective of this study was to measure urinary perchlorate and thiocyanate levels in a cohort of pregnant women in Toronto, Canada.
This was a cross-sectional, observational study of 150 pregnant women recruited from four low-risk antenatal outpatient clinics in Toronto, Canada, who provided a spot urine sample for the measurement of perchlorate and thiocyanate.
Women (mean age 33.8±4.4 years) were in their second and third trimesters (mean gestational age 29±7.9 weeks) and primarily Caucasian (73%), well educated (96% more than a high-school education), and relatively affluent (64% with median annual income greater than $100,000). The median urinary perchlorate concentration was 3.2 μg/L (range, 0.5–48.1 μg/L), and the median urinary thiocyanate concentration was 351 μg/L (range, 28–1195 μg/L). These pregnant women were iodine sufficient (median urinary iodine concentration 227.1 μg/L), as was previously presented at the 2011 American Thyroid Association meeting.
This is the first report describing population urinary perchlorate and thiocyanate concentrations in Canada. The low levels of both environmental substances are comparable to those previously reported by us in iodine-deficient and sufficient pregnant women from Wales, Italy, Argentina, and the United States without an effect on maternal thyroid function. These results suggest that the low urinary perchlorate concentrations in Canada would unlikely alter the thyroid function of pregnant women or their fetuses, especially in iodine-sufficient regions.
University of Pennsylvania School of Medicine, Philadelphia, PA
Disorders of Thyroid Function Thursday Oral Clinical 2:10 PM
Subclinical hyperthyroidism affects 1–2% of individuals aged 65 and older, yet the degree to which it persists over time and its associated health risks in this population are unclear. We examined transitions in the thyroid status over a 2–3-year period and the risks of cardiovascular and total mortality in older individuals with subclinical hyperthyroidism.
In 5,009 US-community-dwelling men and women aged 65 and over who were enrolled in the Cardiovascular Health Study and not taking thyroid medications, serum TSH and free-T4 concentrations were measured in banked specimens at 1989–90, 1992–93, and 1996–97 visits. We identified 70 subjects with subclinical hyperthyroidism (TSH<0.45 mU/L with a normal free-T4 level) at their first TSH measurement and examined persistence, resolution, and progression of subclinical hyperthyroidism over 2–3 years. Cox proportional hazards models were used to determine the relationship between subclinical hyperthyroidism and cardiovascular and total mortality over ten years of follow-up, using 4194 euthyroid individuals (TSH 0.45–4.5 mU/L) as a reference group. All models were adjusted for age, sex, race, and initiation of thyroid medications.
Of the 70 individuals with subclinical hyperthyroidism, 60% were women, 24% were nonwhite, and mean age was 73.7 years. Among those with subclinical hyperthyroidism who obtained follow-up thyroid testing or were taking thyroid medication at follow-up (n=44), 43% persisted; 41% became euthyroid; 5% progressed to overt hyperthyroidism; and 11% initiated thyroid medication. There was no association between initial TSH and total or cardiovascular mortality (see Table).
Comparison of Initial TSH and Mortality
Subclinical hyperthyroidism persists in nearly half of older individuals, with high rates of reversion to euthyroidism. Although numbers were small, subclinical hyperthyroidism was not associated with overall or cardiovascular mortality.
Thyroid Cancer Thursday Oral Clinical 2:25 PM
UPEA of selected NNM in patients with PTC was first reported in 2002 (AJR 178:699). In 1993, we ablated a 35-year-old woman with PTC, who had been treated with two neck surgeries, 135 mCi of 131I, and 5400 cGy of external irradiation. She had an inoperable 32-mm mass adjacent to her internal carotid artery, and was ablated with 1.4 cc of 95% ethanol, delivered in 3 sessions over 10 months under ultrasound guidance. In 2011, her avascular node measured 7 mm on sonography and was associated with an undetectable serum thyroglobulin of <0.1 ng/mL. During the past 20 years, we have treated with UPEA another 148 PTC patients (114 localized to neck and 34 distantly spread), selected from one endocrinologist's practice.
In this report, we describe details of the 88 patients (61 women, 27 men), who presented with pTNM stage I disease and had their NNM ablated during 1993–2012. At UPEA, the mean patient age was 37 years (range 18–64). In total, 131 recurrent nodes (largest mean diameter 11 mm; range 4–32) were initially injected with a mean of 0.8 cc (range 0.1–2.1) of 95% ethanol. Three patients were not reassessed; five recently ablated in 2012. The 80 patients, who had post-UPEA reassessment, were followed for a median of 5 years (range 0.3–19).
At latest follow-up, all ablated NNM in 80 evaluated stage I patients were shrunken and had no Doppler flow; 57/119 (49%) NNM could no longer be identified on sonography. In 74 autoantibody-negative patients, latest median serum thyroglobulin was 0.3 ng/mL; 31% had thyroglobulin levels <0.1 ng/mL. No patient after UPEA developed permanent hoarseness. Nineteen out of 79 (24%) had successful treatment of further new NNM: 15 (79%) with UPEA alone and 4 with repeat neck surgery.
UPEA of NNM in stage I PTC patients is highly effective, harmless, and considerably cheaper than reoperation. In this series, UPEA prevented 80 reassessed stage I PTC patients from undergoing 95 potentially hazardous neck re-explorations. The resultant cost savings (JCEM 96:2718, 2011) for treating these 80 patients alone are estimated to be in excess of 3.65 million dollars. It is surely long overdue for other centers of excellence to introduce UPEA of NNM in PTC patients to their therapeutic repertoires.
Endocrine Oncology Unit, Gustave Roussy Institute, Villejuif, France
Thyroid Cancer Thursday Oral Clinical 2:40 PM
Bone metastases (BM) are frequent in patients with differentiated thyroid cancer and may impair the quality of life. We aimed to study the frequency of bone progression in patients treated with tyrosine kinase inhibitors (TKI) because of progressive soft tissue disease of radioactive iodine refractory-differentiated thyroid cancer.
In this monocentric retrospective study, we reviewed patients with BM treated with TKI, from 2007 to 2012. BM were monitored by clinical exam, CT, or TEP-CT imaging every 3 months. Bone progression was defined by the occurrence of a skeletal event and/or the appearance of a new bone lesions and/or progression of known measurable bone lesions.
Thirty patients (19 men, mean age 57 years, 11 with papillary, 9 with follicular, and 10 with poorly differentiated thyroid cancer) were treated with vandetanib (n=12), sorafenib (n=19), sunitinib (n=8), or motesanib (n=2), with 4 patients receiving two successive TKIs and 3 patients receiving 3 successive TKIs. Response to TKI treatment at 3 months according to RECIST 1.0 was a partial response in 4 (10%) cases, stable disease in 24 (59%) cases, and progressive disease in 13 (31%) cases. Among the 28 nonprogressive patients under treatment, 19 (68%) had stable bone disease, and 9 (32%) had bone progression, including 2 with new bone lesions, 1 with a skeletal-related event, and 6 with progression of known bone lesions. Among the 13 patients with progressive disease during treatment, 7 (53%) had stable bone disease, and 6 (47%) had bone progression, including 2 with a skeletal-related event and 6 with progression of known bone lesions.
Evaluation of bone metastases of patients under TKI is essential, because 32% of the patients with nonprogressive soft tissue lesions can disclose bone progression during treatment.
BRAF MUTATIONAL ANALYSIS IDENTIFIES NO ADDITIONAL CARCINOMAS FOLLOWING AFIRMA GENE EXPRESSION CLASSIFIER TESTING OF INDETERMINATE THYROID FINE-NEEDLE ASPIRATES (FNAs )
Thyroid Nodules & Goiter Thursday Oral Clinical 2:55 PM
The Afirma® gene expression classifier (GEC) measures the RNA expression of 142 genes and has been shown in a large prospective validation study to classify indeterminate thyroid FNAs as either benign or suspicious with high sensitivity. Conversely, BRAF DNA mutational testing identifies thyroid malignancies with high specificity. We hypothesized that adding a diagnostic test with high specificity to one with high sensitivity might increase clinical utility.
We used the Competitive Allele-Specific TaqMan PCR method to measure the BRAF V600E mutational status in DNA from 208 frozen (−80° C) FNAs with indeterminate cytology: n=95 atypia/follicular lesion of undetermined significance (AUS/FLUS); n=70 follicular neoplasm/suspicious for follicular cell neoplasm (FN/SFN); and n=43 suspicious for malignancy (SM). The malignancy status was determined through blinded gold standard surgical pathology diagnosis.
Twenty-one cytologically indeterminate samples (10.1%) were BRAF+, the vast majority occurring in the SM category. Still, of 31 malignancies in this category, only 17 (55%) were BRAF+. Only 2 mutations were found in the AUS/FLUS category (2.1%), and only 1 (1.4%) was positive in the FN/SFN category. While the intended use of the GEC is for indeterminate cytology nodules, we explored BRAF testing in the benign (B) and malignant (M) cytology categories. Of 40 cytology B samples, 2 (5.0%) were BRAF+. Both samples were also GEC suspicious. Of 48 cytology M samples, 36 (75%) were BRAF+. No BRAF mutations were found in GEC benign samples, and all BRAF+ samples were GEC suspicious. Thus, the addition of BRAF testing to GEC testing did not increase the detection of malignant nodules. BRAF testing without the GEC missed 55/75 malignancies in this data set, rendering the test inadequate to rule out malignancy preoperatively (sensitivity 27%, specificity 99%, PPV 95%, and NPV 71%).
BRAF mutational testing in AUS/FLUS and FN/SFN cytology categories provides minimal clinical utility due to its very low frequency in these subtypes. While BRAF+ detection supports the decision of therapeutic total thyroidectomy, absence of a BRAF mutation may not change this decision in cytologically SM nodules, where the risk of malignancy remains high.
Division of Endocrinology, Diabetes and Metabolism, University of Miami, Miller School of Medicine, Miami, FL
Thyroid Hormone Metabolism & Regulation Thursday Oral Basic 1:40 PM
The type 2 deiodinase (D2) catalyzes the conversion of T4 to T3 and thus plays a role in the T4-mediated TSH feedback mechanism. However, the role played by D2 in the different anatomical sites within the central nervous system has not been defined.
Here we used p-flox technology to develop two new mouse strains, the first lacking D2 activity in pituitary thyrotrophs (Pit-D2KO) and the second lacking D2 activity in astrocytes (Astro-D2KO).
Neither mouse strain exhibited gross phenotypic abnormalities, with development and reproductive function largely preserved. In both new strains, the analysis of body weight, brain, epididymal fat, liver, and muscle weight, showed no difference when compared to the respective Cre-expressing controls. The Pit-D2KO mouse exhibited normal serum T3 and was systemically euthyroid, but had an elevated serum T4 due to a disruption in the T4-mediated TSH feedback mechanism. The elevated serum T4 decreased paraventricular TRH mRNA, defining a critical role for hypothalamic D2 in the T4-mediated TRH feedback mechanism. Furthermore, these animals also exhibited lower pituitary TSHa mRNA levels, whereas TSHb mRNA remained unaffected. The reduction in TRH expression and its implication for TSH glycosylation (prolonged half-life and decreased biological activity) explain why Pit-D2KO mice had an elevated serum TSH that only minimally affected the thyroid gland. That this critical role played by hypothalamic D2 resides in the tanycytes is defined by the analysis of the Astro-D2KO mouse, in which there was almost complete D2 inactivation in the brain, except for the hypothalamic tanycytes that preserve thyroid economy.
These data indicate the existence of close coordination between T4-to-T3 conversion in thyrotrophs and tanycytes. The disruption of the D2-mediated T4 signaling in the pituitary is compensated for by an increase in D2-mediated T4 signaling in the hypothalamus, which preserves thyroidal activity and T3 serum levels.
Department of Molecular Virology, Immunology, and Medical Genetics, The Ohio State University, Columbus, OH
Thyroid Cancer Thursday Oral Basic 1:55 PM
While both follicular and papillary thyroid cancer (FTC and PTC, respectively) generally respond well to treatment, it is known that FTC has a greater risk of progression, including distant metastases, and these patients have few treatment options. Thus, it remains of utmost importance to identify molecular changes that lead to aggressive and metastatic FTC in hopes of identifying novel drug targets for therapy. Our lab has demonstrated that thyroid-specific ablation of the Carney Complex gene, PRKAR1A, leads to hyperthyroidism and FTC in mice (R1a-TpoKO mice). However, while these animals develop FTC, none developed distant metastases.
To better study the molecular basis for aggressive FTC formation, we crossed the R1a-TpoKO mice with animals carrying a conditional null allele of the Cowden Syndrome gene Pten, which has been shown to promote tumorigenesis in many tissues, including the thyroid.
These
These mice represent an important and reliable new tool for the study of molecular mechanisms that drive the formation of distant metastases in FTC and may lead directly to the development and testing of novel FTC therapies.
A GENOMIC ANALYSIS OF THYROID HORMONE REGULATION OF HEPATIC METABOLIC FUNCTIONS
Thyroid Hormone Metabolism & Regulation Thursday Oral Basic 2:10 PM
Thyroid hormone regulates various metabolic functions through the modulation of gene transcription by activation of its receptor in liver (primarily THRB). The specific regulation of lipid metabolism has been targeted in the development of selective thyromimetic drugs, which exhibit beneficial effects on serum lipid parameters in various preclinical models, although concern over side effects has precluded their clinical use. Previous studies using drugs targeting constitutive androstane receptor (CAR), an evolutionarily related nuclear receptor that is also expressed in the liver and binds to similar DR4 DNA elements, have indicated that its activation also exerts similar beneficial effects on serum lipid parameters.
Our studies have focused on clarifying the mechanisms of thyroid hormone hepatic lipid metabolic regulation through comparative analysis of gene regulation by thyromimetics and CAR activators. We have performed complementary analyses of THRB and CAR regulation in an in vitro cell culture model by expression array and genome-wide binding analysis (ChIP-Seq) and in analysis of metabolic parameters in animal models.
Our results have suggested overlapping patterns of metabolic pathways regulation, mediated by commonly regulated target genes, as well as distinct, receptor-specific targets. These observations have suggested that THRB induces a key set of metabolic genes, including mediators of hepatic lipid uptake, nutrient homeostasis, and bile acid metabolism, consistent with observed patterns of metabolic regulation in animal models.
These results suggest a complex model of overlapping, yet distinct gene regulation by hepatically expressed nuclear receptors resulting in similar, but distinct physiological outcomes. These studies have defined key steps in the hepatic metabolic regulation of thyroid hormone, adding to our understanding of its mechanisms, as well as related thyromimetics.
College of Pharmacy, Univ Minnesota, Duluth, MN
Disorders of Thyroid Function Thursday Oral Basic 2:25 PM
Iron (Fe) and iodine/thyroid hormone (TH) deficiencies during development lead to similar molecular, cellular, and behavioral abnormalities that persist into adulthood, and often coexist in individuals living in developing countries. We recently demonstrated that fetal/neonatal Fe deficiency results in a mild perturbation of the thyroid axis, suggesting that TH insufficiency contributes to the neurodevelopmental abnormalities associated with Fe deficiency. We hypothesized that combining Fe deficiency with an additional mild thyroidal perturbation during development would result in a more severe insult to the neonatal thyroid axis and to TH-responsive gene expression in the neonatal brain.
To test this hypothesis, pregnant Sprague-Dawley rats were assigned to one of seven different treatment groups early in gestation: control, Fe-deficient (FeD), mild TH-deficient (1 ppm PTU), moderate TH-deficient (3-ppm PTU), severe TH-deficient (10-ppm PTU), FeD/1-ppm PTU, or FeD/3-ppm PTU. At postnatal day 15 or 16 (P15 or P16), thyroidal status and brain TH-responsive gene expression were assessed.
Iron deficiency or 1-ppm PTU treatment alone had mild effects on neonatal thyroidal status, reducing serum total T4 concentrations by 64% and 74%, respectively, without significantly altering serum total T3 concentrations. Neither treatment alone significantly altered cortical or hippocampal T3 concentrations. Interestingly, however, FeD combined with 1-ppm PTU treatment produced a more severe effect on neonatal thyroidal status reducing serum total T4 by 95%, and lowering hippocampal and cerebral cortical T3 concentrations by 24% and 31%, respectively, compared to controls. Combined FeD/1-ppm PTU also resulted in a more severe effect on brain TH-responsive gene expression than either treatment alone, significantly altering the hippocampal and cortical mRNA levels for Parvalbumin, Type 2 deiodinase, and Hairless.
These data suggest that combining mild thyroidal insults during pregnancy and early-neonatal life results in significant perturbation of the thyroid axis and impairment of TH-regulated brain gene expression.
Division of Endocrinology, Department of Medicine, Mount Sinai Medical Center, New York, NY
Autoimmunity Thursday Oral Translational 2:40 PM
Autoimmune thyroid disease (AITD) has become increasingly recognized as a complication of interferon-alpha (IFNα) therapy in patients with chronic hepatitis C virus (HCV). Interferon-induced thyroiditis (IIT) can manifest as clinical thyroiditis in ∼15% of HCV patients receiving IFNα and subclinical thyroiditis (i.e., thyroid antibody positive) in up to 40% of patients, possibly resulting in discontinuation of IFNα. Data regarding susceptibility genes in IIT are sparse and inconclusive. We aimed to identify genetic markers that can potentially recognize patients at risk of IIT before initiating IFNα treatment and thereby prevent the complications associated with thyroid disease.
To identify susceptibility genes in IIT, we used the customized infinium immunochip covering 9021 genes to genotype a cohort of 245 patients with chronic HCV infection and compared their genotypes to those of a set of 851 healthy Caucasian controls. Due to an ethnically mixed patient population, we performed principal component analysis to ensure appropriately matched controls and to avoid population stratification. Association analyses were performed on 2 groups: 1) all IIT patients compared to chronic hepatitis C patients who did not develop thyroiditis and 2) Caucasian IIT patients compared to healthy Caucasian controls.
Of the 245 patients included in our analyses, we confirmed presence of IIT in 53 individuals and absence of disease in 192 individuals after at least 12 weeks of IFNα therapy. Based on p-value<0.005 and on gene function, we selected up to 25 candidate genes distinguishing IIT cases from both chronic HCV and healthy Caucasian controls. Strong genetic association with IIT was found with significant overlap noted between the 2 groups analyzed (see Table), and several genes known to be associated with AITD, including HLA, TSHR, and CTLA-4, were also identified.
List of Candidate Genes Shown to be Associated with Thyroiditis in Hepatitis C Virus Patients that Received Interferon Compared to HCV Patients that Did Not Develop Thyroiditis Following IFNα1 and Compared to Healthy Caucasian Controls
Immunochip analyses identified candidate genes predisposing to IIT with evidence for shared susceptibility with thyroid autoimmunity. These represent markers that may identify individuals at risk of thyroiditis induced by IFNα therapy.
Thyroid Cancer Thursday Oral Translational 2:55 PM
Due to the limitations of fine-needle aspiration biopsy (FNAB) cytology, a large proportion of individuals who present with nodular thyroid disease eventually undergo thyroidectomy as a diagnostic procedure for cancer. The objective of this study was to determine whether whole-transcriptome profiling could be utilized to identify novel biomarkers that allow for accurate thyroid cancer diagnosis.
Nucleic acids were extracted and amplified for microarray expression analysis on the Human Exon 1.0 ST GeneChips from a total of 60 thyroid tumors (30 cancers and 30 benign lesions) obtained from formalin-fixed paraffin-embedded 1-mm-diameter tissue cores. A training cohort of 40 patients was evaluated utilizing the histopathological diagnosis to select for differential expression based on t-tests and fold-difference metrics for significance, and subsequently validated in a blinded fashion on a testing cohort of 20 patients.
Ninety percent of the greater than 5,000 differentially expressed features that were identified in the training cohort have not been previously reported for thyroid lesions. A subset of 10 RNA transcripts was combined into an expression signature to discriminate malignant from benign disease and validate predictive power in the testing cohort. The 10 RNA transcript expression signature correctly identified 9/10 benign lesions (misclassifying a single-follicular adenoma as a cancer) and 9/10 malignant lesions (misclassifying a single-papillary carcinoma as benign disease). For the entire cohort of thyroid tumors that had an indeterminate preoperative FNAB, the agreement between the expression signature and histopathological diagnosis was 90% (27/30).
Whole-transcriptome profiling of thyroid nodules identified many novel differentially expressed transcripts, and a subset of 10 expressed transcripts was able to readily distinguish benign and malignant tumors in the majority of cases, including those with a preoperative indeterminate FNAB diagnosis.
Orals 17–28 can be found under “Friday, September 21, 2012,” starting on Page 45.
Orals 29–36 can be found under “Saturday, September 22, 2012,” starting on Page 81.
THE TSH RECEPTOR HINGE REGION AS A SURROGATE LIGAND: IDENTIFICATION OF LOCI CONTRIBUTING TO THE COUPLING OF TSH BINDING TO RECEPTOR ACTIVATION
Autoimmunity Thursday Poster Basic
The TSH receptor (TSHR) plays a vital role in metabolic homeostasis as well as in disease pathophysiology. The hinge region of the receptor, the least well-understood component, bridges the leucine-rich repeat and transmembrane domains. We report data on clusters of charged residues in the hinge region whose mutation to Ala is compatible with cell surface expression and normal or near normal TSH binding affinity yet with a relative reduction in receptor activation. This phenomenon represents partial uncoupling between ligand binding and signal transduction.
Mutated TSHRs were stably transfected into CHO cells. TSHR activation by bovine TSH was assessed by measuring the cAMP response in cultured cells. TSH binding affinities were determined using 125I-TSH and nonlinear regression analysis.
Mutation to Ala of E409 at the junction between the hinge region and transmembrane domain was the most potent in uncoupling TSH binding and signal transduction (∼22-fold less sensitive than the wild-type TSHR) and was unique among the residues studied in reducing both the amplitude and the sensitivity of the ligand-induced signal. Unexpectedly, a dual E409A/D410A mutation partially corrected the major suppressive effect of TSHR-E409A. The combined Ala substitution of a cluster of positively charged hinge residues (K287, K290, K291, and R293; termed K3R1) synergistically reduced sensitivity to TSH stimulation ∼21-fold without altering the TSH binding affinity. Simultaneous Ala substitutions of a cluster of acidic hinge residues D392, E394, and D395 (termed DE392-5A) partially uncoupled TSH binding from signal transduction (4.4-fold reduction in sensitivity), less than for E409A and K3R1A. Remarkably, the combination of the K3R1A and DE392-5A mutations was not additive, but ameliorated the major uncoupling effect of K3R1A. This lack of additivity suggests that these two clusters contribute to a common signaling pathway.
The present data identify several TSHR hinge residues involved in coupling ligand binding to signal transmission. These data support the concept that the hinge regions of the TSHR (and other glycoprotein hormone receptors) act as surrogate ligands for receptor activation.
Department of Endocrinology Diabetes and Metabolism, Temple University School of Medicine, Philadelphia, PA
Autoimmunity Thursday Poster Basic
Several studies have reported that women with autoimmune thyroid disease (AITD) are at increased risk of birth defects in the offspring. We present a case of tetrasomy-13 offspring born to a mother with undiagnosed, symptomatic hyperthyroidism during pregnancy.
A 20-year-old African American woman with no medical history presented to our hospital 5 months postpartum with florid symptoms of thyrotoxicosis with an increase in the neck size with pain, compressive symptoms, palpitations, diaphoresis, fatigue, heat intolerance, dry itchy eyes, and diplopia for almost 1 year. On exam, she was anxious looking with proptosis, lid lag, tremors, tachycardia, and diffusely enlarged thyroid gland with a bruit. Biochemical workup revealed a suppressed TSH-0.01 mIU/mL with an elevated FT4-5.4 ng/dL and FT3-2840 pg/dL with positive TPO antibody >1000 IU/mL. She was treated with antithyroid medications, beta-blockers, and lugols iodine for a clinical diagnosis of Graves' disease. Her history dates back to the time when she was pregnant and noticed to have increase in the neck size and bulging eyes. However, due to poor antenatal follow-up and manageable symptoms, she was never seen for her thyroid problem. At 34 weeks of gestation, she delivered a malformed baby with multiple midline hemangiomas, dysmorphic facial features, and failure to thrive. Genetic testing revealed terminal triplication of the long arm of chromosome 13, tetrasomy13q32.2qter. Despite several attempts for resuscitation, the baby expired within 3 months.
We believe that the birth defect in the baby of this young woman was associated with her uncontrolled Graves' disease during pregnancy. Autoimmune thyroid disease is a rare cause of congenital fetal anomalies, especially trisomy, and there have been only few studies and one case report. However, a causal association has not been established.
Currently, there is no consensus on universal screening for thyroid disease in pregnancy. Given the increased risk of adverse fetal and maternal outcomes, we encourage that every woman should be screened for thyroid disease in the perinatal period.
Medicine, Kuma Hospital, Kobe, Japan; 2Pharmacovigilance, Chugai Pharmaceutical Co., Ltd., Tokyo, Japan
Autoimmunity Thursday Poster Clinical
Agranulocytosis (AGR) is rare, but one of the most serious, complications caused by antithyroid drugs (ATD). It is considered that AGR often occurs suddenly, and routine examinations of white cell counts may not prevent its occurrence. In Japan, death was reported of a patient with Graves' disease who was administered ATD approximately once a year.
Under the Medical Practitioners Law, doctors in Japan should report adverse drug reactions to pharmaceutical companies that should collect from the medical institutions' detailed information, including age, sex, time to onset of adverse reaction, dose at time of onset, adverse reaction type and severity, examination data, treatment details, and outcome. We analyzed the reported cases of AGR.
As of April 2011, the pharmaceutical company has collected information from a total of 733 cases of Graves' disease in patients treated with ATD since 1981. Among them, 215 patients had white cell count measurements within 90 days before the onset of AGR. The duration between the last examination and the onset was continuous between one and 82 days. Surprisingly, normal granulocyte counts were confirmed in 64 patients (30%) within one week before onset and in 131 patients (61%) two weeks before onset. This shows that AGR develops rapidly. Thirty patients died, including two old cases from our hospital. Excluding six cases with insufficient information reported, we analyzed 24 patients. Based on physician reports in 14 cases, there might be some room for improvement of therapeutic procedures, for example, giving patients more sufficient ATD safety information, careful differential diagnosis of AGR from common cold, and stopping ATD immediately when AGR is suspected. On the contrary, it might have been very difficult to save the lives of 10 patients, because the granulocyte counts just a few days before were normal, or because the condition of the patient was deteriorating very rapidly without responding to promptly administered intensive care.
This study provides the first direct evidence that AGR develops rapidly. Giving sufficient information on AGR to every patient is very important when ATD is prescribed.
Endocrinology & Metabolism, M S Ramaiah Medical College, Bangalore, India
Autoimmunity Thursday Poster Clinical
The optimal method for determining 131I treatment doses for Graves' disease (GD) is controversial. Fixed dosing and calculations based upon gland size, iodine uptake, and iodine turnover are used. The objective of this retrospective analysis was to compare the 1-year outcomes of 2 fixed doses of 131I radioiodine therapy (5 vs. 10 mCi) in newly diagnosed female patients with GD.
The clinical outcome of 227 female patients with GD treated with 131I at initial diagnosis from 1998 to 2006 was evaluated. Seventy-seven patients received 5 mCi of 131I, and 150 patients received 10 mci. All the patients in the study group were followed-up for at least 12 months after 131I treatment. Independent samples Student's t-test and Chi-squared tests were used to compare baseline parameters and assess the difference in outcomes between the two groups at 1 year. The predictors of remission were determined by logistic regression.
The mean age of the sample was 38±10.8 yrs. Baseline total T4 was higher in the 10-mCi group than the 5-mCi group (p<0.01%). In other aspects, both groups were comparable. The overall success rate of single dose of radioiodine was 92.5% (90.9% 5-mCi group, 93.2% 10-mCi group). One year after ablation, 81.8% of patients in the 5-mCi group were hypothyroid; 9.1% were euthyroid; and 9.1% had relapsed. The corresponding rates for the 10-mCi group were 78.6%, 14.6%, and 6.8%. The outcomes were not different between the two groups by Chi-squared tests. Age, weight, height, baseline T4, and TPO positivity were not predictors of successful treatment in logistic regression. Worsening of ophthalmopathy was seen in one patient in the 5-mCi group and in 3 patients in the 10-mCi group.
Ten mCi of radioiodine was no more effective than 5 mCi in female patients with GD. We recommend that a routine use of 10 mCi in a fixed-dose approach is not warranted in GD.
Comparison of Outcomes Between the 5-m Ci and 10-m Ci Groups at 1 year After 131I Therapy
#Chi-square test (p<0.05 significant).
Autoimmunity Thursday Poster Clinical
In general, autoimmune thyroid disease was much more seen in women compared to men.
In this study, we evaluated the prevalence of thyroid dysfunction and antithyroid antibodies among serial 90 anti-HCV-positive patients (44 men and 46 women) from Jan 2011 until May 2011 who visited the Department of Hepatology, Fukuoka Tokushukai Medical Center. Among them, 28 patients had already treated interferon (IFN) therapy 6 months before the study, and 19 of the above 28 patients were in a sustained virological response (SVR). IFN-untreated HCV patients had more elevated AST, ALT, and γ-GTP than IFN-treated patients.
Overt hyperthyroidism was not seen in this series of 90 patients. Subclinical hyperthyroidism was found in 2 patients of IFN-treated HCV patients (7.1%), but not in IFN-untreated HCV patients (p<0.05). Subclinical hypothyroidism was seen in 12 of IFN-untreated HCV patients (19.4%) and 2 of IFN-treated HCV patients (7.1%). Overt hypothyroidism was 2 of IFN-untreated HCV patients (3.2%) and 2 of IFN-treated HCV patients (7.1%). On the other hand, antithyroglobulin antibody was positive in 3 of IFN-treated HCV patients (10.7%), but not in IFN-untreated HCV patients (p<0.001). However, antithyroid peroxidase antibody was positive in 9 of IFN-untreated HCV patients (14.5%) and in 5 of IFN-treated HCV patients (17.9%). Thus, IFN affected thyroid function and altered thyroid autoimmunity as previously reported. Interestingly, the prevalence of thyroid dysfunction and antithyroid antibodies was not different between men and women of HCV-positive patients who treated with or without IFN therapy.
IFN affects both thyroid function and thyroid autoimmunity, and furthermore, even in men, thyroid dysfunction and thyroid autoimmunity were seen in HCV patients.
Department of Medicine, Section of Endocrinology, Tulane University School of Medicine, New Orleans, LA
Autoimmunity Thursday Poster Clinical
We describe a case of hyperthyroidism secondary to Graves' disease in a patient with end-stage renal disease (ESRD) on hemodialysis (HD), highlighting the complexities of treatment with radioactive iodine (RAI).
A 34-year-old woman with a medical history of ESRD on HD was referred to an endocrine clinic for evaluation and treatment of recently diagnosed hyperthyroidism. She reported a 50-lbs. weight loss in one month, palpitations, and increase in the neck size. Physical examination revealed a heart rate of 114 bpm, hand tremors, and thyromegaly without any audible bruit. Thyroid function tests were consistent with severe hyperthyroidism. Thyroid-stimulating immunoglobulin levels were elevated. Thyroid ultrasound showed diffusely increased size and vascularity of the gland. RAI uptake and scan was performed 24 hours after HD: uptake of 73.9% (4–16) at 4 hours. She was pretreated with methimazole and propranolol for 10 weeks. After detailed communications between endocrinology, nephrology, and nuclear medicine, she was given 12 millicuries of 131I, 24 hrs after and before HD.
131I is mainly cleared by the kidneys in patients with normal renal function; hence, many issues arise in patients who are on HD, including modification of dose and optimal timing of HD after 131I therapy to maximize treatment benefit while minimizing risk to the patient and dialysis personnel. Fewer than 15 similar cases have been reported in the literature so far. Although the dose of 131I need not be adjusted for HD patients, first dialysis after RAI therapy must be delayed until maximum uptake has occurred in the thyroid, which is approximately 10 hours for patients with normal renal function as well as on HD. Radiation monitoring and precautions should be continued for several weeks after treatment as the thyroid continues to process and secrete 131I for several weeks.
131I may be used as definitive treatment of hyperthyroidism in patients with ESRD on HD. However, the optimal dose and timing of HD post-treatment require careful consideration and interdisciplinary communications to minimize risks to patients and medical personnel.
Ciencias Biológicas, Universidad Nacional Andrés Bello, Santiago, Chile
Disorders of Thyroid Function Thursday Poster Basic
Maternal thyroid hormones (MTH) during gestation play an essential role for the appropriate development of the fetus central nervous system (CNS). Among other things, MTH are involved in neuronal development, such as neurite outgrowth, neuronal migration, synapse formation, neuroglial cell development, number of oligodendrocytes, and its myelination. Even though there are few reports in the literature that suggest that MTH are important for the offspring immune system, we show in this work that mice that were gestated in a hypothyroidism condition suffer a strong autoimmune disease at the CNS. Multiple sclerosis (MS) is a chronic autoimmune disease at the CNS characterized by autoimmune reaction, inflammation, demyelination, and axonal damage. Patients that suffer MS have muscle weakness, cognitive impairment, and physical disability among other symptoms.
Mice gestated in mothers with MTH were induced with experimental autoimmune encephalomyelitis (EAE) as a murine model for MS. After 21 days of induction, spinal cord slices were analyzed for demyelination, immune cell infiltration, and oligodendrocyte cells death. To analyze the effects of MTH during pregnancy on oligodendrocyte viability after tumor necrosis factor α (TNFα), primary oligodendrocyte cultures were performed from rats gestated in MTH.
We have shown that the offspring gestated in a hypothyroidism condition suffer a strong EAE than mice gestated in an euthyroid condition. The offspring gestated in a hypothyroid condition showed a higher EAE score, demyelination, immune cell infiltration, and oligodendrocyte cell death than mice gestated in the euthyroid condition. In vitro studies using primary oligodendrocyte cell culture obtained from the offspring gestated in hypothyroid condition showed increase cell death in the presence of TNFα.
These results suggest for the first time that hypothyroidism during gestation can impair the outcome of an inflammatory CNS disease, such as EAE in the offspring. These data strongly support the need for thyroid hormone diagnosis for pregnant women and the treatment of hypothyroidism during pregnancy. Funding: Fondecyt 1100926, Proyecto Interno UNAB DI-11-11/R Millennium Institute on Immunology and Immunotherapy (MIII) P09-016-F.
LATE-GESTATION UNDER-NUTRITION AND EARLY-POSTNATAL-LIFE OVER-NUTRITION HAVE LONG-TERM IMPLICATIONS FOR THYROID HORMONE AXIS FUNCTION IN SHEEP
Disorders of Thyroid Function Thursday Poster Translational
Fetal programming appears to be a risk factor for development of obesity and metabolic diseases later in life, such as insulin resistance and cardiovascular disease (see Figure). Reversal of the epidemic development of these diseases is globally a major public health concern. Mounting evidence led us to hypothesize that 1) the thyroid hormone (TH) axis can be permanently programmed by late-gestation under-nutrition (LG-UN) and contribute to predispose for adverse health outcomes later in life; 2) early-postnatal-life over-nutrition (EL-ON) exacerbates consequences of fetal programming on the TH-axis function.
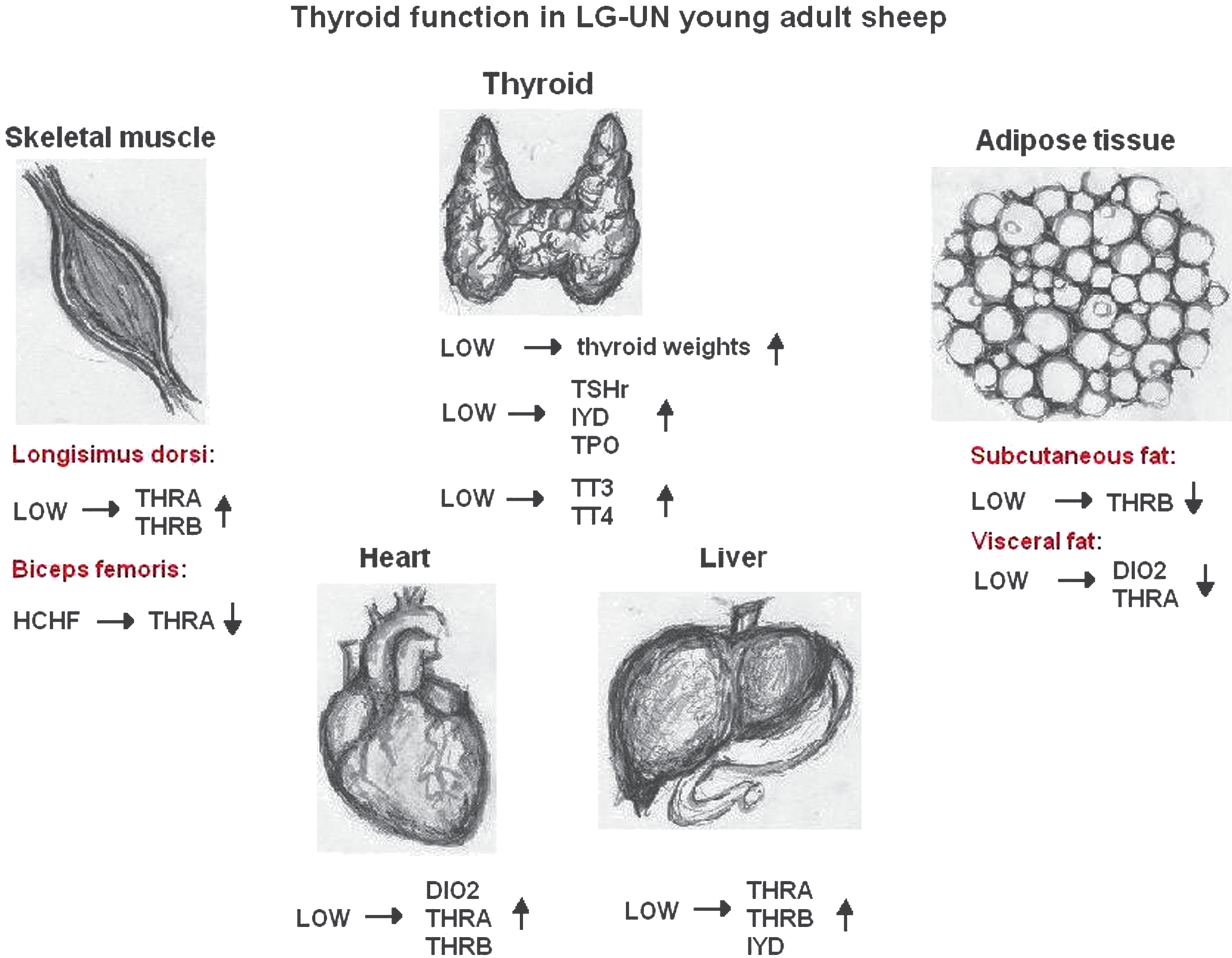
Systemic overview of significant alterations (significantly up- or downregulated, compared to controls) mediated by the different treatments on thyroid function in young adult sheep. NORM and LOW refer to the plane of nutrition offered to twin-pregnant ewes during late gestation, and CONV and HCHF refer to the postnatal diet fed to either of the twin-lambs from day 3 to 6 months of age, thus giving rise to 4 treatment groups: NORM-CONV, NORM-HCHF, LOW-CONV, and LOW-HCHF. We previously reported that exposure to the prenatal LOW compared to NORM diet close to significantly increased weight (as a proportion of the total body weight) of thyroids in both young growing and adult animals (p=0.055). This dietary consequence has therefore been included in the figure. Illustrations by Ms. Rikke Lenitha Larsen.
In a 2×2 factorial experiment, 21 twin-bearing sheep were fed one of two diets during late gestation: NORM (fulfilling energy and protein requirements) or LOW (50% of NORM). From postnatal day 3 to 6 months, twin lambs were assigned to each their diet: a conventional or high-carbohydrate–high-fat diet, where after half the lambs were slaughtered. Remaining sheep (exclusively females) were raised on the same moderate diet until 2 years of age. At 6 months and 2 years of age, fasting challenges were conducted, and target tissues were collected at autopsy.
LG-UN was associated with adult hyperthyroidism (increased serum TH in fed and fasted state), increased TH receptor expression (THRA or THRB or both) in liver, cardiac, and longisimus dorsi muscles, and decreased receptor expression in visceral and subcutaneous adipose tissues. EL-ON increased TH levels in adolescent lambs, but this was reversible upon diet correction.
Upregulation of THRA and THRB in major target tissues concomitant with upregulated or unaltered expression of DIO2 implies that the hyperthyroid state is not induced by peripheral TH resistance or lowered intracellular T4→T3 conversion. Rather, regulation of thyroid secretion must have been programmed at a higher level of the HPT-axis. We conclude that LG-UN programmed the TH-axis at the secretory level and differentially at target tissue level, which was increasingly manifested with age. Future studies are needed to clarify the implications of early programming of TH function on growth and health later in life.
Disorders of Thyroid Function Thursday Poster Clinical
Even though prompt and sufficient treatment of congenital hypothyroidism (CH) leads to normal intelligence, affected children still have mild IQ reductions and subtle visuospatial, sensorimotor, and auditory-processing deficits. Rodent models show a lack of thyroid hormone in the same period, as CH leads to abnormal cortical layering and reduced process growth in axons and dendrites. While recent MRI studies of CH adolescents show subcortical abnormalities, no study has as yet directly examined cortical morphology, which is now possible with advanced MRI processing.
Participants were 83 who were 10–16-year olds, 41 with CH, and 42 matched controls. All received MRI on a 1.5T GE magnet. Anatomical scans were processed using FreeSurfer v4.4 default pipeline. Groups were compared within FreeSurfer using the General Linear Model corrected for multiple comparisons and for average cortical thickness within regions using SPSS. Within CH, results were also analyzed by indices of disease severity.
CH showed multiple areas of cortical thinning, especially in the right hemisphere as well as some cortical thickening relative to controls (see Figure). Thinning was primarily observed along lateral (superior) aspects of cortex, whereas thickening was seen more medially. Thickening, but not thinning, was correlated with CH severity at diagnosis. The dyshormonogenesis group was less affected than dysgenetic groups. Regions showing thinning corresponded to substrates of weak-ability areas in this population.
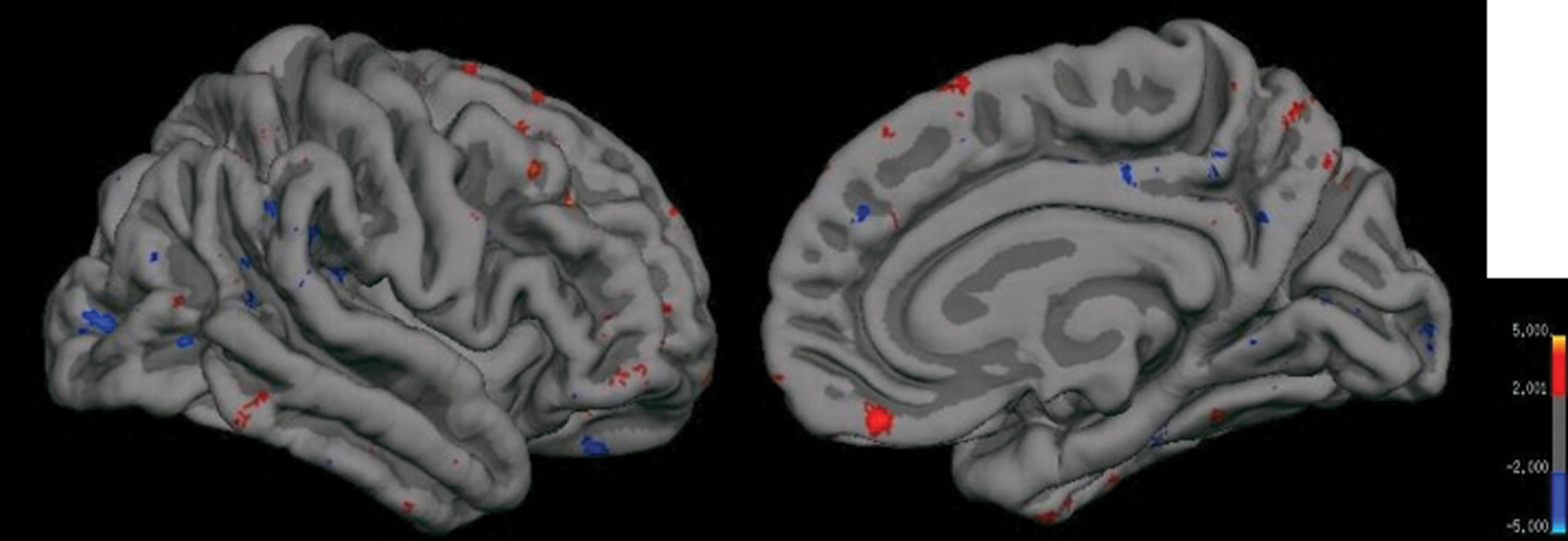
Cortical thickness map of right hemisphere showing comparison between 42 controls and 41 CH. Areas shown in red signify cortical thinning in CH, whereas areas shown in blue signify cortical thickening. Left is lateral view, and right is medial view. Similar effects were observed in left hemisphere (not shown).
Present results suggest that the persisting cognitive deficits in adolescents with CH may reflect distinct neurodevelopmental perturbances from early TH insufficiency. Cortical thickening observed in earlier-developing medial brain regions may reflect abnormal neuronal migration in the perinatal period, whereas cortical thinning in later-maturing lateral/superior brain regions may reflect abnormal process growth in the infancy period before euthyroidism. The specific functional implications of these cortical morphology abnormalities have yet to be determined.
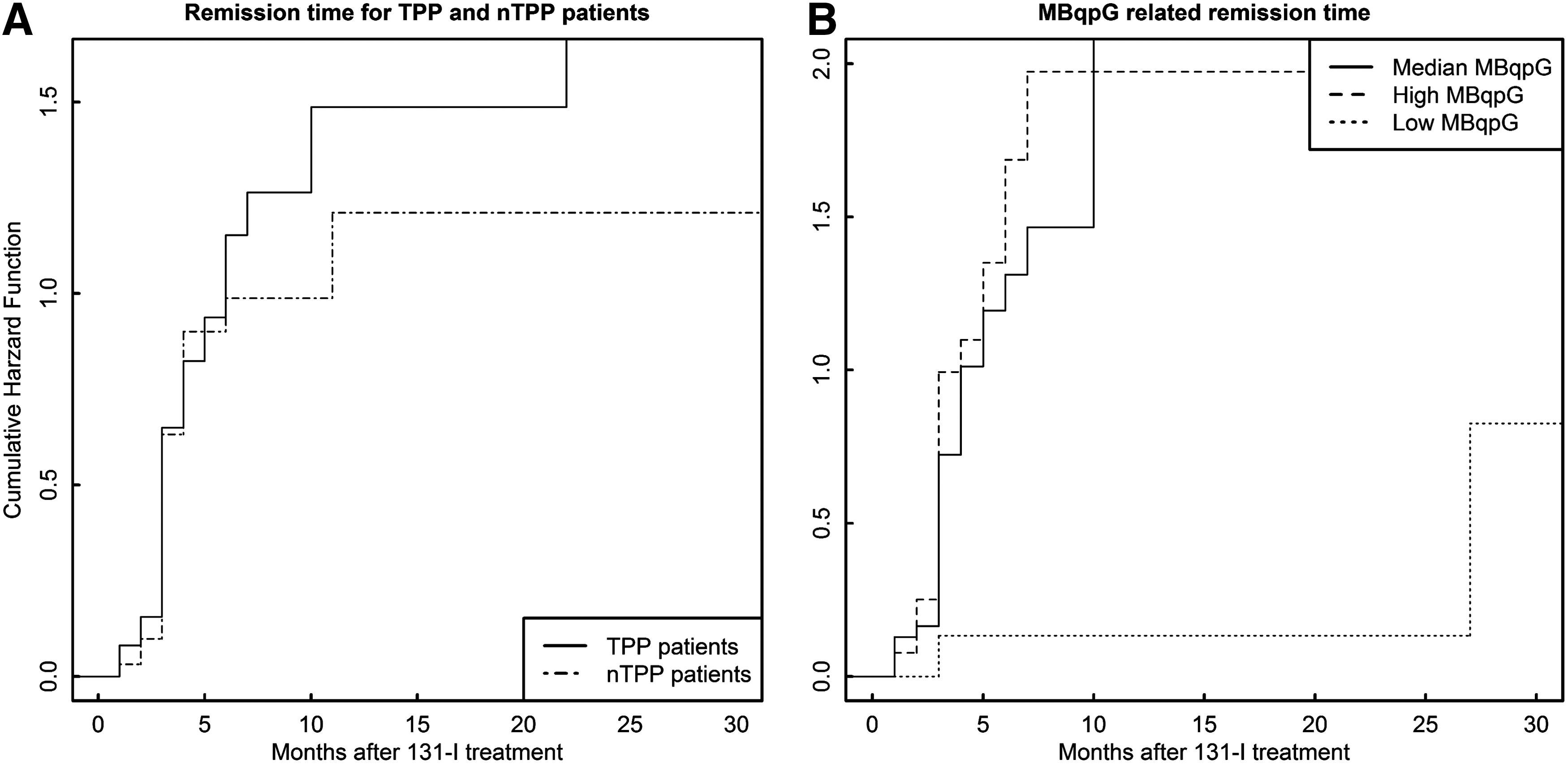
Disorders of Thyroid Function Thursday Poster Clinical
Thyrotoxic periodic paralysis (TPP) is a complication of thyrotoxicosis mainly observed in male Asian patients. Patients are observed to have lower thyroid hormone level. We want to prove this observation and to evaluate whether a lower 131I dose is feasible for prompt control.
One hundred thirty TPP patients were enrolled into study in a 7-year period. Their baseline characteristics were compared with 33 thyrotoxic patients without periodic paralysis (nTPP). A different 131I dose was given to 90 TPP patients. They were followed-up for a median time of 11 months, and the outcome was evaluated.
Around 94.6% of TPP patients were men, with a median age of 33 years (95% CI: 20–53 years), which was 9 years younger than nTPP patients (p<0.001). All patients had elevated free T3 (fT3) and free T4 (fT4). Around 98.7% of patients had elevated serum total T3 (tT3), while only 87.8% had total T4 (tT4) elevated. FT3, fT4, and tT4 in TPP patients were reduced by 22.7%, 23.5%, and 13.9% compared with that in nTPP patients (p=0.012, 0.034, and 0.007, respectively). After 131I therapy of different dose, patients who received lower 131I radioactivity per gram thyroid tissue (MBqpG) reached an undesirable overall and 3-month remission rate of only 28.6% and 12.5%, respectively, both of which were much lower than that of the median MBqpG (93.5%, p<0.001; 48.5%, p=0.021). Longer time to remission (p=0.004, HR=1.846, 95%CI: 1.216–2.798) was also observed in patients with lower MBqpG.
TPP mainly took place in younger Chinese men. Their serum thyroid hormone levels tend to be lower. Low-MBqpG dosimetry failed to achieve rapid control of thyrotoxicosis and should be avoided.
Time before remission between
Disorders of Thyroid Function Thursday Poster Clinical
The initial treatment for children with Graves' disease (GD) is antithyroid drug (ATD) treatment. The remission rate with ATD treatment in children is considered to be lower than that in adults. The prognostic factor for remission in each study was different.
We retrospectively studied 1138 children aged 18 years or younger who were newly diagnosed with GD between 1982 and 2006 [median age 16 (3–18) yr, 995 females]. GD diagnosis was based on thyrotoxicosis and high TRAb level or elevated diffuse thyroid uptake of radioactive iodine. All patients were initially treated with ATD. The median duration of follow-up was 10.8 (1–28.4) yr. Remission was defined as maintaining euthyroidism more than 12 months without ATD treatment.
Of 1138 patients, 723 continued ATD; 271 underwent surgery or radioactive iodine therapy before ATD withdrawal; and 144 dropped out. Of 723 patients, 639 stopped ATD [the median duration of treatment: 3.8 (0.3–24.8) yr], and 84 continued ATD treatment. Of 639 patients, 334 (52.3%) achieved remission, 247 (38.7%) relapsed, and 58 (9.1%) dropped out. In relapsed 247 patients, 32 had definitive therapy, and 215 continued ATD treatment. GD recurred in 182 of 247 (73.7%) patients within 2 years after ATD withdrawal. In this study, no significant prognostic factor associated with remission was detected, even though the potential variables previously reported were analyzed. The prevalence of all adverse events induced by methimazole (MMI) and propylthiouracil (PTU) was 21.4% and 18.8%, respectively: itching eruption [17.8% and 8.9% (p<0.01)], liver dysfunction [0.6% and 5.5% (p<0.01)], agranulocytosis (0.4% and 0.7%), and joint pain (1.1% and 0.7%). Positive antineutrophil cytoplasmic antibody was detected in 5 cases treated with PTU. High-dose MMI (∼6 mg/kg/day) resulted in a significantly higher incidence of eruption than low dose (p<0.01).
The remission rate was relatively high (52.3%), and no significant prognostic factor was identified in this study.
Endocrine Unit, San Francisco VA Medical Center, University of California, San Francisco, CA
Disorders of Thyroid Function Thursday Poster Clinical
Hypoparathyroidism (HypoPARA) is a rare endocrine disorder characterized by absent or low levels of parathyroid hormone (PTH), leading to hypocalcemia and hyperphosphatemia. Therapy is limited to symptomatic management with large doses of calcium (Ca) and calcitriol; however, their long-term use may lead to complications.
A phase III randomized, double-blind, placebo (PBO)-controlled, 24-week study assessed whether recombinant human parathyroid hormone (rhPTH[1–84]) reduced Ca and calcitriol needs, while normalizing or maintaining albumin-corrected total serum Ca levels in HypoPARA. Patients received 50 μg/day SC injections of rhPTH(1–84) or PBO; dose escalation up to 75 and then to 100 μg/day was permitted if calcitriol and oral Ca supplements could be further reduced. Of the 134 randomized patients, 53% of rhPTH(1–84) and 2% of PBO-treated patients were responders (p<0.001; defined as patients whose need for oral Ca and calcitriol could be reduced by 50% at week 24 while maintaining a serum Ca level of ≥baseline). rhPTH(1–84) treatment was generally well tolerated, with hypocalcemia, muscle spasm, paresthesia, headache, and nausea being the most common adverse events. Here we report the efficacy of rhPTH(1–84) in those who developed HypoPARA postsurgery (n=99) and those due to nonsurgical causes (n=35).
HypoPARA resulted from surgery in 76% of rhPTH(1–84) and 71% of PBO patients. Nonsurgical causes included genetic disorder, radiation exposure, autoimmune, or idiopathic disease. Within the postsurgical subgroup, a significantly higher proportion of rhPTH(1–84) patients were responders compared to PBO (57% [39/68] vs. 3% [1/31]; p<0.001). This was also observed within the nonsurgical subgroup with a significantly higher response rate among rhPTH(1–84) patients compared to PBO (41% [9/22] vs. 0% [0/13]; p=0.0131). Among rhPTH(1–84)-treated patients, the response rate was similar, but not statistically significant between the postsurgical and nonsurgical subgroups.
A high proportion of both subgroups responded to rhPTH (1–84), suggesting that surgical or nonsurgical etiology does not impact the efficacy of rhPTH(1–84) for treatment of patients with HypoPARA.
SUCCESSFUL MANAGEMENT OF THYROID STORM WITH PLASMAPHERESIS
Disorders of Thyroid Function Thursday Poster Clinical
A 53 YO man with h/o CHF with EF of 20–30% and Graves' disease presented with worsening SOB, due to tachycardia-induced cardiomyopathy with flash pulmonary edema. He was found to be in atrial fibrillation (afib), which cardioverted to NSR. TSH was <0.01; FT4 was elevated 4.22(0.8–1.9) NG/DL; FT3 was 9 (2.3–4.2) PG/ML. Because of worsening respiratory distress, he was intubated. We started Methimzaole 20 Q4H, propranolol, Hydrocortisone 100 Q8H, and potassium iodide (KI). While on propranolol, he developed severe hypotension that required vasopressors, and the patient developed acute liver and kidney injuries; his AST went up from 32 IU/L on admission to 13390, while his ALT increased from 27 IU/L to 6060 by the third day of admission. During the first five days of his hospitalization, this current treatment failed to control his afib or his thyroid function. We started plasmapharesis, and we also added Cholestyramine 4 GM Q6H. The response was very slow, but the patient showed gradual improvement in his thyroid function after three days of plasma exchange. His cardiovascular and liver function parameters improved. We tapered his thyroid medications, and he was finally extubated. We continued hemodialysis for an additional week. His thyroid, liver, and kidney function normalized to baseline.
Conclusions: Thyrotoxicosis management can be challenging, and thyroid storm can have devastating outcomes. Our patient failed to respond to the standard regimen, possibly due to impaired intestinal absorption from underlying GI edema. Parenteral forms of PTU or Methimazole are not available in the United States, but the rectal form has been used, although not routinely available. Special request and preparation for rectal form are required, which poses a barrier to expedited utilization. Furthermore, difficulty in administration of therapy is inconvenient for both the patient and ancillary staff. The thought of decreased gastrointestinal (GI) absorption due to GI edema was entertained. Based on the available published case reports regarding plasma exchange use as an adjunct therapy for refractory thyrotoxicosis and thyroid storm, we report our experience with a successful use of plasmapheresis in the management of resistant thyroid storm.
CLINICAL FEATURES OF AUTOIMMUNE THYROID DISEASE IN THE HOSPITAL OF H. HASHIMOTO—(1) CHRONIC THYROIDITIS
Disorders of Thyroid Function Thursday Poster Clinical
Clinical features of chronic thyroiditis were evaluated in the Kyushu University about 60–100 years after the report by H.Hashimoto.
Iodine intake in this area was 0.1–10 mg/day. Between 1972 and 2012, 2700 patients with chronic thyroiditis, diagnosed by the presence of thyroid autoantibody excluding Graves' disease, visited our Department. Thyroid function was evaluated in 1968 untreated patients, who were classified by thyroid weight (Wt) estimated by palpation and Allen-Goodwin formula, or by echography (normal 5–18g; n=152), such as (A) impalpable (Wt<10g) 347 cases, (B) small (10–30g) 773 cases, (C) moderate (30–60g) 611 cases, and (D) large (>60g) 237 cases.
Prevalence of thyroid dysfunction was as follows: euthyroid (45%), latent hypothyroid (19%), overt hypothyroid (TSH>40 mU/L) (26%), painless thyroiditis (10%), acute exacerbation (0.6%), and malignant lymphoma (0.7%). Among overt hypothyroid patients, 9% were postpartum (mostly Group B and C), 30% were nonpostpartum reversible hypothyroid (Group B–D), 43% were irreversible hypothyroid (Group A and B), and 19% were undetermined. The prevalence of the patients with large goiter (Group D), tentatively diagnosed as classical Hashimoto thyroiditis with TSH-independent goiter more than three times larger than normal, was rare in the young generation, but increased with age, about 9% in the people aged between 40–70 and 12% in the people aged 70 or over.
Clinical manifestation of chronic thyroiditis was various. Although about 50% of the patients were euthyroid, reversible or irreversible dysfunction was observed mainly in the patients with moderate or small goiter, respectively. The prevalence of goitrous so-called Hashimoto thyroiditis was estimated to be about 12% and increased with age. It is important to predict and prevent the growth of goiter and occurrence of lymphoma.
Endocrinology, McGill University, Montreal, QC, Canada
Disorders of Thyroid Function Thursday Poster Clinical
It is now recognized that thyroid autoimmunity, including Graves' disease, can occur after radioactive iodine treatment for nonimmune thyroid nodular disorders. In contrast, Graves' disease as a sequelum of thyroid surgery for thyroid nodules is less well known. We describe two patients who were documented to have Graves' hyperthyroidism after hemithyroidectomy for thyroid nodule.
Case 1: A 32-year-old female patient with a 5-cm nodule in the right thyroid lobe. Euthyroid and test for anti-TPO antibody negative. Strong family history of thyroid disease, involving her mother and 3 maternal aunts. Right hemithyroidectomy was carried out, and the final pathology was benign. Subsequently, developed a cystic lesion in the left lobe, for which she underwent multiple aspirations. Nine years after the hemithyroidectomy, she became thyrotoxic, and tests for both anti-TPO and TSH-receptor antibodies became strongly positive. There was increased uptake by the left lobe on thyroid scanning. The patient was treated with radioactive iodine.
Case 2: A 28-year-old female patient with a nodule in the left thyroid lobe, suspicious for a follicular neoplasm. TSH normal and anti-TPO antibody negative. Both parents have hypothyroidism. Left hemithyroidectomy carried out with benign pathology. Eight years later, she developed hyperthyroidism and ophthalmopathy with positive anti-TPO and TSH receptor antibodies. Thyroid uptake was increased at 53% with homogeneous distribution of the tracer. She was treated with Methimazole.
The development of thyroid autoimmunity after thyroid surgery for nonimmune nodular disease is unusual. There is a plausible mechanistic explanation for this sequence. It is postulated that the surgical intervention caused the release of an excess amount of thyroid antigens, and in susceptible persons, this could trigger an immune response to the appropriate antigens, including the TSH receptor. Documentation and study of such cases are not only clinically relevant but also pertinent to understanding the repertoire of pathogenetic mechanisms in thyroid autoimmunity.
ASSESSMENT OF URINARY IODINE CONCENTRATION IN KOREAN ADULTS
Iodine Uptake & Metabolism Thursday Poster Clinical
An adequate iodine consumption has been a worldwide health issue. Because approximately >90% of dietary iodine is excreted in the urine, urinary iodine concentration (UIC) is considered as an index of recent iodine intake. We investigated urinary iodine excretion in Korean adults to evaluate the status of dietary iodine intake.
The euthyroid subjects who visited the clinic were retrospectively reviewed from August 2009 through February 2012. The study included iodine measurement in a spot urine sample, of whom TSH information was available. We excluded patients with iodine-containing drugs such as amiodarone, previous CT scanning history within 90 days, or renal insufficiency. The iodine content was assessed by UIC and by iodine/creatinine ratio (μg/gCr) to minimize the variation in the urinary volume. We conducted logarithm transformation of the UIC and iodine/creatinine ratio and statistically analyzed using SPSS 19.0.
Nine hundred ten subjects were included in this study (751 women and 159 men). All subjects were in euthyroid state at the time of urinary iodide survey (mean TSH 2.06 mIU/L, 95% CI 1.99–2.13). The mean age was 48.4 years (SD 12.40). Median UIC was 374.1 μg/L (range 3.9–5819.0 μg/L), and the median iodine/creatinine ratio was 341.2 μg/gCr (range 8.9–12, 101.7 μg/gCr). There was no significant difference between women and men (p=0.405). The study subjects were divided subgroups by stratifying for age (<30 yr, 30s, 40s, 50s, >61 yr). There were significant differences in UIC (Log[UIC], p=0.042) and urinary iodine/creatinine ratio (Log[I/Cr], p<0.001) between the age groups. UIC and urinary iodine/creatinine ratio had slightly increased patterns according to age (p<0.001).
Dietary iodine intake of euthyroid Korean adults was excessive according to the World Health Organization criteria for assessing iodine nutrition (excessive>300 μg/L). Old age was associated with significantly higher UIC and urinary iodine/creatinine ratio, which reflect higher iodine consumption in this age group.
DECREASED HEALTH-RELATED QUALITY OF LIFE AFTER REMISSION OF DIFFERENTIATED THYROID CANCER
Thyroid Cancer Thursday Poster Clinical
Overall survival of patients with differentiated thyroid cancer (DTC) has been very excellent. However, there were few studies focusing on the health-related quality of life (QoL) in the disease-free survivors of DTC after remission. The aim of this study was to assess the QoL in the long-term disease-free survivors of DTC.
Total 268 patients with DTC at least 1 year after remission and 82 healthy controls were included. The 36-Item Short-Form (SF-36) was used to measure their health-related QoL. It is a widely used validated questionnaire, which measures physical health in 4 domains: physical functioning, role-physical, bodily pain, general health, and emotional health in 4 domains: vitality, social functioning, role-emotional, and mental health. Two summary scores, Physical component summary (PCS) and Mental component summary (MCS) were calculated using a norm-based (mean 50, SD=10) scoring method.
Among 268 patients, 246 (91.8%) patients completed questionnaires. Median time from the disease remission was 35.9 months (95% CI 38.76–45.50). Based on the TNM stage, 184 (74.8%) patients had stage I disease; 5 (2.0%) had stage II; and 52 (21.1%) had stage III disease. Radioactive iodine therapy was performed in 226 (91.9%) of the patients, and the mean cumulative dose was 126.6 mCi (median 105 mCi, range 0–660 mCi). When compared with healthy controls, disease-free survivors of DTC demonstrated significant impairment in the MCS score (mean MCS, patients 45.94, controls 49.14, p=0.018), especially in Vitality (p=.001) and Mental health (p=.006) domains. PCS score did not show significant differences between patients and controls (p=0.928). Thyroid function did not affect QoL of the patients, when adjusted variables for age and gender (PCS p=0.690; MCS p=0.003).
Our results showed that disease-free survivors of DTC experience decreased QoL, especially in the mental component area, independent of their age and gender. Thus, clinicians need to pay attention to the factors that might affect QoL in the care of these patients.
PCS and MCS Scores in Patients with DTC After Remission Compared with Controls
Thyroid Cancer Thursday Poster Basic
Previous analysis aimed at identifying differentially expressed genes in papillary thyroid carcinomas identified the gene, hNAA15 (previously called NATH), as upregulated in tumor tissues, and especially in aggressive tumors, compared to matching nontumor tissue (Fluge et al., Oncogene, 2002). Further studies revealed that this gene encoded a subunit in the protein complex, NatA (Arnesen et al., Proc Natl A, 2005). This complex is the major N-terminal acetyltransferase (NAT) in eukaryotic cells, catalyzing the transfer of an acetyl moiety from acetyl co-enzyme A to the N-termini of nascent polypeptides. This process is shown to be occurring on nearly 80% of all proteins in humans (Arnesen et al., Proc Natl Acad Sci U S A, 2009) and is thought to occur mainly cotranslational, but may also occur post-translationally. Recently, knockdown studies of NatA in several different thyroid cancer cell lines showed inhibition of cell proliferation and increased sensitivity to drug-induced cytotoxicity (Gromyko et al., International Journal of Cancer, 2010), making NatA a potential drug target for thyroid cancer.
Based on the defined catalytical mechanism of one of the NATs (Evjenth et al., J Biol Chem, 2012) and defined substrate specificities of the NATs, we have designed and synthesized several bisubstrate analogs for several NATs, including NatA. The potency and specificity of the inhibitors have then subsequently been tested in vitro.
The in vitro data demonstrate that we have successfully identified potent and specific NAT-inhibitors with IC50 values in the low μM range. For one inhibitor, we have showed that it follows a typical slow-binding inhibitor pattern with Ki* in the low nM range.
As the in vitro data appear promising, we are now in the process of making these inhibitors cell permeable and testing their direct effect on downstream Nt-acetylation within cells as well as their effect on inhibiting cancer cell proliferation and survival.
Endocrinology, Diabetes, and Metabolism, Duke University Hospital, Durham, NC
Thyroid Hormone Metabolism & Regulation Thursday Poster Translational
Nonalcoholic fatty liver disease (NAFLD) is strongly associated with dyslipidemia, metabolic syndrome, and hypothyroidism. Whether serum thyroid hormone (TH) levels are associated with NAFLD disease severity is unclear. Objective: To define serum TH levels and thyroid-related liver gene expression differences between early and advanced NAFLD.
RNA was extracted and microarray performed from liver tissue of 70 patients with biopsy-proven NAFLD (42 early NAFLD and 28 advanced). Serum collected on the same day as biopsy was analyzed for thyroid-stimulating hormone (TSH), free T4 (fT4), free T3 (fT3), and reverse T3 (rT3). TH levels were compared between early vs. advanced NAFLD using Wilcoxon Rank-Sum tests. Logistic regression models were built with severity as the outcome and serum marker as the covariate. Differential gene expression was determined on normalized data by an empirical Bayes method with a 5% False Discovery Rate control.
No difference in age, gender, ethnicity, or history of hypothyroidism was noted in patients with early vs. advanced NAFLD. Diabetes mellitus was more prevalent in those with advanced NAFLD (p<0.01). Hyperlipidemia was more prevalent in early NAFLD (p=0.039). Serum fT3 was higher (p=0.024) and rT3 lower (p=0.004) in early vs. advanced NAFLD. After adjusting for age and BMI, fT3 and rT3 remained significant (p=0.026 and p=0.03, respectively). The fT3/rT3 ratio was lower in those with advanced NAFLD (p=0.001, adjusted p=0.007). Gene expression analysis revealed increased expression of THRSP in early NAFLD and increased expression of tissue-remodeling genes in advanced NAFLD (IGFBP6, RCAN2, and ITGAV). Spearman's rank correlations indicate a significant positive relationship between the serum fT3 and fT3/rT3 ratio, with RAC3 expression (ρ=0.55, ρ=0.46) (p<0.001), a gene important in morphogenesis and cellular migration.
Early NAFLD is associated with higher fT3 and lower rT3 levels than to advanced NAFLD. There are unique thyroid-specific gene expression differences in early vs. advanced disease. Our findings suggest that TH levels and/or hepatic responsiveness to TH may contribute to NAFLD disease severity.
Endocrinology, Diabetes, and Metabolism, Duke University Medical Center, Durham, NC
Thyroid Cancer Thursday Poster Basic
Hedgehog (Hh) signaling is a morphogenic pathway involved in cell fate decisions in many endodermally derived adult tissues. Hh signaling is critical in migration, differentiation, and growth of progenitor cell populations. Recent reports have established that Hh signaling is present in thyroid tumors, specifically follicular adenomas, papillary, and anaplastic thyroid cancers. No report has established that this cell-signaling pathway is present in medullary thyroid cancer (MTC). Objective: To determine if the Hh signaling pathway is present in endodermally derived parafollicular cells, specifically MTC.
Using both human thyroid tissue and established MTC human cell cancer lines, we used immunohistochemical (IHC) staining, quantitative real-time PCR, and Western Blot to determine presence of Hh in parafollicular cells. We manipulated Hh using various concentrations of SAG (0–2 uM), a compound shown to induce Hh activation through canonical signaling pathways, and GDC-0449 (Vismodegib) (0–10uM), a potent antagonist of Hh signaling.
Hh signaling is upregulated in MTC compared with normal thyroid tissue by IHC. Sonic Hedgehog (Shh) and Glioblastoma Family 2 (Gli2), a downstream target of Hh, are highly expressed in human MTC. Established human MTC cells lines, TT and MZ-CRC-1, were grown in F12K media+10% FBS+Pen/Strep and DMEM 1×Glucose+10% FBS+Pen/Strep, respectively. Cell lines were treated with SAG and GDC-0449 as varying concentrations. A dose–response curve showed that Hh activity in these MTC cell lines was only minimally activated by SAG, but significantly inhibited by GDC-0449 at doses of 0.4, 2, and 10 uM. GDC-0449 downregulation of Hh signaling was documented at the mRNA level and at the protein level. Cell Counting Kit-8 (CCK-8) was utilized and showed that at 24, 48, and 72 hours, SAG significantly increased cell number, whereas GDC significantly reduced cell number after treatment.
Hh signaling is a novel pathway in medullary thyroid cancer. It can be manipulated by canonical signaling agents: SAG and GDC-0449. Reduction of cell number with GDC-0449 as determined by CCK-8 assay suggests that this pathway may be important for novel drug therapy in MTC.
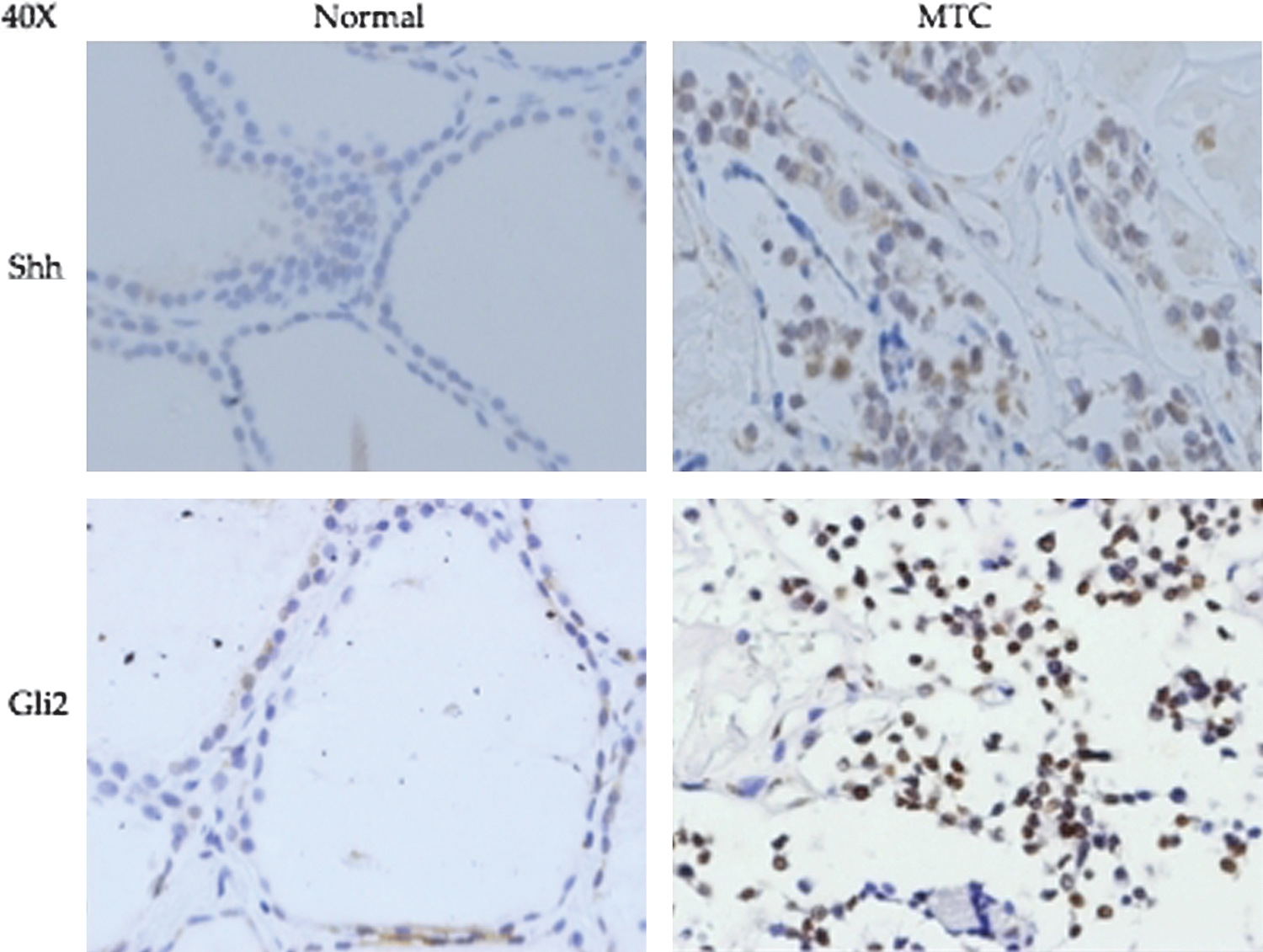
Hh signaling is upregulated in MTC compared with normal thyroid tissue by IHC. Sonic Hedgehog (Shh) and Glioblastoma Family 2 (Gli2), a downstream target of Hh, are highly expressed in human MTC.
Pathology, University of Pittsburgh, Pittsburgh, PA
Thyroid Cancer Thursday Poster Basic
The follicular variant of papillary carcinoma (FVPTC) shares features of papillary (PTC) and follicular (FTC) thyroid carcinomas. While the clinical course and the nuclear features are closer to PTC, the pattern of growth resembles FTC. We characterize the miRNA profile of the follicular variant of papillary carcinoma (FVPTC) and correlated it with clinicopathological data.
Seventeen (17) FVPTC, 27 classic PTC, and 8 normal thyroid tissues were studied for expression of 768 miRNAs using Human Microarray Assays (Applied Biosystems) on ABI 7900. miRNAs were isolated using the RecoverAll Total Nucleic Acid kit (Ambion) from FFPE tissue specimens (n=52). Data Assist, Statminer, and SPSS program were used for data analysis.
We found 14 miRNAs in the FVPTC to be significant dysregulated with a fold change of more than 5 (up/down). miRNAs that previously found to be upregulated in classic PTC, including miR-221, 222, and 146b, were strongly upregulated in FVPTC. In addition, novel miRNAs were found to be dysregulated in FVPTC, including miR-375, 551b, 181-2-3p, and 99b-3p. The latter two showed a significant adverse outcome in a Kaplan–Meier analysis, which was confirmed by multivariate-analysis (Cox regression).
Despite high similarity in miRNA expression between classic papillary carcinoma and follicular variant of PTC, several miRNAs were unique for FVPTC and showed association with adverse outcome. Strongly upregulated miRNA (miR-375) could serve as a novel diagnostic marker for papillary thyroid carcinoma.
Department of Otolaryngology-Head and Neck Surgery, McGill University, Montreal, QC, Canada
Thyroid Cancer Thursday Poster Basic
The aim of this study was to prospectively review the role of sentinel lymph node (SLN) biopsy in the management of well-differentiated thyroid carcinoma (WDTC), and to determine the efficacy of intraoperative frozen-section analysis at detecting SLN metastasis and central compartment involvement.
The SLN biopsy protocol using 1% methylene blue was performed in 271 patients undergoing thyroidectomy for WDTC. A central compartment neck dissection (CCND) was performed on all patients. Lymph nodes staining blue were considered as SLNs. Both frozen- and permanent-section analyses were performed.
SLNs with metastasis were found in 14.8% (40/271) of cases. Of this, 11.4% (31/271) were positive on intraoperative frozen-section analysis. Frozen-section results failed in predicting central compartment involvement in 14 cases (5.2%), whereas central neck compartment involvement was missed in 5 cases (1.8%) when based on permanent-section results. On frozen-section analysis, the sensitivity, specificity, positive predictive value, and negative predictive value (95% CI) of our SLN biopsy technique aiming to remove all disease from the central compartment were 68.9% (53.2; 81.4), 100% (97.9; 100), 100% (86.3; 100), and 94.2% (90.2; 96.7), respectively, with p<0.0001. On permanent-section analysis, the values were 88.9% (75.2; 95.8), 100% (97.9; 100), 100% (89.1; 100), and 97.8% (94.8; 99.2) with p<0.0001.
These data series demonstrate that patients with WDTC have positive SLNs in 14.8% of cases. Moreover, when the SLNs are negative for metastasis on frozen section, the central compartment was disease-free in 94.2% of cases. Finally, this study shows that 22.5% of positive SLNs were false negatives on intraoperative frozen section. According to these data, SLN involvement is an accurate predictor of central compartment metastasis; however, surgeons should use caution when relying on intraoperative frozen section to determine whether to perform a CCND.
THYROID CANCER STEM CELLS REVEALED BY CHEMOTHERAPY OF HUMAN ANAPLASTIC THYROID CANCER
Thyroid Cancer Thursday Poster Basic
Anaplastic thyroid carcinoma (ATC) has a rapidly fatal clinical course, being resistant to multimodal treatments. Cancer stem cells (CSCs) have been and hypothesized as responsible for resistance to traditional chemotherapy and subsequent tumor relapse. In this study, we aimed to identify and characterize chemotherapy-resistant cells derived from human ATC to determine whether CSCs are responsible for such resistance.
We used the ATC cell line T238. This line expressed the TSH receptor, Pax8, and TTF1, confirming thyroid origin. A resistant subpopulation of T238 cells was generated by continuous exposure to fluorouracil (5-Fu) (250 uM) for 5 days, which is known to induce thymineless death in susceptible cells. We then assessed the resistant T238 cells for their cancer stem cell-like traits.
The expression of pluripotent stem cell markers SSEA-1, Oct4, Sox2, Nanog, and CD133 was significantly enhanced in the resistant T238 cells when analyzed by qRT-PCR. By FACS analyses, we observed that cells expressing SSEA-1 were enriched by treatment with 5-Fu from <3% to >55% of the cell population. Using confocal microscopy, for live-cell imaging of fluorescently labeled SSEA-1 and α-tubulin, we were able to show that such cells had a greatly enhanced degree of asymmetric cell divisions (a 50% increase), illustrating the generation of heterogeneous progeny. These SSEA-1 positive cells also showed evidence of EMT initiation as evidenced by enhanced vimentin gene expression and decreased E-cadherin gene expression (a 260% increase versus 0.57% decrease, respectively) compared to SSEA-1-negative cells. Furthermore, these chemoresistant cells possessed multipotential differentiation capabilities, and under appropriate culture conditions, matured into lipid-containing adipocytes.
Our findings demonstrate that the T238 contains a heterogeneous cell population, including cells resistant to chemotherapeutic agents. This resistant phenotype has stem cell-like features. These cells likely arise from the original transformed thyroid cells and are able to perpetuate the cancer, suggesting that stem-like cells are the common product of neoplasia. Chemotherapy needs to be directed at this subpopulation of cells.
Internal Medicine, Endocrine and Metabolic sciences and Biochemistry, University of Siena, Siena, Italy
Thyroid Cancer Thursday Poster Basic
Praja2 is a RING ligase, which degrades regulatory subunits of PKA, thus controlling the strength and duration of PKA signal in response to cAMP. TSH, through activation of its receptor, increases cAMP inside the cells, sustaining tyrocyte growth and hormone production. Differentiated thyroid cancer (DTC) is a TSH-dependent tumor, and its function is modulating by TSH levels. We aimed to analyze the expression of PRAJA2 in a group of 36 DTC, 14 benign nodules, and 6 anaplastic thyroid cancer (ATC).
To this purpose, we measured mRNA levels by real-time RT-PCR and protein by western blot and immunohistochemistry. Possible association between PRAJA2 mRNA and presence of known mutations was evaluated.
We found a statistically significant (p<0.001) increase of mRNA levels in PTC compared to benign nodules and ATC. In particular, PRAJA2 RNA expression was maximal in well-differentiated histological variants and decreased progressively with loss of differentiation, ATC having the lower expression. Western blot revealed that PRAJA2 mRNA was translated into a functional protein with OD arbitrary units for PTCs significantly higher (p<0.001) compared to the benign nodules without data overlapping. By immunohistochemistry, we observed a marked cytoplasmatic localization of PRAJA2 in PTCs, which decreased in the less-differentiated variants and completely disappeared in the ATC. We then measured mRNA levels in three different cell lines stably expressing BRAFV600E mutation, RET/PTC1, and RET/PTC3 rearrangements. We observed a significant (p<0.01) increase in mRNA expression in RET/PTC1-positive cells compared to RET/PTC3, but not against BRAF-positive cells. Similar results were obtained with cancer tissues with the same mutations. Analysis of the clinical data showed that protein expression was not associated with outcome, TNM, and tumor diameter.
PRAJA2 is markedly overexpressed in DTC, and its protein expression decreases together with tumor dedifferentiation. The expression might be linked to the mutational status of the tumor.
Otolaryngology-Head and Neck Surgery, Johns Hopkins, Baltimore, MD
Thyroid Cancer Thursday Poster Translational
PD-L1, a protein displayed by many tumors, binds the PD-1 co-inhibitory receptor on activated T cells, leading to immunosuppression. Blockade of the PD-1/PD-L1 pathway has shown promising clinical results in patients with treatment-refractory solid tumors. In the current study, we assessed the presence of PD-1+T-cells in the tumor microenvironment, as well as tumor cell expression of PD-L1, to better characterize this novel mechanism of immune escape in papillary thyroid cancer (PTC).
Patients diagnosed with PTC who were undergoing surgical resection were eligible for the study. Mononuclear cells were isolated from the peripheral blood, primary thyroid tumor, and contralateral normal thyroid tissue (CNT). From these mononuclear cells, T-cell populations were evaluated for the expression of CD4, CD8, CD45, CD3, and PD-1 using multicolor flow cytometry. In addition, these same cell populations were evaluated in multinodular hyperplasic (MNH) specimens (benign control). Surgical PTC specimens were also analyzed by immunohistochemistry for expression of PD-L1.
CD4+/PD-1+ T-cells were increased in tumors and CNT when compared to blood (means: 63.90%, 64.20%, and 8.03%, respectively, p=0.0079). Cytotoxic CD8+/PD-1+ T-cells were also increased in tumors and CNT when compared to blood (means: 69.40%, 66.0%, and 17.3%, respectively, p=0.016). In MNH, there was no observed difference in CD8+ or CD4+ T-cell frequencies between blood and tissue. In PTC, membranous staining of PD-L1 was observed in 89% of specimens.
We identified an increase in CD4+/PD-1+ and CD8+/PD-1+ T-cells in PTC when compared to blood or MNH. In addition, membranous expression of PD-L1 was observed in PTC, suggesting that the presence of PD-1+ T cells may be driving tumor cell expression of PD-L1 to create an immunosuppressive microenvironment, a mechanism that we term adaptive immune resistance. Further studies are needed to identify individual factors produced by T-cells that drive PD-L1 expression in the tumor cells. It is the eventual hope that blockade of the PD-1/PD-L1 pathway will offer a clinical benefit to patients with treatment-refractory PTC.
GENETIC ALTERATIONS IN ANAPLASTIC AND POORLY DIFFERENTIATED THYROID CARCINOMA
Thyroid Cancer Thursday Poster Translational
Anaplastic thyroid carcinoma (ATC) is a very aggressive malignancy. Its incidence is 1–2% among all thyroid tumors. ATC can originate directly or develop from pre-existing thyroid tumors after the acquisition of specific genetic alterations. Poorly differentiated thyroid carcinoma (PDTC) is classified as a separate entity with respect to ATC and well-differentiated thyroid cancer. Its incidence is about 5%, and its prognosis, although severe, is relatively better than ATC prognosis. Molecular mechanisms responsible for the development of ATC and PDTC are not well defined, although many genes (i.e., BRAF, RAS, beta-catenin, PIK3CA, TP53, AXIN1, PTEN, and APC) have been found to be altered in these tumors. The purpose of this study was to define the prevalence of genetic alterations in ATC and PDTC.
Our series consisted of 14 cases of ATC and 13 cases of PDTC. Fresh tumoral thyroid tissues (n=22) and fine-needle aspirated material (n=5) were used for DNA extraction. Somatic mutations were analyzed by PCR and direct sequencing.
In the group of ATC, genetic screening allowed the identification of 2 cases with the BRAFV600E mutation, 2 cases with a somatic mutation in exon 8 of p53 gene (R273N and R267W), and a complex mutation of the PTEN gene (one base-pair deletion at codon 119 followed by an heterozygous somatic mutation Q97R). In PDTC, we found the AKTQ17K mutation in one case, a PIK3CAH1047R mutation in one case, and the BRAFV600E mutation in another case. No mutations of the RAS and beta-catenin genes were found. In addition to mutations with transforming activity, we identified the T1493T polymorphism of the APC gene in 6/8 cases (4 homozygous and 2 heterozygous) of PDTC, and in 8/11 cases (4 homozygotes and 4 heterozygotes) of ATC. We also found the p53 gene polymorphisms (R213R) in one ATC case.
These data show a quite low prevalence (5/14, 35%) of mutations in ATC. In particular, only 2 cases (14%) with p53 mutations have been found. An even lower prevalence (3/13, 23%) of mutations was observed in PDTC. In this group, there were no mutations of the p53 gene. Finally, the prevalence of the APC polymorphism was not different from the prevalence of the same polymorphisms in healthy controls (n=200).
Internal Medicine, Asan Medical Center, Seoul, Republic of Korea
Thyroid Cancer Thursday Poster Translational
X-linked inhibitor of apoptosis protein (XIAP) is a member of the inhibitor of the apoptosis (IAP) protein family that selectively blocks caspases-3, 7, and 9, and inhibits cell death. Embelin, an XIAP inhibitor, is known to exhibit anti-inflammatory and apoptotic activities. Recent reports suggest that embelin interferes the signal transducer and activator of transcription 3 (STAT3) pathway and the nuclear factor-kB (NF-kB) signal pathway. In this study, we investigated the anticancer efficacy of embelin by measuring its effects on apoptosis of thyroid cancer cell lines. We also explored the mechanism underlying these effects.
We used cell viability assay and apoptosis assay to analyze the effects of embelin in thyroid cancer cell lines such as FTC-133, CAL-62, KTC-1, and 8505C. We used western blotting to establish the effect of embelin on the p38 pathway.
We found that embelin induced the apoptosis of human thyroid cancer cell lines. The effect was more prominent in BRAF V600E-mutant thyroid cancer cell lines (KTC-1 and 8505C) than in BRAF wild-type cell lines (FTC-133 and CAL-62). The effect of embelin on cell apoptosis was associated with increased phosphorylation of p38. SB203580, a specific inhibitor of p38-MAPK, inhibited the embelin-mediated induction of cleaved caspase-3 activity in V600E-mutant thyroid cancer cell lines. Interestingly, embelin induced apoptosis in BRAF wild-type cancer cell lines, even after treatment of SB203580. These results indicated that another signaling pathway, not a p38 pathway, might be responsible for embelin-induced apoptosis in BRAF wild-type thyroid cancer cell.
Embelin-induced XIAP suppression resulted in an increase of apoptosis via phosphorylation of p38 in BRAF V600E-mutant thyroid cancer cell lines. Regulation of XIAP activity may be potentially useful as a treatment of thyroid cancer, especially in BRAF V600E-mutant thyroid cancer.
Surgery, University of Pittsburgh, Pittsburgh, PA
Thyroid Cancer Thursday Poster Clinical
Recurrence develops in ∼20% of patients with papillary thyroid cancer (PTC). Molecular testing is increasingly utilized in the management of PTC. However, as a novel technique, few studies with sufficient follow-up are available to assess the impact of its results on PTC recurrence. The aim of the present investigation was to examine the predictive ability of clinicopathologic parameters, including mutation testing, for PTC recurrence with long-term follow-up.
We conducted a single-center retrospective review of clinicopathologic characteristics in a consecutive series of PTC patients who had initial operation between 6/99 and 12/01, archived tissue available for molecular testing, and >1 year clinical follow-up. Retrospective molecular testing was performed for BRAFV600E, NRAS61, HRAS61, and KRAS12/13 mutations, and RET/PTC1 and RET/PTC3 rearrangements. Recurrence was diagnosed if 1) there was pathologic or cytologic confirmation of disease after reoperation, or 2) radiographic imaging demonstrated local or distant metastasis.
Analysis included 80 patients with a mean age of 46 years (range 13–78) and mean follow-up of 102 months (range 12–149). The recurrence rate was 19% (15/80) with mean time to recurrence of 55 months (range 1–133). The incidence of mutation-positive PTC detected by the study panel was 55/80 (69%). All 15 recurrences were mutation positive (12 BRAFV600E, 1 HRAS61, and 2 RET/PTC1), and no recurrences occurred in the 25/80 patients who were mutation negative, resulting in 27% PPV and 100% NPV for the panel in predicting PTC recurrence. Recurrence was also associated with extrathyroidal extension (p=0.03), lymph node metastasis (LNM) (p=0.001), and TNM stage III/IV (p=0.008) at presentation, but not with age >45 years (p=0.06), male gender (p=0.55), or PTC size >2 cm (p=0.05). Only LNM predicted recurrence on multivariable analysis (p=0.013).
With long-term follow-up, only mutation panel results and LNM at presentation were predictors of PTC recurrence. To optimize surveillance strategies, the routine use of molecular testing to identify PTC patients at risk for recurrence should be strongly considered.
Surgery, Eulji University College of Medicine, Seoul, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
Robotic total thyroidectomy (TT) with modified radical neck dissection (MRND) using a gasless transaxillary approach has been reported a safe and effective procedure with notable cosmetic benefits. In his study, we compared the oncological outcomes and quality of life in patients undergoing robotic TT and MRND with outcomes of those treated by conventional open procedures.
Between March 2010 and July 2011, 86 papillary thyroid carcinoma patients with lateral neck node metastasis were enrolled in this study; 40 underwent a robotic TT with MRND (robot group); and 46 an open TT with MRND (open group). These two groups compared in terms of their oncologic outcomes and safety as well as functional outcomes such as postoperative subjective voice or swallowing difficulties. Moreover, neck pain, discomfort, stiffness, sensory change, and cosmetic satisfaction after surgery were also evaluated using a modified quality-of-life symptom scale. An arm abduction test (AAT) and questions modified from neck dissection impairment index (NDII) were applied to all patients to measure neck and shoulder disability.
Although the mean operating time was significantly longer in the robotic group than in the open group, there were no significant differences in postoperative complication rates and oncologic outcomes, including the results of RI scans and serum Tg levels after surgery. The results of subjective voice and swallowing parameters were also similar. Postoperative neck stiffness and sensory change were significantly more frequent in the open group than in the robotic group. In particular, the mean cosmetic satisfaction score was significantly higher in the robotic compared to the open group. Although the recovery time of shoulder movement trends toward a little longer in the robot group, the results of postoperative AAT and NDII were not significantly different in the robotic group compared with the open group.
Robotic TT with MRND was found to be similar to conventional open procedures in terms of oncologic outcomes and safety. Moreover, this robot technique could offer several benefits for quality of life, including excellent cosmetic results, reduced postoperative neck stiffness, and sensory change.
Surgery, Eulji University College of Medicine, Seoul, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
To compare long-term outcomes after total thyroidectomy (TT) or thyroid lobectomy (LT) in a large cohort of patients with papillary thyroid microcarcinoma (PTMC), and to determine whether the tumor size (≤0.5 cm versus >0.5 cm) has a significant impact on the extent of surgery.
We evaluated 2014 patients with PTMC who underwent TT (n=1015) or LT (n=999) between March 1986 and December 2006 and for whom complete follow-up data were available for at least 5 years (median 11.8 years; range 5–26 years). Using propensity score (PS) matching to reduce the impact of treatment selection bias and potential confounding in an observational study, we compared overall survival (OS) and disease-free survival (DFS) in the overall cohort and in patients with tumors ≤0.5 cm and >0.5 cm in size.
After adjustment for differences in baseline clinicopathologic risk factors, we observed no significant differences between the LT and the TT groups in the risk of death (hazard ratio [HR] for the LT group, 1.05; 95% confidence interval [CI] 0.71 to 1.47, p=0.891) and locoregional recurrence (HR for the LT group, 3.08; 95% CI 1.99 to 8.05, p=0.194) in the overall matched cohort. Similar results were observed when we compared LT and TT in patients with tumors ≤0.5 cm and >0.5 cm.
The long-term rates of death and locoregional recurrence were similar in patients with PTMC who underwent LT and those who underwent TT. Moreover, the tumor size 0.5 cm was not a significant determinant of the extent of surgery in patients with PTMC.
Faculty of Medicine, McGill, Montreal, QC, Canada
Thyroid Cancer Thursday Poster Clinical
The goal of this study was to (1) determine the incidence of well-differentiated thyroid cancer (WDTC) in the contralateral thyroid lobe in patients undergoing completion thyroidectomy, and (2) identify features of the malignant tumor in the initial resection that increase the likelihood of malignancy in the contralateral lobe.
The medical records of consecutive patients (n=98) undergoing completion thyroidectomy between 2006 and 2012 at the McGill University Thyroid Cancer Centre were retrospectively reviewed. Pathology reports from the initial surgery and the completion thyroidectomy were reviewed. Other patient and thyroid nodule characteristics ascertained by the McGill Thyroid Nodule Score (ultrasound findings, exposure to ionizing radiation, etc.) were recorded as well. The group was divided based on final pathology findings following completion thyroidectomy (malignant vs. benign). The Independent T test and the two-tailed Fisher's exact test were used to assess statistical significance of correlation between the individual measured variables and recurrence.
Of the 98 patients, 48 (49%) had a malignancy in the contralateral lobe. The mean age of both groups were similar 46 vs. 48.2 (malignant vs. benign). The mean time to completion was 103 days (125.1 malignant vs. 82.3 benign). In the contralateral lobe, 89% (43/48) of malignancies were micropapillary carcinomas, and 40% (19/48) of malignancies were multifocal. The presence of at least one focus of micropapillary carcinoma in the initial hemithyroidectomy was associated with a 60% chance of malignancy in the completion thyroidectomy (p=0.042). There was no statistical significant correlation established for the following variables: presence of positive cervical nodes, extrathyroidal extension, positive resection margins, size, encapsulated tumors, angiolymphatic invasion, and the subtype of WDTC. Moreover, there was no correlation between any of the variants of papillary thyroid cancer and recurrence.
In this study, the rate of malignancy in the contralateral lobe was 49%. The presence of at least one focus of micropapillary carcinoma in the initial hemithyroidectomy was found to be a predictor of contralateral malignancy.
General Surgery, University of British Columbia, Vancouver, BC, Canada
Thyroid Cancer Thursday Poster Clinical
The current guidelines for surgical management of papillary thyroid microcarcinoma (PTMC) are largely based upon high-risk features. Some reports suggest that tumors <5 mm are less likely to have high-risk features than those >5 mm and may be managed conservatively. Our objective was to compare the clinical and histological characteristics of small (<5 mm) to large PTMC (>5 mm).
From 2002 to 2011, data were collected prospectively from 1459 sequential patients undergoing thyroid surgery at a single institution. Among these patients, 132 (9%) were found to have PTMC of <1 cm without the presence of a macrocarcinoma (>1 cm). We performed a retrospective analysis of these PTMC cases. Fisher's Exact test was used. Statistical significance was set at p<0.05 a priori.
Overall, 75 cases (57%) revealed small PTMC, 84 (64%) were aged >45, and 105 (80%) were women. Small PTMCs were identified more frequently than large PTMCs in older patients (63% vs. 37%) and female patients (61% vs. 39%), but this did not reach significance (p=0.07 and 0.09, respectively). High-risk features were assessed, including multifocality in 38 cases (29%), bilaterality in 8 cases (6%), extrathyroidal cancer extension (ETE) in 6 cases (5%), lymph node metastases in 9 cases (7%), and distant metastases in 1 case (<1%). A relationship between larger cancers and high-risk features was seen only with ETE. Six of 57 large PTMC (11%), but none of 75 small PTMC (0%) had ETE (p<0.01). Lymph node metastases were present in both small PTMC (5/9 cases) and large PTMC (4/9 cases). In the patients with LN metastases, 3/9 had zero high-risk features, 2/9 had a single high-risk feature, and 4/9 had two high-risk features. Extrathyroidal extension was seen in only 2 of the 9 patients with LN metastases. The single case of distant metastases was diagnosed in a 3-mm PTMC.
Diagnosis of PTMC is common after thyroid surgery. However, neither cancer size <5 mm nor the absence of high-risk features excluded the possibility of synchronous lymph node metastases. The significance of high-risk features in PTMC requires further study to identify the optimal management of this common endocrine malignancy.
Otolaryngology-Head & Neck Surgery, Oregon Health & Science University, Portland, OR
Thyroid Cancer Thursday Poster Clinical
The application of appropriate treatment for differentiated thyroid cancer (DTC), including extent of surgery and adjuvant therapy, is predicated on accurate patient risk stratification. Although risk factors for mortality from DTC have been well described on the population level, they have not been unified into a single algorithm to predict individual risk. This study aimed to develop a nomogram to estimate 10-year cause-specific mortality in well-to-poorly DTC.
A historical cohort of 9,666 patients with DTC recorded in the SEER National Cancer Registry from 1985 to 1995 was used to identify and quantify the most clinically relevant predictors of 10-year thyroid cancer-specific mortality. Competing risk regression was used for model selection and nomogram development. The predictive accuracy of the nomogram was internally validated using bootstrapping methods and assessed using the area under the receiver operating characteristic curve (AUC).
Ten-year cause-specific mortality was 3.7%. Significant predictors of mortality included age, gender, extracapsular extension, tumor size, nodal status, distant metastasis, and histology. The nomogram successfully estimated an individualized risk of mortality from DTC by assigning relative weights to each of these risk factors. Model discrimination and calibration were found to be very good.
This nomogram is the first prognostic model developed to predict the likelihood of thyroid cancer mortality for an individual patient with DTC. More accurate patient risk stratification using the nomogram has practical applications for clinical care and research.
Multivariable Test of Significance Stratified By Histology
Multivariable competing risks regression stratified on histology (compared to other histology, which includes poorly differentiated thyroid carcinoma).
Thyroid Cancer Thursday Poster Clinical
Refractory Thyroid Cancers (rTC) include differentiated thyroid carcinoma refractory to radioiodine treatment (rDTC), inoperable or metastatic medullary thyroid carcinoma (MTC), and anaplastic carcinoma (ATC). Their estimated incidence is 350 new cases per year in France.
Following a National project from the French National Institute of Cancer (INCa) for the standardization of clinical care of patients with rare cancers, a national network, called TUTHYREF, was created in 2008. It aims to standardize management of patients with rTC, to facilitate the access to innovation to all patients in France and enrolment in clinical trials, to set up a national database of rTC and to promote research. All patients are followed by regional multidisciplinary teams that include an endocrinologist, a surgeon, a nuclear medicine physician, and a medical oncologist. The network includes 34 regional expert teams localized all over France (including overseas departments), and a national expert team (IGR). Twice a month, a national Web conference is organized with the participation of all regional expert teams to present difficult clinical cases and determined through discussion a personalized care plan, in accordance with international guidelines. Then, recommendations are applied by each regional center.
Since September 2008, 79 Web conferences have been organized, with an average presentation of 9 rTC patients per Web conference. In May 2012, the National Clinical Database included data from 952 refractory patients (455 men, median age 56 years), 69% rDTC, 22% MTC, and 9% ATC. The TUTHYREF centers participated to 7 prospective trials, enrolling approximately 50 patients per year.
TUTHYREF improves standardization of care in France and facilitates access to the new treatment and research protocol. It allows studies on a large cohort of patients, including clinical and basic research.
Department of General Surgery, Vanderbilt Univ Med Ctr, Nashville, TN
Thyroid Cancer Thursday Poster Clinical
Incidental thyroid cancer (iTC) in patients treated operatively for benign thyroid disease has been historically low (<5%). Previous series have not specifically addressed iTC incidence in both euthyroid and hyperthyroid patients. This study examined the iTC frequency in patients referred for removal of benign thyroid disease in a multi-institutional surgical series.
Approximately 2551 patients underwent thyroidectomy at three tertiary-care institutions. Indeterminate/malignant diagnosis by FNA was excluded (n=1028). Cases of iTC were compared among 1523 patients with Graves' (G, n=264), nodular goiter (MNG, n=1095), and toxic nodular goiter (TG, n=164). Fisher's Exact and Chi-squared tests, ANOVA, and nonparametric t-tests were used.
Overall, 243 iTCs were recorded (15.9%): G (16/264, 6.1%), MNG (191/1095, 17.4%), and TG (30/164, 18.3%). iTC rates were significantly different between these groups (p<0.01) and significantly higher in MNG and TG vs. G (17.4% and 18.3% vs. 6.1%, respectively; p<0.01). No association was noted with iTC for gender, age, or performance of preoperative FNA (p>0.05). Mean iTC size was 1.05 cm (46%>0.5 cm and 39%>1 cm). Overall, 287 patients had lymphocytic thyroiditis (19%), but no significant association with iTC was found (p=0.42). Most patients underwent total thyroidectomy (80%) followed by lobectomy/other.
These data confirm higher-than-expected iTC rates compared to historical controls in the largest multi-institutional surgical series to date (15.9% vs. 3–5%). The percentage of iTC cases in nodular goiter or toxic nodular goiter patients was significantly higher than the iTC rate in Graves'. Thyroiditis was not associated with iTC. This study provides evidence that in patients referred for thyroidectomy, the best surgical approach to non-Graves' toxic goiter is a total or near-total thyroidectomy. These data also suggest that similar treatment may be prudent for nodular goiters regardless of preoperative FNA results.
Endocrinology, Mayo Clinic, Rochester, MN
Thyroid Cancer Thursday Poster Clinical
UPEA can effectively manage NNM in papillary thyroid carcinoma (JCEM 96: 2717–20, 2011). In 1991, we used UPEA to treat two left-central compartment NNM (9-mm and 1.1-cm diameter) in a psychiatrist, who had earlier undergone three neck surgeries with resulting transection of his right recurrent laryngeal nerve, and was now facing possible tracheostomy. His ablated MTC nodes disappeared on high-resolution sonography within 10 months and did not recur after 21 years of follow-up. In 1994, we used UPEA to treat hepatic metastases and selected NNM in a second MTC patient. Since 2001, we have ablated NNM with ultrasound-guided injections of 95% ethanol in another five MTC patients.
In this report, we describe these seven patients, their UPEA treatments, and their final status. At presentation, pTNM stages were II in one, IVA in 3, and IVC in 3. Pre-UPEA serum calcitonin levels were universally raised (median 619 pg/mL; range 24–35,000). UPEA was performed on selected NNM after a mean of eight years since initial presentation (range 4–16). Mean age of patients at UPEA was 50 years (range 38–72). Nine recurrent nodes (largest mean diameter 13 mm; range 10–18) were initially injected with a mean of 0.8 cc (range 0.35–2.3 cc) of 95% ethanol. Patients were followed-up for a median of 10 years (range 4–21).
At latest follow-up, all ablated NNM had shrunk and had no Doppler flow; 4/7 (57%) had disappeared on sonography. No patient after UPEA developed hoarseness. No ablated node re-grew, requiring further treatment. Four patients progressed locally. Two required neck re-exploration for NNM at different locations from UPEA sites; two had UPEA, avoiding re-exploration. In the two patients with localized disease (T2-4 N1M0), no further neck intervention occurred after 10 years follow-up, and calcitonin levels fell significantly. In the seven patients, nine neck re-explorations were avoided, and >346,000 dollars were saved. All seven patients are surviving after a mean of 19 years (range 14–33) since initial thyroidectomy.
UPEA will not usually influence the ultimate outcome in MTC, but it can effectively, harmlessly, and inexpensively eliminate selected NNM, avoiding the expense and morbidity of further neck surgery.
Metabolism, Endocrinology and Diabetes, University of Michigan, Ann Arbor, MI
Thyroid Cancer Thursday Poster Clinical
There is a variation in the use of radioactive iodine as treatment for thyroid cancer, and the factors involved in physician decision making remain unknown.
We surveyed physicians involved in thyroid cancer management from 251 hospitals. Respondents were asked to rate the factors important in influencing whether a thyroid cancer patient receives radioactive iodine. Multivariable analyses controlling for physician age, gender, specialty, case volume, and whether they administer radioactive iodine were performed.
The survey response rate was 63% (534/853). Extent of disease, adequacy of surgical resection, patients' willingness to receive radioactive iodine, and patients' age were the most important factors influencing recommendations regarding radioactive iodine to patients with thyroid cancer. Interestingly, both physicians' and patients' worry about death from thyroid cancer was also important in determining radioactive iodine use, especially for physicians with fewer thyroid cancer cases per year. In multivariable analyses, lower physician thyroid cancer patient volume was associated with a greater importance placed on patients' (p-<0.001) and physicians' worry about death (p=0.016). Other factors with higher importance to physicians with lower thyroid cancer patient volume include accepted standard at affiliated hospital (p=0.020), beliefs about radioactive iodine expressed by colleagues co-managing patients (p=0.003), and patient distance from the nearest facility administering radioactive iodine (p=0.012).
In addition to extent of disease and adequacy of surgical resection, physicians place importance on physician and patient worry about death from thyroid cancer when deciding whether to treat a patient with radioactive iodine. The factors important to physician decision making differ based on physician thyroid cancer case volume, with worry about death being more important for low-volume physicians. As the mortality from thyroid cancer is low, the importance placed on death in decision making may be unwarranted.
Nuclear Medicine Department, Peking Union Medical College Hospital, Beijing, China
Thyroid Cancer Thursday Poster Clinical
Clinical features of differentiated thyroid carcinoma (DTC) in pediatric and adolescent patients differed from that of adult patients. Study concerning clinical and pathological characteristics of this population would make a great contribution upon clinical management of pediatric and adolescent DTC.
A total of 32 DTC cases (≤18 years old) were enrolled in this study. They were stratified according to different age and gender. Aggressive features of these patients were analyzed.
Bilateral, multifocal, as well as extrathyroid invasion was more often in patients younger than 12-years old. Patients with bilateral tumor invasion, lymph node metastasis, or distant metastasis were younger than those without (p=0.042, 0.027, and 0.031, respectively). The aggressive features were similar between male and female gender in younger patients, while it appeared to be more aggressive in male adolescents. Papillary pattern, bilateral invasion, and multifoci were related to lymph node metastasis (p=0.000, 0.007, 0.001, respectively). Compared to patients received initial total thyroidectomy, a higher rate of distant metastasis was observed in those who did not (47.37% vs. 92.31%, p=0.011).
Pediatric and adolescent DTC presents with a more aggressive pattern, especially in male and patients younger than 12-years old. More attention should be paid on DTC patients with above features, and total thyroidectomy should be applied to reduce the risk of distant metastasis.
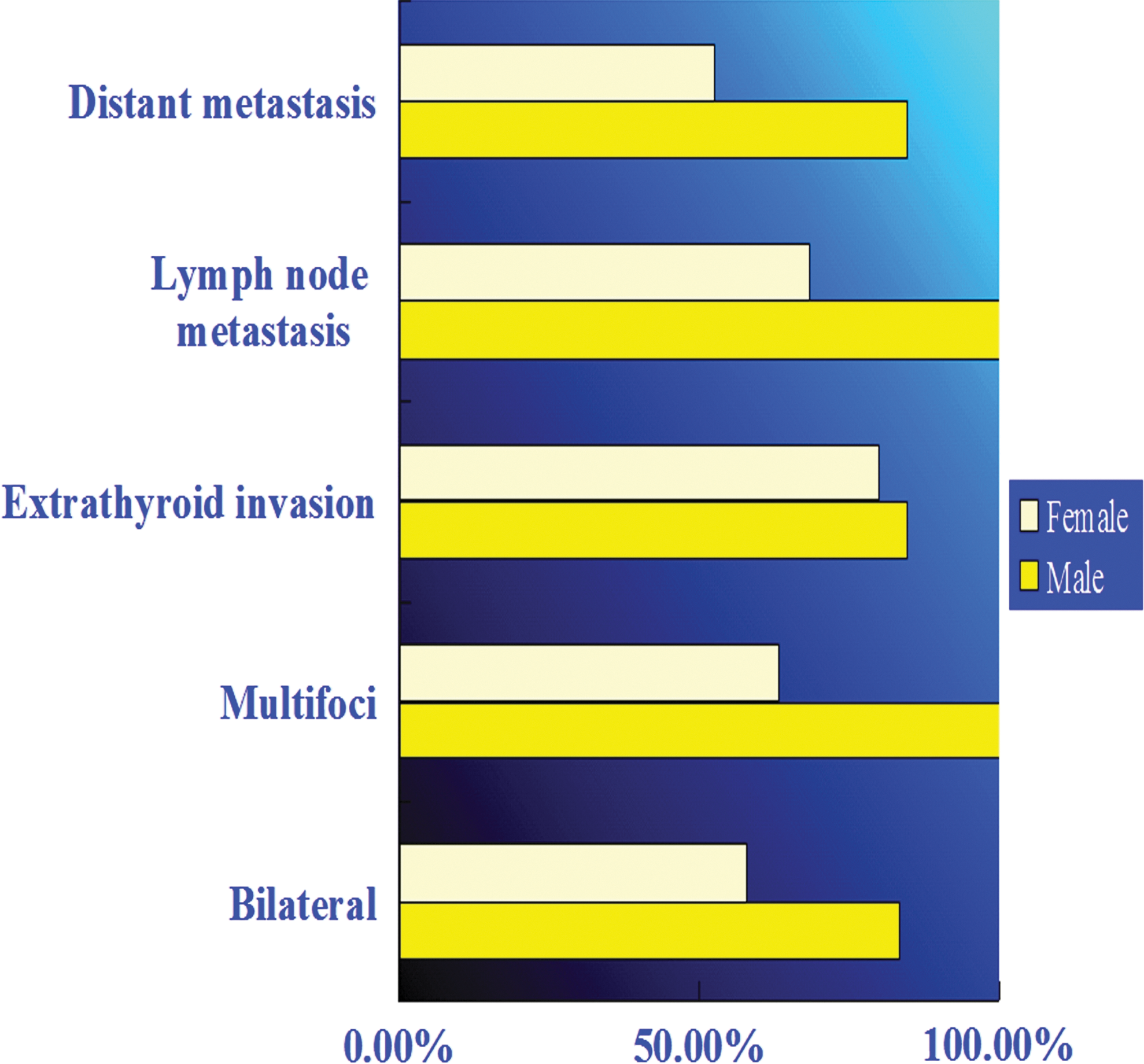
Investigation of aggressiveness of differentiated thyroid carcinoma in pediatrics and adolescents.
Thyroid Cancer Thursday Poster Clinical
There are limited studies examining the relationship between the volume of surgery and clinical outcome in thyroid cancer. Similarly, the effect of specialization in thyroid cancer surgery is of interest, as improvement in outcome has been demonstrated in other surgical specialty. We evaluated the volume–outcome relationship and the effect of specialization using preablation radioiodine-131 (131I) thyroid bed uptake scanning as a surrogate marker for the size of thyroid remnant after thyroidectomy for differentiated thyroid cancer (DTC).
We analyzed data of 651 patients in our thyroid cancer database. Patients data were included if the following criteria were met: 1) diagnosis of DTC, 2) total or near total thyroidectomy, 3) preablation 131I scan before radioiodine ablation (RAI), 4) no distant metastasis, and 5)>3000 MBq ablative dose of 131I. 131I diagnostic whole-body scans (DxWBS) and measurement of thyroglobulin (Tg) levels were carried out 3–9 months after RAI. Three hundred five patients were included in the final analysis.
Four endocrine,19 otolaryngology, and 25 general surgeons undertook thyroidectomies in the study with median preablation 131I thyroid bed uptake values of 1.0%, 1.8%, and 2.9%, respectively (p=0.0031). There was no statistical association between preablation 131I thyroid uptake value and Tg levels or thyroid bed uptake values in the DxWBS at 3–9 months post-RAI. The optimal number of cases required to achieve the lowest median preablation 131I thyroid bed uptake value in this study was 11.
Thyroid remnant quantification after thyroidectomy for DTC using the preablation 131I uptake scan is a useful tool to demonstrate the relationship between the volume of surgery and the size of thyroid remnant. The study also demonstrated beneficial effects of specialization with specialist surgeons achieving the smallest thyroid remnant. The median radioiodine activity given in our study (3500 Mbq) was effective in ablating large thyroid remnant.
THYROID STUNNING IN THE USE OF PREABLATION DIAGNOSTIC RADIOIODINE-131 SCANS IN DIFFERENTIATED THYROID CANCER: FACT OR FICTION?
Thyroid Cancer Thursday Poster Clinical
The stunning effects in thyroid tissue by diagnostic activities of radioiodine-131 (131I) remain controversial with conflicting data in the literature in the management of differentiated thyroid cancer (DTC). Many previous studies' endpoint examining the effect of stunning was determined by serial 131I diagnostic whole-body scans (DxWBS) rather than clinical outcome.
In 2004–2008, our institutional practice was to perform preablation 131I diagnostic scan 1 week before radioiodine ablation (RAI) in a patient with DTC after total thyroidectomy. The preablation diagnostic 131I dose was 30–40 MBq, and the scan was carried out at 24 hours after 131Iadministration. We changed our practice in only performing post-therapy 131I WBS without preablation scan from 2009 onward. We evaluated the clinical outcome in these 2 cohorts of the patient group in terms of TSH-stimulated thyroglobulin (Tg) levels, DxWBS after RAI, and the rates of local and distant recurrence in patients with DTC. Patients with distant metastases at presentation were excluded from the study.
About 305 patients had preablation DxWBS without post-therapy 131I WBS, and 237 patients had only post-therapy 131I WBS after RAI. The relationship between the TSH-stimulated Tg levels and DxWBS performed at 3–9 (median=6) months after RAI are summarized in the Table. There was no statistically significant difference in the 2 groups. At a median follow-up of 46.5 months, there were 13 (4.3%) and 8 (3.4%) recurrences (local and distant) in the preablation and post-therapy group, respectively, p=0.91.
The use of preablation 131I diagnostic dose of 30–40 MBq 1 week before RAI is not associated with adverse clinical outcome refuting the thyroid-stunning effect using low diagnostic I−131 dose.
The Relationship Between Tg Levels and Radioiodine Scan at 3–9 (Median =6) Months Following RAI
p=0.62.
Thyroid Cancer Thursday Poster Clinical
A patient with well-differentiated thyroid cancer treated with thyroidectomy and radioiodine who has detectable thyroglobulin (TG) in the context of negative diagnostic radioiodine scan suggests residual or recurrent thyroid cancer. We evaluated sensitivity and specificity for different radiological tests in detecting recurrence.
We reviewed results of investigations in patients with a raised TG after treatment, identified on a prospective database of patients with thyroid cancer in the Greater Manchester Network. Patients with thyroglobulin antibodies were excluded in the study.
From 2004 to 2010, 742 patients were treated radically (surgery and radioiodine ablation). Seventy (9%) had a raised TG during follow-up, and 38 (54.2%) of these were confirmed to have recurrence (45% local only, 42% distant alone, and 13% both local and distant recurrence). No specific level of TG correlated with the likelihood of detecting recurrence. Ultrasound alone (n=63) had a sensitivity of 47.6%, specificity 88.1%. USS plus biopsy (n=18) gave a greater sensitivity of 90.9%, specificity 88.1%. A second USS increases sensitivity to 55.6% and specificity is unchanged, 87.5% (n=33). PET-FDG scans had the highest sensitivity for recurrence, 91.7%, specificity 66.7% (n=33). CT sensitivity was 84.2% and specificity 90.9% (n=30). MRI neck sensitivity was 100%, specificity 71.4% (n=12).
Patients with raised TG investigated in this study, only just over half had their recurrence detected through various investigations. Ultrasound has a high specificity and is a useful first-line test. If a biopsy is possible, the sensitivity increases to 90.9%. A negative USS should prompt further investigations. PET scans offer superior sensitivity, but have less specificity for recurrence. A CT of neck and thorax offers the highest rates of detection and may be the most suitable second-line test. MRI neck has a sensitivity of 100%, but is limited to detecting local recurrence only.
THE UTILITY OF INTRAOPERATIVE ULTRASOUND IN MODIFIED RADICAL NECK DISSECTION: A PILOT STUDY
Thyroid Cancer Thursday Poster Clinical
Although the value of surgeon-performed neck ultrasound for thyroid nodules has been validated, the utility of intraoperative ultrasound in modified radical neck dissection (MRND) has not been reported in the literature. The aim of this study was to analyze utility of intraoperative surgeon-performed neck ultrasound in assessing the completeness of MRND for thyroid cancer.
Between 2007 and 2011, a total of 25 patients underwent MRND by one surgeon for thyroid cancer. All patients underwent intraoperative surgeon-performed neck ultrasound, which was repeated at the end of the neck dissection (completion ultrasound) to look for missed lymph nodes (LNs). The number of LNs removed, operative time, estimated blood loss (EBL), the number and location of missed LNs, complications, and recurrences were analyzed from an IRB-approved database.
There were 10 male and 15 female patients with a mean age of 55 years. Pathology included 23 papillary and 2 medullary carcinomas. The number of LNs removed per case was 23±2 and positive LNs 5±1. In 4 (16%) cases, intraoperative US detected 7 residual LNs, which would have been missed, if completion ultrasound was not done. These missed LNs were located in low level IV (3 nodes), high level II (2 nodes) and posterior level V (2 nodes) and measured 1.9±0.2 cm. In follow-up, recurrence was seen in 2 (8%) patients, including a superior mediastinal recurrence in a patient with tall-cell cancer and a jugular LN recurrence at the level II in another patient with papillary thyroid cancer.
This pilot study shows that intraoperative surgeon-performed ultrasound can help assess the completeness of MRND. According to our results, intraoperative completion ultrasound identifies LNs missed by palpation in 16% of the time.
Surgery, Jersey Shore University Medical Center, Neptune, NJ
Thyroid Cancer Thursday Poster Clinical
The rate of thyroid cancer has been increasing, which has also been attributed to improved detection. The aim of this study was to evaluate the initial mode of thyroid nodules detection in patients who underwent thyroidectomies, to correlate that with the pathology, especially differentiated thyroid carcinoma (DTC).
Five hundred and four consecutive patients underwent thyroidectomy from 2007 to 2011. Charts, family history, history of radiation exposure, surgery, and pathology reports were analyzed.
Of the 504 patients (430 women [85.3%], 74 men [14.7%]), 195 (38.7%) had DTC (PTC-176 [90.3%], FTC-6 [3%], HCC-9 [4.6%], and MTC-4 [2.1%]). Self-examination (96 patients [19.05%]) and examination by their primary-care physician (PCP) (96 patients [19.05%]) were the most common modes of detection. Twenty-eight (29%) of the self-examined patients and 33 (34.4%) of examined by PCP had DTC. Endocrinologists and gynecologists discovered nodules in 73 (14.5%) patients. CT, MRI, PET, and CXR (excluding US) detected nodules in 70 (13.9%) patients. Neck US (excluding thyroid) incidentally discovered nodules in 97 (19.2%), and 46 (47.4%) of them had DTC. Of the same 97 patients, 20 (3.97%) were discovered by carotid US, they had the highest rate of DTC (13/20=65% patients [2.6% of all DTC]). Together all imaging studies, 79 of 195 (40.5%) patients had DTC. The largest nodules were discovered by a third-party observer (∼3.76 cm), self-examination (∼2.55 cm), by gynecologist (∼2.54 cm), and by endocrinologist (∼1.69 cm), and they have a relatively high rate of DTC (16/33=48.5%). Family history of DTC in the first-degree relatives 29/504=5.75%, 16(55%) of them developed DTC (PTC-13, FTC-1, and MTC-2); in the 2nd-degree relatives 14/504=2.8%, 8 of them (57%) developed PTC. Radiation exposure were detected in 42 patients (8%), and 14 of them (33%) had DTC (2.78% of all DTC).
Self-examination and examination by the PCP are the most common mode of initial detection of thyroid nodules. Nodules incidentally found by imaging studies, especially carotid US, have a higher rate of DTC. Endocrinologists found DTC in earlier stages. Family history of DTC in the 2nd-degree relatives as important as in the 1st degree, those patients should have low threshold for surgery.
Initial Modes of Detection of Thyroid Nodules
Thyroid Cancer Thursday Poster Clinical
Paragangliomas (PGs) of the thyroid are extremely rare, slow-growing, locally aggressive neuroendocrine tumors, but have malignant potential and can be misdiagnosed. From 1964 to 2011, only 31 cases in the English literature were reported. The mean age of the patients was 48-years old (9 to 73 years), and the follow-up duration ranged from 3 months to 9 years.
We report the case of a 45-year-old man whose initial diagnosis was changed from medullary thyroid carcinoma (MTC) to malignant paraganglioma (PG) several years later after the review of original histology by expert pathologists during follow-up with his oncologist.
The patient was initially treated with total thyroidectomy and radioiodine ablation (small-papillary thyroid cancer component was thought to be present as a collision tumor) with thyroxine replacement therapy. The patient remains well and alive 13 years after initial presentation. It was a sporadic tumor without any positive family history of SDH B or SDH D gene mutations. This case is unique in that it was advanced stage (pT4 NX MX, TNM 5th Ed.) at diagnosis with one of the longest follow-ups reported (13 years), and it is one of very few reported in men.
This case highlights that 1) paraganglioma of thyroid can be misdiagnosed; 2) close collaboration between the clinician and pathologist is required; 3) in cases where there is a doubtful histology, especially when equivocal for MTC, specific immunohistochemical stains must be carried out and correctly interpreted by expert pathologists to rule out paraganglioma; 4) consensus guidance on optimal diagnosis and management of this rare type of tumor is needed; 5) expert multidisciplinary team (MDT) approach, including surgery, biochemical, and genetic screening and follow-up can lead to cure even in advanced tumors.
Northern Centre for Cancer Care, Freeman Hospital, Newcastle Upon Tyne, United Kingdom
Thyroid Cancer Thursday Poster Clinical
Introduction differentiated thyroid cancer (DTC) incidence is increasing worldwide. External beam radiotherapy (RT) is recommended in locoregional recurrence or locally advanced disease, when complete resection is not possible and/or when tumors do not concentrate radioactive iodine (RAI). Conventional radiotherapy techniques often cannot deliver high curative doses to all parts of the thyroid tumor. This is because the tumor-bearing area lies closely applied to normal organs at risk (OARs), particularly the spinal cord, parotids, constrictor muscles, esophagus, and larynx, where the radiotherapy dose must be kept within safe tolerance limits of the organs, which is well below the tumoricidal dose. Intensity-modulated RT (IMRT) where differential doses can be given to different parts of the tumor and normal organs has been recommended for thyroid cancer. Helical tomotherapy (HT) is a linear accelerator with a built-in CT scanner and can deliver superior quality of IMRT with image guidance (image-guided radiotherapy), in which daily pretreatment CT scan allows more accurate localization of the tumor target and avoids normal structures throughout a long course (5–6 weeks) of daily radiotherapy. FDG-PET CT scans, which are often used to stage recurrent and radioiodine refractory DTC, also delineate the most metabolically and biologically active part within the tumor with increased tumor cell burden, which can be radioresistant to standard doses. Focal higher dose of radiotherapy to these PET-avid areas with IM-IGRT is increasingly used in head and neck and other cancers in an attempt to increase local control and cure while safeguarding OARs.
We present our preliminary experience of safe dose escalation using PET-based delineation and HT in DTC.
HT has dosimetric advantages with less early and late side effects despite dose escalation PET-CT allows better coverage and dose escalation with HT, which may improve local tumor control.
To our knowledge, this is possibly the first report of this kind and merits further study.
Northern Centre for Cancer Care, Freeman Hospital, Newcastle Upon Tyne, United Kingdom
Thyroid Cancer Thursday Poster Clinical
Anaplastic thyroid cancers are rare and have a dismal prognosis. While surgery for limited disease has the best outcome, majority present late, and neoadjuvant adjuvant, definitive, and palliative chemo-/radiotherapy is usually associated with a median survival of between 3 and 12 months. In recent years, chemotherapy with Taxol and high-dose radiotherapy has been recommended. Because of the very short doubling time of the tumor cells, dose-dense chemotherapy with weekly Taxol is an attractive idea.
We have recently treated 3 anaplastic thyroid cancers with induction of weekly Taxol 80 mg per sq meter body surface area for 2 to 3 courses followed by 40 mg per sq meter weekly with tomotherapy-based high-dose intensity-modulated radiotherapy giving 66 Gy in 30 fractions to the tumor and 54 Gy to uninvolved nodal areas in 2 patients.
This is a preliminary finding, but the tolerance is better than other chemotherapy regimes, and the early responses are quite encouraging. Most importantly, patients have been able to finish their 6-week-long course of radiotherapy, which quite often is not possible. One patient required temporary NG feeding, and his histology was poorly differentiated squamous cell carcinoma incompletely resected, but has local control in the neck.
While it is not curative treatment, it would appear in our preliminary experience that weekly Taxol with high-dose tomotherapy-based intensity-modulated radiotherapy might be an option, which merits further study for anaplastic thyroid cancer.
Internal Medicine, Asan Medical Center, Seoul, Republic of Korea
Thyroid Cancer Thursday Poster Clinical
Obesity has been associated with increased incidence of cancers of the esophagus, colon, kidney, breast, melanoma, rectum, and gall bladder. There have been few studies on the relationship between obesity and thyroid cancer. We conducted this study to evaluate the association between obesity and incidence of thyroid cancer.
We recruited data of 16,481 (8,741 men and 7,740 women) subjects who were free of prior or family history of thyroid disease (thyroid dysfunction, nodule, cancer, and surgery), and who underwent thyroid ultrasonography from 2007 to 2008 in the Health Screening and Promotion Center of Asan Medical Center, Seoul, Korea. We retrospectively reviewed the medical records and analyzed risk factors predicting presence of thyroid cancer separately in men and women.
Of the 16,481 subjects, thyroid cancers were diagnosed in 227 (100 men and 127 women) patients, which were confirmed by surgery. In men, there was no significant association between the body–mass index (BMI) and incidence of thyroid cancer. In women, thyroid cancer incidence was significantly associated with BMI (per 5 kg/m2 increase) (OR=1.63, 95% CI: 1.20–2.18, p=0.001), after adjustment of age, smoking, TSH values. We also found that thyroid cancer was negatively associated with tobacco smoking in women (OR 0.29, 95% CI: 0.07–0.78, p=0.036).
Obesity was an independent risk factor for thyroid cancer in women when evaluated in a routine health check-up. Not only increased detection but also true increase of incidence caused by obesity might be responsible for the increasing incidence of thyroid cancer over recent decades.
THE IMPACT OF INTRAVENOUS IODINATED CONTRAST AGENT ON URINE IODINE EXCRETION IN PATIENTS WITH DIFFERENTIATED THYROID CANCER
Thyroid Cancer Thursday Poster Clinical
Current thyroid cancer management guidelines recommend delay of radioactive iodine therapy (RAIT) in patients who have been exposed to iodinated contrast agent in past 3–4 months. We aimed to evaluate the impact of iodinated contrast on urine iodine excretion (UIE) after contrast-enhanced computed tomography (CT) and to provide an appropriate time interval for RAIT preparation after iodinated contrast administration.
We retrospectively reviewed UIE levels of 1,063 patients with differentiated thyroid cancer (DTC) who underwent preoperative CT with iodinated contrast agent, total thyroidectomy, and 1 week of low-iodine diet (LID) in preparation for RAIT within 6 months of CT scan. UIE was measured as spot urine iodine (μg) divided by gram Cr (I/Cr) (μg/gCr). The study subjects were divided into five groups according to the time interval between CT and RAIT (31–60, 61–90, 91–120, 121–150, and 151–180 days).
The median UIE in groups 31–60 (n=21), 61–90 (n=164), 91–120 (n=573), 121–150 (n=231), and 151–180 days (n=74) was 44 (interdecile range [IDR]: 13.2–126), 34.6 (IDR: 16.9–241.6), 33.4 (IDR: 15–153.6), 32.3 (IDR: 14.4–114.9), and 32.4 (IDR: 13.1–178.5) μg/gCr, respectively. Median UIE levels at the time of radioactive iodine administration were not significantly different between groups (p=0.471). The proportion of patients who achieved the appropriate LID status according to our previously reported cut-off value (≤66.2 μg/gCr) was 71.4% in 31–60 days, 72% in 61–90 days, 74.9% in 91–120 days, 73.6% in 121–150 days, and 73% in 151–180 days (p=0.95).
This study showed that UIE achieved by LID after 1 month (30 days) of CT scan using iodinated contrast agents was not higher than that of after 5 months of CT scan in patients who underwent total thyroidectomy for DTC treatment. Current guidelines that recommend the delay of RAIT for 3–4 months after CT scan with iodinated contrast agent should be revisited, and future studies to clarify the acceptable intervals between CT scan and RAIT are warranted.
Medicine (Endocrinology), McGill University, Montreal, QC, Canada
Thyroid Cancer Thursday Poster Clinical
Background lymphocytic thyroiditis (LT) has been reported in 0.5–38% of papillary thyroid cancer (PTC) patients. Several, but not all, reports have shown this association to affect favorably PTC prognosis. The idea is that thyroid follicular cells in LT express both FAS (apoptosis antigen 1) and the FAS ligand, hence triggering FAS-mediated apoptosis resulting in destruction of the thyroid benign and tumor tissue. A lower prevalence of BRAF mutation has also been reported in LT patients with PTC.
We conducted a retrospective review of 475 consecutive PTC patients treated at the McGill University Health Center. Tumor size, vascular or capsular invasion, multifocality, extrathyroidal extension, lymph node metastases, distant metastases, background LT, status of the disease at 6–12-month post-therapy, and survival were recorded.
Background LT was present in 35% of PTC specimen. Background LT was associated with higher percentage of stage I disease and fewer disease persistence. After stratification by age, background LT association with a reduced frequency of disease persistence was present only in patients over 45 years of age. In patients younger than 45 years, the presence of LT was associated with higher rate of extrathyroidal extension, capsular invasion, and multifocality. Disease multifocality in the presence of chronic lymphocytic thyroiditis has been previously reported.
The potential protective effect of LT in PTC seems to be particularly relevant in older patients.
Clinicopathological Parameters of 475 Patients with PTC Stratified by Presence of Background Lymphocytic Thyroiditis
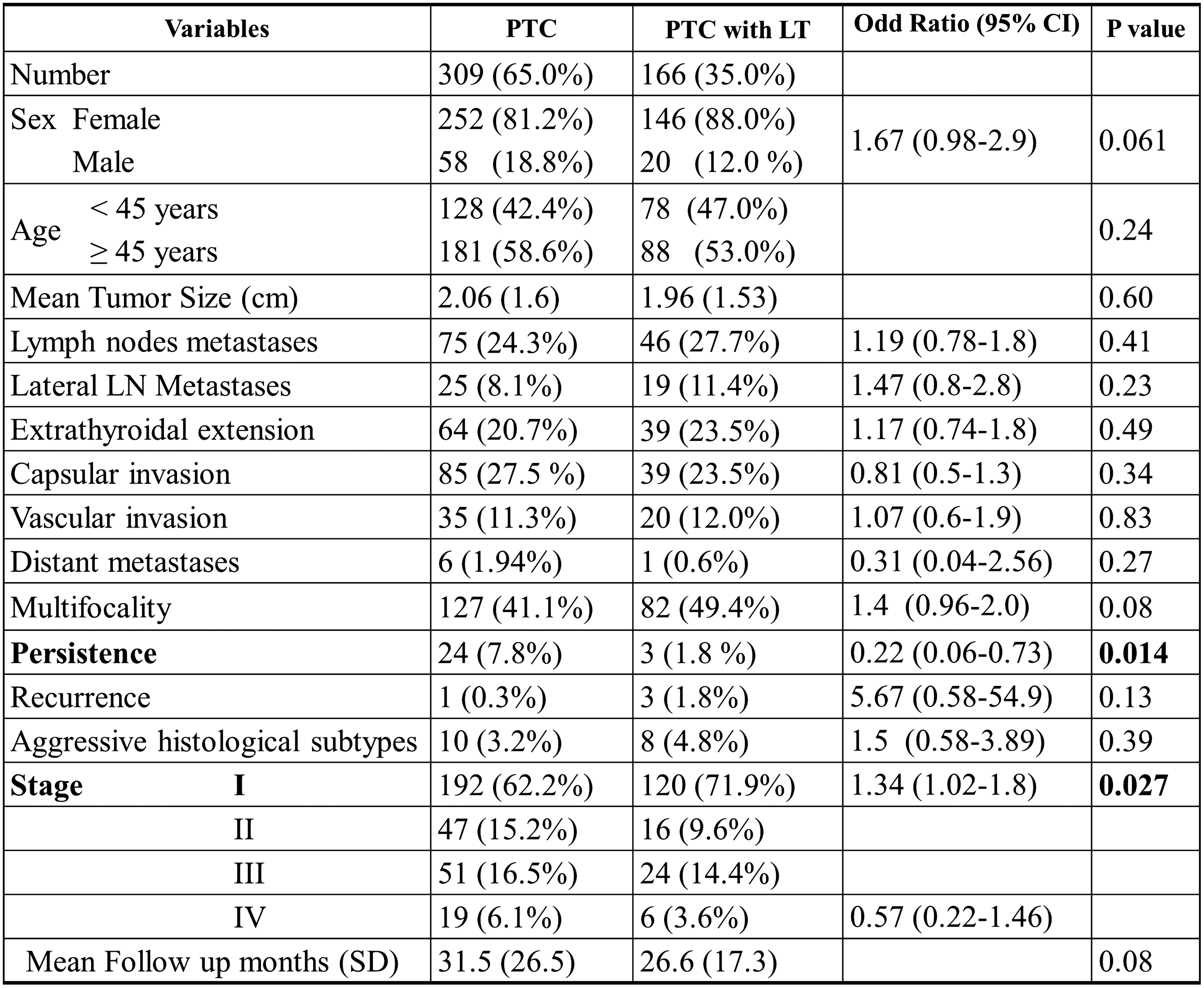
Thyroid Cancer Thursday Poster Clinical
Brain metastases from thyroid carcinoma (TC) are uncommon. Therefore, many questions about brain metastatic TC patients are unsolved. The objective of this study was to analyze the characteristics, prognosis, and management of these patients.
Among the 1460 patients followed in our cancer center for a differentiated TC between 1989–2010, 17 patients with brain metastases were retrospectively studied. The patient's characteristics, the histological findings on initial thyroidectomy specimen according to the UICC 2009 classification, the treatments, and the time to death were reviewed.
There were 10 women and 7 men with a mean age at the diagnosis of brain metastases of 63 years (range, 50–81). Ten patients had an OMS performance status <2 and 7≥2. The primary tumor histology was papillary for 10 cases (6 classic, 3 with follicular variant, and 1 encapsulated), follicular for 4 cases, and poorly differentiated for 3 cases. The pathologic TNM stages were 1 pT0, 2 pT1, 3 pT2, 5 pT3, 2 pT4a, 4 pTx, 7 pN0, 1 pN1a, 3 pN1b, and 6 pNx. Before or at presentation of brain metastases, 12 patients had other distant metastases: 8 lung, 8 bone, and others (1 liver, 1 adrenal gland, and 1 uterine cervix). The average interval between the diagnosis of the primary tumor and the brain metastases was 8.9 years (range, 0–30), and the average interval between the first and the brain metastases was 3 years (range, 0–8.3). The mean number and the mean size of brain metastases were, respectively, 3 (range, 1–10) and 22 mm (range, 3–42 mm). Surgery was performed for 7 patients and radiotherapy (RT) for 14 with 1 stereotactic radiotherapy (SRT), 1 conformal RT limited to the metastasis, and 12 whole-brain radiotherapy (WBRT) with or without boost. The median overall survival after brain metastases was 6.7 months (range, 1–50 months). The overall survival at 1 and 2 years was 41% and 33%. In the 7 long survivors, 6 had a performance status <2; 5 had surgery; and all underwent RT (5 with boost).
Brain metastases from thyroid carcinoma could have an indolent evolution with prolonged survivals. Therefore, optimal treatments (surgery and/or SRT and WBRT) must be proposed to patients with good performance status.
Nuclear Medicine and Endocrine Oncology Service, Institut Gustave Roussy, Villejuif, France
Thyroid Cancer Thursday Poster Clinical
Low muscular mass (MM) has been associated with dose-limiting toxicity in patients with solid tumors treated with chemotherapy and with renal cell carcinoma treated with sorafenib. The aim of this study was to assess the association between body composition, toxicity, and plasma level of vandetanib in patients treated for metastatic or locally advanced medullary thyroid carcinoma.
Thirty-two patients (24 men and 8 women, mean age of 54 years) treated with vandetanib (300 mg/d) were included (ZETA trial). Plasma vandetanib concentration was measured using a reverse-phase high-performance liquid chromatography coupled with tandem-mass spectrometry. Cross-sectional areas (cm2) of visceral adipose tissue (VAT), subcutaneous adipose tissue (SAT), and MM were assessed by computed tomography (CT) imaging at 0, 3, 6, and 12 months of treatment and were indexed for height (cm2/m2). Significant toxicities, defined as requiring a dose reduction or treatment withdrawal, were collected.
A total of 14 patients (44%) [8 men (33%) and 6 women (75%)] had significant toxicity during vandetanib treatment. The most frequent toxicities were asthenia grade 3 (36%), prolongation of the QTc interval (25%), and cutaneous symptoms (11%). In women, no significant relationship was found between body composition, vandetanibemia, and toxicity. In men, a significant lower mean MM (37 vs. 45 cm2/m2; p=0.007) and higher mean vandetanib plasma concentration (1006 vs. 698 ng/mL; p=0.04) were associated with toxicity. When all patients were analyzed together (n=32), patients with significant toxicities had lower mean MM (37 vs. 44 cm2/m2, p=0.003) and a higher mean vandetanib plasma concentration (1091 vs. 739 ng/mL, p=0.03). Furthermore, patients with the highest plasma concentrations (defined as ≥20% of median) had significantly lower MM (37 vs. 45 cm2/m2; p=0.003). Correlations with the body–mass index, VAT, and SAT were not significant in any studied group.
Our study is the first to highlight the importance of body composition and plasma vandetanib concentration assessments while prescribing vandetanib.
Nuclear Medicine and Endocrine Oncology Service, Institut Gustave Roussy, Villejuif, France
Thyroid Cancer Thursday Poster Clinical
Muscle (MT) and adipose tissue (AT) share common intracellular pathways with tumor tissue; thus, it is not surprising to observe metabolic consequences with targeted therapies. The aim of the study was to assess the effects of vandetanib, a tyrosine kinase inhibitor (TKI) that demonstrated efficacy for the treatment of advanced MTC on MT and AT.
Thirty-three patients (25 men and 8 women, mean age of 54 years) with metastatic MTC received vandetanib 300 mg/d (n=23) or placebo (n=10) in the setting of the ZETA study. Cross-sectional areas (cm2) of visceral adipose tissue (VAT), subcutaneous adipose tissue (SAT), and MT were assessed by computed tomography imaging at 3rd lumbar vertebra and were indexed for height (cm2/m2).
At 3 months, compared to baseline, patients treated with vandetanib gained 1.5 kg, 1.3 cm2/m2 of MT, 5.1 cm2/m2 of VAT, and 4.5 cm2/m2 of SAT. In contrast, patients under placebo lost 1.5 kg (p=0.02), 1.0 cm2/m2 of MT (p=0.009), 5.5 cm2/m2 of SAT (p=0.004) and gained significantly less VAT (0.6 cm2/m2) (p=0.02). At 12 months, compared to baseline, patients treated with vandetanib gained 2 kg (NS), lost 0.3 cm2/m2 MT (NS), gained 4.5 cm2/m2 of VAT (95% CI, 0.4 to 8.6) and 9.8 cm2/m2 of SAT (95% CI, 3.4 to 16.1). A significant decrease of calcitonin (defined as ≤50% compared to baseline) was associated with higher weight (p=0.01), VAT (p=0.01), and total adipose tissue (p=0.02).
Beyond its proved efficacy in MTC treatment, and despite common intracellular pathways, vandetanib is the only studied TKI to preserve MT and to restore AT. Further research is needed to explore whether the relationship between changes of VAT and vandetanib treatment results from a direct metabolic effect of vandetanib or is a consequence of biochemical tumor control.
Medicine, Schulich School of Medicine and Dentistry, University of Western Ontario, London, ON, Canada
Thyroid Cancer Thursday Poster Clinical
Thyroid cancer is increasingly diagnosed in North America. Some studies have suggested a higher rate of thyroid cancer in patients with higher insurance rate and higher socioeconomic status (SES). However, it is not known if the stage of thyroid cancer at diagnosis varies with SES. We studied the relation between SES and thyroid cancer stage at presentation in a large thyroid cancer database.
We used data from South-Western Ontario from the Canadian Thyroid Cancer Consortium, a large thyroid cancer registry. We included patients who presented between January 1998 and December 2010 with documented thyroid cancer. We determined thyroid cancer status, sex, and age at presentation, and determined AJCC stage (I, II, III, IV/A, and IV/B or C). Data from the Canadian Census of Population for the years 1996, 2001, and 2006 were used to determine SES based on the individual postal code. A logistic regression model (ordered logit) was used to determine odds ratios of the thyroid cancer stage related to SES, using highest income as denominator.
We included 1563 patients form South-Western Ontario, and were able to assign census data to 1334 cases. Odds ratios (95% confidence intervals) were 1.718 (1.23–2.39) for lowest SES quintile, 2.077 (1.62–2.66) for male sex versus female sex, and 1.010 (1.00–1.02) for age. Time-trend analysis demonstrated an odds ratio of 0.962 (0.93–1.00) compared to the base year.
The pattern in the income quintile estimates clearly indicates that lower average household income is associated with a more advanced stage of thyroid cancer at diagnosis. Advanced age is associated with more advanced stage at diagnosis. Compared to the baseline year, the time-trend analysis indicates that the odds of being diagnosed at a more advanced stage decline by ∼4% per year. Thus, thyroid cancer is being diagnosed earlier over time.
Endocrinology, Complejo Hospitalario de Toledo, Toledo, Spain
Thyroid Cancer Thursday Poster Clinical
Thyroid carcinoma is the most common endocrine malignancy. BRAF V600E point mutation is the most frequent detected genetic change in papillary thyroid carcinomas (PTC). There are some discrepancies regarding its relationship with clinicopathological parameters of poor outcome.
The objective of the study was to investigate the relationship of clinicopathological features of PTC with BRAF mutation.
We analyzed 132 consecutive patients (80.4% female, mean follow-up 41.2±31.5 months, mean age at diagnosis 46.2±15.7 years) with pathological diagnosis of PTC. DNA was extracted from paraffin-embebbed tissue sections, and V600E mutations were detected by HRM, followed by sequencing confirmation. Demographic, clinical, and pathologic characteristics were analyzed. Univariate (Chi-Squared and Student t-test) and multivariate analysis were realized. For statistical processing, we used SPSS version 15.0.
BRAF (V600E) was detected in 49.2% of the study group. The histologic subtype-specific prevalence of mutation was significantly different between BRAF (V600E)-positive and wild-type patients (p<0.05) (see Table). BRAF (V600E) mutation was associated with age (p<0.05), extrathyroidal invasion (p<0.05), and with tumors of greater size or locally invasive (T1+T2 vs. T3) (p<0.05). There were no associations with sex, tumor size, multicentricity, or lymph node metastasis. BRAF (V600E) was negatively associated with the presence of distant metastasis in our group (p<0.05). By multivariate analysis, only age (OR 1.04; CI 95% 1.0–1.1, p<0.05) and extrathyroidal invasion (OR 4.5; CI 95% 1.2–15.5, p<0.05) were independently associated with the presence of BRAF (V600E) mutation.
Subtype-Specific Prevalence of Mutation
Our data confirm that BRAF (V600E) mutation in this European group occurred in less than half PTC population and was associated with some histological subtypes (classical) of PTC and with local invasive growth cancers. This work was supported by the grant PI-2009/16 from Sanitary Research Foundation of Castilla-La Mancha (FISCAM).
Thyroid Cancer Thursday Poster Clinical
Even mild subclinical hyperthyroidism is considered a risk factor for development of osteoporosis. The patients with thyroid carcinomas derived from follicular thyroid cells are routinely given the thyroid hormone supplementation that keeps their TSH suppressed to below the lower limit of the reference range after the treatment with surgery and radioactive iodine is done. This suppression is maintained for years and in some patients indefinitely. This practice has been reported to expose the patients to higher risk for osteoporosis.
We tried to determine if measurements of the 25(OH)-Vitamin D and/or urinary N-telopeptide can identify the individuals at risk for development of osteoporosis while being treated with thyroid hormone supplementation. Our study group was comprised of 92 hypothyroid individuals (84 women and 18 men) who were treated with T4. We excluded 6 individuals who were receiving antiresorptive therapy at the time or 1 year before the study. We examined the correlation of TSH, free-T4, and 25(OH)-Vitamin D levels with urinary N-telopeptide levels in an attempt to determine which of these parameters should be further studied as a risk factor or development of osteoporosis.
Results failed to show a meaningful correlation between the parameters in the whole group or when analyzed only for women or only for patients who have diagnosis of thyroid carcinoma. The coefficients of correlation between TSH and N-telopeptide ranged −0.075 to −0.087, free T4 and N-telopeptide 0.24 to 0.25, while Vitamin D and N-telopeptide showed correlation of 0.012 to 0.04 in different groups.
We conclude that the TSH, free-T4, or Vitamin D levels are not useful as predictors of the risk for osteoporosis, and recommend that all of these individuals undergo bone mineral density measurements if the TSH suppression is to be extended beyond the three years after the initial treatment for thyroid carcinoma.
DOES OBESITY INCREASE THE RISK OF THYROID CANCER?
Thyroid Cancer Thursday Poster Clinical
In theory, obesity increases the risk of differentiated thyroid cancer (DTC). Increased leptin in obese patients increases TSH. Increased TSH increases thyroid volume. Obese patients have increased circulating levels of cytokines causing vasodilatation and increase thyroid hypoechogenicity. DTC risk is higher in hypoechogenic thyroid nodules. We hypothesized that obese patients are at an increased risk of DTC.
We did a retrospective chart review of 450 post-thyroidectomy patients at the Ochsner Clinic Foundation between 2009 and 2011. Patients with family history of thyroid cancer, radiation to head and neck, and nonthyroidal cancers were excluded. We obtained data on age, sex, body–mass index (BMI), thyroid peroxidase antibody (TPO), thyroglobulin antibody, type, and stage of cancer and fine-needle aspiration pathology. The relationship between cancer and BMI was assessed by Chi-squared t-tests and bivariate logistic regression.
After applying exclusion criteria, 369 patients were included. Mean age was 57 years, and the body–mass index (BMI) was 32 kg/m2, respectively. Patients were classified into 4 groups based on BMI (≤25, 26–30, 31–39, and ≥40). A significant relationship was found between thyroid cancer and patients with BMI≥40 (p=0.031). Patients with BMI>40 had lesser risk of thyroid cancer (OR=0.41; 95% CI: 0.18, 0.93). We also found a significant relationship between fine-needle aspiration (FNA) and BMI, in which patients with BMI≥40 are 73% less likely of abnormal FNA (OR=0.27; 95% CI:0.12, 0.62). In addition, patients with abnormal FNA were 3.14 times more likely to develop cancer than patients with normal FNA (95% CI: 1.9, 4.9).
In our institution, abnormal FNA results correlated pretty well with thyroid cancer rate. Patients with BMI>40 had thyroidectomies for reasons other than abnormal FNA explaining the low rate of thyroid cancer in this group. In our study, the relationship between obesity and thyroid cancer is not well established. Few limitations of our study include a high mean BMI and selection of only post-thyroidectomy patients for the study. Further studies are needed to determine the relationship between thyroid cancer and obesity.
Percent of Post-Thyroidectomy Patients with Thyroid Cancer of Abnormal FNA
Thyroid Cancer Thursday Poster Clinical
Primary thyroid lymphoma (PTL) is rare, constituting <5% of all thyroid malignancies. Diagnosis of PTL is challenging, and treatment of PTL depends on clinical features, stage, and histopathology of lymphoma.
A 79-year-old woman with history of IgM-kappa monoclonal gammopathy of undetermined significance and nontoxic multinodular goiter presented with rapid progression of goiter, compressive symptoms, and a 23-pound weight loss in 3 weeks. Patient denied symptoms of hypothyroidism, fever, and night sweats. On examination, patient had a firm, fixed goiter that moved with deglutition and positive Pemberton's sign. Lab tests showed TSH of 6.025 μIU/mL (reference range, 0.4–4), FT4 of 0.99 ng/dL (0.71–1.51), absent TPO antibody, normal LDH, and elevated uric acid. Thyroid ultrasound showed a large goiter and 4 heterogeneous nodules with largest nodule measuring 3.4×2.6×2.4 cm. CT scan of neck showed a mass effect with tracheal deviation to the left. FNA of thyroid nodules showed follicular epithelial cells with moderate nuclear atypia, numerous lymphocytes, and poorly preserved lymphoid component. A week after initial presentation, patient developed hoarseness of voice and right-vocal-cord palsy. Patient underwent emergency partial right thyroid lobectomy, isthmusectomy, and tracheostomy. Pathology showed diffuse large B-cell lymphoma (DLBCL) with germinal center origin. Patient is currently receiving R-CHOP chemotherapy and is tolerating it well.
Our patient with stage-1 DLBCL was a unique case of PTL occurring in the setting of nonautoimmune thyroid disease. FNA of thyroid is often nondiagnostic in PTL; large-bore needle or excisional biopsy may be required. PTL is very chemosensitive, and primary treatment involves combination chemotherapy with Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) and radiation therapy.
Surgical resection should be considered in PTL patients with rapid progression of compressive symptoms presenting as a life-threatening emergency.
Diffuse large B-cell lymphoma (DLBCL) with germinal origin.
Thyroid Cancer Thursday Poster Clinical
Fine-needle aspiration (FNA) is the optimal diagnostic test for evaluating thyroid nodules for malignancy. Ultrasound-guided FNA (USGFNA) is more commonly performed and is more resource intensive compared to palpation-guided FNA (PGFNA). The purpose of this study was to compare inadequacy rates of PGFNA versus USGFNA of thyroid nodules.
A retrospective review of clinical data and cytology reports of thyroid FNA biopsy specimens from three hospitals between 2006 and 2010 was conducted. Specimens were included if the nodule size was ≥1.5 cm, and thus likely palpable. The FNA was determined to be PGFNA or USGFNA based on accompanying radiology or clinic notes.
Of the 247 patients included, 55 had PGFNA, and 192 had USGFNA. Inadequacy rates were 34.55% in the PGFNA group and 41.15% in the UGFNA group, which were not significantly different (p=0.3777). Logistic regression was used to obtain adjusted odds ratios for nodule size and consistency. Although there were no significant differences, there was a trend toward a higher likelihood of an inadequate sample if the nodule was not solid (i.e., mixed or cystic), and if the USGFNA-versus-PGFNA technique was used.
There was no significant difference found in inadequacy rates between USGFNA and PGFNA in thyroid nodules >1.5 cm. Thus, the PGFNA technique should be encouraged in the clinic setting for palpable nodules, given the benefits it holds of lower cost and patient convenience.
MALIGNANT HOT THYROID NODULE
Thyroid Cancer Thursday Poster Clinical
Hot thyroid nodules are usually benign with 1% rate of malignancy. Because of low cancer incidence and chance of false positivity, biopsy is not recommended. However, multiple cases of malignant hot thyroid nodule have been reported in literature.
A 55-year-old man was found with hyperthyroidism after presenting with chest pain and insomnia. Thyroid functions revealed TSH 0.01 (0.35–5.5 μIU/mL), FT4 2.4 (0.8–1.8 ng/dL), FT3 634 (320–420 pg/dL), and thyroid-stimulating immunoglobulin 160 (≤125%). He was noted to have an enlarged and irregular thyroid with 3-cm R-sided mass. He had fine tremor on outstretched hands and warm clammy palms. His family history was positive for thyroid cancer in his twin brother. As indicated, thyroid US was done and showed hypoechoic R thyroid nodule measuring 1.2×1×1 cm and hyperechoic L nodule measuring 1.9×1.7×1.4 cm with increased vascularity. There were no abnormal calcifications. 123I scan was notable for increased 24-h uptake of 38% with heterogeneous distribution suggestive of Graves' disease. There was an area of photopenia on the left and increased uptake on the right corresponding to nodules on US. The patient was started on methimazole for hyperthyroidism. Fine-needle aspiration of L-sided nodule was performed and showed follicular neoplasm. The patient then underwent total thyroidectomy with final histology showing L-sided Hurthle cell follicular adenoma, incidental R-sided 9-mm papillary thyroid carcinoma inside of reported R-sided hot nodule, and additional 3-focus 8, 3, and 3 mm of papillary thyroid cancer.
We are presenting a patient with malignant hot thyroid nodule on the background of Graves' disease and positive family history for thyroid cancer.
American Thyroid Association guidelines suggest not to biopsy hot thyroid nodule. Therefore, cancer diagnosis could be missed. We propose an individualized approach to patients with hot thyroid nodule to evaluate for potential biopsy based on risk factors, i.e., concomitant Graves' disease, family history of thyroid cancer, h/o head, and neck irradiation or suspicious US features.
PAPILARY THYROID CARCINOMA PRESENTING AS A SUPRACLAVICULAR MASS WITH THE INICIAL DIAGNOSIS OF ECTOPIC THYROID
Thyroid Cancer Thursday Poster Clinical
Ectopic thyroid is a rare condition that is usually located in the base of the tongue. Its estimated prevalence is about one case of 200,000 people. It is more common in women, young adults, and in Asians population, and it's mostly asymptomatic. Some theories try to explain this rare anomaly, such as failure in the descent of the gland and the presence of thyroid tissue in cervical lymph node capsules. The differential diagnosis of ectopic thyroid is mainly metastatic differentiated thyroid carcinoma, and the cytological finding might be expected to be atypical features in the presence of thyroid carcinoma.
Case Report: A 45-year-old man presented with a lump in the anterior cervical region and the right supraclavicular region. Ultrasonography (US) showed a solid nodule of 1.1 cm in the left lobe (LL) of the thyroid, a solid nodule of 1.1 cm in the right lobe (RL) of the thyroid, and a solid nodule of 2.8×2.2 cm with the texture of the thyroid in the right supraclavicular region. Fine-needle aspiration (FNA) showed atypical follicular cells suggested of follicular neoplasm in the thyroid nodule, but not in the extrathyroid lesion. A second FNA continues to show no atypical features in the ectopic lesion. Neck exploration confirmed the presence of unifocal intrathyroid papillary carcinoma. Supraclavicular lesion confirmed to be metastatic foci, which was also presented in 3 resected lymph nodes.
This case illustrates an unusual presentation of metastatic papillary thyroid carcinoma. Sometimes, these neoplastic tissue are so well differentiated that can resemble normal thyroid in cytology, a pitfall that should always be remembered during evaluation of an ectopic thyroid tissue in an adult one.
TOMOGRAPHY DOUBLE LOCATION OF ECTOPIC THYROID DISPLAYED TO HIGH-RESOLUTION COMPUTED TOMOGRAPHY
Thyroid Nodules & Goiter Thursday Poster Clinical
Ectopic thyroid is a rare abnormality involving errors in the embryogenesis of the thyroid during its passage to its final pretracheal position, and it can coexist with a normal gland. It occurs more commonly in women, young adults, and Asian people, and the majority of patients are asymptomatic. The most frequent location (90% of cases) is in the base of tongue, in particular at the foramen cecum. The presence of two simultaneous ectopic lesions is even more unusual. The iodine scintigraphy is the method of choice for detecting ectopic thyroid tissue, and imaging studies such as computed tomography (CT), magnetic resonance imaging, and Doppler ultrasonography (US) can help determine the extent of the disease. Cytology obtained by fine-needle aspiration (FNA) confirms the diagnosis, and is capable to detect malignant lesions, which are described in <1% of cases.
CASE REPORT: A 54-year-old woman underwent, two years ago, total thyroidectomy (removal of both lobes and isthmus), which revealed no malignancy. Neck US described a nodule below thyroid right lobe (right parathyroid) measuring 0.8×0.7 cm. Blood tests showed PTH: 65; calcium: 9.1; albumin: 4.5; 25(OH)-D: 41. Due to the elevation of PTH, Sestamibi scintigraphy was requested and showed early uptake in the right lower parathyroid region and in the region of the sternal notch. This result was incompatible with the presence of parathyroid tissue, whose capture would be expected at the late phase. Cervical CT showed two nodules (0.7×0.7 cm below the right lobe and 1.8 cm in sternal notch). FNA revealed follicular cells in both lesions, and PTH dosing in the aspirate was 22pg/mL, compatible with the diagnosis of ectopic thyroid. Scintigraphy with 131I showed uptake in both lesions.
This case demonstrates a rare presentation of cervical nodules.
Endocrinology, General Hospital Chieti, Chieti, Italy
Thyroid Cancer Thursday Poster Clinical
The evolutionary behavior of differentiated thyroid carcinoma (DTC) seems to correlate with the morphological appearance on the one hand, but above all, in relation with the tumor capsule infiltration (Evans HL). In fact, in the papillary thyroid carcinoma, capsular invasion without the overcoming of this is related to a good prognosis, while the presence of capsular invasion in encapsulated follicular carcinoma is associated to a bad prognosis (Evans HL).
We reported our observations about our surgical series related to the pathology of EPTC, starting from a description of a case of a young woman.
We have observed a 25-year-old woman who discovered a thyroid nodule of 13-mm diameter in 2003. It increased along the scale of 8 years till 40-mm diameter. At the beginning of 2012, it was decided a surgical resection of the nodule. Histological features showed encapsulated papillary carcinoma. Enlarged lymph nodes were not observed nor alterations in the remaining thyroid parenchima. Therefore, it was decided not to reoperate In a subsequent intervention casistic of 150 thyroidectomy, the percentage of thyroid carcinomas was 14%, and 4 (20%) were encapsulated papillary carcinomas, with a diameter ranging between 30 and 40 mm, and in all our behavior was conservative surgery (hemithyroidectomy). In any case, we were sure about the integrity of the lymphonodes and the remaining lobe with previous and intraoperative ultrasonography, with the probe adhering and in contact with the lobe.
In our series, we followed the Evans and Rosai criteria to classify DTC; consequently, in EPC, we suggest a conservative surgery considering a new technique of intraoperative ultrasonography that ensures the integrity of the remaining thyroid tissue. Finally, with regard to the EPC, likewise follicular neoplasm classification, it could be proposed the definition of papillary adenoma instead papillary carcinoma when it is encapsulated, reserving the definition of PTC only to those that exceed the capsule.
Hematology/Medical Oncology, Emory University, Atlanta, GA
Thyroid Cancer Thursday Poster Translational
Thyroid cancer is the most common endocrine cancer worldwide with increasing number of patients with incurable metastatic disease. Newer treatment approaches are warranted to improve clinical outcome. We evaluated the efficacy of everolimus, an mTOR inhibitor, and pasireotide (SOM230), a somatostatin analog, using preclinical tumor xenograft. We also report the preliminary result of an ongoing phase II clinical trial of everolimus and pasireotide in thyroid cancer.
In vivo efficacy of everolimus and pasireotide was tested in a xenograft model of thyroid cancer using BCPAP and TPC-1 cell lines. Tumor-bearing mice were treated with vehicle, everolimus (oral), or pasireotide LAR (subcut). Tumor growth inhibition was assessed after 28 days on treatment. In a phase II clinical trial, subjects≥18 years, ECOG PS 0–2, with radiorefractory differentiated or medullary thyroid cancer, adequate organ function, were enrolled and randomized to receive pasireotide LAR (60 mg once every 4 weeks), everolimus (10 mg once daily continuously), or the combination. Using a Simon's 2-stage design, each arm will enroll 28 patients to assess the response rate of P0=5% vs. P1=15%, power=80%, and α=0.05. Patients were treated until disease progression by the RECIST criteria as assessed once every 2 cycles (cycle=28 days) or with development of intolerable toxicity.
Everolimus and pasireotide displayed potent inhibition of TPC1 and BCPAP thyroid cancer xenograft growth in vivo without inducing significant toxicity. This result has been successfully translated into a phase II efficacy clinical study in advanced thyroid cancer (NCT01270321) that has enrolled 13 patients to date: M/F (6/7); histology: medullary (4), differentiated (9). Eight patients achieved a best response on treatment of stable disease, 3 with progression, and 2 still indeterminate. Median duration on therapy was 168 days (range: 14–539 days). Salient adverse events include fatigue, anemia, stomatitis, elevated glucose, cholesterol, and triglyceride.
Everolimus and pasireotide showed efficacy in a preclinical model with successful translation into early clinical testing. These agents may provide additional therapeutic options for thyroid cancer patients in the future.
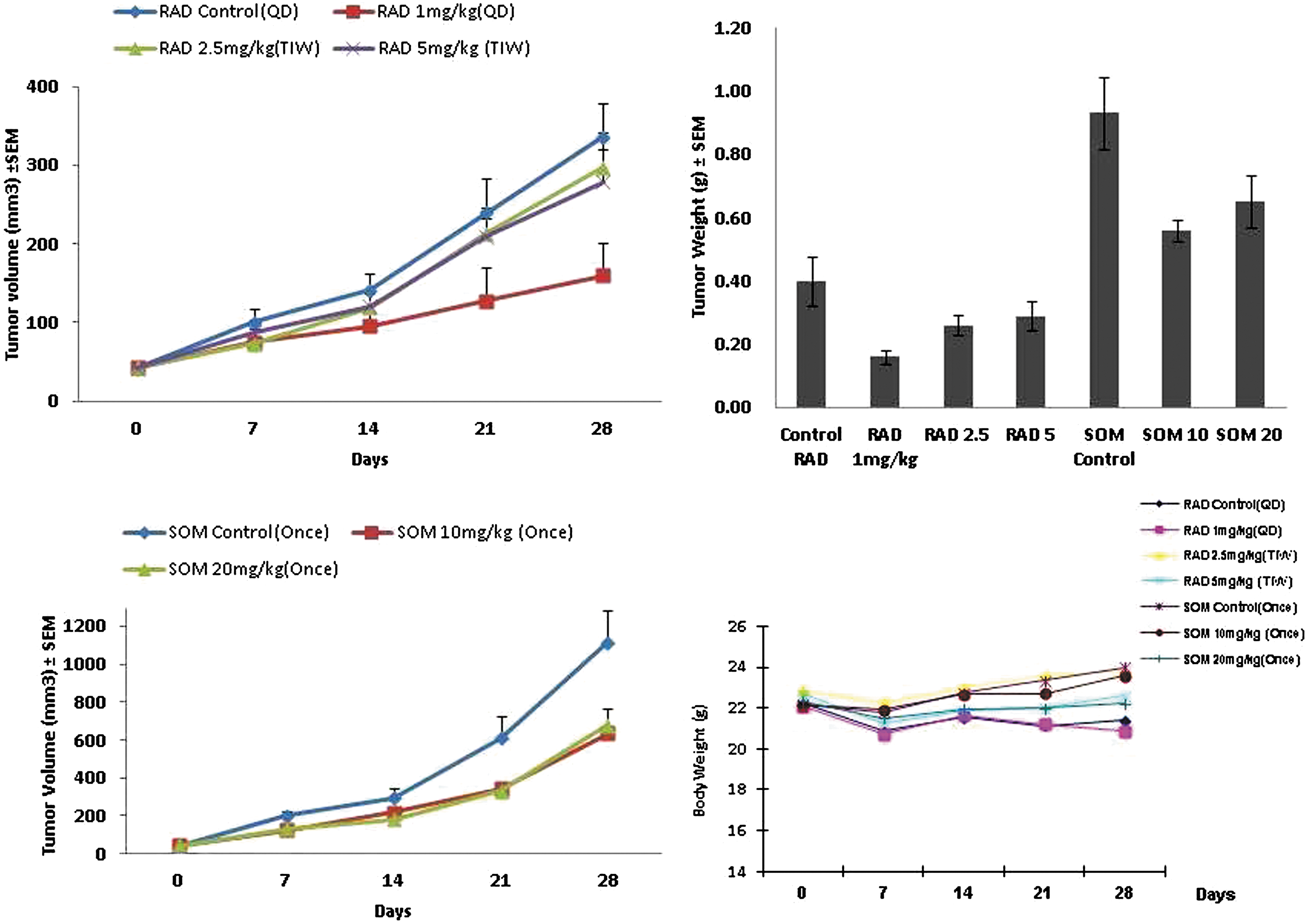
Tumor growth curves in tumor-bearing mice treated with everolimus/vehicle (top left); pasireotide/vehicle (lower left); animal weight during treatment with vehicle, everolimus, or pasireotide (lower right); harvested tumor weights at the end of treatment (upper right).
Thyroid Cancer Thursday Poster Clinical
Phase II studies of small-molecule kinase inhibitors demonstrated the efficacy of targeted biologic agents as frontline systemic therapy in patients with radioiodine refractory and medullary thyroid cancer. Whether thyroid cancer patients benefit from salvage therapy with another kinase inhibitor following progression on frontline therapy is not yet established. This retrospective study assessed the efficacy of targeted biologic agents as second-line therapy for advanced thyroid cancer patients.
We retrieved records of patients with advanced radioiodine refractory and medullary thyroid cancer treated in the Medical Oncology Clinic at our institution from 2007 to 2012. Salient clinical data, including date of diagnosis, type of biologic agent, treatment duration, and survival outcomes, were analyzed for efficacy endpoints of time to treatment failure (TTF), progression free survival (PFS), and overall survival (OS). The clinical outcome with first- and second-line kinase inhibitor therapy as well as differences in TTF and PFS based on gender and histologic subtypes were also compared. Survival curves were generated by the Kaplan–Meier method; differences in survival were assessed using log-rank test, and a p-value<0.05 was considered significant.
We identified 26 patients out of 61 patient referrals (42.6%) treated with biologic agents; median age: 55 years. Clinical variables included gender: M/F (16/10); and histology: medullary (9), nonmedullary (17). The clinical efficacy of second-line targeted biologic agents was inferior to first-line treatment in terms of TTF (median 4.6 vs. 10.6 months, p-value=0.0526) and PFS (median 4.6 vs. 14.4 months, p-value=0.0100). Male patients had better outcomes with frontline (median PFS: 19 vs. 9 months, p-value=0.0072) and postfrontline treatment (median PFS 6 vs. 3 months, p-value=0.028). There were no significant efficacy differences based on histologic tumor types.
Thyroid cancer patients derived clinical benefits from salvage second-line therapy with targeted biologic agents. The magnitude of benefit is smaller than observed with frontline use of these agents. Gender may predict the benefit of second-line treatment with biologic agents.
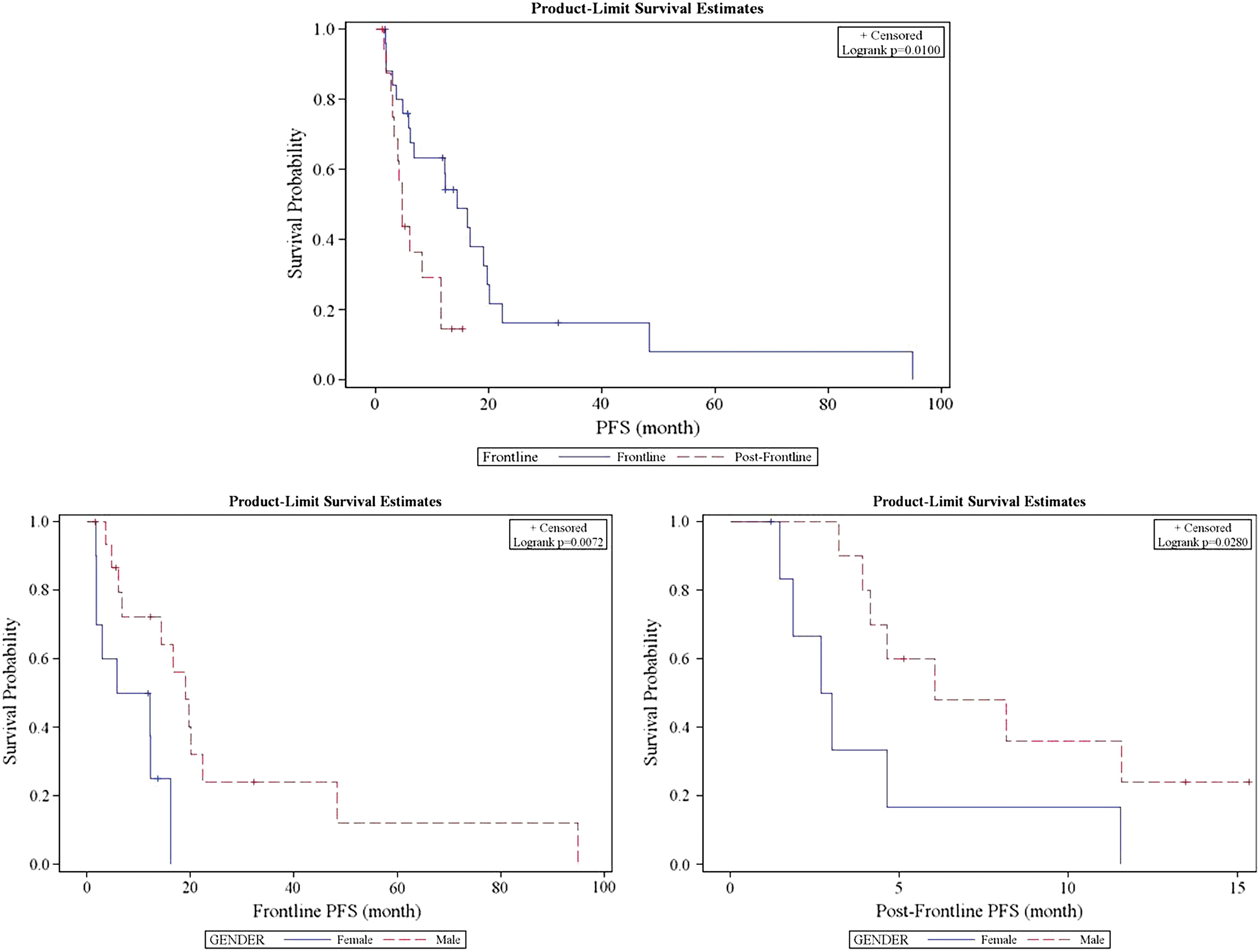
Top: Kaplan–Meier survival curves for PFS in patients treated with biologic agents as frontline versus postfrontline therapy. Bottom Left: differences in PFS based on gender with frontline therapy. Bottom Right: differences in PFS based on gender with postfrontline therapy.
Thyroid Development Thursday Poster Clinical
Congenital hypothyroidism (CH) is a relatively common disorder occurring in about 1 in 1,700 live births. In the years 2000–2010, there were 1.43 million births in five New England states (MA, ME, NH, RI, and VT). Multiple births (58,378) accounted for almost 4% of these newborns. CH was diagnosed in 921 newborns. Congenital hypothyroidism was present in six pairs of twins; however, diagnosis of permanent hypothyroidism was problematic in one or both of each pair because of prematurity with either relatively low concentrations of thyroid-stimulating hormone or late onset of laboratory abnormalities. We now report the first presentation of congenital hypothyroidism caused by thyroid dysgenesis in a pair of dizygotic twins.
Diamniotic dichorionic twin males were born at 37-week gestation, after in vitro fertilization, by cesarean section to a 39-year-old healthy mother. Twin A weighed 2243 grams and twin B 2571 grams. Newborn screening on the third day of life in both twins demonstrated TSH>500 mIU/mL. Thyroxine (T4) concentrations of twins A and B were 4.4 and 5.4 μg/dL respectively. Both were started on liquid levothyroxine 0.025 mg/day.
We first saw the twins on day 14 of life. There were no symptoms or signs of congenital hypothyroidism in either one of the twins. Biochemical studies for twin A demonstrated TSH>500, T4 7.7, and for twin B, TSH 181, T4 9.8. Both twins had Technetium 99m scintography. There was no tracer uptake in the normal thyroid bed in either one. However, in both, tracer uptake was located in identical positions in the sublingual area. Both patients were given higher doses of levothyroxine tablet 0.05 mg/day for a week before titrating the dose down to 0.0375 mg/day. At four weeks of life, laboratory studies for twin A showed TSH 1.42, T4 12.3, and for twin B, TSH 2.63, T4 12.6. At 6 months of life, they are growing along growth curves and meeting developmental milestones.
To our knowledge, this is the first report of permanent congenital hypothyroidism in a pair of dizygotic twins. The rarity of concordance for CH in twins suggests that this disorder does not have a clear genetic cause and may be the result of one or more epigenetic phenomena.
Genetic and Molecular and Cellular Physiology Center_ CNRS 5534 UMR, Lyon 1 University, Villeurbanne, France
Thyroid Hormone Action Thursday Poster Basic
It has been previously demonstrated that specific TRa1 overexpression in murine intestinal epithelium accelerates tumorigenesis in the background of the constitutively activated WNT pathway. The objective was to elucidate which molecular programs are specifically affected by TRa1 during intestinal tumorigenesis.
Samples were collected from i) wild-type mice intestine (WT), ii) tumoral lesions of APC+/1638N mice with a constitutively activated WNT pathway (AT), and iii) tumoral lesions of APC+/1638N mice overexpressing TRa1 in intestinal epithelium vil-TRa1/Apc+/1638N (TRAT). Transcriptomic analyses were performed using Mouse GE 4x44Kv2 Microarray (Agilent) to identify genes associated with the tumorigenic AT_WT sequence and those associated with the tumorigenic TRAT_WT sequence. The in vivo biological effects of TRa1 overexpression were further bioinformatically examined by applying the Ingenuity® Pathway Analysis (IPA) and Gene Set Enrichment Analysis (GSEA).
The most significant functions specifically associated with the TRAT_WT sequence, as compared to the AT_WT sequence, were organogenesis, morphogenesis, and tissue development, in particular in the gastrointestinal tract. Expectedly affected in the AT_WT sequence, the WNT pathway was significantly further affected in the TRAT_WT sequence. TRAT-specific alterations of the WNT pathway included multiple regulations of WNT activators and inhibitors. HNF4A target genes were found as specifically altered in the TRAT_WT sequence (stimulation vs. inhibition in AT_WT sequence). Additionally, significant over-representation of genes in the NOTCH pathway was disclosed in the TRAT_WT sequence by GSEA.
Specific functions and pathways are impacted by TRa1 overexpression during intestinal tumorigenesis. They include gastrointestinal development, a function strongly reminiscent of the well-known role played by TRa1 during intestinal organogenesis and histogenesis. The WNT pathway is specifically altered by TRa1 as well as other pathways involved in colorectal carcinogenesis, such as HNF4A and NOTCH.
T2 PARTICIPATES IN GROWTH THROUGH A DIFFERENT TRβ1 ISOFORM IN TILAPIA
Thyroid Hormone Action Thursday Poster Basic
Considered the biologically active thyroid hormone (TH), T3 actions involve TH-dependent de novo gene transcription and are mediated by TH nuclear receptors (TR). We have recently shown that 3,5-T2 (T2) is also bioactive at least in teleosts. The effects of T2 appear to be mediated by a different isoform of TRβ1 that contains a 9-amino-acid insert in its ligand-binding domain, and which we have denominated long TRβ1 (L-TRβ1).
We used body growth as a physiological model to analyze T2 bioactivity, as well as the regulation of its signaling pathway. To this end, we treated tilapia fingerlings by immersion with 1 nM of T3, T2, or the inactive isomer rT3. A negative control group was treated with methimazole (MMI). All experimental groups were treated for 8 hours, three times a week for one month. We recorded growth gain and measured the expression of GH, IGF-1, S-TRβ1 (short TRβ1), and L-TRβ1. To further evaluate the independent effect of each TH, we induced a partial blockade of TH with MMI and simultaneously supplemented with 1 nM of T3 or T2 under the above-described administration protocol.
Growth gain of fish exposed to T3 or T2 was significantly higher than that of the control group, whereas growth of tilapia exposed to rT3 was similar to control fish. Tilapia treated with MMI showed the lowest growth rate. Intrahepatic expression of GH and IGF-1 was upregulated by T2 and T3, whereas the expression L-TRβ1 increased only in the T2-treated fish, and S-TRβ1 was upregulated only by T3. MMI+T3 and MMI+T2 treatments significantly decreased intrahepatic T3 concentrations; however, MMI+T3 treatment stimulated growth, whereas that with MMI+T2 maintained growth similar to the control group. MMI+T3-treated tilapia showed a euthyroidal GH expression, whereas fish treated with MMI+T2 exhibited a significant increase in the expression of this gene. Both, MMI+T3 and MMI+T2 groups maintained the expression of IGF-1 euthyroid. L-TRβ1 and S-TRβ1 expression was upregulated in fish treated with MMI+T2 and MMI+T3, respectively.
All together, our results support the notion that T3 and T2 participate in the growth process; however, their effects are differently mediated by specific TRβ1 isoforms (CONACYT 080420 and PAPIIT IN203409).
AN UNUSUAL CASE OF THYROID STORM IN A PATIENT POST-THYROIDECTOMY
Thyroid Hormone Action Thursday Poster Clinical
A 36-year-old woman with history of Graves' status post-thyroidectomy in 2007, with postsurgical hypothyroidism on Levothyroxine presented after an attempted suicide. The patient had slit both her wrists when she presented to the ER. She was complaining of palpitations, heat intolerance, and worsening tremors. She reports nausea and vomiting, but no diarrhea, anxiety, or insomnia. She was febrile on presentation with Tmax of 101 degrees, and sinus tachycardia with a maximum pulse of 140 bpm. She reports taking 300 μg of Levothyroxine for the past month. Previously, she had been on 150 μg of Levothyroxine, but reports her dose was increased secondary to abnormal TFTs. When she presented to the Endocrine clinic, TSH was 0.03, and FT4 was 2.42. She was advised to discontinue her Levothyroxine and follow-up the next week to be reassessed; however, the patient developed worsening symptoms for which she went to the ER.
In the ER, her TSH was undetectable; FT4 was >8.0 ng/dL, and FT3 was 11.7 pg/mL. Per the Burch and Wartofsky diagnostic criteria for thyroid storm, the patient had a score >60. She was admitted to the ICU for thyroid storm secondary to Levothyroxine over replacement.
The patient was started on PTU to block the T4-to-T3 conversion, as well as propranolol and dexamethasone. The patient would not admit to excessive ingestion of exogenous thyroid hormone, and was evaluated by psychiatry for depression. By discharge, her symptoms had significantly improved, and her steroids and PTU were tapered off. Her repeat FT4 was 1.79 ng/dL, and the patient was started on Levothyroxine 100 μg daily.
The incidence of thyroid storm among hospitalized patients is <10%. It is important for the physician to be vigilant in diagnosing thyroid storm as it carries significant morbidity and mortality. There has been a case previously described of thyroid storm due to thyrotoxicosis factitia; however, not many cases are reported in the literature. One should suspect over replacement with exogenous thyroid hormone in a patient with a history of thyroidectomy on replacement therapy, underlying mental health issues, and a rising FT4 level despite recommendations to discontinue the medication.
Medicine, Imperial College London, London, United Kingdom
Thyroid Hormone Metabolism & Regulation Thursday Poster Basic
Thyroid hormones control chondrocyte differentiation. The type 1 and 2 deiodinases (D1 and D2) convert T4 to T3 by 5′-deiodination, whereas the type 3 deiodinase (D3) irreversibly inactivates T4 and T3. The activities of D2 and D3 in target tissues determine local intracellular T3 availability. Osteoarthritis is characterized by accelerated articular chondrocyte differentiation and cartilage destruction. Recently, genome-wide association studies have identified D2 and D3 as susceptibility loci for osteoarthritis. Thus, we investigated osteoarthritis susceptibility in mice lacking 5′-deiodinase activity.
Knee joints from 16-week-old adult male D2KO, D1D2KO, and wild-type (WT) mice were analyzed. Five-micrometer coronal and sagittal sections at 80-μm intervals were stained with Safranin-O Fast-Green and scored using the Osteoarthritis Research Society International grading scale of 0 to 6 (0=normal articular cartilage and 6=clefts or erosions extending to the mineralizing front and covering>75% of the articular cartilage). Maximum and standardized osteoarthritis scores were determined.
A maximum osteoarthritis score of 2 was recorded in D2KO, D1D2KO, and WT mice (Kruskal–Wallis, ns, n=3–5). A score of 2 indicates loss of articular cartilage surface lamina and the presence of superficial clefts. Median standardized osteoarthritis scores did not differ among genotypes [WT 7.84 (0–13.5); D2KO 2.07 (0–12.8); D1D2KO 8.26 (0–15.2); median (range) total osteoarthritis score/articular surface, Kruskal–Wallis, ns, n=3–5].
Deletion of D2 or both D1 and D2 did not affect susceptibility to the development of spontaneous osteoarthritis in adult mice. Further investigation of the role of local T3 availability in osteoarthritis will require the use of provocation models in which osteoarthritis is induced, for example, by surgical destabilization of the knee.
SONIC HEDGEHOG DEPENDENCE OF THE UBIQUITINATION OF TYPE 2 DEIODINASE IS CONTROLLED BY UBIQUITIN LIGASE USAGE
Thyroid Hormone Metabolism & Regulation Thursday Poster Basic
Type 2 deiodinase (D2) is the key enzyme that catalyzes thyroid hormone (TH) activation. D2 undergoes substrate-accelerated ubiquitination along the ERAD pathway. This mechanism ensures rapid and fine-tuned regulation of TH levels in the brain and other tissues. D2 ubiquitination is driven by WSB-1 and Teb4 E3 ubiquitin ligases, allowing the conjugation of ubiquitin chain to the D2 protein. These E3 ligases are coexpressed with D2 in tanycytes, in specialized glial cells located in the floor and wall of the third ventricle forming the T3-generating center of the mediobasal hypothalamus. Using fluorescence resonance energy transfer (FRET), we have previously shown that the Teb4-D2 interaction occurs between the RING domain-containing N-terminus of Teb4 and the cytosolic C-terminus of D2 in living HEK-293 cells. In the present study, we aimed to understand molecular mechanisms underlying D2 ubiquitination in D2/WSB-1/Teb4-coexpressing cells.
We used Dual Luciferase promoter assay and set up a 3-FRET system based on D2-YFP/CFP-Teb4/WSB1-mCherry fusion proteins.
First, we used promoter assay to study the regulation of the two E3 ligases along the Sonic hedgehog (Shh) pathway, known to accelerate WSB-1-mediated D2 degradation. We have cloned and characterized the ∼3.5-kb 5′-flanking region (5′FR) of the human Teb4 (hTEb4) gene. The hTeb4 has a GC-rich promoter without TATA box and removal of Sp1 sites ∼-130 bp decreased its basal promoter activity ∼50%. The hTeb4 5′FR did not respond to Shh effector transcription factor Gli2 in HeLa cells, while the ∼3-kb WSB-1 5′FR-positive control was readily induced. Then, we moved to 3-FRET that allowed the parallel detection of interactions between D2/WSB-1/Teb4 in living HEK-293 cells. We tested the T4 sensitivity of D2 ubiquitination in the presence of both ligases and found that WSB-1 and Teb4 contribute equally to substrate-mediated ubiquitination of D2.
We conclude that unlike substrate-mediated regulation, responsiveness to Shh signaling is E3 specific during D2 ubiquitination. The distinct regulation of WSB1 and Teb4 by Shh could contribute to the complex regulation of T3 generation in hypothalamic tanycytes and might underlay self-renewal of this cell type.
WHAT IS THE RISK OF MALIGNANCY OF A THYROID NODULE WITH SUSPICIOUS SONOGRAPHIC FEATURES?
Thyroid Cancer Thursday Poster Clinical
Ultrasound remains the study of choice for evaluation of thyroid nodules. Some have noted that sonographic features such as calcification, hypervascularity, hypoechogenicity, uninodularity, large size, and nodule growth are associated with malignancy. In this study, we sought to determine the relative risk of malignancy in a thyroid nodule with suspicious sonographic features using univariate and multivariate analysis.
We queried our thyroid tumor registry dating 2003–2011 for patients with at least one thyroid ultrasound who progressed to biopsy or surgery and identified 530 patients. We analyzed the demographic characteristics and sonographic features, including calcification, hypervascularity, hypoechogenicity, uninodularity, nodule size >4 cm, and nodule growth of 5 mm on subsequent ultrasound, to the final surgical pathology or to fine-needle aspiration (FNA) in those patients that did not progress to surgery. We used univariate analysis to identify variables that were significant predictors of cancer (p<0.1). We then used multivariate logistic regression models with those variables to predict thyroid cancer.
Of all 530 patients, 352 progressed to surgery, while 172 had only FNA. Of the 530 patients, 132 (24.9%) had a diagnosis of malignancy on final pathology, and 398 (75.1%) had benign pathology. The only sonographic feature significantly associated with malignancy was calcification (OR 2.85, 95% CI 1.78–4.55).
While a thyroid nodule on average carries a 5–10% risk of malignancy, there is a threefold increase in the risk of malignancy in a thyroid nodule when calcifications are present on ultrasound.
THE RESIDUAL THYROID BELL CURVE: AN ASSESSMENT OF RESIDUAL THYROID TISSUE AFTER TOTAL THYROIDECTOMY FOR DIFFERENTIATED THYROID CANCER
Thyroid Imaging Thursday Poster Clinical
The amount of residual thyroid tissue after total thyroidectomy and factors that result in a larger thyroid remnant are unknown. We sought to quantify how much residual thyroid tissue remains after total thyroidectomy at the university and community hospitals and determine factors that are associated with a larger remnant.
We queried our hospital's radiology database for patients with 123I or 131I thyroid uptake scans after total thyroidectomy performed for differentiated thyroid cancer between 2007 and 2011. This included patients who had their surgery performed at our institution as well as outside institutions. Patients with prior thyroid surgery and 131I ablation were excluded. Type of operation, tumor pathology, and percent residual radioactive iodine uptake in the thyroid bed were noted.
A total of 109 patients fit our inclusion criteria. The average residual radioactive iodine uptake for all patients after total thyroidectomy was 0.97%, with a range from 0.03% to 6.5%, and a standard deviation of 1.05. Patients with residual thyroid tissue up to 3.08% were within 2 standard deviations from the mean, which constituted 94.5% (103/109) of all patients. The average residual uptake was 0.74% for patients with surgery performed at university hospitals versus 1.41% at community hospitals (p<0.05). Patients who underwent combined thyroidectomy with a lymph node dissection (either central or lateral, or both) did not have significantly different residual thyroid compared to patients who had a total thyroidectomy alone. Tumor size, histologic type (papillary, follicular variant of papillary, follicular, and Hurthle cell carcinoma), and the presence of lymphovascular invasion did not affect the quantity of residual thyroid tissue.
The amount of residual thyroid tissue as measured by radioactive iodine uptake after total thyroidectomy for differentiated thyroid cancer averages 1%, with 95% of all patients having a thyroid remnant under 3%. Patients with thyroidectomies performed at university hospitals have significantly less residual thyroid tissue than those performed at community hospitals.
DOES NODULE SIZE PREDICT COMPRESSIVE SYMPTOMS IN PATIENTS WITH THYROID NODULES?
Thyroid Nodules & Goiter Thursday Poster Clinical
Thyromegaly and thyroid nodules are known to cause compressive symptoms, but the exact relationship between the nodule size and development of compressive symptoms is unclear. We sought to determine whether compressive symptoms are directly related to nodule size.
A retrospective analysis of the patients who experienced preoperative compressive symptoms and subsequently underwent thyroidectomy or thyroid lobectomy by a single surgeon between July 2008 and January 2012 was performed. Compressive symptoms were defined as experiencing dysphagia, dyspnea, choking, or globus (neck fullness). We compared this cohort to a control group of all patients who also underwent thyroidectomy during this time period, but were asymptomatic preoperatively.
A total of 99 patients were identified of which 51 had compressive symptoms, and 48 were asymptomatic. Average nodule size in patients with compressive symptoms was 3.8 cm (SD 1.8) versus 2.2 cm (SD 1.3) in asymptomatic patients (p<0.0001). Average lobe diameter was 6.2 cm (SD 1.9) in patients with compressive symptoms versus 4.9 cm (SD 1.0) in asymptomatic patients (p<0.001). Visible thyromegaly was present in 65.2% of patients with compressive symptoms and 15.4% of asymptomatic patients (p<0.0001). The most common symptom was dysphagia, occurring in 80% of patients, followed by globus (69%), choking (49%), and dyspnea (32%). Patients with large left-sided nodules and patients with larger left thyroid lobes trended toward experiencing more dysphagia symptoms than those on the right; however, the difference was not significant. Of patients who underwent surgery for compressive symptoms, 92.7% had improvement in their symptoms postoperatively. Of patients with a thyroid nodule >1.5 cm, 97% showed improvement in symptoms postoperatively compared to only 1 in 3 (33%) of patients with a thyroid nodules <1.5 cm.
Thyroid nodule size and lobe size directly correlate with compressive symptoms. Of patients with compressive symptoms and a thyroid nodule >1.5 cm, 97% will experience improvement in symptoms postoperatively.
HOW THE ANTI-OXIDANT SYSTEM NRF2/KEAP1 RESPONDS TO OXIDATIVE STRESS IN THE THYROID GLAND
Thyroid Nodules & Goiter Thursday Poster Basic
Oxidative stress is an imbalance between pro-oxidative substances and antioxidant defenses. Unchecked oxidative stress can threaten homeostasis by oxidizing macromolecules. The transcription factor Nrf2 is a major mediator of transcriptional antioxidant responses that aim to sustain homeostasis and avert permanent cell damage. The goal of the present study was to investigate (1) whether the Nrf2 system is present and can be activated in cultured thyroid cells and (2) whether the Nrf2 system is activated in rodents during experimental goitrogenesis.
A well-characterized rat thyroid cell line (PCCL3) was used as an expedient model of Nrf2 function. As readouts for Nrf2 activation (i) the mRNA expression of its target gene NQO1; and (ii) an ARE-luciferase reporter construct were used. Next, the role of Nrf2 was tested in vivo in a mouse model under normal and goitrogenic conditions. A 3-week diet low in iodine and water supplemented with propylthiouracil was used in WT and Nrf2-KO mouse model.
As shown from the data (see Figure), Nrf2 mediates antioxidant transcriptional responses in cultured rat PCCL3 thyrocytes. Treatment of PCCL3 cells with glucose oxidase or with the Nrf2 activator sulforaphane induced the Nrf2 reporter construct, ARE-luciferase, as well as the Nrf2 target gene NQO1. To test whether the induction of NQO1 by sulforaphane was mediated by Nrf2, Nrf2 expression was knocked down by RNA interference (RNAi) before treatment with sulforaphane. RNAi was successful in decreasing NQO1 mRNA expression in response to sulforaphane treatment. Further, mRNA expression of the Nrf2 target gene NQO1 was observed to increase during goitrogenesis in a WT mouse model [see Figure, panel (C)]. In Nrf2 KO mice, no induction of NQO1 mRNA was observed, indicating that the induction seen in WT mice was mediated by Nrf2.
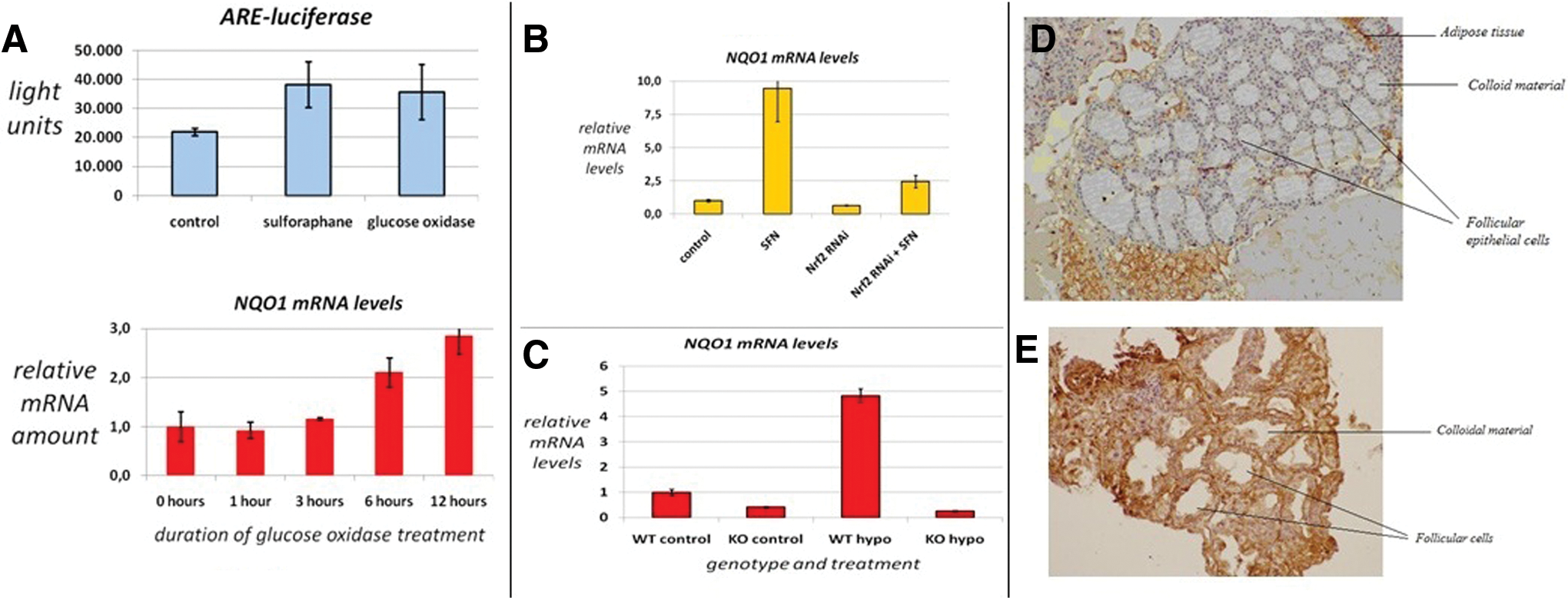
The results obtained in the present study support the hypothesis that Nrf2 is expressed in the thyroid, can be activated by oxidative stress, and can induce the transcription of its target genes during exposure to oxidative stress or during goitrogenesis.
Thyroid Nodules & Goiter Thursday Poster Translational
Recent studies have suggested that differentiated thyroid cancer (DTC) is associated with insulin resistance and adipokine expression. To investigate if these cytokines were able to identify thyroid nodule malignancy, we investigated serum levels of adiponectin (Adipo), leptin (Lep), resistin (Rtn), and ghrelin (Ghrl).
We quantified serum levels of Adipo, Lep, Rtn, and Ghrl through ELISA assays in 83 DTC patients (72 women, 11 men, 46.09-±13.80-years old); 55 benign cases (Ben: 44 women, 11 men, 49.41-±14.42-years old); and 105 controls (Ctl: 92 women, 13 men, 43.37-±13.39-years old) carefully matched for age, gender, and body–mass index (BMI).
We observed that DTC patients had lower Adipo serum levels (2.46±0.84) when compared with Ben (3.03±1.73, p<0.0001) and Ctl (4.81±2.89, p<0.0001. Lep was higher in DTC (9.82±0.70) than Ben cases (1.95±0.67, p<0.0001), but surprisingly, Ctl presented higher levels (19.42±14.66) than the nodule groups (p<0.0001). Ghrl levels were similar between DTC (84.56±24.02) and controls (89.29±29.24), but differed between DTC and Ben (133.57±18.00, p<0.0001) and Ben×controls (p<0.0001). Rtn levels were higher in DTC (14.80±1.53) than in Ben (1.99±0.66, p<0.0001) and Ctl (10.40±6.43, p<0.0001). A multiple logistic regression analysis confirmed that Adipo and Ghrl differentiated DTC from Ben cases. Every 1-unit increase of Adipo diminished in 31% the risk of DTC (p=0210; OR=0.699; 95% CI=0.516–0.948), and each Ghrl unit decrease diminished the risk of DTC 8% (p<0.0001; OR=0.923; 95% CI=0.898–0.949). AN ROC curve demonstrated that Adipo identified malignancy with a sensitivity 90%, specificity 56%, and accuracy 62.3%. Ghrl diagnosed malignancy with 95.1% accuracy, sensitivity 93.3%, and specificity 100%. Cytokine serum levels did not correlate to any clinical or pathological feature.
In conclusion, our data suggest that the reduction in serum Adipo and Ghrl levels may be associated to the development of DTC and could be useful in the identification of thyroid nodule individuals who may benefit more from preventive measures aiming to reduce weight.
Institute for Healthcare Studies, Northwestern University, Chicago, IL
Thyroid Nodules & Goiter Thursday Poster Clinical
On-site evaluation (OSE) of cytohistologic adequacy during fine-needle aspiration (FNA) reduces the rate of unsatisfactory results, but adds cost. We hypothesized that the addition of routine OSE to initial ultrasound-guided FNA of thyroid nodules is not cost effective.
Formal cost-effectiveness analysis from the societal perspective was performed using a decision model to compare strategies of routine initial OSE versus restriction of OSE to cases of prior unsatisfactory FNA. All FNAs performed with OSE were assumed to be adequate. Adequacy rates for FNA without OSE and utility adjustment for undergoing repeat FNA were estimated based on the literature review and institutional experience. Costs in 2011 US$ were estimated using Medicare limiting charges and Bureau of Labor Statistics wage rates. A one-time utility adjustment of 0.25 days was assigned to outcomes requiring repeat FNA. The threshold for cost effectiveness was defined as an incremental cost-effectiveness ratio of $100,000/quality-adjusted life year (QALY). Sensitivity analysis was used to examine the uncertainty of probability, utility, and cost estimates.
The routine OSE strategy produced a gain of 0.00007 QALY at an additional cost of $43.75 for an incremental cost-effectiveness ratio of $639,144/QALY when compared to restriction of OSE to cases with prior unsatisfactory results. On sensitivity analysis, routine OSE became cost effective if the FNA adequacy rate without OSE decreased from 90% to 85%; the cost of OSE decreased from $116 to $75; the cost of FNA increased from $366 to $735; hourly wage increased from $23 to $115, or utility detriment for repeat FNA increased from 0.25 to 1.6 days.
OSE for initial ultrasound-guided FNA of thyroid nodules is not cost effective unless the adequacy rate without OSE is <85%. When experienced operators perform FNA, OSE should be reserved for cases with previous unsatisfactory results.
Withdrawn
COMPARISON OF MINIMALLY INVASIVE VIDEO-ASSISTED THYROIDECTOMY (MIVAT) VERSUS CONVENTIONAL THYROIDECTOMY: A PROSPECTIVE ANALYSIS
Thyroid Nodules & Goiter Thursday Poster Clinical
Since the introduction of MIVAT in 1998, most of the published literature is from European centers. There is a paucity of data comparing this technique to conventional open thyroidectomy among Asian patients. We analyzed our results of MIVAT with that of conventional thyroidectomies for benign symptomatic goiters.
Between April 2011 and March 2012, data were collected prospectively for patients undergoing hemithyroidectomy by a single surgeon using either MIVAT or conventional open method. Inclusion criteria for both groups were FNAC-proven benign symptomatic goiters. A thyroid lobe volume of <35 cc or dominant nodule diameter <35 mm were prerequisites for the MIVAT approach. Larger goiters underwent conventional hemithyroidectomy. Patients with previous neck surgery and proven malignancy were excluded. The thyroidectomies were performed using a sutureless technique with ultrasonic shears and clips in both groups. The operative time, incision length, complications, and pain score were analyzed.
Twenty-one patients underwent MIVAT, and 15 patients underwent conventional hemithyroidectomy. Patients in both groups were comparable in terms of demographic profile and comorbidities. The mean operating time for MIVAT [111 min (±19.5 minute)] was not statistically significant compared to the conventional group [112 min (±25 minutes), p=0.9]. Patients undergoing MIVAT had significantly less pain in the postoperative period than the open surgery group (mean pain score 2.3 vs. 4.8, p<0.001). Mean incision length in the MIVAT group was 2.5 cm and that in conventional group was 6.3 cm (p<0.001). There were no major complications in any group. One patient in the MIVAT group required conversion to open technique due to technical difficulty.
In selected cases, MIVAT has the advantage of reduced pain, smaller scars with comparable operative time, and safety compared to conventional thyroidectomy.
Poster 118 can be found after Oral 28 on Page 50.
Friday, September 21, 2012
Experimental Therapeutics, Ohio State University Medical Center, Columbus, OH
Thyroid Cancer Friday Oral Clinical 5:00 PM
The majority of MTC cases occur sporadically, while the rest arise as part of inherited autosomal dominant syndromes. Germline mutations in RET are present in patients with inherited MTC, and tumor-associated RET mutations are found in up to 65% of patients (pts) with sporadic MTC. The common mutation RET M918T indicates poor prognosis. Bone metastases (mets) are common and debilitating events.
Pts were required to have documented RECIST progression within 14 months of screening. There were no restrictions on prior therapies, including treatment with tyrosine kinase inhibitors (TKIs). The primary endpoint was progression-free survival (PFS) as assessed by an independent radiology committee using RECIST. Objective response rate (ORR) was a secondary endpoint. Prespecified subgroup analyses included prior use of TKI, RET mutation status, and presence of bone mets.
Overall, 330 pts (RET mutation status: pos 48.2%, neg 12.4%, unk 39.4%; prior TKI: yes 20.6%, no 77.9%, unk 1.5%; bone mets: yes 49.4%, no 49.4%) were randomized 2:1 to cabozantinib (cabo, 140 mg free-base qd, n=219) or placebo (P, n=111). At the primary endpoint analysis, PFS was significantly prolonged (est median 11.2 mo for cabo vs. 4.0 mo for P, HR 0.28, 95% CI 0.19–0.40, p<0.0001). Overall, PFS results favored the cabo group across all subgroup analyses. RET mutation pos, neg, and unk subgroups showed HRs of 0.24, 0.47, and 0.30, respectively. Pts with hereditary and sporadic MTC showed HRs of 0.08 and 0.32. The poor prognosis subgroup of RET M918T-positive pts showed PFS HR of 0.17. The HRs for pts with and without bone mets at baseline were similar. Prior use of TKIs did not adversely impact response to cabo (HR=0.16). ORR was 28% for cabo vs. 0% for P (p<0.0001). ORR was consistent across subgroups, varying between 25% and 32% for the RET mutation status subgroups, and 21% each for pts with bone mets or prior TKI treatment. Analysis of tumor RAS mutation status is ongoing, and subgroup analysis will be presented.
The study met its primary objective of demonstrating substantial PFS prolongation with cabo vs. P in pts with progressing MTC. PFS results favored the cabo arm across prespecified subgroups.
ARUP Institute, ARUP Laboratories, Salt Lake City, UT
Thyroid Cancer Friday Oral Clinical 5:15 PM
Quantitative measurement of thyroglobulin (Tg) plays an important role in the follow-up of patients treated for differentiated thyroid cancer (TC). Circulating Tg autoantibodies (Tg-AAb) can mask epitopes and cause false-negative results when tested with immunoassay (IA). As a result, commercially available Tg IAs are unreliable for accurate measurement of Tg in many patients. We developed a liquid chromatography–tandem-mass spectrometry (LC-MS/MS) method that overcomes the drawbacks of commercial IAs and allows accurate measurement of Tg in the presence of Tg-AAb.
Tg is enriched from human serum samples; proteins are denatured, reduced, and digested using trypsin. A Tg-specific tryptic peptide is then enriched from the digests using antipeptide antibody conjugated to magnetic beads. After the enrichment, the samples are analyzed using LC-MS/MS; the analysis cycle time is 6.5 min per sample.
Limit of quantitation of Tg in serum was 0.5 ng/mL (0.75 fmol/mL). The mean imprecision of triplicate measurements in serum samples over 5 days (concentrations range 2 to 400 ng/mL) was 5.2%. Comparison with Beckman Coulter Access IA using serum samples free of Tg-AAb (n=61) showed good agreement between the methods; LC-MS/MS=1.05*IA+1.9, r=0.916, Sy/x=12.8. A set of 69 samples tested positive for Tg-AAb (Tg-AAb concentrations 19 to 3000 IU/mL; Tg recovery 27 to 97%) was analyzed by this LC-MS/MS method, and the concentrations were compared to the concentrations determined with a Beckman Coulter analyzer. In 16% of samples, concentrations of Tg measured by the IA were false negative, while concentrations determined by the LC-MS/MS method were above 1 ng/mL. False-negative results were likely caused by presence in the samples of Tg-AAb that interfered with the IA.
Proteolytic digestion of serum samples releases a Tg peptide targeted in the method and removes endogenous Tg-AAb that can interfere with traditional IA. This method has sensitivity and robustness sufficient for a routine clinical use. The method allows quantification of femtomolar quantities of Tg in the presence of Tg-AAb and would allow detecting recurrence of TC in patients with Tg-AAb more accurately than the immunoassays.
Institute of Metabolic Science, University of Cambridge, Cambridge, United Kingdom
Thyroid Hormone Action Friday Oral Clinical 5:30 PM
Resistance to thyroid hormone (RTH) is usually due to heterozygous mutations in the THRB gene with rare cases being homozygous for receptor defects. Here, we describe an RTH case due to a homozygous TRβ mutation (R243Q).
We describe the clinical and biochemical features of a consanguineous family with RTH.
The Proband (man, 8.4 yrs), was born at term with low birth weight (1.9 kg) to consanguineous parents. A prominent nasal bridge, goiter, and low body weight (10th centile) were noted; he has recurrent tonsillitis and is hyperactive, but has normal auditory function. Echocardiography showed mitral and tricuspid regurgitation, and 24-hour cardiac monitoring recorded sinus tachycardia. His circulating thyroid hormones (FT4>4-fold; FT3>8-fold raised) are very elevated, with normal TSH levels (see Table). THRB gene sequencing showed homozygosity for a nucleotide substitution, corresponding to an arginine-to-glutamine change at codon 243 (R243Q) in TRβ. Less abnormal thyroid function (FT4 1.2–1.8-fold, FT3 1.2–1.9-fold raised) in each parent and 3 siblings (see Table) was associated with heterozygosity for the R243Q TRβ mutation. Goiter, hyperactivity, and recurrent infections had also been noted in another sibling. He developed mitral regurgitation and cardiomegaly and died of heart failure at 13 years, despite diuretic therapy. Although his THRB mutation status is unknown, elevation of his thyroid hormones (FT4>3-fold, FT3>13-fold raised, see Table) comparable to the Proband suggests homozygous RTH, with cardiac hyperthyroidism contributing to his mortality
Characteristics of Studied Subjects
Previous studies indicated unique properties of R243Q TRβ, with normal T3 binding to mutant receptor in solution, but significantly impaired ligand-dependent dissociation of mutant receptor homodimers bound to DNA and delayed corepressor release. These characteristics likely account for unexpectedly significant dominant negative inhibition by R243Q mutant TRβ in vitro, correlating with our observed severe homozygous RTH phenotype. Future management, including prevention of possible cardiac decompensation in the proband, will be a therapeutic challenge.
Thyroid Nodules & Goiter Friday Oral Clinical 5:45 PM
The aim of the study was to evaluate the accuracy and impact of the thyroid imaging–reporting and database system (TI-RADS) for the diagnosis of thyroid carcinomas on a population encountered in a day-to-day practice.
We conducted a prospective study on a modified TI-RADS score developed to estimate the individual risk of thyroid carcinoma with ultrasound. We evaluated 4182 nodules in two years, all patients being referred for fine-needle aspiration biopsy (FNAB). Elastography was performed on a subset of 1306 nodules using manual compression with quantitative elasticity measurements. Each nodule was attributed a grade ranging from 1 to 5 (1: normal, 2: benign, 3: very probably benign, 4A and 4B: low and high risk of carcinoma, 5: carcinoma). Then, all nodules were submitted for FNAB, and the results read according to the Bethesda system. Results of TI-RADS grayscale score alone, elastography alone, and combination of the two methods were compared. Interobserver reproducibility was also tested using Cohen's kappa coefficient.
Prevalence of carcinoma in the studied population was 3.2%. Comparing TI-RADS grayscale score alone and its combination with elastography, sensitivity was, respectively, 96% and 99%, specificity 61% and 48%, negative predictive value 99.7% in both cases, and accuracy 62% and 48%. Positive predictive value of scores 4A, 4B, and 5 were, respectively, 6% and 4%, 69% and 42%, and 100% in both cases. Biopsying only nodules scored 4 and 5 would lead at least to a 34% decrease of the total number of FNABs, taking into account that lesions initially scored 2 and 3 whose size increases are also amenable to biopsy. Kappa coefficient was 0.72: substantial interobserver reproducibility was achieved.
TI-RADS score is a simple tool with good interobserver reproducibility that can be used to decide whether or not to make FNAB of thyroid nodules, even when applied to the population with low prevalence of thyroid carcinoma encountered in real clinical practice. It allows to detect the vast majority of thyroid carcinomas and dismisses 34% of all nodules for FNAB. Although a hard nodule should always be considered as highly suspicious, elastography was of little help in the diagnosis of thyroid carcinomas.
Statistical Results
Thyroid Cancer Friday Oral Clinical 6:00 PM
Tyrosine kinase inhibitors (TKIs) are used to treat patients with advanced refractory thyroid cancers, including radioiodine-resistant differentiated thyroid carcinomas (DTC) and medullary thyroid carcinomas (MTC). We hereby report the use of TKI as an off-label therapy for refractory thyroid cancer in 5 French-referral oncology centers.
All adult patients with thyroid cancer treated with a TKI outside of a clinical trial were evaluated. There were 65 patients (28 women, 37 men, mean age of 60 years); 22 (34%) had papillary thyroid carcinoma; 10 (15%) had follicular thyroid carcinoma; 13 (20%) had poorly DTC; 17 (26%) had MTC; and 3 (5%) had anaplastic thyroid carcinoma. Thirty-five (54%), 26 (40%), and 4 (6%) patients were treated with, respectively, one, two, and three lines of TKIs, which were sorafenib (47%), sunitinib (20%), vandetanib (29%), motesanib (2%), cabozantinib (1%), and lenvatinib (1%). Primary endpoints were response rate and progression-free survival (PFS), according to RECIST 1.1.
In the 55 patients with progressive and iodine-resistant DTC treated with sorafenib or sunitinib, the partial response (PR) rate was 18%, and median PFS was 7.0 months. In the 14 MTC patients treated with vandetanib, the PR rate was 36%, and median PFS was 39.1 months. In first-line sorafenib or sunitinib therapy, PR was seen in 36% of 28 DTC patients, but there was no PR with second- (n=24) and third- (n=3) line treatments; however, PFS was similar in second- compared to first-line treatment (6.7 vs.7.6 months). Liver metastases (n=18) were the most responsive (-28%) to treatment in all patients followed by lung (n=62) and lymph node (n=76) metastases, with respectively a mean morphologic response of −18% and −17%. Bone (n=17) and pleural (n=10) lesions were the most refractory to treatment (+1% and −8%).
This is the largest study evaluating off-label TKI therapies and the first to compare sequential treatments in thyroid carcinomas. DTC patients treated with second- and third-line therapies had stable disease as a best response without PR.
A 9-GENE MOLECULAR SIGNATURE ENHANCES DIAGNOSIS OF THYROID NODULAR GOITER
Thyroid Nodules & Goiter Friday Oral Clinical 6:15 PM
Although FNA is currently considered to be the best initial diagnostic test for evaluation of a thyroid nodule, it cannot always discriminate between benign and malignant thyroid tumors. To address this issue, we developed a molecular assay for thyroid FNAs that tests both the expression of genes that becoming expressed in cancerous thyroid tissues, as well as the presence of the oncogenic BRAF V600E mutation.
We used a cohort of 102 cases (105 nodules), 88 women and 14 men, aged 46.6-±15-years old, presented with nodular or multinodular, nontoxic goiter. Thyroid ultrasound-guided FNABs were performed. Tissues from 2 aspirations of the needle were used for a cytological examination. A third aspiration was transferred into a tube containing nucleic acid stabilization buffer. A molecular 9-gene signature that tests the expression of 8 genes encoding cell surface receptors and oncogenes and the presence of BRAF V600E mutation was performed, by quantitative real-time PCR.
A positive 9-gene signature was obtained in 20 cases (19%). Agreement between gene signature and cytology assessment was found in 102 out of 105 nodules (97%). Three cases (15.7% of all positive cases) were positive for malignancy by gene signature and negative by cytological criteria. However, all 3 cases were found to be positive for malignancy after surgery, which underscores the value of this molecular assessment. We have validated this gene signature with surgical samples from 29 thyroidectomies. BRAF V600E mutation was absent only in one case of a positive biopsy.
We developed a combined gene expression and mutation analysis assay as an accurate tool for determining the presence/absence of malignancy in thyroid FNAs. This methodology will enhance the diagnosis of thyroid nodules, particularly in those cases in which it is necessary to resolve uncertainties.
Endocrinology and Metabolism, Academic Medical Center Amsterdam, Amsterdam, Netherlands
Thyroid Hormone Metabolism & Regulation Friday Oral Basic 5:00 PM
Nonthyroidal illness syndrome (NTIS) is associated with decreased TRH expression in the paraventricular nucleus (PVN) of the hypothalamus. This is probably due to increased local production of T3 by type 2 deiodinase (D2), an enzyme that is expressed in tanycytes lining the wall of the third ventricle. Administration of lipopolysaccharide (LPS), which is an established model of NTIS in rodents, increases D2 expression in tanycytes. We studied the involvement of the inflammatory signal transduction pathways in LPS-induced upregulation of D2 in tanycytes using an in vivo and in vitro approach.
For the in vivo approach, mice were injected intraperitoneally with bacterial endotoxin (LPS) or saline, and the periventricular area (PE) and arcuate nucleus region (ARC) were isolated. An in vitro model was established using a primary culture of tanycytes from the brains of 10-day-old rat pups. These cultures were stimulated with LPS for 6 hours. We assessed mRNA expression of NFkB p65, JNK, and C/EBPa mRNA as key elements of the inflammatory pathway by qPCR. The presence of tanycytes in primary cell cultures was confirmed by qPCR for DARPP-32, nestin, vimentin, and GFAP and immunostaining for vimentin and GFAP.
NFkB p65 and C/EBPa mRNA levels were increased in the PE and ARC of mice 4 and 8 hours after LPS administration. The tanycyte cultures expressed DARPP-32, nestin, vimentin, and GFAP mRNA and showed immunostaining for vimentin and GFAP, indicating the presence of tanycytes and additional glial cell types in the culture. LPS stimulation of the tanycyte cultures resulted in an increase in D2 and NFkB p65 mRNA expression. No changes were found in mRNA levels of C/EBPa and JNK.
Our results suggest a role for NFkB p65 in the upregulation of D2 in tanycytes during inflammation. Future experiments will include gene-silencing methods to further elucidate the mechanism of inflammation-induced D2 increase in the hypothalamus.
EXTRACELLULAR FLUX ANALYSIS IS A SENSITIVE METHOD FOR SIMULTANEOUS QUANTIFICATION OF THYROID HORMONE-MEDIATED INCREASES IN ENERGY EXPENDITURE AND GENE EXPRESSION IN LH86 HEPATOMA CELLS
Thyroid Hormone Action Friday Oral Basic 5:15 PM
Thyroid hormone (3-3′-5-triiodothyronine, T3) has long been known to influence the metabolic rate. Studies have identified a multitude of genes that respond to T3 and have a metabolic function; however, it is not clear which genes are most important. To clarify the situation, we propose that gene expression should be measured while cells are exhibiting a T3-dependent increase in energy expenditure. Furthermore, the concentration of T3 should be as low as possible to avoid off-target effects.
In this study, we describe and validate a new protocol for extracellular flux analysis using the Seahorse XF96 system, in which groups of cells are experimentally defined to have equal oxygen consumption rates (OCR) and extracellular acidification (of the medium) rates (ECAR) before randomization for treatment with T3 or vehicle.
Using this approach, hypothyroid LH86 hepatoma cells can be shown to increase OCR by ∼5% within 6.5 hours using only 1 nM total T3 (∼40pM free-T3). Glycolytic flux (as reflected in ECAR) increases slightly with T3; this precedes changes in OCR. Because measurement of OCR and ECAR is nondestructive, it is possible to measure gene expression in the same cells exhibiting the energetic phenotype. Microarray analysis of the LH86 cells from the XF96 assays identified 61 differentially expressed genes, with lipid metabolism and the complement pathway being among the most T3-sensitive processes changing while OCR/ECAR are increasing. Results were confirmed via RT-PCR: e.g., upregulated genes included acyl-CoA synthetase medium-chain family member 2A (5.3-fold, p<0.01), mannose-binding lectin (3-fold, p<0.01), and fibrinogen beta chain (2-fold, p<0.0003), while malic enzyme was unchanged.
These data demonstrate an improved method for measuring small changes in energy expenditure in living cells, making it possible to study T3-mediated changes in energy expenditure in real time at both the metabolic (OCR and ECAR) and transcriptional levels using concentrations of T3 at least an order of magnitude lower than prior studies. Follow-up studies will be directed toward sorting the gene set to identify the critical factors mediating the observed changes in energy expenditure.
Otorhinolaryngology: Head and Neck Surgery; Medicine, Hematology/Oncology, Abramson Cancer Center, Philadelphia, PA
Thyroid Cancer Friday Oral Basic 5:30 PM
We conducted a Phase 3 study of cabozantinib (cabo, an oral inhibitor of MET, VEGFR2, and RET) versus placebo (P) in patients with progressive MTC. At the primary endpoint analysis, PFS was significantly prolonged (est median 11.2 mo for cabo vs. 4.0 mo for P, p<0.0001). Exploratory correlative analyses of RET mutational status with PFS and tumor markers calcitonin (CT) and carcinoembryonic antigen (CEA) with tumor response were performed. The effects of cabo treatment on the mechanism-based plasma biomarker sVEGFR2 were explored.
Plasma and serum samples were evaluated for levels of sVEGFR2, CT, and CEA. RET mutational status was determined from blood and archival tumor samples using Sanger and large-scale parallel sequencing methods.
sVEGFR2 showed a cabo-dependent decrease on Day 29 of 33% (p<0.0001) compared to no change with placebo. There was a modest correlation between the extent of biomarker reduction and cabo plasma exposure on Day 29. At week 12, levels of CT and CEA had risen in the P group compared to baseline (57% and 89%, respectively, p<0.0001), but had fallen in the cabo group (-45% and −23%, respectively, p<0.0001). There were statistically significant correlations between the percent change in CT or CEA and the percent change in the sum of target lesion diameters at week 12. Pts achieving biochemical partial response (>50% decrease in CT or CEA) were more likely to have objective tumor response than subjects with biochemical progressive disease (>50% increase). Of the 330 patients enrolled in the study, RET mutation status was determined for 200 (61%). Of these, 79.5% and 20.5% were RET mutation positive and negative, respectively; the mutation most frequently found was M918T (74% of RET-positive pts). PFS hazard ratios and tumor response rates favored the cabo arm among all RET mutation subgroups. RAS mutations are common in RET-negative tumors, and analysis of tumor RAS mutation status is ongoing.
Correlative biomarker studies support the proposed mechanism of action for cabo in the setting of MTC, with decreases in VEGFR2 pathway-related and tumor-related biomarkers, and clinical activity found in both RET mutation-positive and negative pts.
Endocrine Research Centre, Research Institute for Endocrine Sciences, Shahid Beheshti University (MC), Tehran, Islamic Republic of Iran
Autoimmunity Friday Oral Basic 5:45 PM
Epidemiologic studies strongly implicate a genetic contribution to autoimmune thyroid disease (AITD). We used a multistage strategy to identify genetic variants associated with AITD using a DNA pooling-based genome-wide association study (GWAS) of 1,000,000 single-nucleotide polymorphisms (SNPs) in the Iranian population.
A population-based sample from the Tehran Lipid and Glucose Study (TLGS) was used. In the first stage, 1434 subjects aged >20 years from the TLGS were assessed for autoantibody to thyroid peroxidase (TPOAb) levels. AITD was defined as TPOAb levels ≥100 IU/mL; subjects with low (<20 IU/mL) TPOAb levels were chosen as controls. Subjects were age- and sex-matched and assigned to the AITD (n=100, mean age 42.1±13.3 yrs) or control group (n=162, mean age 42.0±13.1 years). Each DNA pool was allelotyped on 4 Illumina Human1M-Duo arrays, and allelotype-based tests of association were used to rank SNPs using GenePool software. In the second stage, to validate and replicate high-ranking SNPs by individual genotyping, we selected 116 SNPs. SNPs were chosen based on two criteria: GenePool-based rank and supporting high rankings of other SNPs in high-linkage disequilibrium with the SNP of interest. The 116 SNPs were genotyped in individual DNA samples from 811 Iranian samples (189 AITD individuals, 74 participated in pools; 622 control individuals, 123 participated in pools) using Sequenom MassArray iPLEX assays.
About 115 SNPs were genotyped successfully and tested for association with AITD using logistic regression implemented in PLINK 1.07. Twenty-six SNPs were associated with AITD (uncorrected p-values 0.05–5.4×10−5), of which 2 SNPs at novel loci (9q33.2 and 20q11.2) remained significant after Bonferroni correction for 115 tests (Padjusted=6.2×10−3, OR=1.96 and Padjusted=3.5×10−2; OR=1.63; respectively). Replication of the most significant markers in ∼1,500 additional AITD (∼500) and controls (∼1,000) is underway.
We have identified novel loci associated with AITD using a multistage DNA pool-based GWAS. Discovery of AITD susceptibility genes holds promise to provide insights into the mechanisms of this disease.
Kolling Institute, University of Sydney, Sydney, NSW, Australia
Thyroid Cancer Friday Oral Basic 6:00 PM
Genetics variants such as rs1867277 close to FOXE1 are strongly associated with papillary thyroid cancer (PTC). We have recently shown that rs1867277 is in tight linkage disequilibrium with a polymorphic polyalanine tract located within FOXE1. We also found that FOXE1 transcriptional activity is altered according to the polyalanine tract length. The aim of this study was to identify FOXE1 cofactors, to assess whether transcriptional disruption by a longer polyalanine tract was due to altered cofactor affinity.
Potential cofactors from Nthy-ori-3.1 cells were identified using a FLAG-FOXE1 construct and the TranSignal™ TF-TF Array Kit (Panomics, Inc., Redwood City, CA). Endogenous FOXE1 and ELK1 were coimmunoprecipitated from Nthy cell extracts. Mammalian two-hybrid assays were performed by transient transfection of GAL4-FOXE1 (C-terminus) and VP16-ELK1 into Nthy cells together with pG5Luc. Nthy cells were also transfected with expression vectors for full-length FOXE1 and ELK1 together with TPO-Luc. For some experiments, EGF (25 ng/mL) or PD98059 (10 uM) was added. ChIP assays were performed using DNA isolated from Graves' thyroid tissue.
The strongest signal identified in the TF-TF array corresponded to ELK1, a transcriptional effector of MAPK activation. FOXE1-ELK1 interaction was confirmed by (a) coimmunoprecipitation of endogenous FOXE1 and ELK1 from Nthy cells; (b) mammalian two-hybrid assays; and (c) cotransfection of full-length FOXE1 and ELK1 on TPO-Luc. Chromatin immunoprecipitation assays confirmed that both proteins simultaneously occupy binding sites within the TPO and TG proximal promoters in human thyroid tissue. MAPK stimulation by EGF treatment disrupted FOXE1-ELK1 interaction as assessed by co-ip. Conversely, treatment of SW1736 thyroid cells (containing BRAFV600E) with a MEK inhibitor (PD98059) increased TPO-Luc expression.
We identified ELK1 as a novel interacting partner of FOXE1. This interaction is sensitive to MAPK activation. Since PTC is essentially dependent on somatic alteration of the MAPK pathway genes, our observations may explain at least in part the association between FOXE1 germline variants and PTC.
Department of Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN
Thyroid Cancer Friday Oral Basic 6:15 PM
Iodination of thyroglobulin (Tg) differs between benign and malignant thyroid tissue. If the precise nature of these differences could be determined and shown to be consistent, assessment of Tg iodination status might become a tool to augment cytological diagnosis of thyroid nodules. We explored this possibility using comparative mass spectrometric assessment of Tg iodination status in metastatic papillary carcinoma (PTC) and benign thyroid nodules.
Four different preparations of purified normal human Tg were digested with trypsin, chymotrypsin, and GlucC to maximize peptide coverage and analyzed by high-resolution LC-MS/MS (ABSciex 5600 Q-TOF). Proteotypic peptides containing consistently iodinated sites were identified by protein database search, focusing on iodination. A total of 20 monoiodinated tyrosines, 11 di-iodo tyrosines, 1 thyroxine, and 1 monoiodinated histidine were found. Based on consistent high iodination, peptides spanning 6 of these sites (4 monoiodinated and 2 mono- and di-iodinated) were selected for quantification by selective reaction monitoring MS/MS in benign and malignant thyroid tissues. The two most intense of these peptide pairs (SHGQDSPAVY*LK and ENILLEPY*) were then quantified in 8 benign thyroid nodule fine-needle aspiration biopsy (FNAB) needle washes and 13 FNAB needle washes from neck lymph nodes with metastatic PTC.
Of the 13 malignant specimens, 2 had insufficient signal for evaluation. The remaining 11 specimens contained almost exclusively the noniodinated versions of the tested peptides, with ratios of noniodinated peptides to matched iodinate peptides of >15:1. One of the 8 benign thyroid FNABs also had insufficient signal for evaluation. Among the 7 benign specimens with adequate signals, all showed identifiable iodinated peptide signals in addition to the noniodinated signals, with ratios of noniodinated to matched iodinated peptides of ∼2:1.
Tg from metastatic PTC lacks iodination, while iodination is strong and consistent in benign thyroid nodules. Measurement of Tg iodination status by mass spectrometry may allow differentiation between benign and malignant thyroid lesions.
Section of Endocrinology, Dept. of Clinical and Experimental Medicine & Pharmacology, University of Messina, Messina, Italy
Disorders of Thyroid Function Friday Poster Clinical
A novel formulation of LT4, in which the hormone is dissolved in a glycerin environment and protected by a soft gelatin shell (Tirosint capsule, IBSA, Switzerland), is bioequivalent to reference LT4 tablet (Synthroid, Abbott, USA) [Colucci et al. Ther Drug Monit 2011;33]. Recently, the capsule showed superiority over the tablet in the setting of coffee-induced LT4 malabsorption [Benvenga et al. Thyroid 2011;21(1)]. PPIs are known to impair the intestinal absorption of LT4.
To evaluate the effect of PPIs on the absorption of LT4 in capsules and in tablets, an acute oral loading test with 600 μg LT4 of either formulation ingested with 240 mL water after an overnight fast was conducted in 16 healthy volunteers (8 per treatment). With a random crossover design, the volunteers repeated the test after being challenged with an acute infusion of 80 mg esomeprazole. Blood sampling was performed from predose up to 24 h postdose. Intragastric pH was monitored by a nasogastric tube.
In baseline (non-PPI) condition, AUC0-24, 0–6 or 0–1 h were (capsule vs. tablet) 788.9±158.1 vs. 867.2±162.3 (−9.0%), 226.7±58.4 vs. 248.9±58.8 (−8.9%), or 5.4±7.6 vs. 9.8±6.1 ngxh/mL (−45.0%) (p>0.20). Cmax was, respectively, 56.8±20.7 vs. 55.4±11.6 ng/mL. Under PPI infusion, absorption of LT4 decreased to a lower extent, compared to the corresponding baseline condition, when LT4 was in capsule. Indeed, capsule AUC0-24, 0–6 or 0–1 h were 743.7±142.1 (−5.7% compared to the aforementioned baseline values), 206.0±54.9 (−9.2%), or 5.6±8.1 (+3.3%). In contrast, tablet AUC0-24, 0–6 or 0–1 h were 776.6±135.9 (−10.4% vs. baseline), 202.3±35.4 (−18.8%), or 7.2±3.8 (−26.6%). Under PPl infusion, Cmax decreased by only 2.8% with the capsule, but by 13.0% with the tablet, compared to the corresponding baseline values.
Under the stressful test of alkalinizing the intragastric pH with PPIs, the absorption of L-T4 from the capsule appears to be far less affected than from the tablet. This in vivo more favorable profile of the capsule is consistent with the in vitro data [Pabla et al. Eur J Pharm Biopharm 2009;72] showing a more favorable dissolution profile of the capsule compared to either reference or generic tablets over a wide range of pH changes.
Section of Endocrinology, Department of Clinical & Experimental Medicine and Pharmacology, University of Messina, Messina, Italy
Thyroid Nodules & Goiter Friday Poster Clinical
By increasing the gastric pH, PPIs impair the dissolution of conventional L-T4 sodium salt tablets before intestinal absorption. We wondered if a liquid formulation of L-T4, already available in our country (Tirosint oral solution, IBSA, Italy), could solve the problem of L-T4 tablet malabsorption that is caused by concurrent therapy with PPIs. This new formulation contains L-T4 (which is a lipophilic hormone) already solubilized in an organic solvent (100 μg L-T4 sodium salt in 243 mg ethanol), and thus ready to be absorbed.
Upon consent, we enrolled 15 such patients (12 F, 3 M), 7 of whom used to take omeprazole, 5 pantoprazole, and 3 lansoprazole. Six out of 15 (40%) were under replacement therapy (REP), while 9/15 (60%) under suppressive therapy (SUP). They were switched to the liquid formulation, maintaining the same daily dose of L-T4. Serum TSH was rechecked at least 2 months after switch. Statistics included Mann–Whitney and Fisher's exact tests.
In the REP or SUP group, serum TSH averaged 2.77±2.05 or 1.15±1.85 mIU/L while taking the L-T4 tablet, but 1.63±0.66 (p=0.087 vs. 2.77±2.05) or 0.12±0.12 (p<0.0001 vs. 1.15±1.85), while under liquid L-T4 for at least 2 months. In the SUP group, the rates of TSH levels ≤0.10 mU/L were 0/19 assays under the tablet vs. 17/22 (77%) assays under the liquid formulation (p<0.001). During the follow-up, the daily dose of liquid L-T4 had to be decreased in 2/9 (10%) SUP patients.
Our data demonstrate that the liquid formulation of L-T4 is capable to solve the problem of incomplete absorption caused by PPIs, because it can be directly absorbed, irrespective of the gastric pH.
Section of Endocrinology, Department of Clinical & Experimental Medicine and Pharmacology, University of Messina, Messina, Italy
Autoimmunity Friday Poster Clinical
Vaccine immunotherapy for malignancies is based on the administration of tumor-associated antigens (TAAs) that are bound by specific HLA molecules. Immunotherapy with NY-ESO-1, a TAA expressed by a number of malignancies, triggered hyperthyroidism or hypothyroidism in two HLA-A2 patients with ovarian cancer (Clin Cancer Res, 2008). Here, we report a case of GD triggered by vaccination with NY-ESO-1 in one HLA A2-negative woman with a different malignancy.
A 32-year-old woman with a synovial sarcoma was treated with radiotherapy, chemotherapy, and NY-ESO-1 combined with an immune adjuvant. Immunotherapy was given for two cycles, each cycle consisting of 5 administrations. The patient typed HLA A11/A33(19), B13/B56(22), Cw3/. One month after having started immunotherapy, clinical thyroid dysfunction was suspected. Data were consistent with hyperthyroidism due to GD, with low TSH (0.02 mU/L), high FT3 (7.4 pmol/L), FT4 (26.2 pmol/L), and thyroid-stimulating immunoglobulins (TSI) (152%, normal range<140). Hyperthyroidism worsened progressively (FT4>60, FT3>30, TSI>500), so that the patient was eventually thyroidectomized. Thyroid histology confirmed GD. Therefore, using the NCBI software BLAST (http://blast.ncbi.nlm.nih.gov/Blast.cgi), we looked for amino acid sequence homologies between NY-ESO-1 and thyroid autoantigens [TSH-receptor (TSH-R), thyroperoxidase (TPO) and thyroglobulin (Tg)]. Using the HLA ligand/motif database (Tissue Antigens, 2003), we searched the HLA-binding motifs in the regions of NY-ESO-1 and thyroid autoantigens that were homologous.
We found 15 regions of NY-ESO-1, all epitopic, which were homologous to 15 regions of thyroid autoantigens, some of which epitopic: 5 segments of TSH-R, 8 of Tg, and 2 of TPO. These homologous segments contain binding motifs belonging to several HLA class I antigens, including the patient's A11 and A33. Furthermore, 2 homologous segments of TSH-R contain HLA-A2-binding motifs.
As vaccines are emerging as a standard treatment for malignancies, vaccine-induced thyroid dysfunctions are expected to increase in genetically predisposed patients over the next years.
State Key Laboratory of Medical Genomics, Ruijin Hospital, Shanghai, China
Autoimmunity Friday Poster Basic
Graves' disease (GD), a common autoimmune disorder characterized by autoantibodies targeting antigens specifically expressed in thyroid tissues, is triggered by a combination of genetic and environmental factors.
To enrich the genetic architecture of GD, we carried out a three-stage genome-wide association study in ∼20,000 subjects to identify new susceptibility loci for GD.
We found strong evidence in the overall populations for six previously undetected or indefinite susceptibility loci: the C1QTNF6-RAC2 region at 22q12-13, SLAMF6 at 1q23.2, ABO at 9q34.2, TG at 8q24.22, GPR174-ITM2A at Xq21.1, and an intergenic region at 14q32.2 (Pcombined<5×10–8). We also found significant heterogeneity between the sexes in the associations of rs5912838 at Xq21.1 and rs2284038 at 22q13.1.
This study increases the number of GD loci with compelling evidence from 9 to at least 15.
Molecular Thyroid Research Laboratory, Gutenberg University Medical Center, Mainz, Germany
Autoimmunity Friday Poster Clinical
Thyroid-stimulating autoantibodies (TSAbs) mediate the activity of Graves' disease (GD) and thyroid-associated orbitopathy (TAO). Scarce data are available on the relevance of TSAbs in children with autoimmune thyroid diseases (AITD). Thus, we aimed to detect and follow serum levels of TSAb in a large pediatric cohort with AITD.
TSAbs were measured with the help of a FDA-cleared chimeric TSH receptor bioassay. TSAbs were reported as percentage of specimen-to-reference ratio (SRR%, cutoff 140%). Thyroid-binding inhibiting immunoglobulins (TBIIs) were also measured in all samples.
A total of 212 serum samples were collected from 172 pediatric patients with AITD: 32 with GD (30 female children, mean age±SEM 13.4±0.7 years, 11 with TAO), 68 with Hashimoto's thyroiditis (HT, 57 female children, 13.4±0.4 yrs.), 27 with type 1 diabetes (T1D, 14 female children, 14±0.5 yrs.), 5 with juvenile arthritis (JA, two female children, 14.3±1.5 yrs.), and 40 healthy controls (C, 18 female children, 12.5±0.7 yrs.) were evaluated for the presence of TSAbs and TBIIs. Of 53 measured samples with GD, TSAbs were detected in 47 (89%) in contrast to TBII positivity in 40 (75%), only (p<0.0001). All six TSAb-negative samples were from euthyroid, pretreated patients. Mean serum TSAb levels were SRR% 403±24 and 239±63 (p=0.02) in untreated and treated children with GD, respectively. Mean TSAb levels were markedly higher (p=0.03) in children with (SRR% 434±27) vs. without (317±37) TAO. Also, in two children with HT and TAO, TSAbs were present (SRR% 429 and 215). In contrast, in the pediatric HT patients without TAO, mean TSAb levels were SRR% 51±4. All 13 children with TAO were TSAb positive, but only 11 (85%) were TBII positive. All children with T1D, JA, and/or C samples were TSAb negative.
These novel data demonstrate the close association between TSAbs and TAO in a large pediatric collective with AITD.
Molecular Thyroid Research Laboratory, Gutenberg University Medical Center, Mainz, Germany
Autoimmunity Friday Poster Translational
The analytical performance of two-chimeric TSH receptor (TSHR) bioassays for measuring TSHR-stimulating (TSAb) and blocking (TBAb) autoantibodies was investigated.
Chinese hamster ovary cells expressing a chimeric TSHR were grown for 15–18 hours at 37°C. Limits of Blank (LoB), Detection (LoD), and Quantitation (LoQ) were measured according to the standardized CLSI EP17-A protocol with the help of commercially available monoclonal thyroid-stimulating (M22) and blocking (K1-70) autoantibodies (MAb). In the TSAb bioassay, cells were treated with M22 dilutions and for TBAb with bovine TSH, K1-70 dilutions, and/or patient serum. Results for TSAb or TBAb were expressed as percentage of specimen-to-reference ratio (SRR%) or as percent inhibition of luciferase expression relative to induction with bTSH alone.
In the TSAb bioassay, LoB and LoD were measured 40 times in duplicate with 1:11 diluted control serum and with eight low M22 concentrations ranging 0.09–0.005 ng/mL, respectively. Each M22 concentration was measured 20 times in duplicate. For TBAb, LoB was measured using 1200+ replicates of 350 control sera. LoD was measured with 100+ replicates with the K1-70 concentrations 10–0.3125 ng/mL in twofold serial dilutions. The half-maximal effective concentration (EC50) was determined based on the dose–response curve obtained with the M22 concentrations 100–0.003 ng/mL in twofold serial dilutions and with the K1-70 concentrations 100–0.1 ng/mL in fourfold serial dilutions, respectively. In the TSAb bioassay, LoB, LoD, and EC50 were found to be 76.09 SRR%, 90.47 SRR%, and 0.02 ng/mL M22, respectively. LoD and LoQ were both determined to be 0.02 ng/mL of M22. With the TBAb bioassay, LoB, LoD, and EC50 were found to be 30.2%, 43.4% inhibition, and 2.44 ng/mL K1-70, respectively. LoD was 1.25 ng/mL of K1-70. Thus, both bioassays detect very low concentrations of MAb.
The data demonstrate the analytical performance of these novel bioassays.
Endocrinology, Deenanath Mangeshkar Hospital & Research Centre, Pune, India
Autoimmunity Friday Poster Clinical
Background: The study aimed at assessing clinical, biochemical profile, quality of life (QOL), and cardiac function in Subclinical Hypothyroidism (ScHt).
Methods: 65 ScHt adults and 11 matched controls from a charitable hospital in Mumbai were invited. ScHt was defined as S.TSH≥5.0 μIU/mL, normal S.FT3, S.FT4 documented twice. Secondary causes (ablative, surgical, drugs, and pregnancy) were excluded. Clinical evaluation, thyroid function tests, lipids, QOL (PCASSE questionnaire—WHO), and cardiac time intervals (41 cases) using Color Doppler were assessed. SPSS (version10.1) was used for analysis.
Observations: The M: F ratio was 1:64 vs. 0:11. Mean age was 38.63 yrs vs. 40.2 yrs in controls. Average BMI was 26.4 kg/m2 vs. 25.0 kg/m2. Mean symptom score 9.2 in patients vs. 3.3 in controls. About 55.3% patients were goitrous (grade 1 in 23%) vs. 9% of controls. Family history was positive for T2DM (27%), hypothyroidism (15.6%), and autoimmunity (6.2%). About 20.3% were postmenopausal, and 51% premenopausal cases had menorrhagia (20%), hypomennorrhoea (11%), oligomenorrhoea (20%), infertility (10.3%), and spontaneous abortions (17.3%). Common symptoms were lethargy (63.1 vs. 18%), fatigue (69.2 vs. 40%), and weight gain (61.5 vs. 44.8%). Common signs were goiter (55.3%), coarse dry skin (36.9%), and puffiness (35.4%). Mean TSH was 10.11 μIU/mL verses 2.02 μIU/mL in controls. S.AMA and S.anti-TPO antibodies were positive in 49% and 58.5% cases. Thyroid FNAC showed Hashimoto's thyroiditis (75%). QOL was significantly reduced mainly due to physical reasons (see Table). The Apo A was low (1.125 vs. 1.527 g/L; p=2.5×10−5), and Apo B was high (1.45 vs. 0.991 g/L; p=0.001). About 22% had ST-T changes in ECG lead III. Diastolic function parameter MAPV and cardiac systolic time interval: PEP and PEP/ET ratio were increased while LVET was reduced.
QOL Scores in ScHt vs. Controls
QOL
Significantly low scores in patients than in controls.
Autoimmune ScHt presents in younger women in India. ScHt has significant, and hence is not literally subclinical.
Disorders of Thyroid Function Friday Poster Clinical
Background: We aimed to study the effect of L-thyroxine therapy on clinical, biochemical profile, cardiac function, and quality of life (QOL) in ScHt over six months.
Methods: 65 ScHt adults (S.TSH≥5.0 μIU/mL, normal FT3, FT4) and 11 matched healthy controls from a charitable Mumbai-based hospital were invited. Secondary causes (ablative, surgical, drugs, and pregnancy) were excluded and randomized into Group A (30 patients receiving L-Thyroxine 50 μg qd, titrated over 6 months), Group B (35 patients on lifestyle measures), and Group C (11 controls under observation). Clinical evaluation, thyroid function tests, lipids, QOL (PCASSE questionnaire—WHO), and cardiac time intervals (CTI in 41 cases) using Color Doppler were assessed at baseline and 6 months. SPSS (version10.1) was used for analysis.
Observations: Group A: S.TSH normalized with thyroxine 1 μg/kg/d, Ankle edema, irritability, reduced memory, weight gain (0.195-kg fall), QOL scores, menses (61.5% vs. 16.6%). S.prolactin level improved (18.51 to 6.73 ng/mL p=0.062) while goiter [28.5% (p=0.002), ApoB reduced (1.43 to 1.25 g/L p=0.021)], Systolic CTI viz: PVPEP (p=0.039), SVR, LVIVRT, MFEPV decreased and diastolic CTI-like LV mass, LVET, and M E deceleration time increased (p=NS). Group B: None became overtly hypothyroid. Dry skin, constipation, irritability, cold intolerance, alopecia, dry hair, myalgia, sweating abnormalities, and goiter (83.3%) persisted. Physical QOL worsened (see Table). Apo B decreased, while Apo A (p=0.021) and S.prolactin increased (6.54 to 10.81 ng/mL p=0.453). SVR, LVIVRT, MFEPV, and M E deceleration time increased and LV mass LVET decreased (p=NS); Group C: HDLc rise (p=0.002) was the only change.
Changes in QOL Scores over 6 Months
Significantly low scores in patients than in controls at baseline, and significant change at 6 months from baseline QOL improved in 73.3% (20% in Group B) worsened in 6.67% (34.28% in Group B).
Summary: Our study favored the use of L-thyroxine therapy as it reduced morbidity. Untreated, one third progressed with reduced QOL.
Pediatrics, Rady Children's Hospital San Diego, San Diego, CA
Autoimmunity Friday Poster Clinical
Subacute thyroiditis (SAT) is rarely reported in children. It is not usually associated with autoimmune thyroiditis. Neck pain or tender goiter usually follows a viral illness. Autoimmunity may be a secondary and/or transient phase. Hyperthyroidism is typically followed by euthyroidism, then possibly hypothyroidism, and ultimately euthyroid within 6–12 mo.
Chart review of 3 pediatric cases with SAT and underlying autoimmunity.
Case 1: A Hispanic female child with goiter, diagnosed at age 10.5 yrs with Hashimoto's thyroiditis, per high antithyroid antibodies, was euthyroid for 9 mo, till she became hyperthyroid, presenting with neck pain preceded by URI. Diagnosed with SAT per low iodine uptake (I-uptake) on thyroid scan, no signs of Graves' disease and negative TSI. Initially hyperthyroid, TSH<0.03 μIU/mL (0.35–5), high free-T4=2.05 ng/dL (0.9–1.4). Free-T4 normalized 10 days later, TSH stayed low, ESR=13 (1 mo postprodrome). Stayed euthyroid 4 mo, then hypothyroid 10 mo later (TSH=34.6), and levothyroxine was started. Case 2: A 14 yo Caucasian male child with Type 1 diabetes (positive GAD and ICA512) for 7 years presented with a tender thyroid preceded by a mild viral illness. Diagnosed with SAT with hyperthyroidism, per low I-uptake, raised ESR=24, and negative TSI. Initially TSH<0.03, high free-T4=1.95 ng/dL (0.71–1.85) and T3=205 ng/dL (84–179). Antithyroid antibodies remained negative since diagnosis of diabetes. One mo later was euthyroid; 2 mo after his hyperthyroidism, he was mildly hypothyroid, TSH=7.43 μIU/mL, T4=4.5 μg/dL (4.3–12.5), and became euthyroid 2 mo later. Case 3: An 18 yo Hispanic woman with pulmonary arterial hypertension presented with dyspnea, tachycardia, and painless goiter. Diagnosed with silent SAT per low I-uptake and negative TSI. Had underlying Hashimoto's thyroiditis with anti-TPO>900 and ANA 1:160. Initial TSH<0.03 μIU/mL, high free-T4=5.06 ng/dL, and T3=290 ng/dL. Methimazole used for 1 mo, stopped once euthyroid. Stayed euthyroid 8 mo, becoming hyperthyroid 1 year post-SAT, with a thyroid bruit and Graves' ophtalmopathy.
Subacute thyroiditis should be considered, even in patients with underlying thyroid or other autoimmunopathies. ESR and thyroid scan early on can aid in diagnosis.
Case Summaries and Chronology of Thyroid Status <3 mo Postdiagnosis
Disorders of Thyroid Function Friday Poster Basic
The thyroid status affects the motility of the intestine, so that hypothyroidism often leads to constipation, whereas hyperthyroidism is associated with diarrhea. The mechanism of this effect is not well known and may involve changes in the sensitivity of the contractile machinery in the intestinal wall.
We induced a condition of hypothyroidism (by administering methimazole) or hyperthyroidism (by supplementation with T3+T4) to a group of male rats, and evaluated the morphological and functional changes in the intestinal wall.
Hypothyroidism caused a condition similar to constipation by reducing the water contents of the feces, while hyperthyroidism caused the opposite (p<0.05). These effects may be due to the direct action of thyroid hormones, for positive immunolabeling of alpha-THRs was found in the nucleus of cells of all layers of the duodenal wall, with the greater numbers in the muscle layers (both internal and external) and the mucosa of the villi. Hyperthyroid animals showed an increase in the number of positive cells in both muscular layers (p<0.05), but hypothyroidism did not cause any significant effect. When assessed in vitro, the spontaneous contractile activity of intestine segments was no affected by the acute stimulation by thyroid hormones, but the thyroid status of the animal modified the response to the autonomic neurotransmitters. Hyperthyroidism potentiated the effect of norepinephrine and reduced that of acetylcholine on the muscular tone and tension (presumably acting on the muscle cells), but acted on the frequency of spontaneous contractions (presumably on the pacemakers) in the opposite way, which results in an overall increase in contraction rate. Hypothyroidism had modest effects on these variables.
These results suggest that the thyroid status affects the intestinal motility mainly by modifying the sensitivity to both the intrinsic and extrinsic controls of the contractile activity.
Department of Surgery, Vanderbilt University Medical Center, Nashville, TN
Disorders of Thyroid Function Friday Poster Clinical
Total thyroidectomy (TT) is the preferred surgical approach to Graves' disease (GD). Previous surgical series are hindered by small numbers and a mix of subtotal and TT approaches spanning several decades. Here we present the outcomes for TT at a single high-volume center.
A retrospective cohort study was conducted on 165 patients undergoing TT for GD from July 2008 through April 2012.
Mean age was 42 years (range: 17–78), and 128 patients (77%) were women. The mean BMI was 28 (range 15–59). About 81% of patients were on methimazole, 14% on propylthiouracil, and 59% remained biochemically hyperthyroid at the time of thyroidectomy. Only 3 (2%) patients received potassium iodide preoperatively. Mean operative time was 131 minutes (range 59–271). Mean gland size and blood loss were 41 grams (range 8–180) and 65 mL (range 5–1000), respectively. Median length of hospital stay was 1 day. No patient developed thyroid storm. Mean follow-up was 12 months (range 0–52). Temporary hypocalcemia developed in 50 patients (30%) persisting for >1 year in only 1 (0.6%). Temporary recurrent laryngeal nerve paresis was present in 12 (7%) patients, remaining permanent in one (0.6%). There were one tracheal injury, one hematoma, and 2 seromas. At least one complication developed in 60 (36%) patients. Female gender (Odds Ratio 2.9, p<0.05) and obesity (Odds Ratio 2.3, p<0.05) were independent risk factors for postoperative complications. There were no recurrences.
Although current ATA recommendations for the management of GD call for routine use of potassium iodide and the achievement of euthyroid state before thyroidectomy, this large series demonstrates no appreciable detriment to patient outcomes when these goals are not met. Transient hypocalcemia and hoarseness are frequent complications of TT for GD, but these resolve within six months for most patients. Female gender and obesity are independent risk factors for postoperative complications.
THYROTOXICOSIS DURING PREGNANCY: ETIOLOGIES AND OUTCOME
Disorders of Thyroid Function Friday Poster Clinical
Objective: 1) Examine etiologies of thyrotoxicosis in pregnancy. 2) Examine the relation between maternal anti-TPO antibody and fetal heart rate.
It is a prospective study of 82 patients screened at the departments of endocrinology and obstetrics, in the Calicut Medical College, India. Cases were matched with a control of 100 normal pregnant subjects. Inclusion criteria: Pregnant women during any gestational age with signs, symptoms, and biochemical evidence of thyrotoxicosis. Exclusion criteria: Biochemical evidence of thyrotoxicosis without clinical signs and symptoms. All patients were followed for the gestational period and two months postpartum. History, physical examination, basic investigations with emphasis on thyroid function test, antithyroid peroxidise antibody, ultrasound thyroid, and antenatal ultrasonogram for assessing fetal heart rate were carried out. All patients with Graves' disease and multinodular goiter were treated with propylthiouracil throughout pregnancy. Thirty-five out of 42 patients with gestational thyrotoxicosis required treatment due to significant symptoms, which was restricted to first trimester. Natural course of the disease, fetal response, and intra-/postpartum maternal, and fetal complications were assessed.
Out of 82 patients included in the study, 42(51%) patients had gestational transient thyrotoxicosis, 18(22%) had Graves' disease, 10 (12%) had toxic multinodular goiter. Five (6%) were diagnosed to have lymphocytic thyroiditis, 3 (4%) each had vesicular mole and toxic adenoma, and one patient had papillary thyroid carcinoma. Fetal heart rate was detected with antenatal ultrasound during 16th to 18th week of gestation. Out of 18 patients with Graves' disease, 15 (83%) were antibody positive and the rest negative. In all anti-TPO-positive patients, fetal heart rate was more than 164 compared to 130–145 in antibody-negative patients. Fetal goiter was detected by ultrasonogram in two patients with Graves' disease.
The most common etiology of thyrotoxicosis in pregnancy is gestational-transient thyrotoxicosis followed by Graves' disease. There is a positive correlation between fetal heart rate and maternal circulating anti-TPO antibodies.
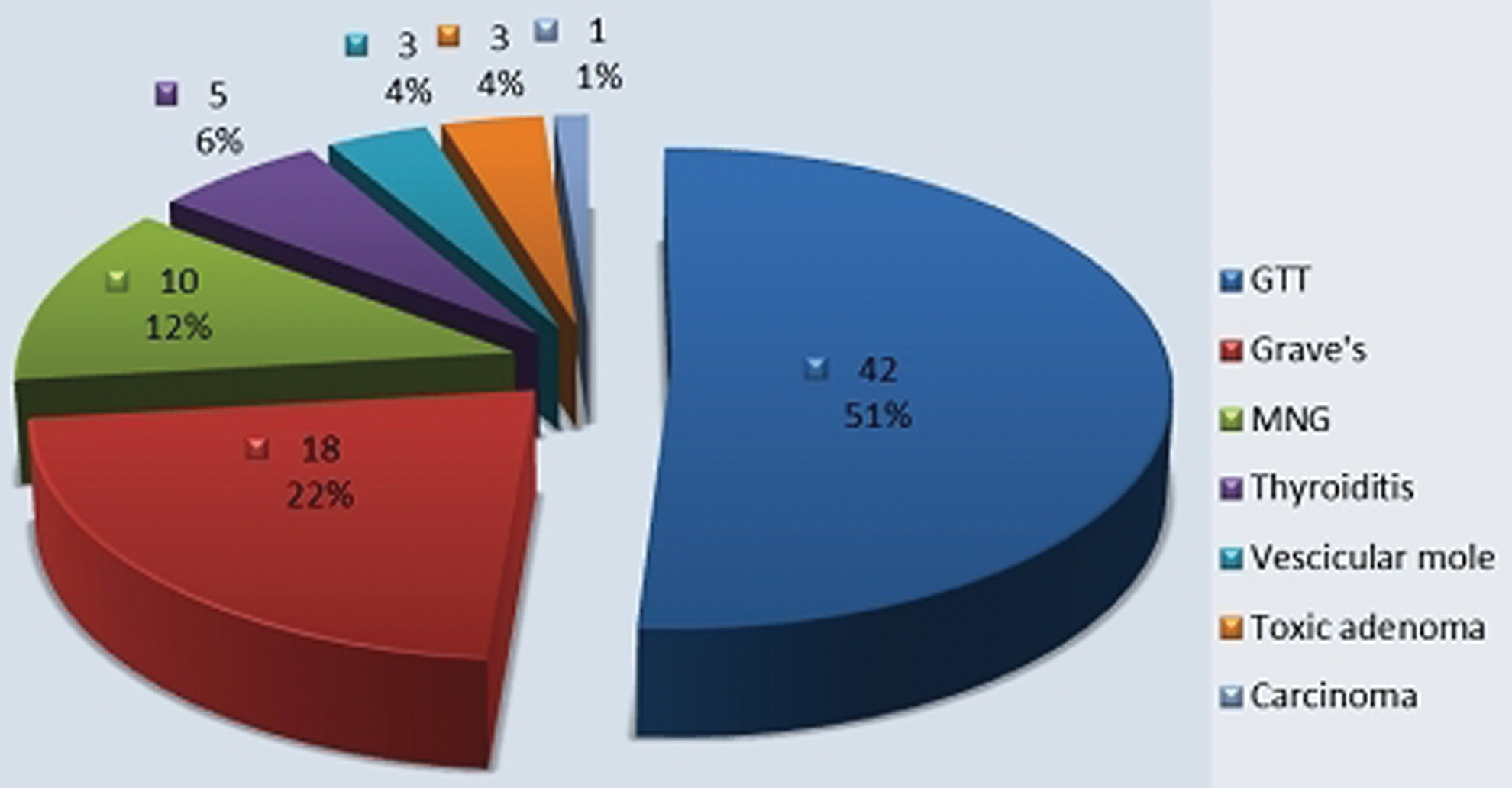
Characteristics of patients included in the study.
Disorders of Thyroid Function Friday Poster Clinical
Objective: To study the impact of SHT in activities of daily living (ADLs) in elderly patients.
Subjects >65-years old (n=187) followed in a from a tertiary ambulatory setting cohort were included. Those in L-T4 use, with overt hypothyroidism (TSH>10 mIU/mL or low serum FT4 [<0, 8 ng/dL]), subclinical, or clinical hyperthyroidism (low serum TSH [<0,4 μIU/mL]), recent use of amiodarone or iodine contrasts was excluded. SHT was defined as serum TSH>4.0 μIU/mL and FT4 0.8–1.9 ng/dL. Functional status was assessed by the Katz Index, which assesses disability in 6 ADLs (bathing, dressing, toileting, transferring, continence, and feeding), with scores from 0 to 6 (independence and total dependence, respectively), and by the Health Assessment Questionnaire (HAQ), which evaluates 8 dimensions (dressing, walking, arising, reach, eating, grip, hygiene, and outside activity), with an index of Disability and Mobility from 0 to 3 (no disability and total disability, respectively). Depressive symptoms were assessed with the Geriatric Depression Scale (GDS-15) and Mini Mental State Examination (MMSE) assessed the cognitive status.
Patients 65–85 years with SHT (n=23) did not differ from euthyroid elderly subjects ≤85-year old (n=119) in respect to KATZ (1.3±1.2 vs. 0.8±1.7; p=0.10), HAQ (1.4±0.9 vs. 1.1±0.9; p=0.16), prevalence of depressive disorder (43.5% vs. 37%; p=0.31), or cognitive deficit (36.4% vs. 52.2%; p=0.17). However, evaluating elderly patients >85 years, those with SHT (n=11) in comparison to euthyroid ones (n=34), had better scores in KATZ (0.7±0.6 vs. 1.4±1.3; p=0.02) and HAK questionnaires (1.1±0.6 vs. 1.7±0.8; p=0.02). There were not statistical differences in the prevalence of depressive disorders (47.1% vs. 81.8%; p=0.10) or cognitive deficits (77.8 vs. 76.7%) in SHT patients >85 years in comparison to euthyroid subjects at the same age.
SHT was associated with better ADLs scores in elderly individuals with 85-year old or more, using the same criteria for subclinical disease for younger patients. There was no difference for cognitive and depression status between the groups evaluated.
Internal Medicine, Tajiri Thyroid Clinic, Kumamoto, Japan
Disorders of Thyroid Function Friday Poster Clinical
Iodine is concentrated and excreted in human breast milk. We assess thyroid function in breast-fed infants whose mothers had Graves' hyperthyroidism and were taking potassium iodide (KI) in Japan (an iodine-rich region).
Forty infants (age 5.5±3.4 months), who were breast-fed while their mothers took KI containing 19–76 mg of iodine daily for Graves' hyperthyroidism, were studied. KI was administered for maternal Graves' hyperthyroidism, because there was a history of adverse effects to antithyroid drugs. Thyroid function in these breast-fed infants was examined at least once during the 1-to-18-month period after the start of KI administration for maternal Graves' hyperthyroidism (total of 64 blood samples from 40 infants). FT4 (normal 0.7–1.5 ng/dL) and TSH (normal 0.5–5.0 μU/L) were tested by the paper filter method using blood specimens obtained by heel puncture with a sterile lancet.
Thyroid function in 34 of the 40 infants was normal (mean FT4 1.14 ng/dL, mean TSH 2.30 μU/L). The remaining six infants had subclinical hypothyroidism (TSH 5.8–8.3 μU/L) 1–2 months after the start of KI administration. In four of these six infants, TSH normalized after one month while the mothers continued taking the same amount of KI. In the other two, TSH became normal with cessation of breast feeding in one case and by reducing the KI dose in the other. There was no relationship between iodine dose and the infant TSH concentration (r=0.01).
This study showed that many mothers can breast-feed with no adverse effects on infant thyroid status during iodine therapy for Graves' hyperthyroidism. However, some infants do suffer from subclinical hypothyroidism. Infant thyroid function should be closely monitored to achieve prompt recovery from this condition.
Second Division, Department of Internal Medicine, Hamamatsu University School, Hamamatsu, Japan
Disorders of Thyroid Function Friday Poster Clinical
The presence of IgG-bound thyrotropin (TSH), called macro-TSH, is a rare phenomenon thought to be due to laboratory interference. TSH-IgG complexes are not efficiently excreted by the kidneys because of their large molecular size, resulting in high accumulation in the serum. Macro-TSH is thought to be immunoreactive, but hormonally inactive, leading to erroneous elevation of the serum TSH level.
A clinical case report from the Hamamatsu University School of Medicine is presented.
A 74-year old man with chronic hepatitis C was referred to this hospital because of suspected thyroid dysfunction. On physical examination, the patient was clinically euthyroid. Laboratory tests showed a markedly elevated TSH [53.8 μIU/L; reference range 0.5–5.0, despite normal free-thyroxine (FT4) and free-triiodothyronine (FT3) levels, measured using the Elecsys platform (Roche Diagnostics)]. Antithyroperoxidase antibody was 0.4 U/mL (reference range: <0.3 U/mL), marginally positive. To rule out RTH, thyroid hormone receptor (TR) β gene analysis and TSH-releasing hormone (TRH) stimulation test were conducted. No mutation of the TRβ gene was identified. TRH test showed delayed TSH and blunted FT3 responses (see Figure). Since assay interference was suspected, the serum sample of the patient was fractionated by HPLC gel filtration. The presence of TSH was illustrated by one peak located at a position consistent with a slightly larger molecular weight than the IgG peak, suggesting macro-TSH. Elution patterns of FT4 and FT3 coincide with those in the control subject.
There has been no report of TRH stimulation test in a patient with macro-TSH. Our patient showed a gradually elevated TSH and blunted FT3 response after TRH administration. It is considered that because of the excess TSH-binding capacity in the patient serum, most native TSH secreted after TRH appeared to form hormonally inactive macro-TSH, which could not elevate serum FT3.
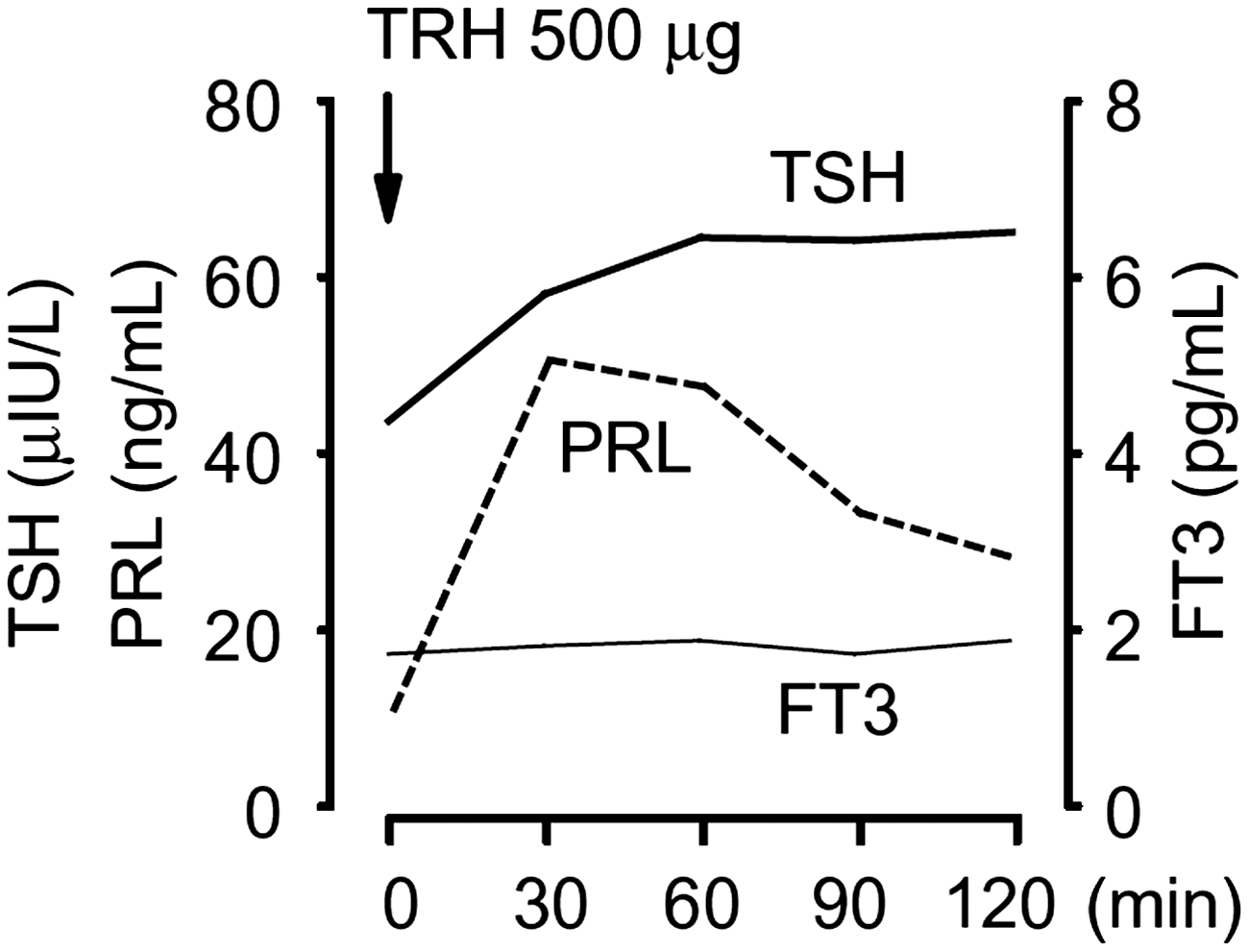
TRH stimulation test.
Thyroid Cancer Friday Poster Clinical
Non-islet cell tumor hypoglycemia (NICTH) is regarded as a major cause of fasting hypoglycemia; it is usually associated with the presence of massive and slow-growing tumors that are mostly of mesenchymal origin such as mesotheliomas, leiomyosarcomas, and fibrosarcoma. Only two cases of thyroid carcinoma associated with NICTH have been previously reported.
A clinical case report is presented.
In March 2000, a 72-year old woman was admitted to this hospital because of respiratory distress secondary to a follicular thyroid carcinoma (FTC). Although a total thyroidectomy was performed, the serum thyroglobulin level remained elevated. Radioactive iodine ablation, using 100 mCi, was administrated twice. The patient developed pulmonary metastases, and surgical resection was performed three times between December 2004 and February 2006. The findings of the histological sections confirmed the diagnosis of pulmonary metastases from FTC. The patient was alive with persistent disease 12 years after the initial treatment. In April 2012, the patient presented to the emergency department because of impaired consciousness (Glasgow Come Scale 11). Laboratory tests showed a low plasma glucose level (34 mg/dL), despite undetectable immunoreactive insulin (IRI), a normal cortisol, and low IGF-I, and GH levels. Computed tomography (CT) scanning revealed multiple massive tumors in the pulmonary fields, bilaterally. The maximum diameter of each lesion was about 1–5 cm. As NICTH was suspected, a serum sample from the patient was fractionated by SDS-PAGE and subjected to Western blot (WB) analysis with anti-IGF-II antibody; most of the IGF-II was detected as high-molecular-weight bands corresponding to big IGF-II. This finding was consistent with the previously reported WB pattern of NICTH. The presence of big serum IGF-II, together with decreased plasma IGF-I, GH, and IRI levels, led to the diagnosis of NICTH. Although no analysis of the pulmonary metastatic lesions, from the FTC, was performed, the absence of any other suspicious lesions on the whole-body CT made the association between FTC and NICTH likely.
This is the third reported case of NICTH associated with thyroid carcinoma.
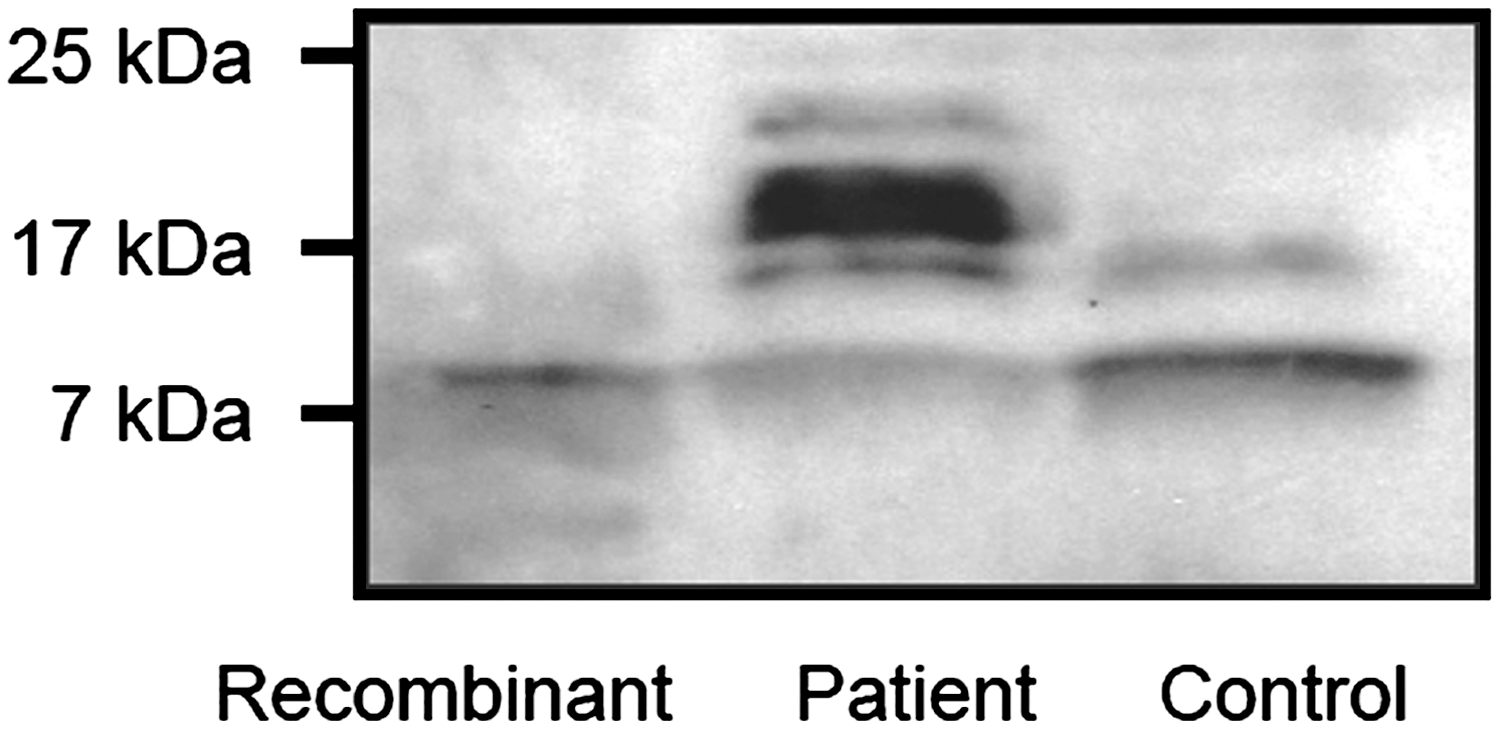
Western blot analysis of recombinant human IGF-II (lane 1), serum IGF-II in the present patient (lane 2), and control subject (lane 3).
Disorders of Thyroid Function Friday Poster Clinical
We report a case of thyrotoxicosis precipitated by a partial molar pregnancy with extremely high hCG>200,000 in a patient with undiagnosed Graves' disease.
A 30 y/o woman presented at 12-week gestation with tachycardia >150. She had no ocular signs of Graves' and no goiter, but had noted episodes of palpitations and tachycardia in the past. She rapidly developed shortness of breath and atrial fibrillation.
TSH was <0.01 μIU/mL (0.49–4.7), FT4>6 μg/dL (0.8–1.8). After being stabilized with IV labetalol and PTU, she was cardioverted. Obstetric evaluation of vaginal bleeding revealed molar pregnancy, and urine hCG was >200,000 mU/mL. She underwent urgent D&C for partial mole. hCG decreased to 88,000 mU/mL the next day. The patient remained on PTU and metoprolol. The hCG level decreased to <5 mU/mL, but 1 month later, T4 was 20 μg/dL (4.5–12), T3 uptake 38.6% (22–35), TSH<0.01 mIU/L (0.4–4.5), FT4 3.6 ng/dL(0.8–1.8), total T3 443 ng/dL (76–181), anti-TPO 207 IU/mL (<35), and TSI 233% (<140). Two months later, T4 13.9, T3 uptake 32%, TSH<0.01 mIU/L, FT4 2.1 ng/dL, and total T3 236 ng/dL. Patient awaits RAI ablation.
High levels of hCG can mimic the action of TSH on the TSH receptor, causing thyrotoxicosis (1,2), but the hyperthyroidism should resolve as the molar pregnancy is successfully treated and hCG levels fall. However, our patient continued to have elevated thyroid hormones 2 months after treatment. In view of her positive TSIg level, she apparently had underlying Graves' disease that was compounded by the thyrotoxic effects of the high hCG levels. We recommend close monitoring of hCG levels and ruling out gestational trophoblastic disease in patients presenting with thyrotoxicosis in pregnancy. This case highlights the importance of close follow-up of cases of hyperthyroidism thought to represent gestational trophoblastic disease, because underlying Graves' autoimmunity might persist.
CONTRAST-INDUCED THYROID STORM IN A PATIENT ON CHRONIC LITHIUM THERAPY: SUCCESSFUL MANAGEMENT AND INSIGHT INTO PATHOGENESIS
Disorders of Thyroid Function Friday Poster Clinical
We report a case of CT contrast-induced thyroid storm in a patient on chronic lithium therapy with previously normal thyroid function.
A 54 y/o man underwent CT head with Omnipaque (iohexol) for chronic hand tremor. He had been on lithium for several years, but lithium levels were never high, and TSH was always normal. There were no recent changes in medications.
Two days before CT, TSH was 1.75 μIU/mL (0.49–4.7) and T4 9.5 μg/dL (4.7–13.3). The day after CT he had agitation, unsteady gait, and neck tenderness. Four days later, he had tachycardia to 114, elevated BP, TSH was undetectable, FT4>6.5 ng/dL (0.7–1.8), total T4>24 μg/dL, and T3 6.5 ng/mL (0.5–1.5). Thyroid ultrasound showed multiple complex nodules bilaterally with no increase in blood flow. His Wartofsky score was 55 with 25 for temperature of 103° F, 20 for CNS effects, and 10 for tachycardia (1). He was treated with propanolol, methimazole, IV hydrocortisone, and lorazepam. Lithium was discontinued, but mental status, tachycardia, and hypertension worsened, and his skin was flushed. He was intubated and put on esmolol drip and propofol drip, and given dexamethasone and SSKI. The same day FT4 fell to 4.7 ng/mL and T3 to 2 ng/mL. He developed aspiration pneumonia, but his total T3 and FT4 and mental status normalized.
Thyroid storm commonly occurs in patients with untreated or undertreated hyperthyroidism, but our patient's TSH was normal only days before storm developed. Hyperthyroidism can occur following iodinated radiocontrast agents, particularly in patients with a nodular goiter and/or low-grade thyroid autonomy, and the patient's thyroid was multinodular on ultrasound. However, massive new hormone synthesis within 4 days seems unlikely. Lithium is well known to increase iodine retention in the thyroid, and patients receiving lithium may be more susceptible to developing iodine-induced hyperthyroidism or silent thyroiditis (2,3). Caution should be used when giving iodinated contrast to patients on lithium, particularly if autoimmune thyroid disease and/or nodular goiter is present. Even if thyroid function is apparently normal, such patients should be closely monitored to aid in the timely detection of acute hyperthyroidism.
THYROID STORM AND FULMINANT HEPATIC FAILURE: REPORT OF TWO CASES AND LITERATURE REVIEW
Disorders of Thyroid Function Friday Poster Clinical
Thyroid storm is a presentation of severe thyrotoxicosis with up to 20–30% mortality rate. Fulminant hepatic failure (FHF) entails encephalopathy with severe coagulopathy in the setting of other symptoms of liver disease. FHF also carries a high mortality rate and ∼60% overall survival for patients undergoing liver transplantation. Fulminant hepatic failure is a rare, but serious, complication of thyroid storm. There are only five previous reported cases with FHF and thyroid storm. We are reporting our experience with two patients with this rare phenomenon.
Two patients presented at our institution with thyroid storm and FHF. Both underwent total thyroidectomy and liver transplantation. The literature was also reviewed to analyze the outcome of five additional cases of concomitant thyroid storm and FHF.
Of the seven total cases of reported fulminant hepatic failure and thyroid storm, two patients died. Only two of the seven patients received thyroidectomy and liver transplant, both at our institution. Both patients who received this treatment survived and were discharged within 10 days after surgery.
Thyroid storm and FHF each independently carry high mortality rates, and managing patients with both conditions simultaneously is an extraordinary challenge. These cases, along with the evidence supporting liver dysfunction in the setting of hyperthyroidism, should compel clinicians to investigate liver function in hyperthyroid patients and to be wary of rapid decline in patients presenting in thyroid storm with symptoms of liver dysfunction. Patients with rapidly progressing thyroid storm and FHF should be considered for total thyroidectomy followed by liver transplantation.
THE ACCURACY OF SURGEON-PERFORMED ULTRASOUND-GUIDED FINE-NEEDLE ASPIRATION IN THE DIAGNOSIS OF THYROID NODULES
Thyroid Nodules & Goiter Friday Poster Clinical
The Bethesda criteria are proposed for appropriate stratification of malignancy risk in thyroid nodules, but controversy exists regarding their accuracy and reliability in the decision making. This study aims to determine the accuracy and outcome of surgeon-performed US-guided FNA in the diagnosis of thyroid nodules using the Bethesda criteria.
A retrospective analysis of US-guided FNAs by a single surgeon during a two-year period was performed. FNA results using Bethesda criteria were compared to final surgical pathology. Additionally, an analysis of nodule size and incidence of malignancy was studied.
FNA results in 212 thyroid nodules were recorded according to the Bethesda criteria: 48% benign, 18% atypia of unknown significance, 16% suspicious for follicular neoplasm, 2% suspicious for malignancy, 5% malignancy, and 10% nondiagnostic. Nodules were malignant 11%, 38%, 29%, 80%, 100%, and 36%, respectively. In size subanalysis, there was no linear trend for malignancy rate across nodule size (p=0.51), with 27% in 1–2-cm, 42% in 2–3-cm, and 19% in >3-cm groups, respectively. A higher false-negative rate was associated with a smaller nodule size (p=0.04).
Surgeon-performed US-guided FNA accurately predicted malignancy risk, and risk stratification was appropriate using the Bethesda system. These data suggest no positive correlation between nodule size and malignancy rate and a higher rate of false-negative benign FNA results with smaller nodules. Surgeon-performed US can guide appropriate initial management and alter management by identification of additional suspicious lymph nodes that require additional comprehensive neck dissection.
Withdrawn
NCEH/DLS/IRAT, CDC, Atlanta, GA
Iodine Uptake & Metabolism Friday Poster Basic
In 2001, the Center for Disease Control and Prevention (CDC) established a program, Ensuring the Quality of Urinary Iodine Procedures (EQUIP), to assist laboratories around the world to assess the accuracy and precision of their urinary iodine procedures. The accuracy and precision of measurements of iodine are important not only to monitor the status of iodine nutrition of populations around the world but also for quality assurance to ensure that accurate data are collected to document efforts to eliminate IDD.
EQUIP urine iodine samples are prepared at CDC and assigned target values using CDC's ICP-MS methodology. Based on the analysis results of the pools and the desired target concentrations, we spike pools using NIST traceable single-element stock standard, if necessary, to obtain concentrations ranging about 10–400 μg/L.
Overall participation in this worldwide program was excellent, with 134 reference laboratories from 70 countries. Most of the participating laboratories use spectrophotometric monitoring of the Sandell–Kolthoff reaction with sample digestion accomplished by using either ammonium persulfate or chloric acid. ICP-MS provides a measurement standard by which other laboratories can assess accuracy and precision when measuring IU.
Since EQUIP was established, our data show the usefulness of the program, supporting the contention that interlaboratory comparisons are an effective tool for laboratory performance improvement. There has been significant improvement in the quality of data from laboratories measuring iodine in different parts of the world. EQUIP will continue to be a tool available to laboratories by encouraging good laboratory practices, providing an assurance of quality data, and also assisting those who are establishing new laboratory or modernizing old ones.
Internal Medicine, University of Nevada, School of Medicine, Las Vegas, NV
Iodine Uptake & Metabolism Friday Poster Clinical
Iodine-containing contrast medium is commonly used for radiologic imaging. When given to hyperthyroid patients, this can result in worsening of their symptoms.
A 52-year-old woman was presented after a fall and altered mental status. On admission, BP was 192/114 mm Hg, and the heart rate was 219/min. She was tachypneic and hypoxic. Patient decompensated and was intubated in the ER. Chest CT with intravenous contrast was done to rule out pulmonary embolism and showed a markedly enlarged thyroid gland. History from family members revealed one year of weight loss, tremors, heat intolerance, and muscle weakness. Workup showed TSH<0.1 μIU/mL, free T3>15 pg/mL, and free T4 4.52 ng/dL. She had positive thyroid-stimulating antibodies. She was treated for thyroid storm with propylthiouracil (started 9 hours after intravenous contrast), saturated solution of potassium iodide, hydrocortisone, and esmolol. She had a prolonged ICU stay with persistent fever, tachycardia, and difficulty weaning her off the ventilator. She eventually recovered, and was extubated and transitioned to methimazole and propranolol.
Patients with Graves' disease and toxic thyroid nodules are at risk of developing thyrotoxicosis after intravenous contrast medium administration. Our patient received 100 mL of Optiray 350, which contains 350 mg iodine per mL of contrast. We believe that this high dose of iodine administered before treatment with antithyroid medication and the delay in initiation of treatment (9 hours in this case) contributed to the worsening of an unrecognized severe hyperthyroidism in our patient. In patients with established hyperthyroidism, unenhanced CT, ultrasound, and MRI should be considered. Caution should be exercised if administration of an iodinated contrast medium is indicated. Prophylactic use of antithyroid drugs should be considered before contrast administration.
Iodine-containing contrasts can exacerbate symptoms in hyperthyroid patients. Alternative imaging modalities should be considered. If iodinated contrast administration is required, prophylactic use of antithyroid drugs is recommended with careful monitoring of symptoms.
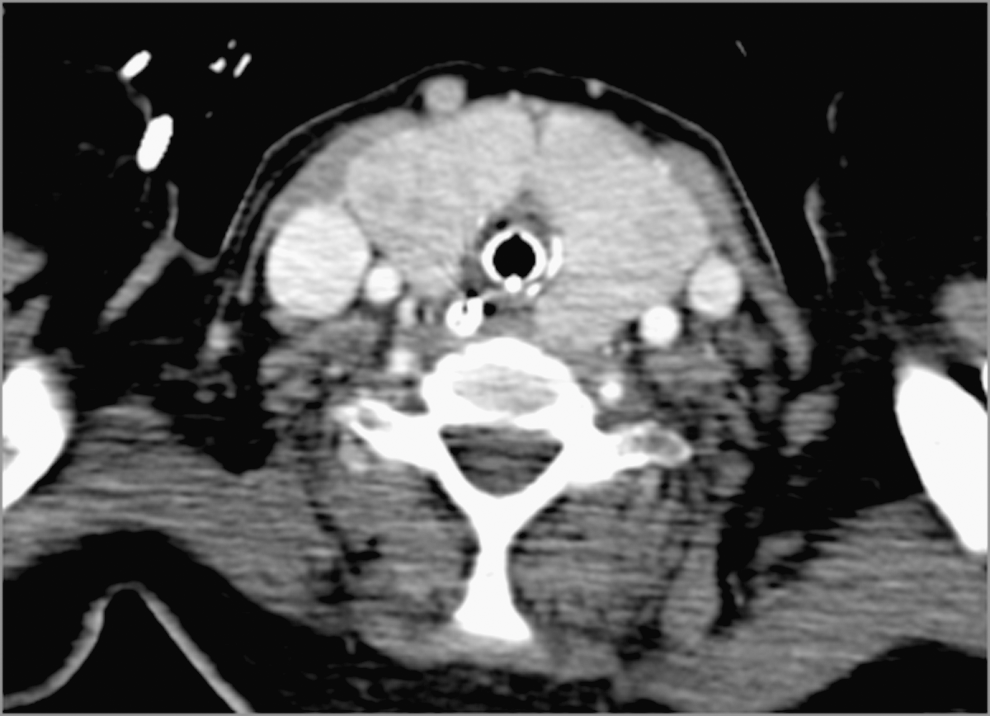
CT chest with IV contrast (there is a markedly enlarged thyroid gland).
Thyroid Cancer Friday Poster Basic
The PTTG-binding factor (PBF) is a relatively uncharacterized gene, which is overexpressed in thyroid tumors. Targeted overexpression of PBF in murine thyroids results in repressed iodide uptake, increased thyroid hormone retention, and significant hyperplasia. Previous research has shown that PBF can bind p53, reducing stimulation of its downstream target genes by competitively binding. Reduced p53 stability was observed when PBF was overexpressed in K1 and TPC-1 thyroid papillary cancer cell lines through increased p53 ubiquitination and subsequent degradation by the proteasome. However, the exact mechanism of this remains unknown.
GST pull-down assays and coimmunoprecipitation assays were used to determine direct protein binding. Half-life assays were used with and without the p53-MDM2-binding competitive inhibitor, Nutlin-3, to investigate protein stability. Ubiquitination was determined via a ubiquitin antibody to immunoprecipitated p53. Immunofluorescence was used to investigate protein subcellular localization.
Pull-down assays demonstrated direct binding between PBF and MDM2, the principal negative regulator of p53. Nutlin-3 inhibition of p53-MDM2 binding blocked the increased degradation of p53 observed when PBF was overexpressed. However, there was no change in p53-MDM2 binding stringency, determined by coimmunoprecipitation, when PBF expression was knocked down by siRNA treatment in K1 and TPC-1 cells. Furthermore, MDM2 subcellular localization was unchanged when PBF was overexpressed. This suggests that another mechanism, other than increased binding or altered subcellular localization, is responsible for the increased MDM2-mediated ubiquitination of p53 elicited by PBF overexpression.
Taken together, these data demonstrate a novel interaction and method of p53 regulation by PBF, mediated by MDM2. Modulation of p53 stability by PBF may be critical in the DNA damage response. Given that PBF potently represses radioiodide uptake, these findings may be particularly pertinent to anaplastic thyroid carcinoma, where p53 is frequently inactivated, and tumors are resistant to radioiodine therapy.
Pathology, University Health Network, Toronto, ON, Canada
Thyroid Cancer Friday Poster Basic
Papillary thyroid carcinoma (PTC) is the most common endocrine malignancy. The diagnosis and classification of this cancer are challenging because of variable criteria. In this study, we aimed to correlate the genotype with morphology to refine the classification of PTCs.
DNA extracted from formalin-fixed paraffin-embedded sections of 129 PTCs was subjected to a panel of 23 multiplexed assays interrogating 286 mutations in 23 genes (AKT1, AKT2, AKT3, BRAF, CDK, CTNNB1, EGFR, ERBB2, FGFR1, FGFR2, FGFR3, HRAS, NRAS, KRAS, KIT, MEK1, MET, NOTCH1, PDGFRA, PIK3CA, RET, SMO, and STK11) on a MassARRAY platform (Sequenom). Mutation calling was determined using TyperAnalyzer software and manual analysis. The status of mutations was compared with histological features.
The results are summarized in the table. There were 68 mutations in 65 tumors (50.4%). Three samples revealed more than one mutation.
Our results demonstrate that BRAFV600E correlates with classical papillary architecture, and BRAFK601E correlates with follicular architecture in PTCs. Most RAS mutations are identified in PTCs that exhibit follicular growth. Although rare EGFR mutations have been described, this is the first report of STK11 mutations in PTC. The presence of STK11 mutations in oncocytic follicular variant PTCs is of interest.
Histological Variants Associated with Each Mutation
(n) designates the total number of mutations detected.
Thyroid Cancer Friday Poster Basic
It has been reported that papillary thyroid cancer has a high incidence of BRAFV600E mutation and thyroiditis; however, how BRAFV600E mutation influences inflammatory cytokines of thyroid carcinogenesis is not certain. The aim of this study was to investigate how two selective inhibitors of BRAFV600E PLX4032 and PLX4720 affect the proliferation and inflammatory cytokine levels of thyroid cancer.
After the two thyroid cancer cell lines TPC1 and 8505C were treated with PLX4032 and PLX4720, the cell growth, cell cycle, the degree of apoptosis, and the levels of inflammatory cytokines were analyzed.
Both cell lines showed a dose-dependent reduction in the growth rate, but had a different IC50 value for PLX4032 and PLX4720. The reaction to the two drugs was more sensitive in the 8505C cells than in the TPC1 cells. Both drugs induced a G2/M phase arrest in the TPC1 cells and a G0/G1 phase arrest in the 8505C cells. Specifically, PLX4032 induced apoptosis only in the 8505C cells. Following the treatment with PLX4032 and PLX4720, the TPC1 cells showed decreased levels of VEGF, GM-CSF, and CCL2/MCP-1, whereas the 8505C cells showed significantly decreased levels of IL-8, Serpin E1/PAI-1, and MMP-3.
PLX4032 and PLX4720 were cytotoxic in both TPC1 and 8505C cells, but induced apoptosis and downregulation of inflammatory cytokines such as IL-8 and MMP-3 in 8505C cells only. These findings suggest the possibility and need to target the inflammatory signaling pathway in the treatment of BRAFV600E mutant thyroid cancer.
A COMPARATIVE ANALYSIS OF ENDOSCOPIC VERSUS CONVENTIONAL OPEN THYROIDECTOMY IN THE TREATMENT OF DIFFERENTIATED THYROID CANCER ACCORDING TO PREOPERATIVE RISK STRATIFICATION
Thyroid Cancer Friday Poster Clinical
Differentiated thyroid cancer (DTC) has a good prognosis and high incidence in young women. Although the low-risk patients might be treated with endoscopic thyroidectomy with the consideration of both the clinician's decision and patient's desire, however, some of the low-risk group occasionally challenges the changes in the risk stratification status during or after surgery. The aim of the study was to review our criteria to select surgical modality and surgical results and to confirm the feasibility of a tailored surgery according to the preoperative risk stratification in the treatment of differentiated thyroid cancer.
From May 2009 to April 2012, we performed thyroid surgery with conventional open or endoscopic method according to the AJCC stage (see Figure). The procedure of endoscopic thyroidectomy was according to the BABA method. In the low-risk group (n=188), patients were divided into two groups according to operation methods (endoscopic group, n=69; open group, n=99).
In the low-risk group (n=188), female patients preferred the endoscopic surgery. The operative time of the endoscopic group was significantly longer than the open group; however, the length of hospitalization was shorter in the endoscopic group, and there was no difference in the complication rates. The mean tumor size was 0.93±0.88 cm and 1.22±0.96 cm in the endoscopic and open group, respectively, which was not significantly different (p=0.054). There were no significant differences in the Off T4–thyroglobulin level between two groups. Six patients of the low-risk endoscopic group challenged the changes (1=central lymph node metastasis; 5=minimal extrathyroid extension) in postoperative the risk stratification status, but there was no change in surgical modality from preoperative plan during or after surgery, because we could perform total thyroidectomy and central lymph node dissection in the high-risk conversion group safely.
Endoscopic thyroidectomy is a feasible method for treatment of selected cases of thyroid cancer such as, low-risk group, according to the preoperative risk stratification.
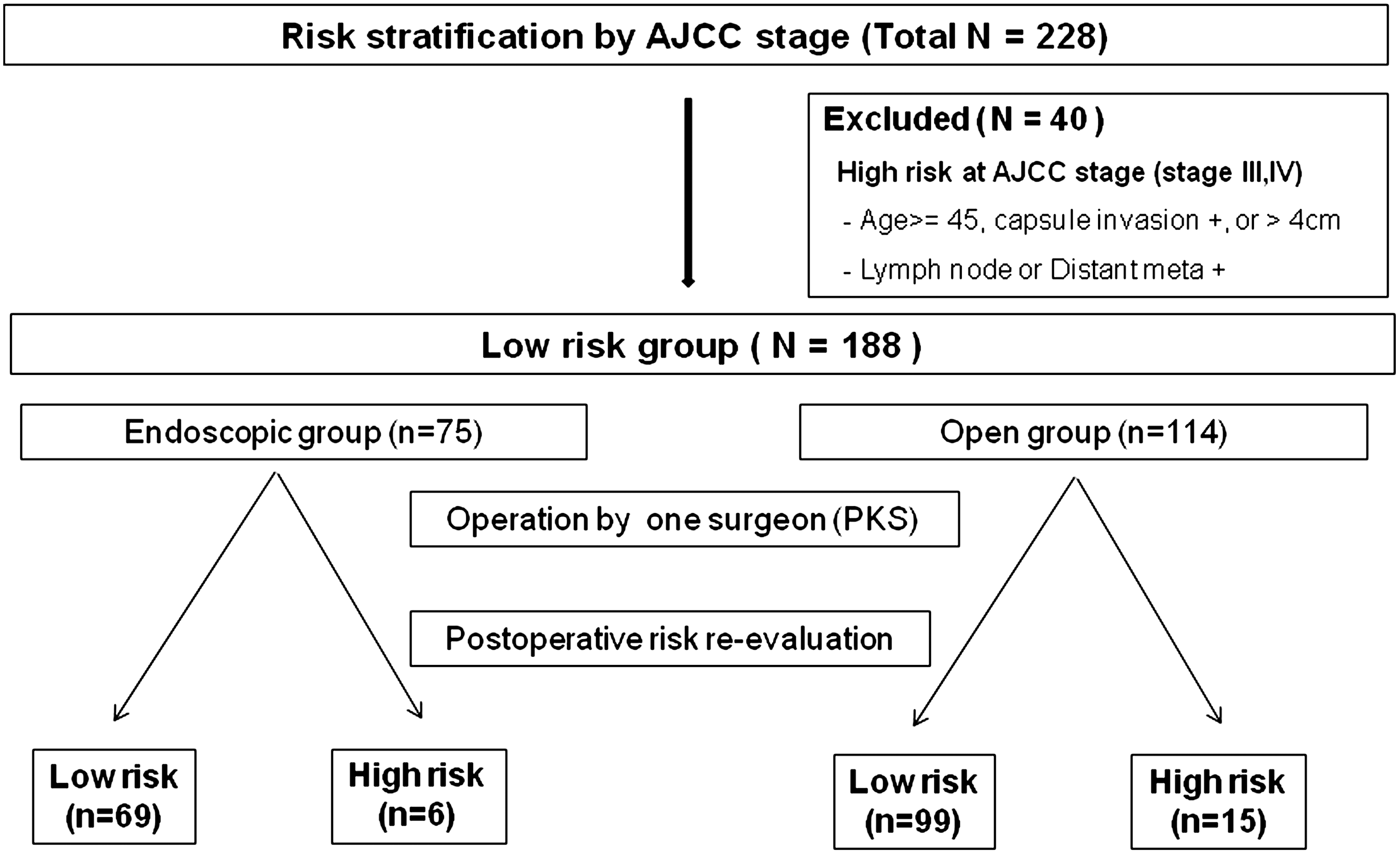
Tailored thyroid surgery according to risk stratification by the AJCC Stage.
Thyroid Cancer Friday Poster Translational
Papillary carcinoma is the most common type of thyroid cancer, and its accurate diagnosis in thyroid nodules is important. Mutations that occur most frequently in thyroid cancer thus are typically included in diagnostic panels are BRAF V600E and K601E, NRAS codon 61, HRAS codon 61, and KRAS codon 12/13 point mutations and RET/PTC1, RET/PTC3, and PAX8/PPARγ rearrangements. The prevalence of these and other less-common mutations has not been studied in a large series of tumors.
We analyzed 501 consecutive papillary carcinomas from 480 patients for the commonly tested mutations as well as for rare mutations, including NRAS codon 12/13, HRAS codon 12/13, and KRAS codon 61 point mutations, rare types of RET/PTC rearrangement, NTRK1 gene rearrangements, and BRAF exon 15 point mutations and BRAF/AKAP9 rearrangement. Point mutations were detected by real-time PCR and fluorescent melting curve analysis and Sanger sequencing. Rearrangements of PAX8/PPARγ, RET/PTC1, and RET/PTC3 were detected by TaqMan real-time PCR assays. BRAF/AKAP9 was detected by amplifying the fusion product. NTRK1 and all types of RET rearrangements were detected using RT-PCR as the preferential expression of the tyrosine kinase domain.
Of 501 tumors, 456 had sufficient material available for informative molecular testing. Of those, 317 (69.5%) tumors were found positive for commonly tested mutations, including 184 BRAF V600E (40.4%), 82 NRAS 61 (18%), 33 HRAS 61 (7.2%), 2 KRAS 12/13 (0.4%), 7 RET/PTC1 (1.5%), 4 RET/PTC3 (0.9%), and 5 PAX8/PPARγ (1.1%). In addition, we detected 17 (3.7%) rare mutations, including 7 KRAS 61, 2 HRAS 12/13, 1 NRAS 12/13, 3 NTRK1 rearrangements, 2 rare RET rearrangements, and 3 rare BRAF rearrangements or point mutations. There were 121 (26.5%) cases negative for mutations.
Our analysis of a large series of papillary carcinomas reveals that common mutations are found in 69.5% of tumors, whereas additional known point mutations and rearrangements can be additionally detected in 3.7% of tumors. These mutations, with KRAS codon 61 mutation and NTRK1 rearrangements most prevalent, should be added to the routine mutational panel to improve the detection of papillary carcinoma in thyroid fine-needle aspiration samples.
Cancer Biology, Mayo Clinic, Jacksonville, FL
Thyroid Cancer Friday Poster Translational
Follicular thyroid carcinoma (FTC) is a well-differentiated cancer that encompasses 15%–20% of all thyroid cancers, and invasion is frequently seen in the vascular structures within the thyroid gland and neck. FTC is associated with up to 40% of all thyroid cancer-related deaths with no curative treatments beyond surgery and 131I. We report three new authenticated FTC cell lines (SDAR1, SDAR2, and SDAR3) from a patient diagnosed with metastatic FTC to a lymph node and neck. A fourth FTC cell line (THJ-306T) was derived from another FTC patient, each with features of radioiodide-insensitive tumors.
Cell lines were developed. Validations studies included short tandem DNA repeat (STR) analysis, measurement of thyroid-specific genes by RT-PCR, DNA mutation analysis by RT-PCR, and Western analysis of oncogenes. Cell proliferation and cell death assays were performed to examine antitumor synergy of combined Akt and MEK inhibitors.
STR validated that the cell lines were derived from the patient tumor tissues. The SDAR cell lines were not mutated for retinoblastoma (Rb), PTEN, KRas, HRas, PI3K, BRAFV600E, or PAX8/PPAR. However SDAR1 was mutant for p53. Expression of Pax8 and TSHR mRNA was present, while PDS, DIO2, TPO, and NIS were absent. For the fourth FTC cell line, THJ-306T contained Rb and NRas mutations and expressed only TTF1 and Pax8 mRNA. The oncogenic signaling pathways, pERK and pAkt, were elevated in all four cell lines. We thus tested and demonstrated antitumor synergy using an MEK inhibitor combined with an Akt inhibitor. Combinatorial Index values (<1=synergy) were 0.071, 0.29, 0.24, and 0.29, respectively, for SDAR1, SDAR2, SDAR3, and THJ-306T. Propidium iodide measurement of cell death revealed antitumor synergy. pERK and cyclin D1 inhibition was validated for the MEK inhibitor, while loss of Akt Ser473 phosphorylation was verified for the Akt inhibitor.
Thus, inhibiting two oncogenic pathways in novel FTC cell lines demonstrated strong antitumor synergy and may provide a rationale for clinical trial design. We are now examining the role of RhoB in the observed synergy as well as exploring whether these cells when exposed to combinatorial therapy respond to iodine uptake and retention.
Medicine, Laboratory of Cancer Molecular Genetics, Faculty of Medical Sciences, University of Campinas (Unicamp), São Paulo, Brazil., Campinas, Brazil
Thyroid Cancer Friday Poster Translational
B7-H1 is widely expressed in tumor cells and has been demonstrated to mediate T-cell inhibition, but its role in thyroid tumor progression and its clinical potential as a marker of prognosis are still not clear.
We analyzed formalin-fixed paraffin-embedded thyroid tissue samples from 407 patients (340 women and 67 men, 43.6±15.9 years old), including 253 papillary thyroid carcinomas (PTC) and 40 follicular carcinomas, managed according to a same standard protocol, 58 nodular goiters, and 56 follicular adenomas. In addition, there were 5 normal thyroid tissues. Also, we obtained fresh thyroid tissue samples from 85 out of the 293 differentiated thyroid carcinoma (DTC) cases and from 31 of the benign thyroid lesions. Aggressiveness at diagnosis was ascertained using the TNM and stage classification systems for DTC. Patients were followed-up for 12–298 months (43.50±33.29 months). According to their serum Tg levels and other lines of evidence, they were classified as no evidence of disease (233 cases) or persistence of disease/recurrence (60 cases, including 10 deaths). B7-H1 expression was assessed and quantified using an immunohistochemistry quantitative method. B7-H1 mRNA expression was measured by a quantitative real-time PCR assay.
Malignant tissues presented higher B7-H1 staining levels than benign tissues (p<0.0001), and PTC cases (37.7859 AU) had higher B7-H1 staining levels than goiters (21.0166 AU; p=0.0004). Tumors with concurrent chronic lymphocytic thyroiditis (CLT) presented higher B7-H1 levels than tumors without CLT (p=0.00647). DTC also presented higher B7-H1 mRNA levels (52952.3 AU) than benign tissue (18771.4 AU; p<0.0001). Tumors classified as stage II–IV presented higher B7-H1 mRNA levels than stage I tumors (p=0.03522). We observed a positive linear correlation between age at diagnosis and B7-H1 mRNA levels (p=0.02896). However, a log-rank test failed to show B7-H1 as a prognostic marker.
Our data suggest that B7-H1 expression is associated to features of thyroid tumor aggressiveness, confirming its possible role in the immune evasion process. We suggest that B7-H1 could be a target for immunotherapy in patients with poor prognosis characteristics.
Thyroid Center: Division of Endocrinology and Diabetes, Children's Hospital of Philadelphia, Philadelphia, PA
Thyroid Cancer Friday Poster Translational
Medullary thyroid carcinoma (MTC) is uncommon in children and generally associated with mutations in the RET proto-oncogene. Few causative genetic alterations have been identified in RET(-) MTC. We describe a case of RET(-) MTC associated with chromothripsis, a catastrophic genetic rearrangement associated with carcinogenesis.
Whole-genome SNP array, RET gene sequencing.
An 11-year-old healthy male child presented with an incidental thyroid nodule noted on physical examination. He reported several weeks of anorexia and nausea. Family history of endocrine disease or malignancy was negative. Examination revealed a right-sided thyroid nodule without cervical lymphadenopathy and an absent MEN 2B phenotype. Ultrasound revealed a 2.9-×1.9-×2.4-cm solid, hypoechoic, and hypervascular nodule without microcalcifications or lymphadenopathy. FNAB demonstrated a cellular lesion composed of spindle cells. Calcitonin (Ct) and carcinoembryonic antigen were 4,421pg/mL (normal<6pg/mL) and 80.8 ng/mL (normal<2.5 ng/mL), respectively. Preoperative staging demonstrated no regional or distant metastases. Total thyroidectomy and central neck dissection confirmed MTC confined to the thyroid. Ct decreased to <5pg/mL postoperatively. Germline and somatic RET proto-oncogene testing was negative. Whole-genome SNP array demonstrated chromothripsis of chromosome 1p, all of chromosome 4, and loss of one copy of chromosome 9.
Chromothripsis describes a single, catastrophic shattering of a chromosome with subsequent attempted repair. Surviving cells emerge with a mutated genome conferring tumorigenic advantage through disruption of tumor suppressor genes or activation of oncogenes. We present the first case of RET(-) MTC with chromothripsis of chromosomes 1p and 4. While the incidence or impact of chromothripsis in MTC tumorigenesis is not known, deletions of chromosome 1p, 4, and 9 are associated with sporadic MTC. One potential target of this event may be altered expression of the SDHB gene, found in 23% of sporadic MTC and located on chromosome 1p36.1-p35. Further studies are underway to determine if altered expression of SDHB or RET occurred and to determine whether the presence of 1p and 4 chromothripsis may be common in sporadic RET(-) MTC.
Genetics, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia
Thyroid Cancer Friday Poster Translational
The activating gene mutations in the mitogen-associated protein kinase (MAPK) signaling pathway, such as RET/PTC rearrangement, RAS, and BRAF mutation, are considered to be mutually exclusive in papillary thyroid carcinoma (PTC). However, concomitant mutations in RET/PTC and BRAF have been reported recently. Their association with disease progression has not been investigated.
To investigate the frequency of concomitant mutations in PTC from an Arab population and its association with disease progression, we studied 67 PTC samples (61 classic PTC, 3 tall-cell variants, and 3 follicular variants of PTC) by DNA sequencing analysis of BRAF exon 15, all coding exons of KRAS, NRAS and HRAS, and RT-PCR-sequencing analysis of RET/PTC transcripts.
BRAFV600E mutation was detected in 32 of 61 classic PTC and in all three tall-cell variants (52%, 35/67). KRAS mutation was detected in 2 classic PTC samples (3%, 2/67) and NRASQ61R in one classic PTC and 2 FVPTC (4%, 3/67). RET/PTC-1 rearrangement was detected in 11 PTC (16%, 11/67). Dual mutations of BRAFV600E and KRAS were found in 2 classic PTC samples. Dual mutations of BRAFV600E and RET/PTC-1 were detected in 5 classic PTC samples and one tall-cell variant. Two NRASQ61R-positive FVPTC samples also contained RET/PTC-1 rearrangement. In total, 10 concurrent mutations were found in 67 PTC samples (15%), and most of them were in advanced disease stage (7/10, 70%).
Concurrent mutations in the MAPK pathway are frequent events in advanced PTC, and may represent intratumor heterogeneity. They may offer a gene dosage effect and contribute to disease progression. Acknowledgement: Supported by the KACST Biotechnology grant# 10-BIO957-20
Research and Technology Development, Asuragen, Austin, TX
Thyroid Cancer Friday Poster Translational
Cytological examination of fine-needle aspiration (FNA) biopsies is the standard preoperative tool to detect thyroid malignancies and identify patients requiring surgery. However, in 20% to 40% of cases, FNA cytology cannot distinguish between benign and malignant follicular lesions. The samples are considered indeterminate for malignancy, and as a consequence, a number of unnecessary surgeries are performed every year in the United States. Studies have shown that molecular testing for the most common mutations and translocations observed in thyroid cancer significantly improves the accuracy of preoperative FNA diagnosis by cytology. Testing for BRAF, RAS, RET/PTC, and PAX8/PPARγ was formally recommended in the 2009 Revised ATA thyroid cancer guidelines for patients with indeterminate cytology. Here, we present an interim analysis of the first prospective, blinded, multisite clinical study to validate miRInform® Thyroid, a testing service performed preoperatively on the ATA-recommended panel to assist in resolving indeterminate FNA cytology.
Thyroid FNAs were prospectively collected in RNARetain®, a single-use vial containing a nontoxic solution for the preservation and stabilization of intracellular nucleic acids (Asuragen, Inc.). Specimens were then shipped at room temperature to Asuragen's CLIA lab, where DNA/RNA extraction and molecular testing were performed using multiplex laboratory-developed tests for the ATA-recommended markers. Cytological evaluation was performed before molecular testing and blinded.
From June 2010 to March 2012, a total of 624 FNA samples were collected at 5 independent US sites and tested in Asuragen's CLIA lab. Among the 522 FNAs with known cytological diagnosis, 376 were benign (72%), 88 were indeterminate (16.8%), 21 were malignant (4%), and 37 were nondiagnostic (7%). Mutations were identified in 61 specimens (11.6%). Mutations in the RAS genes were the most common (5.5%), followed by BRAF (4.2%), and PAX8/PPARγ translocation (1.9%).
Accrual of additional samples and collection of outcome data are ongoing. Correlation between cytological examination, histological diagnosis, and molecular testing is in progress and will be presented.
Department of Biostatistic and Epidemiology, Institut de Cancérologie Gustave Roussy, Villejuif, France
Thyroid Cancer Friday Poster Clinical
The randomized phase III ESTIMABL trial (N Engl J Med, 2012;366:1663–1673.) reported an equivalent ablation rate in low-risk thyroid cancer patients for both 131I activities (1.1 GBq or 3.7 GBq) and for both TSH stimulation methods (thyroid hormone withdrawal [THW] or recombinant human thyrotropin [rhTSH]). We report here the cost–effectiveness assessment of these strategies, based on data collected as part of the trial.
The consumed resources included rhTSH, hospitalization for 131I ablation, transportation, and sick leaves, which were prospectively collected for each patient from randomization until 8 months after 131I administration. Costs were assessed from the societal perspective. Quality-adjusted life years (QALYs) were calculated using EQ-5D scores before randomization, at radioiodine ablation, at 2, 4, and 6 weeks and then at 3 and 8 months after 131I.
Results from 2007 to 2010, 752 patients (78% women mean age of 49 years) were included in 24 French centers. A significant deterioration of quality of life (utility score) was observed in patients stimulated by THW, as compared to patients stimulated by rhTSH, both at time of radioiodine ablation and two weeks later (p<0.01). Over the period, the number of QALY was, respectively, estimated at 0.855, 0.864, 0.855, and 0.852 for the strategies 1.1 GBq-rhTSH, 3.7 GBq-rhTSH, 1.1 GBq-THW, and 3.7 GBq-THW, with no difference between groups. The administration of 1.1 GBq allowed a shorter length of hospitalization for ablation, as compared to the administration of 3.7 GBq (respectively, 2.2 and 3.1 days). Total cost of management was, respectively, estimated at 7 172€, 8 976 €, 7192 €, and 7 522 € for the strategies 1.1 GBq-rhTSH, 3.7 GBq-rhTSH, 1.1 GBq-THW, and 3.7 GBq-THW.
The strategy combining 1.1 GBq and rhTSH allows to avoid quality of life deterioration, reduce the length of hospitalization for ablation, and is slightly less expensive than the other strategies.
Department of Diagnostic Ultrasound, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, China
Thyroid Cancer Friday Poster Clinical
No conventional imaging method reliably distinguishes between benign and malignant thyroid nodules. The main aim of this multicenter prospective study was to determine the clinical value of SonoVue_administration for the characterization of thyroid nodule detected in conventional ultrasound not fully characterized.
Two hundred forty-five patients scheduled for surgery for thyroid nodules detected by conventional sonography not fully characterized were enrolled in this prospective study. The diagnostic performance of contrast-enhanced ultrasound (CEUS) in comparison with histology as gold standard was evaluated by blinded off-line assessment. In all, there were 135 benign nodules (105 hyperplasia nodule, 21 follicular adenomas, 5 Hashimoto's disease,1 hyperplasia and granuloma, 1 subacute thyroiditis, 1 suture granuloma, and 1 fat and connective tissue) and 125 malignant nodules (114 papillary carcinomas, 6 follicular carcinoma, 3 medullary carcinomas, 1 metastatic carcinoma, and 1 NHD). The enhancement patterns were classified into one of four patterns by two experienced readers.
In the differentiation between benign and malignant lesions, CEUS yielded a sensitivity of 79.4%, a specificity of 88.1%, a positive predictive value of 89%, and a negative predictive value of 88.4%. About 71.9% benign nodules presented ring enhancement and 87.2% malignant nodules presented heterogeneous enhancement, and the difference is of statistically significant (p<0.05). There were no significant differences between follicular carcinoma and adenoma (p>0.0.5).
These results indicate that CEUS using SonoVue is a competitive and effective diagnostic tool for the characterization of thyroid nodule.
Head and Neck Service, MSKCC, New York, NY
Thyroid Cancer Friday Poster Clinical
Poorly differentiated thyroid cancer (PDTC) accounts for only 2%–5% of all thyroid cancers. Our objective was to report outcomes in a large series of patients with PDTC treated at a single tertiary cancer center.
Retrospective review of thyroid cancer patients treated primarily at MSKCC in 1986–2009 identified 91 patients with PDTC. Histopathological diagnosis was confirmed by review of two independent pathologists. Patient, tumor, and treatment characteristics were recorded and outcomes calculated by the Kaplan–Meier method. Of 91 patients, 62% were women. Median age was 59 (range 16–93). About 90% of patients had total or extended total thyroidectomy, and 10% had lobectomy. Eighteen patients (20%) had central and 23 (25%) both central and lateral neck dissection at initial surgery. Primary tumor staging included 4 patients (4%) with pT1, 14 (16%) pT2, 45 (49%) pT3, and 28 (31%) pT4a. Six patients (15%) had pN0 neck, 12 (29%) had pN1a, 22 (54%) pN1b, and 1 patient had no specified location (N1×). Twenty-four patients (26%) presented with distant metastases; 12 to lung, 6 to bone, and 6 to lung and bone. Seventy patients (77%) had adjuvant therapy: 63 (70%) RAI only, 3 (3%) postoperative radiation (PORT) only, and 4 (4%) both RAI and PORT.
With median follow-up of 50 months (range 1–215 months), the 5-year overall survival (OS) and disease-specific survival (DSS) were 62% and 66%, respectively. Overall, 23 patients (25%) had persistent disease, and additional 17 developed recurrences: 1 local and distant, 2 regional, 5 distant, 2 local, regional and distant, and 7 regional and distant. The 5-yr local and regional controls were excellent (90% and 83%, respectively). However, distant control was poor with 40% having distant disease at 5 yrs: 23 patients presented with, and additional 15 developed, distant disease. Twenty-seven patients died of disease: distant disease accounted for 22 deaths, locoregional recurrence in 4 cases, and locoregional and distant in 1 case.
Patients with PDTC have a poorer outcome than WDTC. With appropriate surgery and adjuvant therapy, excellent locoregional control can be achieved. Disease-specific deaths occurred in a majority of patients due to distant metastases and rarely due to uncontrolled locoregional recurrence.
Withdrawn
A BIG FAMILY WITH VERY LOW-RISK FAMILIAL MEDULLARY THYROID CARCINOMA (FMTC) WITH 666-CODON MUTATION IN THE REARRANGED-DURING-TRANSFECTION (RET) GENE
Thyroid Cancer Friday Poster Clinical
FMTC is a variant of MEN2A with multigenerational MTC without pheochromocytoma (PHE) nor primary hyperparathyroidism (PHP). The RET gene on chromosome 10 codes for a tyrosine kinase receptor. Gain-of-function germline RET mutations are causally linked to MEN2A and FMTC. The clinical problem is the risk of MTC at very young age. Timing of prophylactic thyroidectomy is decisive. Greater than 25 mutations have been described with a wide spectrum of aggressiveness of MTC. The ATA guidelines define 4 classes of mutations from A (lowest risk; operation at >5 years of age possible) to D (very aggressive; operation <1 year).
The index case was discovered as a cold nodule with calcitonin (CCT)=480. An in-frame insertion deletion mutation in exon 11 in codon 666 (c1998delGinsTTCT) was detected (first described by Vandenbosch in 2005). In 2006, in Belgium, 4 cases in 4 unrelated families were known with 7 carriers without evidence of MTC. The undermentioned family was invited for an information session and blood sampling for genotyping. Carriers were invited for intake with CCT, CEA, parathormone testing, and ultrasound and 24-h catecholaminuria.
No cases of PHE nor PHP. Generation (G) 1: 6 siblings °1916–1928, all died, none from MTC; no genetic testing; ≥4/6 should have been carrier (carriers in their offspring!). For one branch, the first child is now being tested. G2: 4 carrier branches: 21 offspring involved (°1946–1966); 3 dead; 17 tested: 10+, 7−; 1 not tested; 4 operations with preop CCT 111/680/318/480 and all postop CCT<13; all 4 mutifocal MTC, no positive lymph nodes. 6 other carriers: 1 died from breast cancer with CCT=580; other 4 CCT ranging 6–21; 1 no CCT available. G3: 10 carrier branches: 31 offspring involved (°1968–1989); 0 dead; 26 tested: 13+, 13−; 5 not tested; 1 operation with preop CCT=32 (unilateral 5 mm) and postop CCT=1.7. CCT<16 in 12 other carriers. G4: 13 carrier branches: so far 16 offspring; 0 dead; none tested.
This big family illustrates the very indolent behaviour of the codon-666 (c1998delGinsTTCT) mutation. There have been no fatalities, no cases of metastasized MTC, and no residual disease in the operated cases. We suggest an A-minus score in the ATA guidelines for this mutation.
HIGH T3/T4 RATIO (R) IN 2 PATIENTS (P) WITH DIFFERENTIATED THYROID (T) CANCER
Thyroid Cancer Friday Poster Clinical
In thyroidectomized p., without tumor load, exogenous T4 is the only source of T4 and T3. Serum T4 reflects both uptake of administered dose and T4-deiodination (d) to rT3 and T3. Serum T3 reflects T4-d and T3-d to T2. Three types of human deiodinase (D): cfr table.
2 p. with increased R, probably due to increased D. Activity in 2 different settings: case 1: A 54-y-old woman, T2N0 pap. Ca. in a 25 g T, neg. AB: thyreoidectomy and ablation 131I: preop. T4=13.7 pmol/L (7–16); T3=4.7 pmol/L (3.8–6); R=0.34; d8 postop. R=0.43 under 150 μg T4; preablation R=0.60; TSH=0.03; TG=3.7 after ablation TSH=0.15, T4=13, T3=8.9, and R=0.66 under 175 μg T4. No T hormone production postop: very low TG, minimal iodine uptake in T bed after ablation. Case 2: A 79-y-old woman with TxN1bM+foll. Ca: 4 years after subtotal thyreoidectomy presenting neck and mediastinal lymph nodes and lung mets; central+lateral neck dissection; 2 ablations with 131I; TG AB+, stable; TG rising (1200–2800). TSHrAB+ and rising: thyroidectomy: pre-R=0.5; post-R=0.22; neck dissection: pre-R=0.65; post-R=0.49; preablation 2: R=0.60. No evidence of T hormone production: low iodine uptake in T bed after ablation; fast T4 drop at withdrawal; suppression with 225 μg T4.
Case 1: increase of R preop versus postop with no endogenous T4/T3 production. Ceteris paribus, this could be due to perop. Disappearance of thyroidal D1 and D2 activity, inducing activity change of D1 (liver and kidney) and/or upregulation of D2 (skeletal muscle). PTU inhibition of D1 (10 days) did not change R, nor rT3. This could mean that D1 activity is not so important, or D2 and D3 activities rise to compensate. Case 2: increase of R with tumor load (op. 1 and 2) with no evidence of endogenous T4/T3 production. This could be due to overexpression of D1 or D2 in tumor; D2-overexpression has previously been found in advanced following Ca. Here no effect of PTU inhibition of D1, so probably no overexpression of D1. TSHrAB is unclear: overexpression of TSH receptor in the cytoplasm in T cancer has been described.
High R in T cancer in 2 different settings with different explanations. In follow-up of T cancer, T3 should be monitored. Endogenous production of T4/T3 in tumor has to be excluded.
Three Types of Deiodinase
Otolaryngology-Head & Neck Surgery, McGill University, Montreal, QC, Canada
Thyroid Cancer Friday Poster Clinical
Confidently predicting locoregional metastasis in well-differentiated thyroid carcinoma (WDTC) has consistently been of primary concern in thyroid cancer management. Sentinel lymph node (SLN) biopsy (SLNB) has recently been shown to be an effective predictive tool. To our knowledge, primary tumor (T) classification has yet to be studied with regard to SLNB outcomes. We hypothesized that larger primary tumors would be correlated with the rate of malignancy in SLNBs.
Data were collected from patients operated for WDTC at the McGill University Thyroid Cancer Center. Our primary inclusion criteria were patients having undergone a total thyroidectomy with SLNB for a WDTC with no distant metastasis. Statistical analyses were performed using a Pearson χ2 test and a Pearson Correlation Coefficient, with a p value of<0.05 considered as statistically significant.
Overall, 68 patients were included in our study and separated into two groups (48 with negative SLNBs and 20 with positive SLNBs). No statistically significant difference was found between the two groups when looking at gender (p=0.426) and age (p=0.973). T classification in patients with negative SLNBs was 60.42% T1, 20.83% T2, 16.67% T3, and 2.08% T4, whereas patients with positive SLNBs had 15%, 5%, 45%, and 35%, respectively, yielding a statistically significant difference (p<0.001) between the two groups. Furthermore, a statistically significant correlation was found between T classifications and SLNB outcomes (r=0.583; p<0.001), such that higher T classifications were positively correlated with SLNB malignancy.
Our findings show that patients with higher T classifications are more likely to have a positive SLNB outcome. As a result, we recommend the use of the Primary Tumor Classification to assess the risk of locoregional metastasis in WDTC.
N1B DISEASE AT PRESENTATION IN PATIENTS >45YRS WITH PAPILLARY THYROID CANCER PREDICTS FOR DISTANT RECURRENCE AND POORER OUTCOME
Thyroid Cancer Friday Poster Clinical
Many risk stratification systems (GAMES/MACIS/AMES) have been developed for patients with papillary thyroid cancer (PTC). All recognize the importance of age and the presence of distant metastases. Primary tumor factors such as size, presence of extrathyroid extension, and aggressive histological features are also recognized, but the presence of nodal metastases generally is not. The impact of nodal metastases on survival is controversial, but appears to be more significant in older patients. The objective of this study was to determine the impact of clinical nodal metastases at presentation on outcome in patients >45 yrs of age.
The records of 799 patients>45-years old with PTC and without distant metastases treated at MSKCC in 1985–2005 were analyzed. Five hundred sixty-two were women (70%); 400 were pT1 (50%), 103 pT2 (13%), 225 pT3 (28%), and 71 (9%) pT4; 583 (73%) were N0; and 216 (27%) were N1. Disease-specific survival (DSS) and recurrence-free survival (RFS) were determined for patients with N0, N1a, and N1b disease using the Kaplan–Meier method.
With a median follow-up of 54 months, the 5y DSS and RFS were 99% and 94%, respectively. There were 17 deaths and 49 recurrences (3 local, 33 regional, and 27 distant). When stratified by N stage, 5y DSS was 100%, 100%, and 91% for N0, N1a, and N1b disease, respectively, p<0.001. The 5y RFS was 98%, 91%, and 79% for N0, N1a, and N1b, respectively, p<0.001 (see Figure). There was a significant difference in local, regional, and distant RFS between N0, N1a, and N1b patients (100%, 99%, and 99%, p=0.004; 99%, 92%, and 91%, p<0.001; and 99%, 100%, and 85%, p<0.001, respectively). No patients died of uncontrolled locoregional recurrence. All deaths were due to distant metastases.
Patients with PTC over 45 yrs of age with N1b disease at presentation have a poorer DSS and RFS compared to patients with N0 or N1a disease. The cause of death is due to distant recurrence rather than locoregional recurrence. N1b disease at presentation in patients >45 yrs predicts for distant recurrence and poorer outcome.
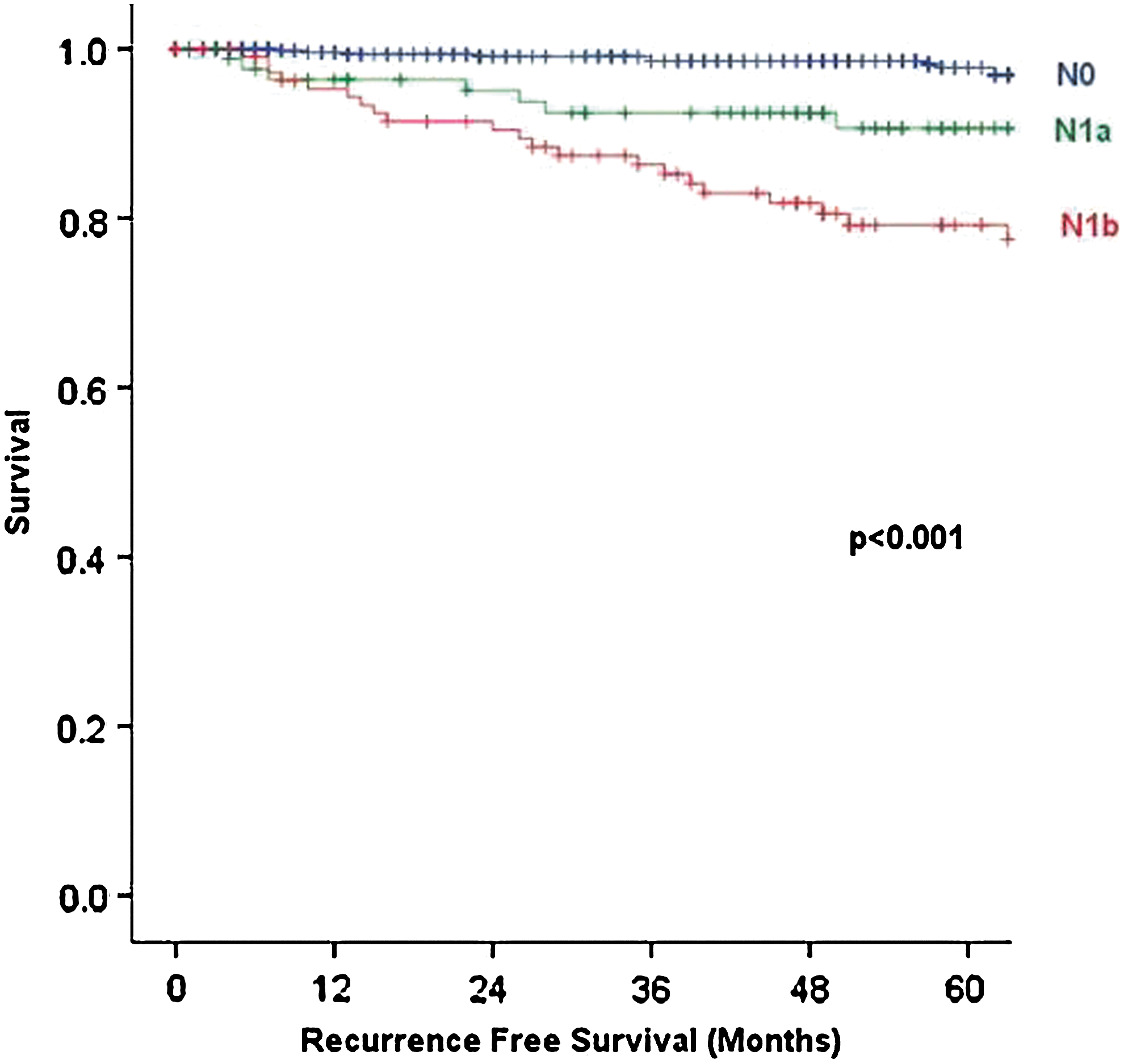
Recurrence in patients over 45y by N stage.
Thyroid Cancer Friday Poster Clinical
The BRAF (V600E) mutation and RET protein expression were found in papillary thyroid cancer (PTC). Recent studies show that BRAFV600E mutation or RET protein expression occurs frequently in patients with PTC showing aggressive clinicopathologic features. However, the features in PTC patients with both BRAFV600E mutation and RET protein expression were uncertain. The aim of the present study was to investigate the aggressive features in PTC patients with concurrent BRAFV600E mutation and RET expression.
Fifty pathologically confirmed PTC patients who had received thyroidectomy were enrolled into this study. BRAFV600E mutation was detected by real-time polymerase chain reaction (RT-PCR), while RET protein expression was measured by immunohistochemical SP method. Clinical and pathological features were compared between two groups, Group 1 (concurrent BRAFV600E mutation and RET protein expression) and Group 2 (only one of BRAFV600E mutation and RET protein expression, or none).
BRAFV600E mutation and RET protein expression were obtained in 76% (38/50) and 56% (28/50) of PTC patients, respectively. Concurrent BRAFV600E mutation and RET expression were detected in 48% of PTC patients. Moderately differentiated tissue, a solid variant that was highly aggressive, as well as higher MACIS score were more frequently observed in Group 1 than Group 2 (p values were 0.011, 0.020, and 0.022, respectively).
PTC patients with concurrent BRAFV600E mutation and RET expression present poorer differentiation, more highly aggressive variant in carcinoma tissues, and higher cancer-related mortality risk.
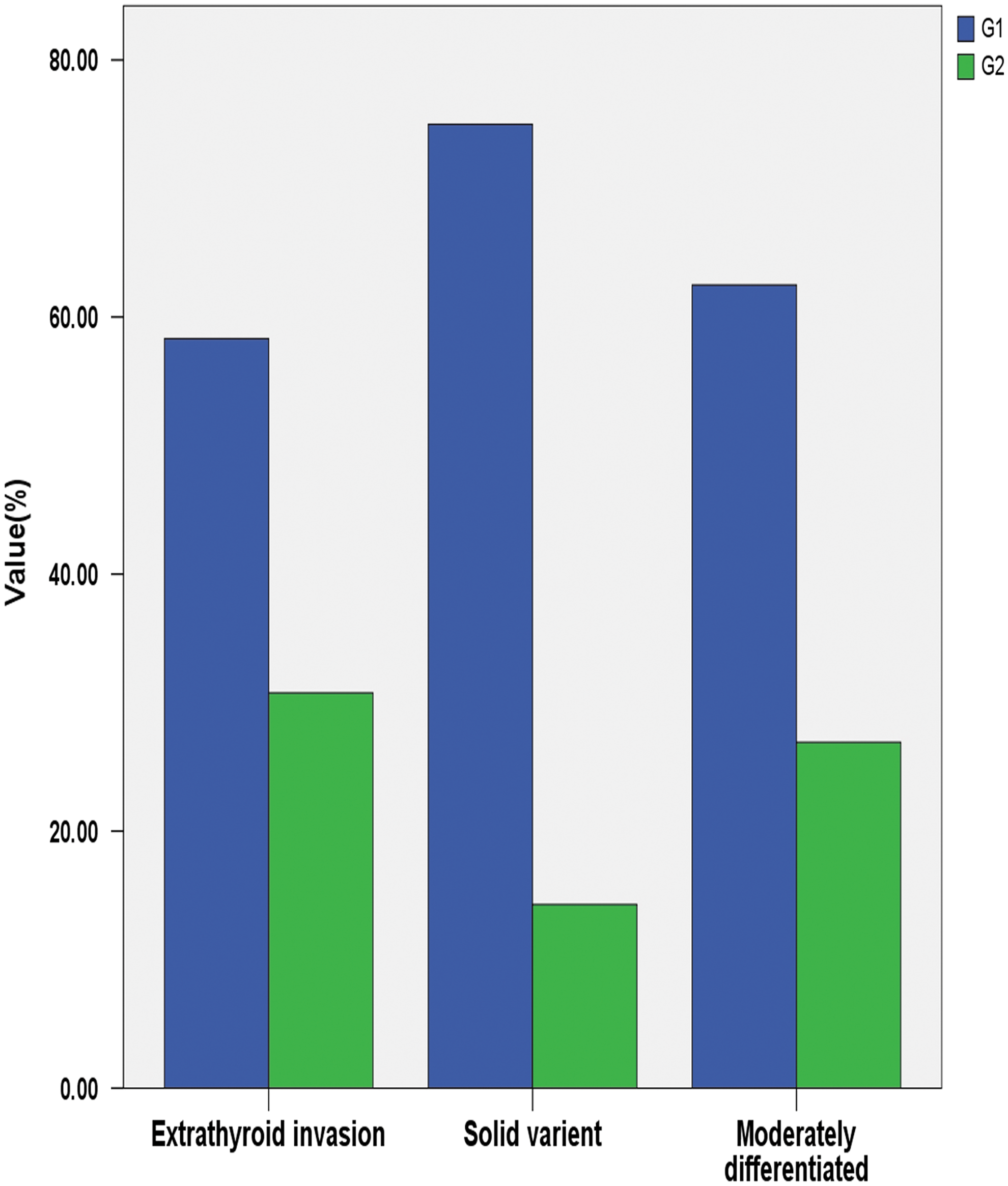
Prevalence of solid variant, moderately differentiation, and extrathyroid invasion between groups.
Thyroid Cancer Friday Poster Clinical
Vascular invasion is a well-known prognostic factor in a variety of carcinomas. It has been considered as important for outcome in patients with follicular thyroid carcinoma, but the prognostic role of vascular invasion is poorly investigated in papillary thyroid carcinoma (PTC). Thus, the aim of the present study was to investigate the prognostic value of histological vascular invasion for the course of disease of patients with PTC.
The institutional database was retrospectively searched for patients with PTC. Three hundred eighty-eight patients (290 women), who were in aftercare at least between 1990 and 2002 at our institution, were included. Data of epidemiological, clinical, and histological characteristics were obtained. All of the patients had undergone total or near-total thyroidectomy and subsequent ablative radioiodine therapy. The mean follow-up was 6.1±5.9 years. Sex, age, T-stage, N-stage, M-stage, and angioinvasion were tested for significant relations with development of persistent or recurrent disease by the use of Fisher and Pearson test, as appropriate. Variables that were statistically significant in prior testing were further evaluated by discriminant analysis with regard to their independent prognostic value.
Forty-three out of 388 patients (11%) showed vascular invasion; 10 of them (23%) had persistent or recurrent disease. Out of 345/388 patients without histological vascular invasion, only 24 patients (7%) suffered from persistent or recurrent disease at the end of follow-up, which was statistically significant (p=0.002). Besides angioinvasion, sex, T-stage, N-stage, and M-stage were significantly associated with persistent or recurrent disease. Discriminant analysis revealed vascular invasion, T-stage, N-stage, and M-stage as significant independent prognostic variables for PTC (p<0.0001, respectively).
Our study showed that angioinvasion is an independent prognostic factor for patients with PTC besides T-stage, N-stage, and M-stage. Therefore angioinvasion should be considered for patient management in PTC.
Surgery, Faculty of Health Sciences, University Beira Interior, Portugal, Covilhã, Portugal
Thyroid Cancer Friday Poster Clinical
The iodine ingestion of the population determines the pattern and prevalence of thyroid pathology. Iodine deficiency (ID) is influenced by many factors: the availability and cost of certain nutrients, cultural and lifestyle patterns, availability of iodized supplements or salt, and public education as to all different adverse consequences of ID. Close to 2 billion people worldwide are ID. ID may lead to a sustained increase in TSH, causing microscopic and macroscopic heterogeneity in the thyroid, increased incidence of thyroid cancer, and a rise in the ratio of follicular to papillary neoplasia. Urinary iodine excretion (UIE) is the most accurate method for assessing the iodine nutritional status of a population. Limited data, only recently published, show that the whole of Portugal to be ID.
Evaluation of pattern of thyroid nodular pathology in the most ID area of Continental Portugal, Beira Interior (BI), lying beyond high mountain ranges; population 211,189 (Census 2011). Data from all major referral Hospitals from BI and from the 3 existing Portuguese Oncology Institutes based on Cytological and Histological reports done from start of 2002 to start of 2008, from patients residing in BI assessed. UIE was measured by spectrophotometry (Sandell–Kolthoff reaction) in 13 patients presenting with thyroid nodules at the main Teaching Hospital of BI over a 3-month period and in 10 controls balanced for age and sex.
UIE of all 23 samples from MTHBI confirmed the recently published data finding of BI as significantly ID, both in the control group and in patients: C Median UIE=76.15 μg/L; P Median UIE=91.83 μg/L. Total of 869 patients evaluated over 6 years: 607 with cytology reports and 278 histology. From the 869 patients, 143 had thyroid neoplasm: 34 had papillary carcinoma, 100 follicular neoplasm, 4 medullary carcinoma, 4 anaplastic/undifferentiated carcinoma, and 1 metastatic carcinoma to the thyroid.
The inland area of Portugal studied of BI is significantly ID as reflected by the inversion of the usual ratio of the papillary/follicular ratio. Correction of this problem can only come from ample public education that leads to pressure on politicians to adopt Universal Salt Iodization.

Sample of 861 patients (Jan. 2002–Jan. 2008).
Thyroid Cancer Friday Poster Translational
Epigenetic control of gene expression has been demonstrated to be involved in the development and progression of thyroid cancer. The aim of this study was to analyze the mRNA expression of several proteins participating to epigenetic control of transcription in a series of 20 papillary thyroid carcinomas (PTCs). The results were further examined comparing subgroups presenting or not BRAF V600E mutation and stratifying the study population according to the risk of disease mortality (low vs. intermediate/high risk).
Quantitative real-time RT-PCR using microfluidic cards (TaqMan Low Density Arrays, TLDA: Applied Biosystems) in an ABI PRISM 7900HT Sequence Detection System (Applied Biosystems) was performed to assess the transcripts levels of histone deacetylases, histone acetyltransferases (HDAC), histone methyl transferases, histone demethylases, and DNA methyltransferases in the tumor tissue mRNA.
We found a light significant increase (p<0.05) of HDAC2 and EZH2 and a decrease of DNMT3B expression in the BRAF mutated PTCs; in contrast, no significant differences were detected between the more aggressive diseases (T3-4, N1, and M1) and the low-risk subgroup.
In conclusion, these preliminary data demonstrate that altered expression of elements of epigenetic pathways is associated with the presence of BRAF mutation and not with a more aggressive behavior of PTCs. Further studies, including larger series of tumors, will contribute to clarify the role of such finding in defining novel molecular biomarker and/or pathogenic element of the BRAF mutated PTCs.
Dipartimento di Medicina Interna e Specialità Mediche, Università di Roma Sapienza, Rome, Italy
Thyroid Cancer Friday Poster Clinical
A genetic susceptibility for thyroid cancer of follicular cell origin has been suggested. Investigation of hereditary forms enables to unmask genetic features of sporadic counterpart, but also provides a basis to understand principles of cancer genetics in general. In this regard, families with ≥3 first-degree relatives affected by differentiated thyroid cancer (FDTC), in which the likelihood to harbor an inherited disorder is higher, would be more representative.
A multicentric study, including patients with FDTC, was established to investigate the clinical–morphological features of the disease, and to identify homogeneous subgroups of individuals in whom genetic analysis could be performed. Blood samples and formalin-fixed, paraffin-embedded tissues are being collected for this purpose. A cohort of 192 families carrying ≥2 cases was identified, including 153 with 2 and 39 with 3 cases. In a preliminary analysis, the latter cohort was compared to a consecutive series of 1681 patients carrying the sporadic forms. Differences in sex distribution, age at diagnosis, histological features, and clinical outcome were explored. Statistical analysis was performed using independent samples t-test and Fisher exact test as appropriate.
No differences in sex distribution and mean age at diagnosis were documented. FDTC cases occurred with a higher rate of multifocality (55% vs. 29%; p<0.0001) and bilaterality (38% vs. 18%; p<0.0001) when compared to sporadic counterpart. The percentage of patients with tumor extension beyond the thyroid capsule was significantly higher in the FDTC series (12% vs. 5%; p=0.009), whereas no differences were observed in the occurrence of locoregional and distant metastases. Disease recurrence/persistence rates and disease-specific survival were similar in the two groups after a mean follow-up of 6.5 yrs.
Preliminary data of our study do not support a more aggressive behavior of FDTC as compared to the sporadic counterpart, even though differences can be foreseen. Larger prospective case series are needed, and we aim to establish a Familial Thyroid Cancer Registry to achieve a correct prognostic assessment and appropriate management of this clinical entity as well to clarify the genetic background.
Dipartimento di Medicina Interna e Specialità Mediche, Università di Roma Sapienza, Rome, Italy
Thyroid Nodules & Goiter Friday Poster Clinical
The past 2 decades have witnessed a steady rise in the frequency of nodular thyroid disease, which is an emerging public health concern. Most of the nodules being discovered are benign and clinically insignificant, and only a subgroup can be expected to grow overtime. The challenge is to find markers that can predict this type of behavior. The factors influencing thyroid nodule growth are currently unknown, and their identification will require large prospective studies.
In Italy, a multicenter prospective observational study has been underway since 2006. Its aim was to characterize the natural history of 1569 untreated, cytologically benign euthyroid nodules (993 patients). This series does not include cystic lesions or individuals with biochemical and morphological evidence of thyroiditis. All patients were followed-up yearly with cervical ultrasound and TSH, fT4, and fT3 assays. Additional information was gathered regarding family history of nodular goiter, way to diagnosis, residence in an endemic area, use of iodized salt, prior
In a median follow-up of 4.5 years (range: 4–5), the majority of thyroid nodules did not grow. Only 15.4% have increased in size, being the mean growth rate of 3.7 mm in maximum diameter and 1.88 mm3 in volume (p<0.0001). Higher growth rates appear to be associated with maximum nodule diameters >7.5 mm, multinodular goiter, and diagnosis before age 47 (HR 28.98, CI 95% 9.93–53.21). Furthermore, thyroid volume increased only in those patients experiencing a nodule growth.
Our findings demonstrated in a large cohort of patients that most solid, benign euthyroid nodules remain stable in size overtime. Only a minority displays any growth at all. Moreover, our study could help to identify thyroid nodules requiring closer surveillance.
Characteristics of the Study Population at the Beginning of Follow-up
Abbreviations: SD, standard deviation; BMI, body–mass index; US, ultrasound
Thyroid Cancer Friday Poster Clinical
Multimodality imaging using 131I SPECT/CT or 18F FDG PET/CT has allowed a better knowledge of atypical foci that may be related to either unusual sites of DTC metastasis or false-positive (FP) 131I uptake. Multiple distant metastases are frequent in refractory thyroid cancer. Rare metastatic sites should be differentiated from FP uptake, as it may impact on the clinical decision and prognosis of patients.
In France, the management of refractory thyroid cancer patients has benefited from the TUTHYREF network, a unique system where individual cases are collectively discussed twice a month during Web conferences among 30 regional expert centers throughout France. Among the TUTHYREF network, we are collecting rare metastases (defined as sites other than lung and bone localizations) or FP 131I images, confirmed by histology whenever possible or follow-up procedures.
We have already collected 12 patients presenting rare metastatic sites (liver, brain, adrenal, muscular or skin metastases, pleural, mesenteric, peritoneal, gastric, and diameter); of note, all of them except one occurred in patients with a refractory thyroid cancer, and mostly with an aggressive histology (8 follicular or poorly differentiated tumors). We have also reviewed 14 131I FP localizations of which histology was sometimes required to eliminate rare metastasis (such as kidney and ovary lesions). Histology, TNM, and age at diagnosis, possible association with lung and/or bone metastases, and delay since primary diagnosis have been collected. Treatments such as surgery, cumulative 131I dose, external-beam radiation therapy, local treatment modalities, and even targeted therapy have been listed.
Work is still in progress, and updated findings will be presented. The final aim will be to present an atlas of rare metastatic localizations and 131I FP images in DTC.
EXTENT OF MINIMAL EXTRATHYROIDAL EXTENSION IN PAPILLARY THYROID CARCINOMA AS A PREDICTIVE FACTOR
Thyroid Cancer Friday Poster Clinical
The prognosis of papillary thyroid carcinoma (PTC) according to the extent of minimal extrathyroidal extension (ETE) has not been clarified yet. The purpose of this study was to evaluate for patients with PTC to have how different prognosis according to the extent of minimal ETE in PTC.
The prospective collecting data were reviewed for 1385 patients with primary PTC who received conventional thyroidectomy from September 2008 to February 2012. We divided patients to three groups according to the extent of minimal ETE. Group A was patients without ETE. Group B was patients with ETE limited to perithyroid soft tissue. Patients with ETE invaded to sternothyroid muscle were classified to group C. The clinicopathologic characteristics of patients were analyzed.
Group A consisted of 682 (49.2%) patients, group B 631 (45.6%), and group C 72 (5.2%). BRAF gene mutation was more frequent in group B than in group A (p=0.007). Multifocality of tumor was more frequent in group B than in group A (p<0.0001). Node metastasis was higher in group B than in group A (p<0.0001), and also higher in group C than in group B (p<0.0001). Mean numbers of metastatic neck nodes were higher in group C than in group B (p<0.0001), and also higher in group B than in group A (p<0.0001). Lateral neck node dissection was more frequently performed in group B than in group A (p<0.0001), and also more frequent in group C than in group B (p=0.015). Radioactive iodine therapy (RI) was more frequently performed in group B than in group A (p<0.0001). Mean withdrawal Tg level was lower in group B than in group C (p=0.006). In patients with node-positive and RI, the mean withdrawal Tg level was lower in group B than in group C (p=0.029).
Patients with ETE limited to the perithyroid soft tissue have poor prognostic factors than patients without ETE however have better prognostic factors than patients with ETE invaded to muscle. However, to classify the prognosis according to the extent of ETE, further study about complications and long-term follow-up should be followed.
COMPARISON OF SURGICAL OUTCOMES BETWEEN HARMONIC ACE® AND LIGASURE PRECISE™ IN CONVENTIONAL THYROIDECTOMY OF PAPILLARY THYROID CANCINOMA: A PROSPECTIVE RANDOMIZED STUDY (PRELIMINARY REPORT)
Thyroid Cancer Friday Poster Clinical
Over the last few years, many surgeons have begun to use an ultrasonic coagulation device (Harmonic scalpel) or bipolar energy-sealing system (LigaSure) to perform thyroid surgery. Recent studies have reported the benefits of these devices over hand-tying techniques. We conducted a prospective randomized study to determine if there are any differences in operative time, clinical results, and morbidities between the two devices.
A prospective randomized trial was performed. Total of 146 patients who required a thyroidectomy for papillary thyroid cancer were randomized to either Harmonic ACE® (H) or LigaSure Precise™ (L). The parameters of operative time, number of retrieved, and metastatic lymph node and morbidities such as transient recurrent laryngeal nerve injury, and hypoparathyroidism were analyzed.
There was no statistically difference in operative time (H vs. L; 73.4 vs. 76.5, p=0.318), number of retrieved lymph node (9.3 vs. 10.1, p=0.486), and metastatic lymph node (1.64 vs. 1.64, p=0.998). In regard to complications, there was no difference in the percentage of patients developing hypocalcemic symptoms (41.6% vs. 39.1%, p=0.449), transient hypoparathyroidism (20.7% vs. 21.7%, p=0.828), and permanent recurrent laryngeal nerve injuries. Although not statistically difference in the rate of vocal cord palsy on postoperative stroboscopy, L groups were higher than H groups (8.7% vs. 2.6%, p=0.105).
In this study, there were no significant differences in the postoperative results and complications between the two devices.
HEMORRHAGE IN METASTATIC LYMPH NODE AFTER ABLATIVE RADIOACTIVE IODINE THERAPY FOR PAPILLARY CARCINOMA–A RARE COMPLICATION
Thyroid Cancer Friday Poster Clinical
RAI is used after thyroidectomy to ablate the residual normal thyroid remnant, as adjuvant therapy and to treat thyroid cancer metastasis. Acute risks post-RAI includes nausea and vomiting, loss of taste, salivary gland swelling, and pain.
A 34-year-old Caucasian woman underwent total thyroidectomy and central neck dissection for papillary carcinoma. Tumor was 5 cm with extension into perithyroidal tissue, and 9/18 lymph nodes were positive, T4N1M0. Patient was treated with 149.6 millicuries of radioactive iodine (RAI) 6 weeks after surgery following withdrawal of thyroid hormone. Pretreatment TSH was 148 mIU/L. Pretreatment scan revealed small-to-moderate uptake in the right neck, and post-treatment scan was read as large amount of uptake in right neck. Three weeks following RAI, patient presented with painful right-sided neck swelling and dysphagia. On examination, trachea was deviated to left due to a tender palpable right neck mass. Ultrasound revealed a 10-cm cystic mass; 12 mL of bloody fluid was aspirated with relief of symptoms. Cytology was nondiagnostic. Patient underwent a modified right lateral neck dissection. Pathology reported 7/46 positive lymph nodes at levels 3 and 5. Large cystic mass was 8×4×1 cm and was positive for papillary carcinoma.
In this patient, hemorrhage occurred in residual metastatic thyroid tissue in lateral neck lymph nodes. Only two similar cases have been reported in literature—1) mediastinal hemorrhage following RAI for thyrotoxicosis caused by retrosternal thyroid tissue and 2) hemorrhage in brain metastases following RAI for treatment of metastatic papillary carcinoma. Possible pathophysiology includes increased vascularity of thyroid metastases and possibly stimulation of growth induced by the TSH stimulation before ablative therapy. The temporal relationship between RAI and hemorrhage into metastases is highly suggestive of causality.
Clinically significant metastatic lymph node hemorrhage postradioiodine therapy has been reported here for the first time. Pretreatment scan indicating significant residual disease should warrant closer surveillance or possibly consideration for additional surgery before treatment with radioiodine.
Department of Head and Neck Oncology, Institut Gustave Roussy, Villejuif, France
Thyroid Cancer Friday Poster Clinical
Prophylactic neck dissection (PND) for differentiated thyroid cancer is controversial due to the absence of high-level evidence showing an improvement in oncologic outcomes. The objective of this study was to analyze the influence of PND on postoperative radioiodine doses and locoregional control.
Retrospective study of patients with differentiated thyroid carcinoma 11–70 mm without ultrasonographic evidence of nodal disease (cN0) treated with total thyroidectomy (TT) or TT with PND of the central compartment bilaterally or of the central compartment and the ipsilateral levels III and IV between 1995 and 2010. All received postoperative radioactive iodine. Recurrences were defined as abnormal ultrasound findings confirmed by cytology, reoperation, or repeat radioactive iodine (131I) treatment. We compared the total cumulative dose of 131I and the number of reoperations in the central compartment between the 2 groups.
A total of 265 patients (mean age 45 years, 205 women (77%) underwent either TT (n=109) or TT with PND (n=156). The groups were similar in age, gender, and tumor size (p>0.05). Median follow-up was 6.4 years, with no difference between the groups. Eighty-one patients were staged pN1 in the TT+PND group (52%). The total dose of 131I received was 3.85 GBq for the TT group and 4.25 GBq for the TT+PND group (p=0.93). Thirteen (12%) of the patients in the TT group underwent reoperation in the central compartment for recurrence versus 3 (2%) in the TT+PND group (p=0.001). The rate of permanent recurrent nerve paralysis was similar in the two groups (4.6% for the TT group and 3.2% for the TT+PND group, p=0.56), and the rate of permanent hypoparathyroidism was higher, but not significantly in the TT group [9.2% versus 4.5% (p=0.12)]. To avoid one reoperation, the number needed to treat with PND was 10 patients.
Reoperation in the central compartment was avoided by prophylactic neck dissection in 10% of patients, despite the relatively short follow-up period of this cohort. When it can be performed safely, PND may be advantageous to avoid reoperation and lower the risk of permanent hypoparathyroidism.
Alex & Simona Shnaider Research Laboratory in Molecular Oncology, Samuel Lunenfeld Research Institute, Mount Sinai Hospital, University of Toronto, Toronto, ON, Canada
Thyroid Cancer Friday Poster Clinical
Currently, there are no biomarkers for aggressive papillary thyroid carcinoma (PTC). There is an urgent need to identify biomarkers for early detection of aggressive PTCs. We hypothesize that proteins secreted by TC cell lines will serve as candidate biomarkers to distinguish benign nodules from malignant PTC and aggressive from nonaggressive PTCs.
Conditioned media from cultured papillary (BCPAP) and anaplastic (SW1736 and C643) TC cell lines were collected for proteomic analyses using liquid chromatography and mass spectrometry. Using Ingenuity Pathway Analysis, protein–protein interactions in key cell-signaling protein networks were analyzed. A panel of nine proteins was chosen for further study in patients' sera and tissues.
APP, APLP2, AXL, PKM2, 14–3-3 zeta, and SET proteins were detected in patients' sera by western blotting. Immunohistochemical analyses showed significant differences in subcellular expression of these proteins in benign and malignant tissues. Increased nuclear expression of a panel of 4 proteins, AXL, hnRNP K, PGK1, and SET, could accurately distinguish benign nodules from malignant TC [p<0.001; sensitivity=87.5%, specificity=99%, area-under-curve (AUC)=0.98]. ALCAM overall (membrane and cytoplasmic) expression was significantly reduced in patients with poorly differentiated PTC/undifferentiated anaplastic (aggressive) TC compared to well-differentiated PTC (p<0.001, AUC=0.865, sensitivity=82%, specificity=74%, PPV=95%) as analyzed in 158 PTCs and 45 benign nodules. Kaplan–Meier survival analysis revealed significantly reduced disease-free survival for TC patients with lower ALCAM expression (median survival of 7.3 years as compared to 13.5 years for patients with higher expression, p=0.002). Using ELISA, circulating ALCAM levels were significantly elevated in aggressive TC patients versus well-differentiated PTC (p=0.04).
Using secretive analysis, several candidate TC biomarkers were identified. Among these, a panel of four proteins could distinguish benign nodules from malignant TC accurately. Reduced ALCAM expression may potentially serve as a useful diagnostic and prognostic marker for aggressive PTC.
VOCAL FUNCTION IS AFFECTED BY THE EXTENT OF SURGERY IN THYROID CANCER: LOBECTOMY VS. TOTAL THYROIDECTOMY
Thyroid Cancer Friday Poster Clinical
Voice and throat symptoms could be documented after thyroidectomy in varying degrees, even without the laryngeal nerve injury. We sought to analyze whether the extent of thyroid surgery affects these functional impairments through serial postoperative evaluations.
Consenting patients undergoing lobectomy (L, n=37), total thyroidectomy (TT, n=42), and total thyroidectomy with radioactive iodine treatment (TTRI, n=103) were prospectively enrolled. Objective and subjective parameters like GRBAS, acoustic voice analysis, including maximal frequency (fmax), minimal frequency (fmin), and frequency range, voice handicap index (VHI), and Glasgow Edinburgh Throat Scale (GETS) to evaluate throat discomfort were serially evaluated. Each session of evaluation was obtained before surgery and 1 month, 6 months, and 1 year after surgery in all enrolled patients.
At 1 month, the L group exhibited significantly better grade (L, 0.37: TT, 0.82: TTRI, 0.86; p=0.0003), roughness (L, 0.43: TT, 0.84: TTRI, 0.77; p=0.0006), and strain (L, 0.08: TT, 0.24: TTRI, 0.31; p=0.033), perceptually. Acoustic parameters like jitter (p=0.0008), fmax (Hz, p=0.0173), and frequency range (p=0.0126) were also significantly better in the L group. VHI was consistently better in the L group. However, these differences at 1 month eventually diminished at 6 and 12 months after surgery. Subjective throat discomfort surveyed with GETS was not different between L and TT.
Objective and subjective vocal impairments are more severe after TT than L around 1 month after surgery. Narrow pitch range, lowered fmax, and increasing jitter are typical, which are normalized after 6 months. RI did not affect voice outcome throughout whole follow-up.
ELLICSR Health, Wellness and Cancer Survivorship Centre, Princess Margaret Hospital, Toronto, ON, Canada
Thyroid Cancer Friday Poster Clinical
The increasing number of thyroid cancer survivors limits the sustainability of specialist-based follow-up care. A greater understanding of the supportive care needs of thyroid cancer survivors could guide intervention development. The purpose of this study was to investigate the supportive care needs of thyroid cancer survivors who have completed primary treatment.
Two hundred two thyroid cancer patients receiving follow-up care at an urban cancer center completed a questionnaire assessing supportive care needs and health care service use. We examined the associations between patient characteristics and supportive care needs.
Respondents were on average 50.1 years of age (SD=14.7), women (64.7%), and a median of 3.6 years postdiagnosis (IQR=4.9). Approximately 40% were born outside of Canada and spoke English as a second language. Respondents had more met (median 8.0, IQR 8.0) than unmet (2.0 median, IQR 7.0) needs. The majority (64.7%) reported at least one unmet need. The top 5 unmet needs reported by 27%–30% of respondents were concerning care coordination, fear of recurrence, ongoing case management, stress, and side effects. Patients who were younger, who were unemployed, who had radioactive iodine or external beam radiation had more unmet needs, or who reported more health care visits had more unmet needs. Women had more met needs, and those who reported more health care visits had more needs overall.
A considerable proportion of thyroid cancer survivors have unmet supportive care needs. Greater needs may be associated with greater use of health care services. Research is needed to determine whether interventions to improve care coordination, address psychosocial issues, and manage side effects could help meet survivors' supportive care needs and optimize health care service use.
Faculty of Medicine, University of Toronto, Toronto, ON, Canada
Thyroid Cancer Friday Poster Clinical
Cancer-related worry can impact psychosocial health and life choices in cancer survivors. The level and nature of cancer-related worry are not known for thyroid cancer survivors.
We conducted a cross-sectional, self-administered, written survey of members of the Thyroid Cancer Canada patient support group. The survey included questions on demographic, social, and thyroid cancer history characteristics. The degree of overall cancer-related worry was measured using the Assessment of Survivor Concerns (ASC) questionnaire, which examines worry about future tests, second primary malignancy, disease recurrence, death, personal health, and children`s health (each scored on a Likert scale, from 1—no worry to 4—worry very much). The overall ASC worry score is the sum of scores to respective questions (possible total scores vary from 6—no worry to 24—greatest worry). In a published reference mixed cancer population used to develop the ASC questionnaire, a mean score of 12.50 could be estimated (sum of mean scores for individual questions).
The effective response rate was 58.6% (923/1576). The majority of respondents were women (822/922 responses, 89.2%) and more than half were younger than 50 years of age (54.1%, 499/906). Most individuals reported being treated with total thyroidectomy (97.3%, 896/921) and one or more radioactive iodine treatments (84.6%, 763/903). The timing of the most recent thyroid cancer treatment received by participants was as follows: less than one year ago—24.2% (222/919), 1 to 5 years ago—50.6% (465/919), or more than 5 years ago–25.2% (232/919). The mean overall ASC worry score was 15.36 (standard deviation 4.68). Thyroid cancer survivors worried the most about personal health and children's health (the latter observed particularly in individuals with children), whereas they worried the least about dying.
Thyroid cancer patients and survivors suffer significant cancer-related worry, but the focus of worry is most frequently on personal health or health of children, rather than a fear of death.
HOW MANY CONTRALATERAL PAPILLARY THYROID CARCINOMAS CAN BE MISSED?
Thyroid Cancer Friday Poster Clinical
When surgeons decide to perform lobectomy as the treatment of papillary thyroid carcinomas (PTCs), they have to consider the possibility of contralateral cancer. The true incidence of contralateral papillary thyroid carcinoma (preoperatively not detected, but pathologically detected) is unknown. We wanted to determine the incidence of bilateral PTC (bPTC) and analyze of characteristics of bPTC. Also, we wanted to identify how many patients with bPTC were missed preoperatively.
From January 2007 to May 2011, a total of 466 patients with PTC who were treated by total thyroidectomy at a single institution were enrolled. Patients were divided into two groups based on bilaterality, and the patients with bilaterality were further investigated for the preoperative presence of contralateral tumor.
Bilaterality was seen in 29.8% of PTC, 36.8% of PTC≥1 cm, and 25.7% of PTMC. The presence of missed PTC in the contralateral lobe was 15.8% in bPTC, and 21.3% in bPTC. The rate of preoperatively nondetected contralateral cancer was 4.7% and 5.5% in PTC and PTCM, respectively. Tumor size and multifocality were factors associated with bilaterality (p=0.014, p<0.001).
Bilaterality was seen in 29.8% of PTC, 36.8% of PTC≥1 cm, and 25.7% of PTMC. According to our results, bilaterality is found more frequently when the tumor size is larger. In addition, multifocality can help predict the possibility of bilaterality. The presence of PTC missed in the contralateral lobe was 15.8% in bPTC, 21.3% in bPTMC, and the rate of preoperatively nondetected contralateral cancer was 4.7% and 5.5% in PTC and PTCM, respectively. Therefore, total thyroidectomy may be necessary for patients with the risk factors mentioned above, and it should be kept in mind that the presence of contralateral cancer can be missed in 5.5% of patients with preoperatively unilateral PTMC.
Departments of Internal Medicine, Catholic University of Daegu, School of Medicine, Daegu, Republic of Korea
Thyroid Cancer Friday Poster Clinical
The aim of this study was to evaluate the usefulness of postablation scan after radioactive iodide remnant ablation in intermediate-risk patients with differentiated thyroid cancer (DTC).
A total of 453 subjects were included in the study: 185 subjects with low risk and 268 subjects with intermediate risk according to the American Thyroid Association (ATA) guideline. All subjects diagnosed with differentiated thyroid carcinoma received 1100 MBq (30 mCi) activity of radioiodine (131I) following total thyroidectomy. At follow-up, all subjects underwent 131I whole-body scan after thyroid hormone withdrawal.
The medians of follow-up time were 8.41±2.86 months in the low-risk group and 7.95±2.54 months in the intermediate-risk group. After initial radioactive iodide remnant ablation, 94.1% of patients from low risk and 91.4% of those from intermediate risk were no uptake at postablation scan (p=0.295). Stimulated thyroglobulin (Tg) levels in no uptake group and thyroid-bed uptake group after postablation scan after radioactive iodide remnant ablation were not significant differences (0.75±2.14 and 1.13±1.62, respectively, p=0.311).
Postablation scan after radioactive iodide remnant ablation in intermediated-risk patients with DTC according to the ATA guideline may not be useful. A selection of patients for 131I postablation scan, at least in some patients together with this strategy of follow-up, will reduce both the cost and exposure to 131I of the treatment and follow-up of intermediated-risk patients with DTC.
PREDICTIVE FACTORS FOR CONTRALATERAL CENTRAL LYMPH NODE METASTASIS IN PAPILLARY THYROID CARCINOMA
Thyroid Cancer Friday Poster Clinical
Background: The aim of this study was to evaluate the incidence and predictive factors of contralateral central lymph node metastasis.
Methods: From March 2007 to April 2012, a retrospective review of 246 patients with papillary thyroid cancer who underwent primary total thyroidectomy and elective bilateral central lymph node dissection. The tumor size was >1 cm. The clinicopathologic results were reviewed, and the incidence and patterns of contralateral central cervical lymph node metastasis were analyzed.
Results: The overall frequency of central lymph node metastasis was 52.6%. Among them, ipsilateral and contralateral central lymph node metastasis was 49.0% and 20.2%, respectively. The univariate analysis revealed that the predictive factors for the contralateral central lymph node metastasis are male patients, the presence of lymphovascular invasion, the patients who do not have thyroiditis and ipsilateral central lymph node metastasis (p<0.05). In the multivariate analysis, male patients, the presence of lymphovascular invasion and ipsilateral central lymph node metastasis were the predictive factor for the contralateral central lymph node metastasis.
Conclusion: Even though the tumor exists only in one side of lobe, the surgeon should perform thorough central lymph node dissection, including contralateral central lymph node during initial thyroidectomy if the patient is male and the presence of ipsilateral central lymph node metastasis.
PAPILLARY THYROID CARCINOMA WITH THYROIDITIS: LYMPH NODE METASTASIS, COMPLICATIONS, AND EXTENT OF OPERATION
Thyroid Cancer Friday Poster Clinical
The development of thyroiditis has made thyroidectomy more difficult. The aim of this study was to evaluate the clinicopathologic characteristics and short-term outcomes, determine the rate of complications, the incidence of central and lateral lymph node metastasis, and the extent of operation in papillary thyroid cancer with thyroiditis.
A retrospective review of 1247 patients with papillary thyroid cancer who underwent primary thyroidectomy was performed. Among them, 316 patients had thyroiditis (Group I), and 931 patients had no thyroiditis (Group II) on the final pathologic reports. The clinicopathologic results were compared between the two groups. The rate of complications and the incidence of central lymph node metastasis were analyzed.
There was no difference in age and mean tumor size between the two groups. Female gender, preoperative hypothyroidism, total thyroidectomy, no extrathyroid extension, no lymphovascular invasion, and no perineural invasion were associated with Group I. The number of central lymph nodes removed was more in Group I than in Group II; however, the number of central lymph nodes with metastasis was less in Group I than in Group II. In the lateral lymph nodes, the number of removed nodes and nodes with metastatic tumor was similar between the two groups. A multivariate analysis revealed that there was a female predominance, more cases of preoperative hypothyroidism, more dissected lymph nodes, and less number of lymph nodes with metastasis in Group I. There was no difference in postoperative complications between the two groups.
This study suggests that the presence of thyroiditis is associated with less central lymph node metastasis. However, because of the pre- and postoperative thyroid function, especially hypothyroidism, total thyroidectomy should still be considered in patients who have papillary thyroid cancer with thyroiditis, and the surgery can be performed with low risk of complications.
Endocrinology, Hospital La Paz, Madrid, Spain
Thyroid Cancer Friday Poster Clinical
Gorlin syndrome (GS) is a rare genetic disorder caused by mutations at the PTCH gene (9q22.3), and characterized by a high predisposition to developing multiple nevoid basal cell carcinomas (BC) and an increased sensitivity to ionizing radiation. Although PTCH is located close to FOXE1, a locus associated with thyroid carcinoma (TC) susceptibility and radiation-related TC, TC diagnosis in GS is exceptional with only 2 reported cases, 1 papillary (PTC) and 1 medullary. The polymorphism Pro1315Leu at PTCH has been associated with an increased risk for multiple BC.
We present 2 female patients with multiple CB, both diagnosed with PTC, in whom a novel PTCH mutation and the PTCH Pro1315Leu polymorphism were identified, respectively.
A 43-year-old female patient with a history of multiple CB noticed a cervical right 3-cm node 1 month after finishing treatment with external radiotherapy (RT) for a recurrent nasal BC. FNA suggested a PTC metastasis. Histopathology after total thyroidectomy (TT) described a PTC of papillary and follicular variants and PTC metastasis in 2/7 resected regional lymph nodes. She received 100 mCi of radioactive iodine (RI) postoperatively, and 2 years after diagnosis, she remained free of disease. Genetic PTCH study revealed the combined novel mutation c.2887insA (p.Ile963AsnfsX29) and c.2885G>A:R962K at exon 17 in the proband and 1 of her 2 sons. Another nonrelated 51-year-old woman, with a history of surgical resection of many CB, had been diagnosed with PTC 3 months after RT for a recurrent BC at esternal region. Thirteen years later, after TT and RI treatment, she remains free of disease. Based on her GS-like phenotype, genetic PTCH study was performed revealing the Pro1315Leu polymorphism.
The evolution of these cases highlights the importance of a close thyroid follow-up in patients with multiple recurrent CB, especially in those who need head/neck RT, considering the increased sensitivity to RT that they may display, due to potential underlying PTCH abnormalities, and the variable phenotypic spectrum they might produce. However, if TC is a new GS feature and what is the relative contribution of each factor (genetic/RT) to TC development/progression in these patients is still unknown.
Head and Neck Surgery, UCLA David Geffen School of Medicine, Los Angeles, CA
Thyroid Cancer Friday Poster Clinical
The purpose of this study was to examine trends in thyroid cancer incidence and treatment for female veterans over a 10-year period at a large urban VA Healthcare System. The incidence of thyroid cancer is increasing steadily in the United States, with about 75% of new cases occurring in women. Although survival rates are excellent for most stages of thyroid cancer, careful surveillance and follow-up are important. The VA Healthcare system is the largest integrated healthcare system in the United States and provides a unique population for study of thyroid cancer, with ready access to coordinated care for multiple specialties, including endocrinology, surgery, nuclear medicine, and radiology, and a nationwide electronic medical records system, which allows tracking of patients even when transferring care to other VA hospitals. The number of female veterans is rapidly rising, and this has resulted in active women's health clinics at most VA hospitals.
The computerized patient record system (CPRS) for the VA Greater Los Angeles Healthcare System (VAGLAHS) was searched using the ICD-9 code for thyroid cancer (193.x) to identify all patients seen at this healthcare system between 2002 and 2011 with a diagnosis of thyroid cancer.
There were a total of 270 veterans with the diagnosis of thyroid cancer seen at VAGLAHS between January 1, 2002, and Dec. 31, 2011, including 34 women and 236 men. The number of unique female patients with thyroid cancer seen annually increased from 7 to 15 during this time period, while the number of unique male patients with thyroid cancer seen annually increased from 55 to 87. Most women were seen initially in a primary care or women's health clinic and subsequently referred for imaging, endocrinology, and surgery consults. About 71% were followed by the endocrinology service at the GLAVA, while 24% moved away and were followed at other VA hospitals. Women who received their treatment at the GLAVA were all treated according to ATA guidelines, including long-term follow-up and surveillance.
The VA provides a comprehensive program for female veterans with thyroid cancer. Ready access to endocrinology, surgery, imaging, cytology, and nuclear medicine allows optimal care for these patients.
Psychosomatic Medicine, Fukuoka Tokushukai Medical Center, Kasuga, Japan
Thyroid Cancer Friday Poster Clinical
Rheumatoid arthritis patients are sometimes comorbid with chronic thyroiditis, namely Hashimoto thyroiditis. Thyroid lymphoma, one kind of lymphoproliferative disorders, is strongly associated with chronic thyroiditis. Recently, lymphoproliferative disorders were frequently developed in patients with rheumatoid arthritis with or without methotrexate and or anti-TNF therapy.
Case report: A 62-year-old woman with rheumatoid arthritis developed goitrous primary hypothyroidism having a marked elevation of antithyroid antibodies. Thyroid hormone replacement therapy was done; however, the enlarged goiter was not reduced, and furthermore, she complained of a swollen throat and hoarseness. The laryngoscopic finding revealed subglottic edema. She received 6 mg weekly of methotrexate and 1.5 mg daily of tacrolimus. Furthermore, she had Helicobacter pylori infection. The withdrawal of both methotrexate and tacrolimus and the eradication of H. pylori caused remission.
Antirheumatoid arthritis therapy such as methotrexate, tacrolimus, and or anti-TNF therapy, and H. pylori infection might produce thyroid lymphoproliferative disorder, which was able to be in remission after discontinuation of antirheumatoid medication or eradication of H. pylori.
Internal Medicine/Div of Endocrinology, Thomas Jefferson University Hospital, Philadelphia, PA
Thyroid Cancer Friday Poster Clinical
Warthin-like tumors of the thyroid are an uncommon variant of papillary thyroid cancer (PTC) and have been consistently described in the background of Hashimoto's thyroiditis. They bear their name for their pathological resemblance to Warthin salivary gland tumors. Here we present a case of a Warthin tumor of the thyroid in a patient with type 2 autoimmune polyglandular syndrome (Schmidt's syndrome).
Case: A 49-year-old woman had a history of Graves' disease diagnosed at age 16 (spontaneous lasting remission after 1 year of methimazole), Addison's disease diagnosed at age 26, and type 1 diabetes mellitus at age 28 (GAD65+). She was found to have a PET-positive 11×6×9-mm right/isthmus nodule, discovered during PET/CT surveillance for a diagnosis of breast cancer treated one year previously with surgery and external radiation. She has no family history of thyroid cancer. Fine-needle aspiration of the right/isthmic nodule was consistent with PTC (no genetic markers tested), and she underwent total thyroidectomy with central neck dissection. Final pathology revealed a 6-mm Warthin-variant PTC in a background of lymphocytic thyroiditis. No lymph node involvement was found in the five evaluated. Postoperative thyroglobulin was undetectable with negative thyroglobulin antibodies. In a 3-year follow-up, she continues to have undetectable thyroglobulin and thyroglobulin antibodies, as well as no recurrence on ultrasound.
Warthin-variant PTC is a rare tumor and may be difficult to distinguish histologically from Hurthle cell tumors, as well as tall-cell and oncocytic variants of PTC. Histologic presentation is papillae lined with eosinophilic polygonal cells with a lymphocytic core. Its clinical implication is not yet clear; however, some report preponderance for lymph node metastasis and extrathyroidal spread. It tends to appear in the background of Hashimoto's thyroiditis. Our patient is unique in that she additionally has a history of Graves' disease in the setting of type 2 autoimmune polyglandular syndrome.
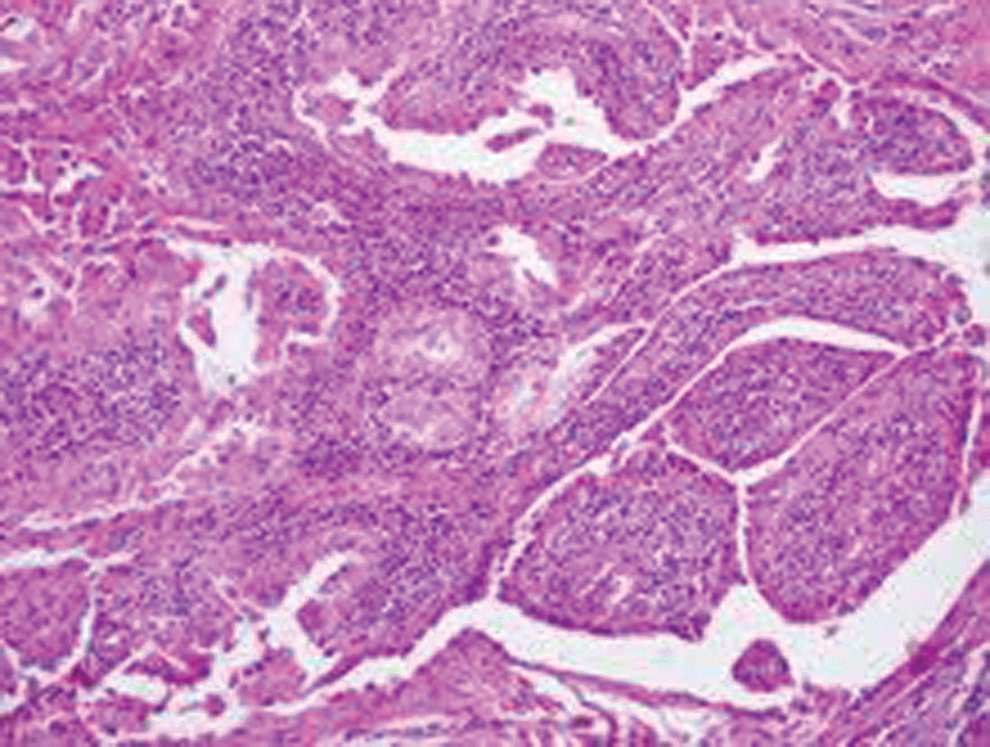
Warthin-variant PTC in a patient with Schmidt's syndrome.
Thyroid Cancer Friday Poster Clinical
Age 45 is used to establish staging in well-differentiated papillary thyroid cancer (PTC) using the AJCC/UICC TNM staging system. Our empiric clinical observation has been that patients aged 45 to 64 years appear to have similar long-term outcomes when compared to patients <45 years of age. We thus questioned the origin and accuracy of age 45 as the prognostic cut-off.
We performed a search of the Surveillance, Epidemiology, and End Result (SEER) database, using the SEERstat software obtained from their Website to obtain data for histology-confirmed papillary thyroid cancer. The following International Classification of Diseases for Oncology (ICD-O) codes were used, which are specific to PTC: 8050, 8260, 8340, 8341, 8342, 8243, and 8344. Data were stratified in 5-year categories by age at diagnosis from 20 to 84 years old, with patients 85 years of age and older categorized together. All stages, race/ethnicity groups, and sexes were included. A total of 53, 581 patients were identified with histologically confirmed PTC.
Overall 5-year survival remained above 90% for all age groups under 65 years. Patients 65 years and above had a progressively less-favorable prognosis with each advancing age group.
A review of the literature to determine the origin of this age marker appears to date back to an article by Byar, et al., published in European Journal of Cancer in 1979. This study was underpowered and not specific to well-differentiated thyroid cancer. While age at diagnosis appears to play a role in PTC outcomes, it appears that a more appropriate age marker for PTC prognosis is >65 years, as it defines a cohort of papillary thyroid cancer patients destined to have less than a 90% five-year survival. Use of this older age marker would result in downstaging of many patients and may be a more accurate reflection of the favorable prognosis of PTC, avoiding potentially additional unnecessary ancillary therapies and allaying patients' fears about the longevity with this condition.

PTC: 5-year survival by age at diagnosis.
PTC: 5-
Thyroid Cancer Friday Poster Clinical
Insular thyroid cancer is a rare, but aggressive, cancer that requires equally aggressive medical care. Recognition of this distinct type has profound implication on therapy.
A 62-year-old Caucasian man underwent total thyroidectomy and left-sided neck dissection after biopsy of a thyroid nodule was suspicious for follicular neoplasm. Pathology revealed insular thyroid carcinoma stage T4N1Mx. Postsurgical PET/CT scan showed an FDG-avid left neck mass, which led to re-exploration and left neck dissection.
Postoperatively, a contrast chest CT scan showed multiple pulmonary nodules and a stimulated thyroglobulin level of 1104 ng/mL. He underwent remnant ablation with 156.7 mCi of 131I. Post-treatment scan showed intense uptake in the neck and suspicious activity in both paramediastinal areas, mid-abdomen, and in the right sacroiliac joint region. This was followed by external beam radiation with 4,500 cGy to the neck and operative bed. His stimulated thyroglobulin level decreased to 465 ng/mL postablation; however, over the next five months, the value remained elevated in the 108–192 ng/mL range despite appropriate TSH suppression. Follow-up imaging showed persistent pulmonary nodules and a hepatic lesion on chest CT scan, negative 123I scan, and low-grade activity in the neck on PET/CT scan. Tyrosine kinase inhibitor therapy was discussed; however, this was not started then. Six months later, stimulated thyroglobulin was still 464 ng/mL. Thyrotropin-stimulated PET/CT scan showed activity in both lungs, a jugular lymph node and a subcutaneous left upper chest nodule. Repeat 131I ablation was done with 106 mCi. Post-treatment scan showed diffuse 131I uptake in the lungs, consistent with diffuse pulmonary metastatic disease. Six weeks later, unstimulated thyroglobulin level remained high at 501 ng/mL, and sunitinib was initiated.
Insular thyroid cancer is rare, but definitely not shy. Metastastic disease is often found at the time of diagnosis, and the mortality rate is high. Due to this, initial surgical management must be aggressive, and postoperative management must be very meticulous. In this case, we also demonstrate the use of tyrosine kinase inhibitors in an advanced poorly responsive metastatic disease.
IS THE REMNANT UPTAKE A POSTOPERATIVE ONCOLOGIC INDICATOR?
Thyroid Cancer Friday Poster Clinical
Although surgeon volume has been associated with fewer post-thyroidectomy complications, data on how surgeon volume impacts the completeness of resection are lacking. The purpose of this study was to examine the utility of remnant uptake on postoperative radioiodine scans as an oncologic indicator after thyroidectomy for differentiated thyroid cancer (DTC).
We conducted a retrospective review of patients undergoing total thyroidectomy for DTC and subsequent radioactive iodine (RAI) treatment at our institution from 2005 to 2011. Of the eight surgeons included, three were considered high volume, performing at least 35 thyroidectomies per year. Patients with distant metastases at diagnosis or poorly differentiated variants were excluded. To control for the effect of varying RAI doses, the remnant uptake was analyzed as a ratio of the percentage uptake to the dose received (uptake to dose ratio, UDR). Multivariate logistic regression was used to determine the influence of UDR on recurrence when combined with other established clinical and pathologic features associated with recurrence.
Of the 223 patients who met inclusion criteria, 21 patients (9.42%) experienced a recurrence. Those who recurred had a 10-fold higher UDR compared to those who did not recur (0.030 vs. 0.003, p=0.001). Similarly, patients with increasing postoperative thyroglobulin measurements (0.339 vs. 0.003, p<0.001) or who required additional neck surgery (0.028 vs. 0.003, p<0.001) also had significantly greater UDRs compared to those without these features. The UDRs of high-volume surgeons were significantly smaller than low-volume surgeons (0.003 vs. 0.025, p=0.002). When combined with other known predictors for recurrence, UDR (OR 3.71, C.I 1.05–13.10, p=0.041) was significantly associated with recurrence. The presence of lymph node metastases was also significantly associated with recurrence in this model (OR 9.5, C.I 2.88–37.97, p<0.001).
Remnant uptake is a useful postoperative oncologic indicator that can predict a patient's risk of disease recurrence and indicate the completeness of resection.
Withdrawn
Dept. of Physiology, ENCB, IPN, Mexico City, Mexico
Thyroid Hormone Action Friday Poster Basic
Thyroid hormones (THs) influence the central nervous system (CNS) function during development and in adulthood. The hippocampus, a brain area critical for learning and memory, is sensitive to TH insufficiency. Synaptic transmission in the hippocampus is impaired following modest degrees of hypothyroidism induced during development. The impact of the TH insufficiency on hippocampal synaptic function in the adult model however has not been as well studied—reports are limited and results inconsistent across laboratories. The present study was designed to assess the effects of adult-onset TH insufficiency on synaptic function in the dentate gyrus of the hippocampus of the rat.
Adult male rats were exposed to the goitrogen propylthiouracil (PTU: 0 or 10 ppm) through the drinking water for 1 month to reduce serum THs. This dose of PTU increased thyroid gland weight and reduced body weight gain and serum T3 and T4. Field potentials were recorded in the dentate gyrus under urethane anesthesia in animals warmed on a heating pad set to 36.5°C. In a second experiment, the contribution of hypothermia induced by hypothyroidism was assessed. Body temperature, brain temperature, and hippocampal field potentials were monitored in control and PTU-exposed animals.
In contrast to TH insufficiency induced during development, excitatory and inhibitory synaptic transmissions were only marginally impaired. However, response latencies were significantly increased in hypothyroid animals, and despite warming, body temperature in hypothyroid animals could not be adequately maintained. Hypothyroidism reduced both brain and body temperature, and this hypothermic response was exacerbated under anesthesia. Warming reduced latencies in hypothyroid animals, whereas cooling increased latencies in controls.
The alterations in field potential amplitudes and latencies are consistent with previous reports of brain temperature and hippocampal function. These data indicate that only modest changes in hippocampal physiology accompany TH insufficiencies induced in adulthood and provide clear evidence that synaptic delays in hypothyroid animals are mediated by brain hypothermia independent of the thyroid status (does not reflect EPA policy).
Radiation Oncology, Cleveland Clinic, Cleveland, OH
Thyroid Hormone Action Friday Poster Translational
Evidence has accumulated that
In this retrospective study, the courses of 3 hypothyroid solid-tumor patients on
Toxicity: there was no T3-related toxicity. Two patients initially experienced mild fatigue until an adequate individualized dosing schedule was established. Response: (see Table) All four patients experienced tumor regression with clinical benefit.
Selective T4 depletion was enabled by supplemental T3 in deteriorating cancer patients with aggressive solid tumors and associated with tumor regression and better outcomes. T3 may be preferable to T4 as a supplement in hypothyroid patients with an active cancer.
Response and Survival in High-Grade Tumors After T4 Depletion
Pre, pre T4 depletion; post, post T4 depletion, TSH (0.27–4.2 mU/L)/FT4 (0.93–1.7 ng/dL).
Thyroid Hormone Action Friday Poster Clinical
Resistance to thyroid hormone (RTH) is an inherited syndrome of reduced tissue responsiveness to thyroid hormone (TH) usually due to mutations in the thyroid hormone receptor β (TRβ). Few studies have been conducted to investigate bone and mineral metabolism in RTH. Objectives: To evaluate clinical and biochemical parameters related to the mineral metabolism in RTH.
Fifteen patients with RTH (RG), 9 adults (26–69 ys), and 6 children (2–12 ys) were compared to control subjects (CG). The diagnosis of RTH was made on clinical, biochemical, and molecular bases. Direct sequencing analysis of the TRβ gene revealed in 14 of these RTH individuals four reported mutations (c.949G>A, c.1358dupC, c.1313G>A and c.1357C>A) and one unpublished mutation (c.991A>C). The biochemical evaluation included serum total calcium (TCa), inorganic phosphate (Pi), alkaline phosphatase (AP), parathyroid hormone (PTH), Vitamin D (25-OHD), osteocalcin (OC), and fibroblast growth factor 23 (FGF-23). Creatinine clearance (CrCl) and renal threshold phosphate concentration (RTPC) were estimated. Bone mass was assessed by Dual X-ray absorptiometry.
There was no difference between groups in Pi, AP, PTH, 25-OHD, OC, FGF-23, and CrCl. Higher levels of TCa were observed in RG than in CG (p=0.048). RTPC was lower in RG than in CG (p=0.04). Additionally, it was verified disturbance on phosphate and calcium regulation by PTH in RG, while CG exhibited strong negative correlation between TCa (r=−0.56; p=0.003) and Pi (r=−0.7; p<0.0001) with PTH the RG lacks this association. Bone mass was decreased in adults patients at all sites, and significant difference was observed in the whole body (p=0.02) and femoral neck (p=0.02).
Our data reveal that patients with RTH have higher levels of serum TCa and lower bone mass than CG. Since TRα1 is the predominant TR in the skeleton, it is possible that these patients exhibit increased bone catabolism. Patients with RTH also presented lower RTPC, indicating a decreased threshold for renal loss of phosphate. Intriguingly, it was observed an alteration on TCa and Pi regulation by PTH. Our data challenge new studies to unveil the control of calcium and phosphorus homeostasis and fracture risk in these patients.
STRUCTURE AND FUNCTION RELATIONS IN THE HUMAN MONOCARBOXYLATE TRANSPORTER 8
Thyroid Hormone Metabolism & Regulation Friday Poster Basic
The human SLC16A2 gene encodes a specific thyroid hormone transporter, monocarboxylate transporter 8 (MCT8). Mutations in MCT8 lead to Allan-Herndon-Dudley syndrome, a severe mental retardation disease, which is characterized by an abnormal thyroid hormone constellation. The biochemical mechanism of MCT8 is still unknown, and there is no 3-dimensional (3D) structure available. We have presented a homology model of MCT8 based on the 3D structure of the bacterial glycerol-3-phosphate transporter. We investigated the homology model searching for a better understanding of the mechanism by which MCT8 interacts with and transports thyroid hormones. Analysis of the MCT8 homology model revealed two His–Arg pairs possibly involved in substrate recognition and substrate translocation. A His–Arg pair (responsible for T3 binding) is also found in the ligand-binding domain of the T3 receptor. Mutations of the conserved His and Arg residues in human MCT8 were biochemically investigated.
His192 and His415 were mutated to Gln, Phe, or Ala to reveal the importance of hydrogen bonds and hydrophobic interactions for T3 binding. Arg301 was mutated to Lys and Ala. MDCK1 cells were chosen for stable transfection of wild-type and mutated MCT8. The stably expressing cells were exposed to 125I-T3, and MCT8-mediated uptake was measured.
Mutations of His192, His415, and Arg301 did not impair protein expression or plasma membrane translocation, except the Arg301-to-Ala mutation, which failed to be stably expressed in MDCK1 cells. We found that His415 and Arg301 are critically involved in MCT8 function and change the T3 transport activity, while mutations of His192 do not play an important role.
Mutations of the conserved His and Arg residues helped to confirm the MCT8 homology model and identified amino acid residues involved in T3 transport.
Oncology, Medicine, Pharmacology&Physiology, OBGYN, Georgetown University Medical Center, Washington, DC
Thyroid Hormone Metabolism & Regulation Friday Poster Clinical
Single-nucleotide polymorphisms (SNPs) in genes involved in thyroid hormone metabolism may affect serum free-thyroxin (FT4), triiodothyronine (FT3), and thyroid-stimulating hormone (TSH) levels. We examined the possible effects of SNPs in the deiodinase (D1 and D2), thyroid hormone receptor beta (THRB), guanine nucleotide-binding protein, q polypeptide (GNAQ), thyroglobulin (Tg), POU class 1 homeobox 1 (POU1F1), thyroid-stimulating hormone receptor (TSHR), and solute carrier organic anion transporter family member 1B1 (SLCO1B1).
The 12 SNPs were identified in public access databases. We determined the genotypes for the identified SNPs in 288 healthy women (18–45 years), and related them to serum FT4, FT3, and TSH levels. After testing the Hardy–Weinberg equilibrium (HWE) and linkage disequilibrium (LD), we conducted linear regression analysis to access the association between the genotypes and the hormone levels. We also considered the effects of haplotypes of three SNPs (rs11206244, rs12095080, and rs2235544) for the same gene (D1). Participant smoking status was divided into three groups: active smokers, n=103; nonsmokers, n=99; and secondhand smokers, n=86. We examined the relationship between the identified SNPs and their smoking status. When statistically significant, we further investigated the modification effect of smoking on the thyroid hormone genetic pathway.
Except for the SNPs in TSHR and TSHRB, distribution of all genotypes is in HWE. The latter analysis found that genotype GG and AG for rs10512065 (GNAQ) is significantly associated with T4 level (p-values: 0.0210 and 0.0341, respectively); GG for rs225014 (D2) is significantly associated with T3 level (p-value: 0.0397); AA for rs10512065 (GNAQ), GG and AG for rs11206244 (D1), AC and CC for rs2235544 (D1), AA and GG for rs4149056 (OATP1B1) are significantly associated with TSH level (p-values: 0.0397, 0.0197, 0.0221, 0.0418, 0.0093, 0.0128, and 0.0067, separately).
We identified SNPs that are significantly associated with FT4 and FT3, and especially with TSH levels. Knowing the interaction between SNPs and hormone levels and the modifying effects of smoking can clarify the mechanism of smoking effect on these pathways.
Withdrawn
Endocrinology, University Medical Centre Groningen, Groningen, Netherlands
Thyroid Imaging Friday Poster Clinical
Surgery and high-dose radioactive iodine (131I) treatment are cornerstones in the treatment of differentiated thyroid cancer. Patients without 131I uptake on the post-therapeutic whole-body scan (WBS), but with detectable thyroglobulin during thyroxine withdrawal (Tg-off) as a sign of tumor presence, receive additional imaging for tumor localization, including 18-fluorodeoxyglucose positron-emission tomography (18F-FDG-PET). Objectives of this study were to assess the yield of 18F-FDG-PET in patients with negative WBS, but detectable Tg-off, and to determine whether the Tg-off level is clinically useful to predict a positive scan and to establish an optimal Tg-off cut-off value.
From 2002 to 2011, 52 patients with a negative WBS and detectable Tg-off were evaluated. Thirty-five PET scans were performed after initial treatment, and 17 after 131I treatment for recurrent disease. Thirty-one patients were on substitution therapy, 18 endogenous, and three recombinant human TSH (rhTSH) stimulated. Median Tg-off value was 8.40 ng/mL (0.18–1870.00). To determine the Tg-off cut-off value, a ROC curve was used.
Nine (17%) 18F-FDG-PET scans were true positive, three (6%) were false positive, 36 (69%) were true negative, and four (8%) were false negative, leading to a sensitivity of 69% and specificity of 92%. In 13%, a true positive scan led to a change in clinical management. The area under the ROC curve is 0.82 (95% CI 0.64–0.99, p<0.01), giving a Tg-off cut-off value of 38.00 ng/mL with a sensitivity of 67% and a specificity of 95%. Ninety percent of patients with a positive 18F-FDG-PET have a Tg-off>2.00 ng/mL before the WBS.
18F-FDG-PET after negative WBS with concurrent detectable Tg-off showed additional tumor localization in 17% of the patients, leading to a change in clinical management in 13%. A clinically useful Tg-off cut-off value predicting a positive 18F-FDG-PET could not be determined, but 90% of positive 18F-FDG-PET scans occurred in patients with a Tg-off>2.00 ng/mL.
School of Clinical and Experimental Medicine, University of Birmingham, Birmingham, United Kingdom
Thyroid Nodules & Goiter Friday Poster Basic
A role for dietary phytoestrogens in preventing thyroid disease remains controversial. Previously, we showed that thyroid-targeted overexpression of the proto-oncogene PTTG-binding factor (PBF) induced striking thyroid gland enlargement in transgenic mice (PBF-Tg)1.
We have now investigated whether PBF-Tg mice fed on diets with different amounts of phytoestrogens affect goitrogenesis and the development of hyperplastic lesions.
PBF-Tg mice fed on a low-phytoestrogen (PE) diet showed an approximate doubling of thyroid weight (mean=5.9±0.9 mg; n=75) at 6 weeks of age compared to PBF-Tg mice fed a high-PE diet (3.3±0.8 mg; n=98; p<0.0001). In contrast, the thyroid weight of wild-type (WT) mice increased only marginally when fed the low-PE diet (mean=2.17±0.5 mg; n=60) compared to the high-PE diet (1.8±0.4 mg; n=68). This increase in thyroid weight was not related to differences in body weight (25.0±1.9g v 24.7±2.4g; p=0.3) or thyroid function, as measured by serum analysis of T3 (172.7±25.9 versus 154.1±46.9 ng/dL, p=0.5), and T4 levels (2.7±0.7 versus 3.2±1.2 μg/dL, p=0.5), between PBF-Tg mice fed either the low- or high-PE diet, respectively. Analysis of mRNA showed a significant increase in cyclin D1 expression (1.6±0.2-fold, p=0.008), as well as mRNAs encoding for growth factor receptors known to induce thyroid cell proliferation, such as PDGFR (1.6±0.3-fold, p=0.0001), FGFR2 (1.5±0.2-fold, p=0.0001), and KDR (1.4±0.2-fold, p=0.003), in thyroids from PBF-Tg mice fed the low-PE diet compared to those on the high-PE diet. Furthermore, histological examination detected a greater frequency of focal hyperplastic lesions in thyroids from 12-month-old PBF-Tg mice fed the low-PE diet (83% of mice; n=10/12) versus the high PE diet (8.3% of mice; n=1/12; p<0.0001). No hyperplastic lesions were detected in thyroids from age-matched WT mice (n=0/12). Positive immunostaining with antibodies targeted to Rad6, Ung1, and Trex1 also indicated extensive DNA damage within hyperplastic lesions.
These results suggest that phytoestrogens can influence goitrogenesis and hyperplasia in PBF-Tg mice, thus implicating a role for phytoestrogens in modulating thyroid disease.
Read ML et al., (2011) Cancer Research 71(19), 6153–6164.
Thyroid Nodules & Goiter Friday Poster Clinical
The application of newly developed automatic periodic stimulation (APS) probes allows continuous intraoperative nerve monitoring (IONM) during thyroid surgery. The APS system was designed to enable early detection and warning of changes in nerve function, providing additional patient safety from traction injury. Herein, we provide our initial experience using this technology in a North American institution.
A retrospective review of our endocrine surgery database was performed to identify all patients who underwent thyroid surgery by a single surgeon. Continuous intraoperative recurrent laryngeal (RLN) and vagus nerve was monitored using the APS system. The vagus stimulation electrode was placed within the carotid sheath circumferentially encircling the nerve. Direct stimulation pulses were generated at 6–10-second intervals. The signal parameters of amplitude and latency were recorded in real time via the endotracheal tube sensor throughout the operation. Overtraction of the RLN was defined as 50% decrease in amplitude and 50% increase in latency. Routine preoperative and postoperative laryngoscopy was performed for all patients.
Twenty-eight procedures were performed on 27 consecutive patients with an average age (±SD) 46.4±15.4 yrs, 20 (74%) were women. A total of 37 RLN were at risk during these procedures. Using the APS system, added an average of five minutes to total operative time. Stable and repeatable signals in latency (5±1.6 msec) and amplitude (559±345 mV) were evocable at a current of 1±0.8 mA during 26 (92.8%) operations. The APS system was helpful in identifying intraoperative strain of the RLN in 6 (21.4%) procedures. Preoperative and postoperative flexible laryngoscopy comparison revealed no instances of vocal cord palsy or paralysis. Furthermore, we attribute no complications to the use of a vagus electrode.
Our initial data demonstrate that continuous IONM using the APS system is safe and feasible. This new adjunct can provide additional protection by identifying early intraoperative strain and possible risk of traction injury to the RLN.
GRAVES' DISEASE IN PREGNANCY PRESENTING WITH FETAL GOITER
Thyroid Nodules & Goiter Friday Poster Clinical
Treatment of Graves' disease during pregnancy with antithyroid drugs is challenging and may result in development of fetal hypothyroidism and goiter. Fetal goiter can cause tracheal compression and may compromise fetal development. Limited data are available on the management of fetal goiter in mother with hyperthyroidism and fetus with hypothyroidism. We have described administration of levothyroxine into amniotic fluid that resulted in complete resolution of the goiter and delivery of normal infant.
A 30-year-old G3P1011 Caucasian woman first diagnosed with Graves' disease in 2009 failed management with propylthiouracil and was to be treated with radioactive iodine. During pretreatment, work-up patient was found to be pregnant. She was maintained on methimazole and propanolol during her pregnancy. Laboratory data at 22 weeks showed an elevation of free T4 and profound suppression of TSH. In the third trimester, a fetal goiter was noted on ultrasound (see Figure) causing notable extension of the fetal head. At 30 weeks, cordocentesis was performed and showed fetal hypothyroidism, with a fetal TSH 9.24 mIU/mL (0.34–5.6) and free T4 of 0.52 ng/mL (0.5–1.25). Using an amniocentesis needle, weekly administrations of Levothyroxine into the amniotic fluid were conducted for management of fetal hypothyroidism. At 30 6/7 weeks, 300 μg Levothyroxine was administered in the amniotic fluid, followed by 350 μg at 31 5/7 and 32 5/7 weeks.
The fetus responded promptly with resolution of the goiter on ultrasound after these three treatments. Patient was delivered via cesarean section at 36 weeks for fetal indications. Infant did not have a goiter at time of delivery, and ultrasound of the infant's thyroid showed increased vascularity. Infant's bloodwork after delivery showed a TSH of 10.9450, a total T3 of 0.840, and a free T4 of 0.53.
Antepartum management of fetal goiter may be achieved via amniocentesis administration of Levothyroxine, yet there remains a paucity of data in the literature regarding dose and frequency of treatment. Our data may help to determine the best approach and guide other physicians in dose of Levothyroxine, route of administration, and therapy for fetal goiter secondary to fetal hypothyroidism.
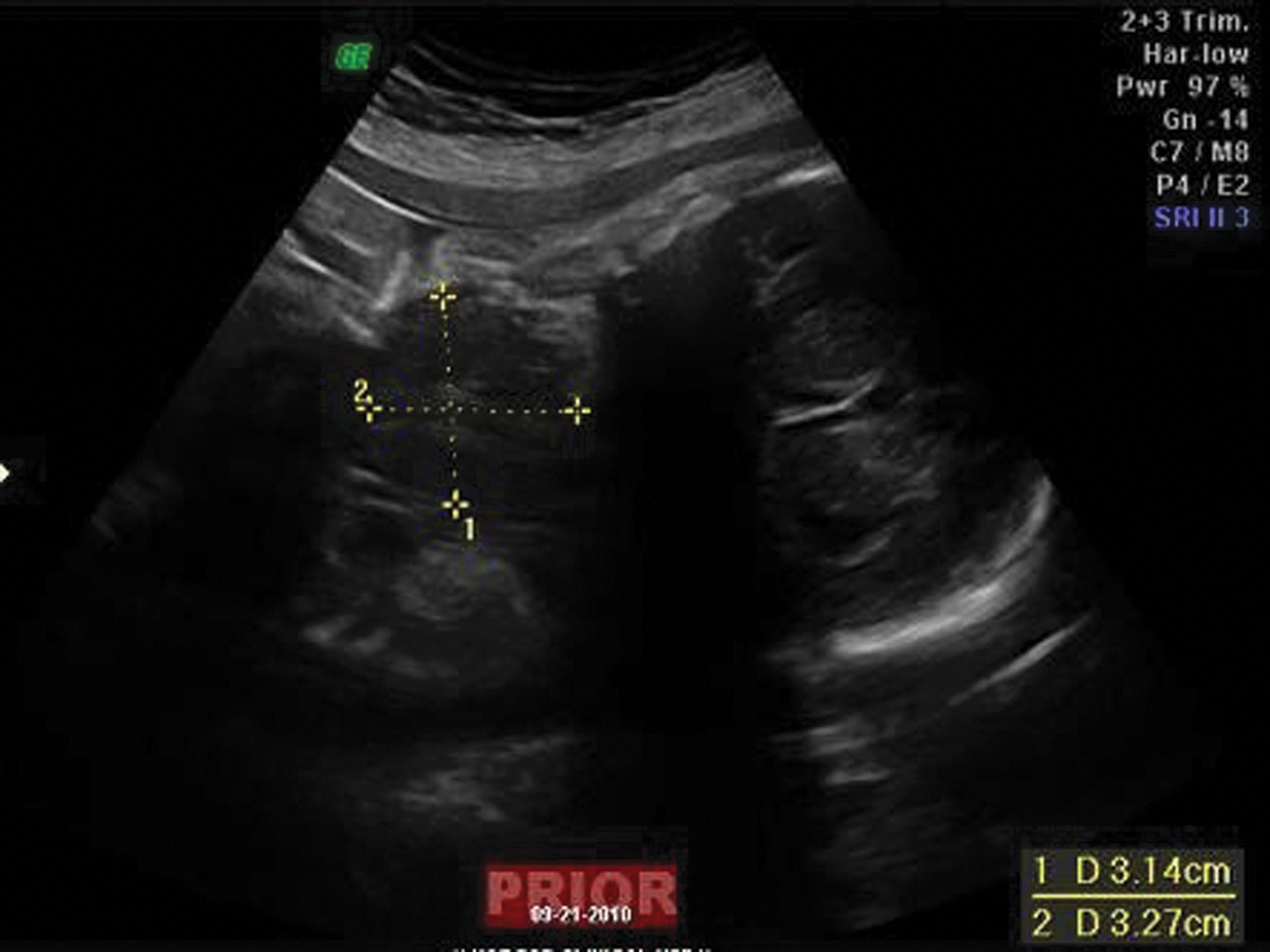
Fetal ultrasound in the 3rd trimester showing fetal goiter.
Thyroid Nodules & Goiter Friday Poster Clinical
Approximately 200 cases of parathyroid cysts have been described in the literature to date. A neck mass, which drains clear colorless fluid on fine-needle aspiration (FNA) with a quantified high concentration of parathyroid hormone (PTH), is its classic description. As seen in the literature, these cysts are usually nonfunctional and treated with recurrent FNAs. We present a single surgeons' experience with 9 parathyroid cysts and review their diagnosis, management, and need for operative intervention.
A review was conducted of all patients with a diagnosis of parathyroid cyst seen by a single surgeon at a Head and Neck clinic in a tertiary care referral center. Data on patient demographics, serum biochemical testing, FNA characteristics and management were examined.
Nine patients were identified with a diagnosis of parathyroid cyst. All but one was a woman with a mean age of 50. All had a serum ionized calcium and PTH level within the normal range. The mean cyst size at first presentation was 4 cm and aspirated 7.1 mL of clear colorless fluid. The PTH of the fluid had a mean concentration of 287.4 pg/mL. Five of the nine patients were treated with operative management, mostly due to multiple recurrences after aspiration. One cyst was removed as a result of compression symptoms and one due to patient preference.
Consistent with the previously described literature, parathyroid cysts are rare nonfunctioning neck masses filled with PTH-concentrated clear colorless fluid. They may be amenable to serial fine-needle aspiration. While most may be drained repeatedly, many eventually move on to definitive excision for a variety of reasons, namely patient preference, accelerated recurrence, and compressive symptoms.
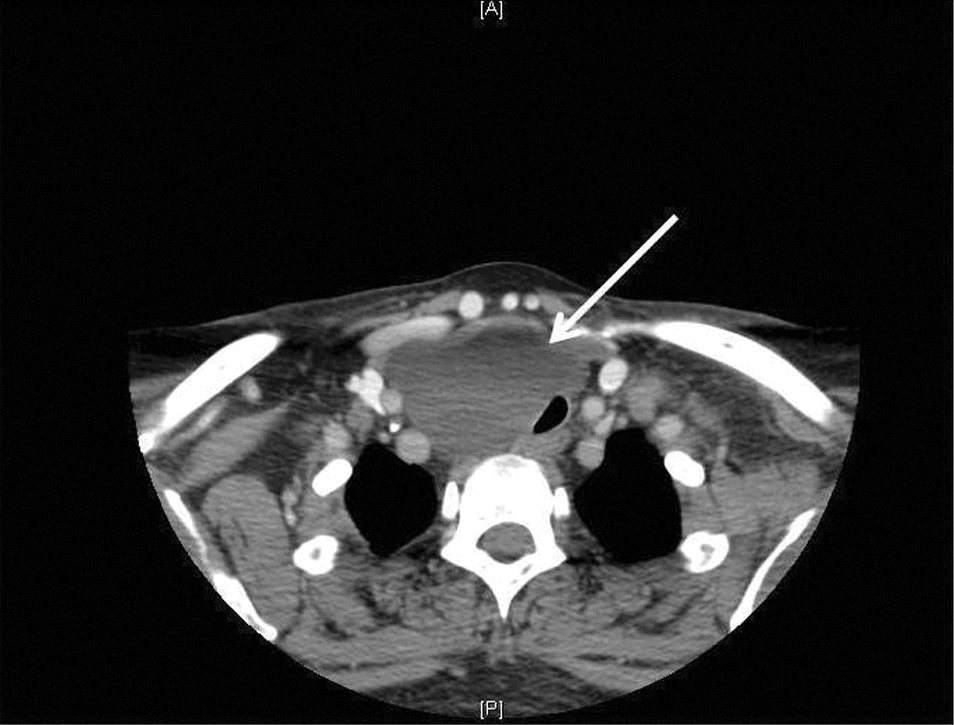
Computed Tomography Axial image. Note the parathyroid cyst (arrow) compressing the trachea.
Thyroid Nodules & Goiter Friday Poster Clinical
Primary hyperparathyroidism is rarely caused by a functioning adenoma within the mediastinum. These patients experience a complicated course often requiring multiple localization studies and surgical procedures. Once a mediastinal adenoma is found, debate still exists on what approach might allow for the best access to the mediastinum. We present a case series to address the relevant issues.
We retrospectively reviewed our prospectively collected database of patients seen at a single center between 2001 and 2011. The charts of those meeting criteria for a mediastinal parathyroid adenoma were identified. Inclusion criteria were 1) biochemical diagnosis of primary hyperparathyroidism and 2) mediastinal parathyroid adenoma excised for curative resection.
Nine patients were identified with mediastinal parathyroid adenomas within the study period. Mean age was 58 years (SD 18.3), and ionized calcium and parathyroid hormone level at diagnosis were 1.50 mmol/L (SD 0.16) and 31.8 pmol/L (SD 24.3), respectively. All patients had preoperative Computed Tomography (CT) of the neck and chest, as well as Sestamibi scan, with a sensitivity of 44% and 33%, respectively. All patients were biochemically cured. After the first operative intervention, 4 of 9 patients were cured. In the remaining cases, the failed first operation included a partial thyroidectomy and thymectomy (3/5 [60%]) and the other 2/5 (40%) had a parathyroid adenoma in the neck as well. After a first operation and biochemical persistence of hyperparathyroidism, patients had reimaging or review of previous CT and Sestamibi scan. One patient had Magnetic Resonance Imaging (MRI) and selective venous sampling. Two patients (22%) required short upper sternotomy for cure, as their mediastinal adenoma was unreachable from a cervical approach. These patients stayed postoperatively in hospital 2 and 3 days, respectively.
Although mediastinal adenomas are rare, appropriate preoperative localization may be helpful in avoiding reoperation. Once localized, a short upper sternotomy may be done with minimal morbidity.
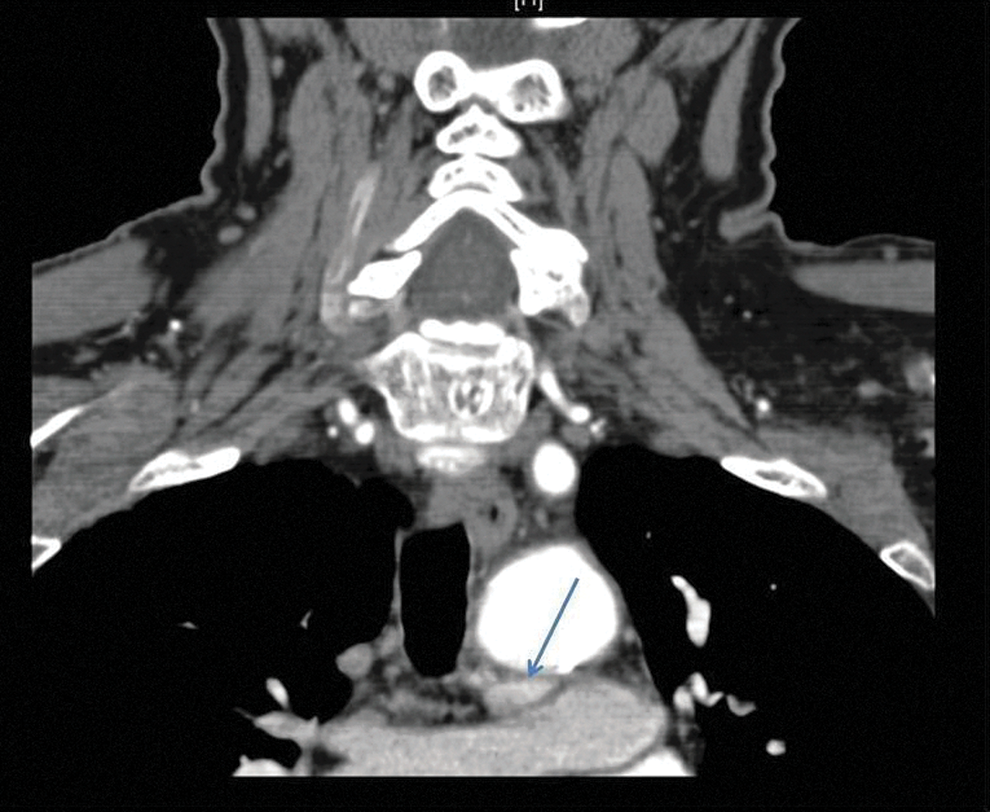
Coronal slice of Computed Tomography of the neck and chest. Parathyroid adenoma is seen inferior to the aorta (arrow).
Saturday, September 22, 2012
Endocrinology and Diabetes Center, Riyadh Military Hospital, Riyadh, Saudi Arabia
Thyroid Cancer Saturday Oral Clinical 2:10 PM
TSH- stimulated thyroglobulin (STG) is the most sensitive method to monitor differentiated thyroid cancer (DTC) patients for residual or recurrent disease. The objective of this study was to determine the completeness of response and frequency of disease in DTC patients who had total or near-total thyroidectomy and radioiodine remnant ablation (RRA) and STG of 0.4–2.0 μg/L at 6–10 months after RRA. We also assessed risk factors predictive of recurrence at 10–24 months after RRA and at final follow-up at a median of 6 years of follow-up.
Eight hundred thirty-nine consecutive patients were retrospectively reviewed, and 95 adult DTC patients followed for a median 6 years (range 2–10 years) after thyroidectomy, and RRA were identified who had a STG of 0.4–2.0 μg/L at 6–10 months after RRA. The patients were classified as having incomplete response or no evidence of disease (NED) at 10–24 months after RRA based on STG, and cross-sectional/functional imaging. The patients were also evaluated and classified at final follow-up visit.
At 10–24 months after RRA, incomplete response was identified in 54 patients (57%). Thirty-eight out of 54 (70.4%) patients had imaging/pathological evidence of disease. The remaining 16 patients (29.6%) had biochemical evidence of disease without structural evidence of disease. Forty-one patients (43%) were classified as having NED at 10–24 months after RRA. Twenty-seven patients (66%) did not receive further radioactive iodine (RAI) therapy, and remained disease-free at a median follow-up of 6.5 years. We determined that a STG level above 0.6 μg/L at 6–10 months after RRA had optimal sensitivity (83.3%), specificity (56%), positive predictive value (71.5%), and negative predictive value (72%) of detecting incomplete response at 10–24 months after RRA. Twenty-three out of 43 ATA low-risk patients had incomplete response after first RRA, and of these 5/23 (21.7%) had recurrent/persistent disease at long-term follow-up.
DTC patients with STG of 0.4–2.0 μg/L at 6–10 months after RRA have to be evaluated for high probability of incomplete response after first RRA irrespective of initial risk stratification, as even ATA initial low-risk category patients may have up to a 21.7% chance of persistent/recurrent disease in long-term follow-up.
The Characteristics of Patients 10–24 Months After Radioiodine Remnant Ablation
Second RAI therapy was given before 10–24-month evaluation.
Thyroid Nodules & Goiter Saturday Oral Clinical 2:25 PM
Fine-needle aspiration cytology provides an accurate diagnosis for most thyroid nodules. However, 10%–25% of nodules prove suspicious for follicular neoplasm, or are atypical (indeterminate), requiring surgical resection for definitive diagnosis. We recently began to use a Gene Expression Classifier (GEC; Afirma™, Veracyte Inc., San Francisco, CA) to further evaluate these nodules. Initial reports claim 96% negative predictive value for the ∼50% of indeterminate nodules that prove GEC benign. We report here our initial experience with Afirma.
We phased in use of the GEC, using our own cytopathology to identify appropriate samples for GEC testing, starting in May 2011. We collected samples from all patients undergoing FNA biopsy who gave verbal consent. Patients with indeterminate cytology were offered GEC testing. Those whose GEC proved benign were offered ultrasound follow-up as an alternative to surgery, while a suspicious GEC led to a recommendation for thyroid surgery. We reviewed surgical and pathology reports from patients undergoing surgery and follow all remaining patients by ultrasound.
We biopsied 1014 nodules from 771 eligible patients, of which 807 (79.5%) were cytologically benign and 75 (7.4%) malignant or suspicious for malignancy. Of the 68 indeterminate samples, 44 patients agreed to GEC analysis. Six samples (13.6%) yielded no information. Of the remainder, 10 (26%) were GEC benign; 1 patient in this group chose surgery for cosmesis, while the other 9 chose follow-up. We have operated on 23 (82%) of the 28 GEC suspicious nodules, confirming malignancy in three patients (13%) (one each of papillary, follicular, and Hurthle cell carcinoma).
Our initial experience with the Afirma GEC in indeterminate thyroid nodules finds a lower than previously reported rate of GEC-benign samples (26% versus 53%; p<0.01). We also find a much lower rate of malignancy in GEC-suspicious nodules (13% versus 38%; p<0.01) than in previously presented data. If confirmed, these findings might significantly alter the cost–benefit ratio of the test. These data strongly support the need for independent confirmatory studies before widespread implementation of this or other molecular adjuncts to thyroid cytopathology.
Pediatrics, University of Toronto, Toronto, ON, Canada
Disorders of Thyroid Function Saturday Oral Clinical 2:40 PM
Thyroid hormone is essential for brain development, particularly neurogenesis and neuronal migration. Rodents exposed gestationally to maternal hypothyroidism show atypical cortical layering and heterotopic neurons. Children born to hypothyroid women (HYPO) show reduced IQ, selective cognitive deficits, and cortical gray matter reductions (Rovet et al., ITC 2010). However, no study has as yet investigated whether these reflect structural abnormalities in the cortex.
Participants were 44 10–12-year olds, 20 HYPO, and 24 controls from a larger cohort followed since birth. All received MRIs on a 1.5T GE magnet. In FreeSurfer v4.4, each anatomical scan was processed using the default pipeline. Groups were compared within FreeSurfer using the General Linear Model with results corrected for multiple comparisons and in SPSSv19 comparing the thicknesses of specific cortical regions. Within the HYPO group, results were analyzed by severity of maternal hypothyroidism.
HYPO showed discrete areas of cortical thinning and cortical thickening relative to controls (see Figure). In HYPO, thinner cortices (p<0.05) were observed in insula (left) and temporal (left fusiform), parietal (right inferior, precuneus), and frontal lobes (right middle frontal), while thicker cortices were seen in parietal (left superior), frontal (left and right superior, left rostral middle), temporal (right pole, right inferior), and occipital (right pericalcarine) lobes. Within HYPO, maternal hypothyroidism severity was associated more with cortical thickening than thinning.
Cortical thickening in HYPO may reflect neuronal migration abnormalities caused by maternal TH insufficiency effects on cerebral cytoarchitecture. In contrast, cortical thinning may reflect abnormalities in neurogenesis or reduced neuropil. Notably, thickening was more pronounced superiorly in left hemisphere and posteriorly in right hemisphere, whereas thinning was more pronounced inferiorly and medially. Overall, these subtle, but diverse, alterations in cortical morphology suggest the human cortex needs adequate maternal thyroid hormone during pregnancy for proper development. The functional implications of these alternations in cortical morphology need to be determined.
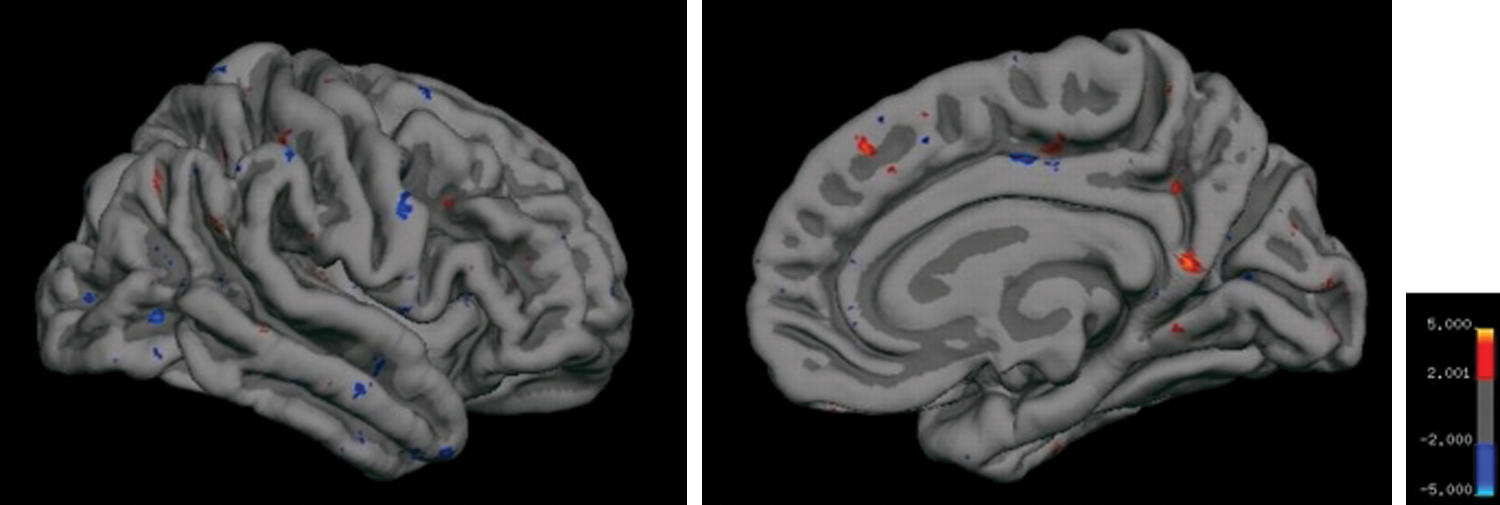
Cortical thickness pial maps of right hemisphere showing comparison between 24 Controls and 20 HYPO. Areas shown in red signify cortical thinning in HYPO, whereas areas in blue signify cortical thickening. Similar, but fewer, effects were observed in left hemisphere (not shown).
Thyroid Cancer Saturday Oral Clinical 2:55 PM
Integrin αvβ3 has been proposed as a potential imaging target with radionuclide-labeled RGD molecular marker for the estimation of tumor angiogenesis, yet has not been applied in differentiated thyroid cancer (DTC) patients with RAI (radioactive iodine) refractory lesions. The current study was conducted to assess the potential of integrin αvβ3 imaging in detection of RAI-refractory DTC lesion by using 99mTc-3PRGD2, thus providing a feasible antiangiogenetic therapeutic target.
A total number of 10 DTC patients (M 2, F 8; mean age±SD, 56.4±9.8y, range 42y-73y) with multiple RAI refractory metastases were recruited, all of which had both elevated thyroglobulin (Tg) levels (Tg+) and negative 131I whole-body scan (131I WBS−). Clinical data were collected, including history, 131I WBS, contemporary CT, ultrasonography, TSH, Tg, and anti-Tg. One or two target lesions were selected on the contemporary CT images by RECIST 1.0 for all patients, and 7 of which were chosen for calculation of lesion growth rates within recent 3 months. WBS at 30 min and regional SPECT over lesions at 1 h were performed, respectively, after injection of 99mTc-3PRGD2 intravenously. Two experienced nuclear medicine physicians read the images in a blinded fashion. The tumor-to-background ratios (T/B) were calculated for further analysis.
All the target RAI-refractory metastatic lesions were identified as positive on 99mTc-3PRGD2 SPECT images. There was a significant correlation between the mean T/B ratios and mean growth rates of target lesions (r=0.878, p=0.009).
The RAI-refractory 131I WBS− Tg+ metastatic lesions can be traced by 99mTc-3PRGD2 imaging, which means these lesions are highly neovascularized. 99mTc-3PRGD2 angiogenesis imaging can be used for localization and growth evaluation of RAI refractory lesions, providing a new therapeutic target and a novel imaging modality to monitor the efficacy of certain antiangiogenetic therapy.
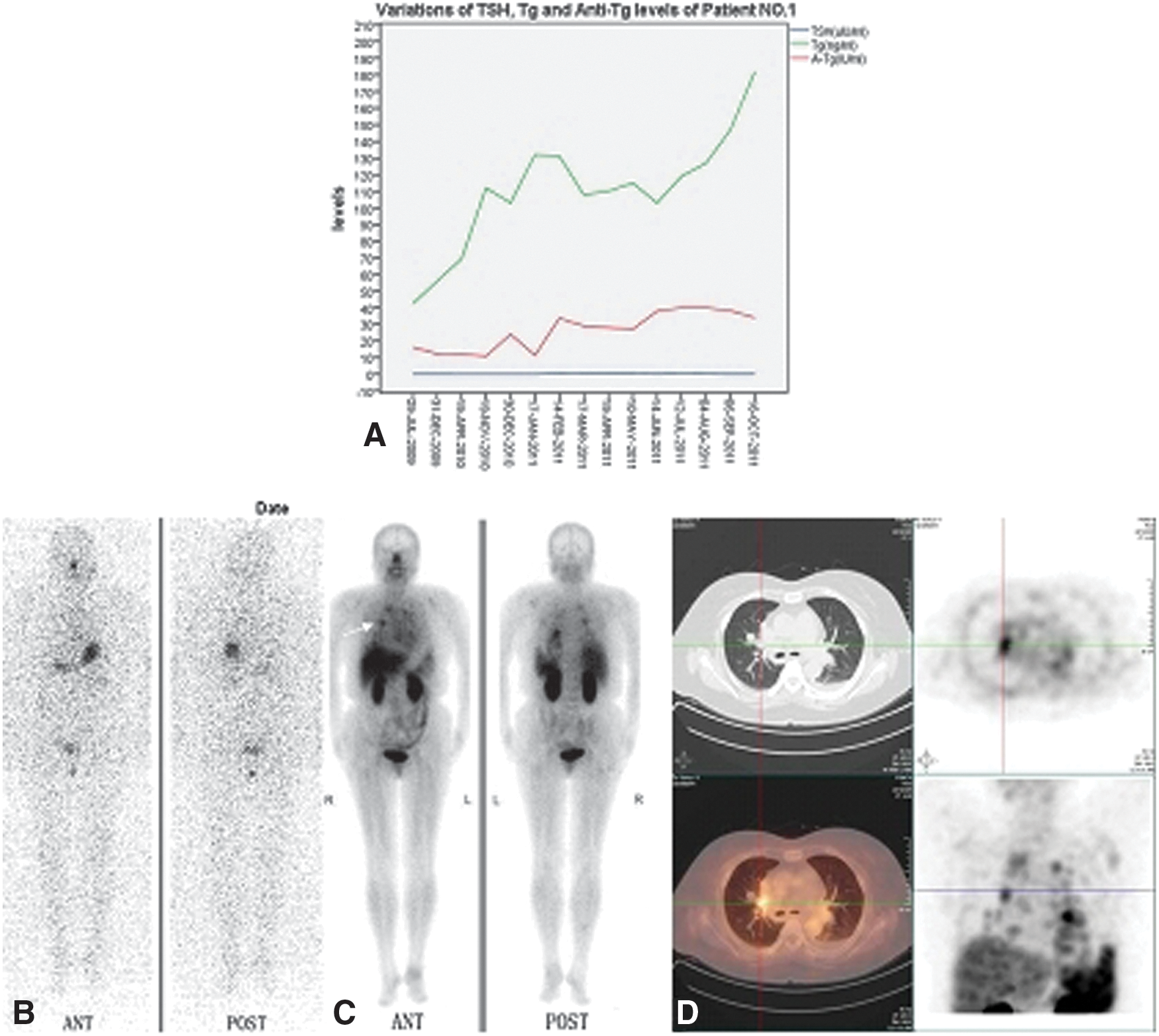
Patient No.1 with elevated levels of stimulated thyroglobulin (ng/mL) and thyroglobulin antibodies (IU/mL) with corresponding TSH
Thyroid Cancer Saturday Oral Translational 2:10 PM
The currently used panel of mutations for preoperative diagnosis of cancer in thyroid FNA samples does not include all known mutations, as this would be associated with high cost and require large amount of nucleic acids. The availability of next generation sequencing (NGS) has opened a possibility of efficient detection of multiple mutations in limited samples without significant cost increase. In this study, we evaluated the utility of a novel NGS platform, Ion Torrent PGM (Life Technologies) for clinical testing of thyroid FNA and surgical specimens.
Forty thyroid samples (4 FNAs, 25 frozen, and 11 FFPE tissues) previously tested using single-gene approach were analyzed for 740 mutations in 46 genes using AmpliSeq Cancer Panel on Ion Torrent PGM platform. All FNA samples had indeterminate cytologic diagnosis and resected specimens consisted of 25 papillary thyroid carcinomas (PTC), 6 anaplastic carcinomas (AC), 2 follicular carcinomas (FC), and 3 normal thyroid tissues. Sequencing was performed using 318 Chip with 8 barcoded samples per run.
Using small amount (10 ng) of DNA, we were able to successfully test all samples (including FNAs) for more than 740 mutations in 46 genes. The NGS Ion Torrent platform allowed to detect all mutations in 10 previously positive samples. However, additional mutations were found in thyroid FNAs and in resected specimens, including RET M918T (1 MC), KRAS Q61R (4 FVPTC), NRAS G12V (1 FVPTC), PIK3CA E707K (1 PTC), and TP53 L194R (1 AC). In addition, germline mis-sense variants were detected in the MET, ATM, and KDR genes. RET M918T was initially detected in the FNA sample with suspicious for malignancy cytology and allowed to establish the definitive diagnosis of medullary carcinoma preoperatively. The sensitivity of mutation detection was 10% and turnaround time was 72 hours.
Targeted sequencing using AmpliSeq Cancer panel on Ion Torrent platform allows to test for a broad spectrum of mutations and may improve further the sensitivity of molecular diagnosis in thyroid surgical and FNA samples.
Surgery, Walter Reed National Military Medical Center, Bethesda, MD
Thyroid Cancer Saturday Oral Translational 2:25 PM
Determining which cases of papillary thyroid cancer (PTC) are more likely to result in recurrence of or death due to disease is useful to counsel patients on treatment regimens and prognosis. Many existing risk-scoring systems exist, including EORTC, AMES, MACIS, and AJCC TNM Staging System (TNM). The objective of this study was to evaluate the machine-learned Bayesian Belief Network (ml-BBN) prognostic risk models of recurrence and mortality using registry data. We sought to compare these models to existing scoring systems and to evaluate levels of comparability between systems.
Under IRB protocol approval, we analyzed 1,630 Department of Defense Tumor Registry records, and 104 variables stratified into time cohorts for classification. Cohorts were defined by follow-up duration (5-year and 7-year cohorts) for statistical modeling. BBNs were trained using machine learning and validated using 10-fold cross-validation.
The ml-BBNs were robust, showing AUCs for recurrence and mortality of 0.70 (95% CI: 0.58–0.82) and 0.69 (95% CI: 0.61–0.78) at 5 years, 0.75 (95% CI: 0.64–0.86) and 0.79 (95% CI: 0.68–0.89) at 7 years from time of operation. First-degree associates of recurrence at both 5 and 7 years included positive family history and AJCC N Stage. First-degree associates of mortality at 5 years included age at diagnosis, gender, N stage, and M stage; at 7 years, they are age and gender. A cohort was identified that contained all the features of the ml-BBNs and the major PTC risk-scoring systems (n=235) at 5 years, and high-risk populations were compared across risk-scoring systems. Sensitivity, negative and positive predictive value for mortality was as follows: EORTC: 20%/95%/60%; AMES: 13%/94%/40%; MACIS: 27%/95%/57%; TNM: 27%/95%/15%; ml-BBN, 67%/97%/15%.
ml-BBNs are able to provide robust estimation of risk of PTC recurrence and mortality. These BBN models provide equivalent, and in some instances, superior, performance to existing PTC risk-scoring systems. These initial findings are promising and warrant further development and prospective validation of an ml-BBN PTC risk scoring system in a larger independent test population.
Leibniz Institute for Age Research/Fritz Lipmann Institute, Jena, Germany
Thyroid Hormone Metabolism & Regulation Saturday Oral Basic 2:40 PM
The monocarboxylate transporter Mct10 (Slc16a10; TAT-1) does not only facilitate the transport of aromatic amino acids but also accept thyroid hormones (THs) as substrates. In mice, Mct10 is present in the kidney, liver, and thyroid where it shows an overlapping expression pattern with the TH transporter Mct8. We therefore hypothesized that Mct10 may act in concert with Mct8 in mediating cellular uptake and/or efflux of TH.
To assess the physiological contribution of Mct10 to the tissue-specific TH passage, we determined serum TH levels, TH transport, TH tissue content, and the expression levels of TH-regulated gene products in various organs of Mct10 ko, Mct8 ko, and Mct10/Mct8 double knockout (dko) mice.
While Mct10 ko animals did not display any abnormalities in TH metabolism and action, Mct10/Mct8 dko mice exhibited strongly elevated serum T3 levels in the presence of normal T4, indicating that the low serum T4 concentrations characteristic for Mct8 deficiency can be normalized upon the simultaneous inactivation of Mct10. As a consequence, the brain of Mct10/Mct8 dko mice was in a less hypothyroid state than the CNS of Mct8 ko mice. In contrast, peripheral organs such as the liver, kidneys, and thyroid were more severely affected by the deletion of both TH transporters. While Mct8 ko mice already showed increased TH concentrations and action in these organs, the tissue TH content was even further elevated in Mct10/Mct8 dko mice.
Overall, our data indicate that both TH transporters may be involved in mediating preferentially the efflux of TH from peripheral organs.
Nuclear Medicine, Peking Union Medical College Hospital, Beijing, China
Disorders of Thyroid Function Saturday Oral Basic 2:55 PM
Striatum dopaminergic activity is often observed to be related to abnormal thyroid function. We established a murine model of Graves' disease through lipoinfection and evaluated changes in striatum dopaminergic activity in these animals.
We linked pCDNA3.1(+) or pUBC to cDNAs of human thyrotropin receptor (TSHR) or TSHR, a subunit to yield four plasmids, which were coupled into liposome and then injected intramuscularly into female balb/c mice. The mice were bled for assays of thyroid hormone as well as anti-TSHR antibodies (TRAbs), and their weight were observed after each immunization. 11C-CFT PET imaging was carried out in representative individuals.
Weight gain in the immunized group was slower than control (p<0.05). Serum TRAb concentration was also obviously elevated. cDNA of TSHR A subunit resulted in even slower weight gain (p<0.001) and even faster TRAb elevation than that of full-length TSHR. Higher fT4 (p=0.023) than control was observed, which is reversely related to weight gain. Lower SUV and %ID/g was observed in immunized mice, with an extent correlated to elevation of fT4.
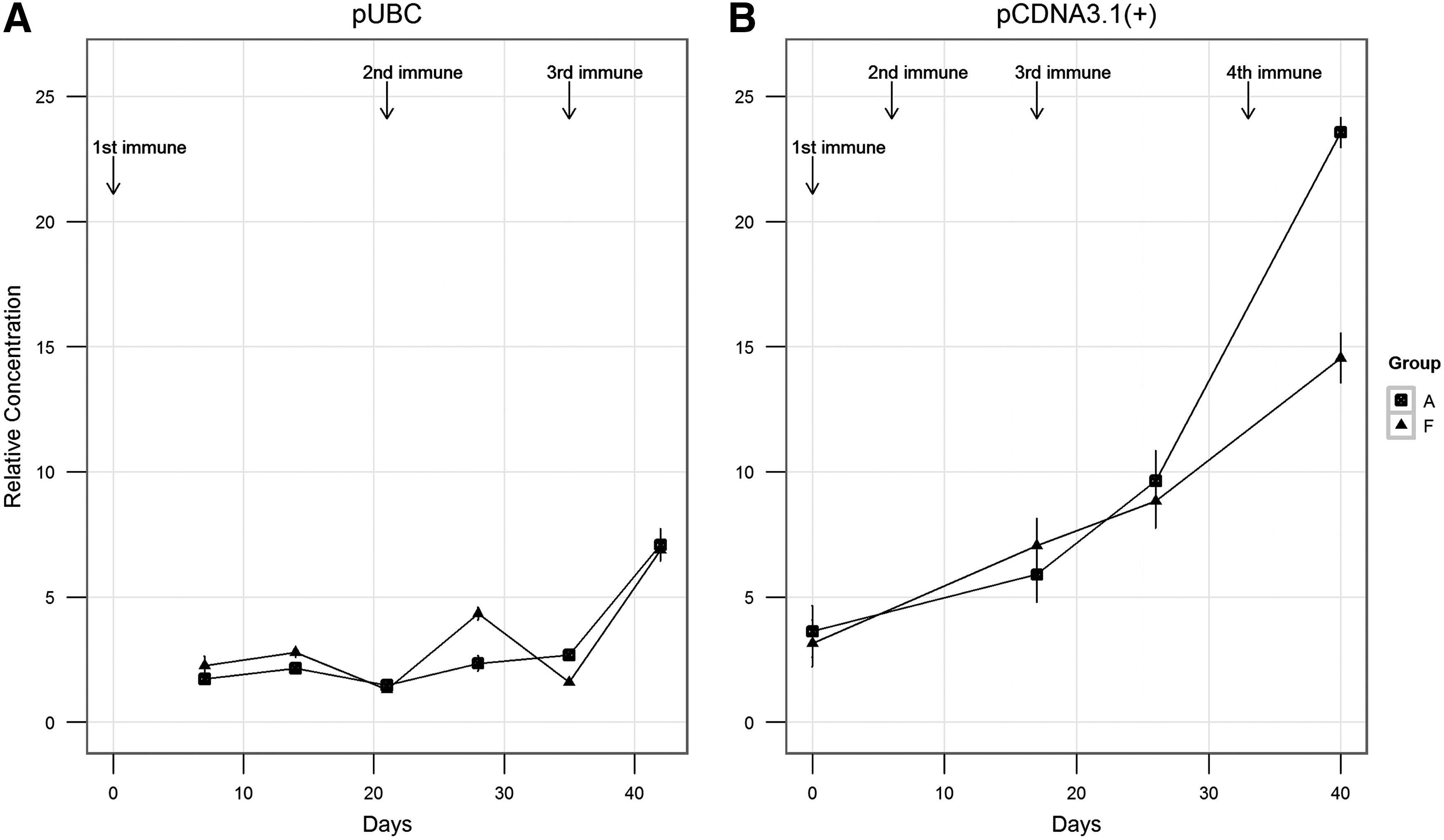
To immunize with liposome containing pCDNA3.1(+) linked with cDNA of TSHR A subunit is an effective method to induce Graves' disease in female balb/c mice. 11C-CFT PET imaging is a promising means to study changes in striatum dopaminergic activity in this model.
Relative concentration of serum thyrotropin receptor (TSHR) autoantibodies in animals transfected with the vector (A) pUBC and (B) pCDNA(+). WT: control group; Asub: animals immunized with cDNA of TSHR A subunit; full: animals immunized with cDNA of.
MOLECULAR CERTITUDE—HOW ONE TSH RECEPTOR ANTIBODY INDUCES THYROCYTE PROLIFERATION WHILE ANOTHER INDUCES APOPTOSIS
Autoimmunity Saturday Poster Basic
Antibodies to the TSH receptor (TSHR-Abs) may have stimulating, blocking, or neutral actions on the thyroid cell. In keeping with this, we have shown previously that all such TSHR-Abs may have distinct signaling imprints on binding to the TSHR, and that such events can have very different functional consequences for the cell. In particular, there is a great contrast between stimulating TSHR-Abs, which can induce thyroid hormone synthesis and secretion and thyroid cell proliferation, while so-called neutral TSHR-Abs may induce thyroid cell apoptosis under appropriate conditions.
Using time-lapse live-cell imaging of FTRL-5 cells, we have observed that labeled stimulating TSHR-Abs induced degradation of the resulting internalized antibody–receptor complexes by 24 hours. Using direct immune staining and Western blot analyses, we showed that cellular stress proteins such as HSP60 and SOD were suppressed, and that such suppression was lost by inhibition of the cAMP/PKA pathway.
By day 3, cell proliferation was activated. In contrast, imaging the effects of labeled neutral TSHR-Ab demonstrated a delayed degradation of internalized antibody–receptor complexes accompanied by multiple cellular stresses, and were still present at 72 hrs. Western blotting of phosphorylated signaling molecules indicated activation of the Ga13/Rho/PKC-d/p38 pathway. In addition, there was inhibition of antiapoptotic proteins Bcl-2/Bcl-xL and elevation of proapoptotic proteins Bax/Caspase-3 leading to apoptosis. Confirmation of these internalization and signaling patterns was obtained by using selective kinase inhibitors and blocking of internalized immune complexes using dynamin (a GPCR-specific inhibitor that prevents clathrin-coated pit internalization).
Our findings indicate how signaling diversity induced by different TSHR-Abs regulate cellular fate. While stimulating TSHR-Abs may rescue cell death and induce thyrocyte proliferation, neutral TSHR-Abs may aggravate the local inflammatory infiltrate within the thyroid or in the retro-orbit by inducing cellular apoptosis, a phenomenon known to activate innate and by-stander immune reactivity via DNA release from the apoptotic cells (supported by DK 080459, DK052464, and DK069713).
Division of Diabetes, Metabolism, and Endocrinology, Showa University School of Medicine, Tokyo, Japan
Autoimmunity Saturday Poster Clinical
The etiology of autoimmune thyroid diseases (AITDs), such as Graves' disease (GD) and Hashimoto's thyroiditis (HT), is largely unknown. However, genetic susceptibility is believed to play a major role. Recently, a study from China identified two new risk loci (6q27 and 4p14) for GD and confirmed four previously reported loci (in the major histocompatibility complex, TSHR, CTLA-4, and FCRL3) using a genome-wide association approach (Nat Genet, 43:897–902, 2011).
We genotyped the two single-nucleotide polymorphisms (SNPs) (rs9355610 and rs6832151) at these loci in 456 Japanese patients with AITD (286 with GD, 170 with HT) and 221 matched Japanese control subjects. Two SNPs were analyzed by the high-resolution melting and unlabeled probe methods. Case–control association studies were performed using the χ2 and Fisher's exact tests with Yates correction.
We found a significant allelic association between AITD and rs9355610 located in 6q27 (p=0.023). GD was significantly associated with this SNP (p=0.0055), while HT showed no significant associations with any SNPs. Moreover, when patients with GD were stratified according to Graves' ophthalmopathy (GO), there were no allelic associations with GO.
These findings suggest the presence of AITD susceptibility genes, especially in distinct subgroups of GD, in or near 6q27.
Dept. of Medicine I, Gutenberg University Medical Center, Mainz, Germany
Autoimmunity Saturday Poster Clinical
Scarce data exist on the role of thyroid-stimulating autoantibodies (TSAbs) in the management of Graves' disease (GD). Using a FDA-cleared TSH receptor (TSHR) bioassay for measurement of TSAbs, we hypothesized that TSAb levels are clinically useful and predictive in GD.
A total of 99 untreated hyperthyroid patients with GD (74 women) were treated with antithyroid drugs (ATD) for 24 weeks. Serum TSAb levels were measured at baseline, at 4, 8, 12, 24, and 36 weeks after starting ATD with a chimeric TSHR bioassay. Response vs. nonresponse to treatment was defined as biochemical euthyroidism at weeks 24 and 36 vs. persistent hyperthyroidism at week 24 and/or relapse at week 36.
In this prospective trial, 74 hyperthyroid patients with GD (57 women, median age 43 years, range 18–74 years, 43 with orbitopathy, GO) have completed the 24-week ATD treatment (methimazole monotherapy 2.5–30 mg/day), and the subsequent 12-week follow-up. Thirty-two out of 74 (43%) responded to ATD treatment of whom 16/32 (50%) had GO. In contrast, 42/74 (57%) were nonresponders, 27/42 (64%) with GO. Already 12 weeks after starting therapy, marked differences of ATD dose (p<0.001) and serum TSAb levels (p=0.007) were noted between responders vs. nonresponders. At week 24 and compared to baseline, serum TSAb levels decreased markedly in responders (median SRR% 410 vs. 301, Δ 27%, p<0.001), but increased in nonresponders (413 vs. 464, Δ 12%, p=0.134). In contrast, serum levels of TSHR-binding inhibiting immunoglobulins (TBII, automated ECLIA assay) decreased in nonresponders at week 24 (15.1 vs. 10.2 IU/L, Δ 33%, p=0.016). TSAb and TBII serum levels closely correlated (r=0.61, p<0.001). Thyroid volume was increased in male nonresponders (p=0.022).
Response to ATD is accompanied with significant decrease in TSAb levels, which remain unchanged or increase in nonresponders, most of whom have systemic GD.
DIVERSE CLINICAL FEATURES OF PATIENTS WITH HYPOTHYROID EPISODES AND THYROID STIMULATION-BLOCKING ANTIBODIES (TSBAB)
Autoimmunity Saturday Poster Clinical
TSH receptor antibodies consist of thyroid-stimulating antibodies (TSAb) and thyroid stimulation-blocking antibodies (TSBAb). In Graves' thyrotoxicosis, TSAb are predominant, whereas the predominance of TSBAb results in hypothyroidism. We retrospectively investigated the clinical features of patients with autoimmune thyroid diseases who experienced episodes of hypothyroidism with positive TSBAb.
Thirty-one patients were enrolled in the study. The initial diagnosis was Graves' disease in 12 patients, hypothyroidism in 15 patients, euthyroid Hashimoto thyroiditis in 3 patients, and type 2 amiodarone-induced thyrotoxicosis (AIT 2) in one patient. Twenty-five patients were women and 6 patients were men. Thyroid function after the detection of TSBAb was investigated in all patients.
In all of the patients who were initially diagnosed with hypothyroidism and 2 hypothyroid patients after remission of Graves' disease, hypothyroidism continued except for one patient whose hypothyroidism was transient and another patient whose condition changed to hyperthyroidism. On the other hand, thyroid function varied in the patients with Graves' disease. Hypothyroidism continued in 5 patients, including 2 patients after radioiodine therapy. In 2 other patients, hypothyroidism was transient. Thyroid function fluctuated between hypothyroid and hyperthyroid in 4 patients. In one female patient with a history of thyroidectomy, transient hypothyroidism occurred several times and thyroid function became hyperthyroid state during pregnancy. Another patient needed thyroxine replacement during pregnancy. In an AIT 2 patient, TSBAb were detected during the hypothyroid phase of destructive thyroiditis. TSBAb are usually detected in patients who are positive for TRAb (TBII). In the present cohort, TRAb were not detected in 6 patients. Among them, 2 female patients with low titers of TSBAb experienced neonatal transient hypothyroidism.
Hypothyroidism continued in the hypothyroid patient with TSBAb, with the rare exception of transient hypothyroidism and conversion to hyperthyroidism. In the Graves' patients with hypothyroid episodes concomitant with TSBAb, the clinical course was diverse.
Endocrinology, Metabolism, Diabetes, & Nutrition, Mayo Clinic, Rochester, MN
Autoimmunity Saturday Poster Clinical
The choice of therapy for Graves' disease requires careful discussion between patient- and physician-concerning risks, benefits, logistics, and effectiveness of the various treatment options, as well as patient values and preferences. However, an objective meta-analysis comparing the effectiveness of the three treatment options for use in this discussion is not available. In addition, wide geographical variations in the selected treatment option exist. The aim of the study was to determine the relapse rate of treatment options for Graves' disease.
A comprehensive search of relevant databases from each database's earliest inclusive dates to March 2012 (humans, any language) was conducted. Eligible studies were randomized clinical trials and comparative cohort studies, including two or more treatment arms [antithyroid drugs—ATDs (methimazole/carbimazole and propylthiouracil), radioactive iodine (RAI), and thyroidectomy] in the management of Graves' disease. Two reviewers worked independently and in duplicate to determine study eligibility, extract qualitative and quantitative data, and assess study quality.
We performed a network meta-analysis of eight studies, which included one randomized trial and seven cohort studies of 1402 patients from six countries: the United States (1), Chile (1), Ethiopia (1), Ireland (2), Sweden (2), and Turkey (1). Mean follow-up duration in months was as follows: ATDs: 57, RAI: 64, and surgery: 59. Studies were at moderate-high risk of bias. The comparison between treatment options revealed more relapse rate with ATDs than RAI [odds ratio (OR)=6.25; 95% confidence interval (95% CI), 2.40–16.67]; and ATDs than surgery [OR=9.09; 95% CI, 4.65–19.23]. There was no significant difference between RAI and surgery. The estimate for incoherence was small (ω=0.000), suggesting consistency of this network.
High-quality evidence quantitating and comparing the relapse rates of the various treatment options is unavailable. However, the objective information gained from this meta-analysis can be included in discussions between physician and patient concerning the choice of therapy for Graves' disease.
Endcrinology, Diabetes, Metabolism, and Nutrition, Mayo Clinic, Rochester, MN
Autoimmunity Saturday Poster Clinical
The optimum therapy for Graves' disease (GD) is chosen after discussion between physician and patient regarding benefits, drawbacks, potential side effects, and logistics of the various treatment options and takes into account patient values and preferences. This cohort study aimed to provide useful information for this discussion regarding the usage, efficacy, and adverse-effect profile of radioactive iodine (RAI), antithyroid drugs (ATDs), and thyroidectomy in a tertiary care facility.
Our cohort included nongravid adults diagnosed with Graves' hyperthyroidism from January 1, 2002, to December 31, 2008, who had complete follow-up after treatment at the Mayo Clinic, Minnesota. Data on different treatment modalities, their relapse rates, and adverse effects were extracted manually and electronically from the electronic medical records. The association of treatments with relapse-free survival was evaluated by Kaplan–Meier analyses.
Our cohort of 723 subjects had a mean age of 49.2, mean follow-up of 3.4 years, 76.6% women, and 17.2% smokers. The initial therapy was RAI in 75.3%, ATDs in 16.4%, and thyroidectomy in 2.75% and 5.5% were observed. The relapse rate at 3 years was 47% for ATDs and 8.3% for RAI (HR: 9.5, CI: 6.5–14.3). Surgery had a 100% remission rate; 65% of observed patients ultimately required therapy. Adverse effects developed in 35 of the 119 patients treated with ATDs, which included urticaria (1.7%), rash (4.2%), pruritis (1.7%), neutropenia (2.5%), elevated liver enzymes/cholestasis (4.2%), arthralgia (<1%), antithyroid arthritis syndrome (<1%), nausea/gastric distress(5%), dysgeusia (8.4%), headache (<1%), dizziness (<1%), for RAI radiation thyroiditis (1.5%), and (for thyroidectomy) hematoma (10%) and superior laryngeal nerve damage (5%).
RAI was the most commonly used modality within our cohort and demonstrated a good efficacy and safety profile. Surgery was also very effective and relatively safe in the hands of experienced surgeons. While ATDs allow preservation of thyroid function, a high relapse rate combined with a significant adverse effect profile was documented. These data can inform discussion between physician and patient regarding the choice of therapy for GD.
A CASE OF HYPERTHYROIDISM ASSOCIATED WITH A SKIN RASH
Autoimmunity Saturday Poster Clinical
Autoimmune thyroid disease is associated with various skin manifestations. Only few cases have been published showing an association of eczema and autoimmune thyroid disease. A case of Hashimoto's thyroiditis leading to hyperthyroidism associated with a skin rash secondary to eczema is described.
Clinical Case: A 52-year-old woman presented to our clinic for evaluation of thyroid gland. She complained of heat intolerance, palpitations, 16-lb weight loss, and an itchy and painful rash. The rash developed 1.5 years ago on her legs, feet, elbows, and abdomen. She had pulse of 84 bpm and blood pressure of 166/93. Physical examination showed mildly anxious woman with warm and moist palms of the hands and fine tremors of the fingers. She had mild thyromegaly without any tenderness or bruit. Skin examination showed an erythematous rash on pretibial regions, dorsum of the feet and elbows bilaterally, and on abdomen. Medical history included a toxic multinodular goiter that was diagnosed 4 years ago without any further management. Family history included a sister with thyroid cancer. Laboratory work- up showed TSH<0.015 mIU/mL (normal, 0.45–4.70 mIU/mL), free T4 2.48 ng/dL (normal, 0.89–1.76 ng/dL), and total T3 256 ng/dL (normal, 60–181 ng/dL). Differential diagnosis at that time included Graves' disease and toxic multinodular goiter in addition to thyroiditis, so the patient was started on methimazole. Thyroid receptor antibodies and thyroid-stimulating antibodies were negative. Anti-TPO antibodies were markedly elevated at 2660 units (normal, 0–100). The patient was diagnosed with Hashimoto's thyroiditis. Skin biopsy showed perivascular lymphocytic infiltrate with excoriation and mild spongiosis consistent with eczema.
N/A
This case describes an association of Hashimoto's thyroiditis with eczema. Only few cases of autoimmune thyroid disease associated with eczema are described in the literature. Possible explanation of this association is autoimmune disease. Careful skin examination should therefore be performed in patients presenting with autoimmune thyroid disease, and the possibility of autoimmune thyroid disease should be kept in mind in cases of resistant eczema.

Pretibial rash in a patient with Hashimoto's thyroiditis.
Disorders of Thyroid Function Saturday Poster Basic
Thyroid hormones exert a crucial role on trophic events of the central nervous system and during adulthood is primary related with neurogenesis and excitability. Particularly, the hippocampal formation is a highly susceptible region to thyroid hormone deficiency. Adult-onset hypothyroidism induces neuronal damage on pyramidal cells in the CA3 region, accompanied by increases in the p53, p21, and Bax/Bcl-2 ratio, indicating cell cycle arrest and apoptotic induction. These cell alterations were prevented when the NMDA receptor antagonist MK-801 is coadministrated with the antithyroid drug methimazole (MMI). The aim of the present study was to evaluate whether MK-801 neuroprotection effect is mediated by modulating cell cycle and/or apoptotic pathways.
Male Wistar rats were assigned to one of four groups: 1) control group drank tap water; 2) hypothyroid group (Hyp) drinking water with MMI (60 mg/kg/day); 3) Hyp+MK-801 group, which received antithyroid treatment plus MK-801 (0.5 mg/kg/day, ip); and 4) which only received MK-801. After four weeks of treatment, rats were decapitated, and the hippocampus was dissected to determine the expression of cell cycle and apoptosis markers by Western blot.
Our results showed that p53 and Bax/Bcl-2 index increase secondary to hypothyroidism is prevented by MK-801, but the p21 rise is not modified.
Our results suggest that NMDA receptor activity is necessary to trigger apoptosis pathways, but not cell cycle alterations induced by hypothyroidism. This work was supported by SIP-IPN 20120880. J. P.-R. is a fellow of DEDICT-COFAA-IPN.
Dept. of Physics and Astronomy, University of Utah, Salt Lake City, UT
Disorders of Thyroid Function Saturday Poster Translational
Point-of-care TSH immunochromatographic assays (TSH assays) are widely used to screen for hypothyroidism, but their acceptability is limited by the semiquantitative nature of the test format and inability to detect low TSH values. TSH assays generate a visual signal by labeling TSH antibodies with colloidal gold nanoparticles. These particles have a diameter between 70 and 100 nanometers, and a plasmon surface reflectance peak centered around 600 nanometers. Smartphones are equipped with an LED flash and digital camera, which operate in the visible spectrum and thus can illuminate and detect colloidal gold. Smartphones are also able to perform image analysis using an imaging application (app). We have developed a device that uses a smart phone's flash, camera, and computation features to quantify point-of-care TSH assays.
TSH assays (True Diagnostics TSH, Carlsbad, Ca.) consisted of a blood filtration element, colloidal gold-labeled mobile-phase anti-TSH β-subunit antibodies, and nitrocellulose membranes to which anti-TSH α-subunit captures antibodies (test-line antibodies), and antibodies that bind the mobile-phase anti-TSH β-subunit antibodies (control antibodies) were linked. Assays used a 30-microliter capillary blood sample and 100 microliters phosphate-buffered saline to solubilize gold-labeled anti-TSH β-subunit antibodies, mix the serum obtained from the blood sample with the mobile-phase antibody, and carry the serum antibody mixture the length of the membrane. Each TSH assay incorporated two control antibody concentrations for a two-point calibration. Using a light pipe and collimating lens to optimize illumination and focusing, a smartphone (Apple iPhone 4; Cupertino, Ca.) collected an image of a completed TSH assay (see Figure). The smart phone app converted the image into a quantitative TSH value using each test calibrators.
This smartphone-based imaging device was able to detect whole-blood TSH concentrations as low as 0.1 mIU/L.
An inexpensive optical device, smart phone, and image analysis app can quantify a immunochromatographic TSH assay with sufficient sensitivity and precision to diagnose hyper- and hypothyroidism and monitor thyroxine therapy at the point of care.
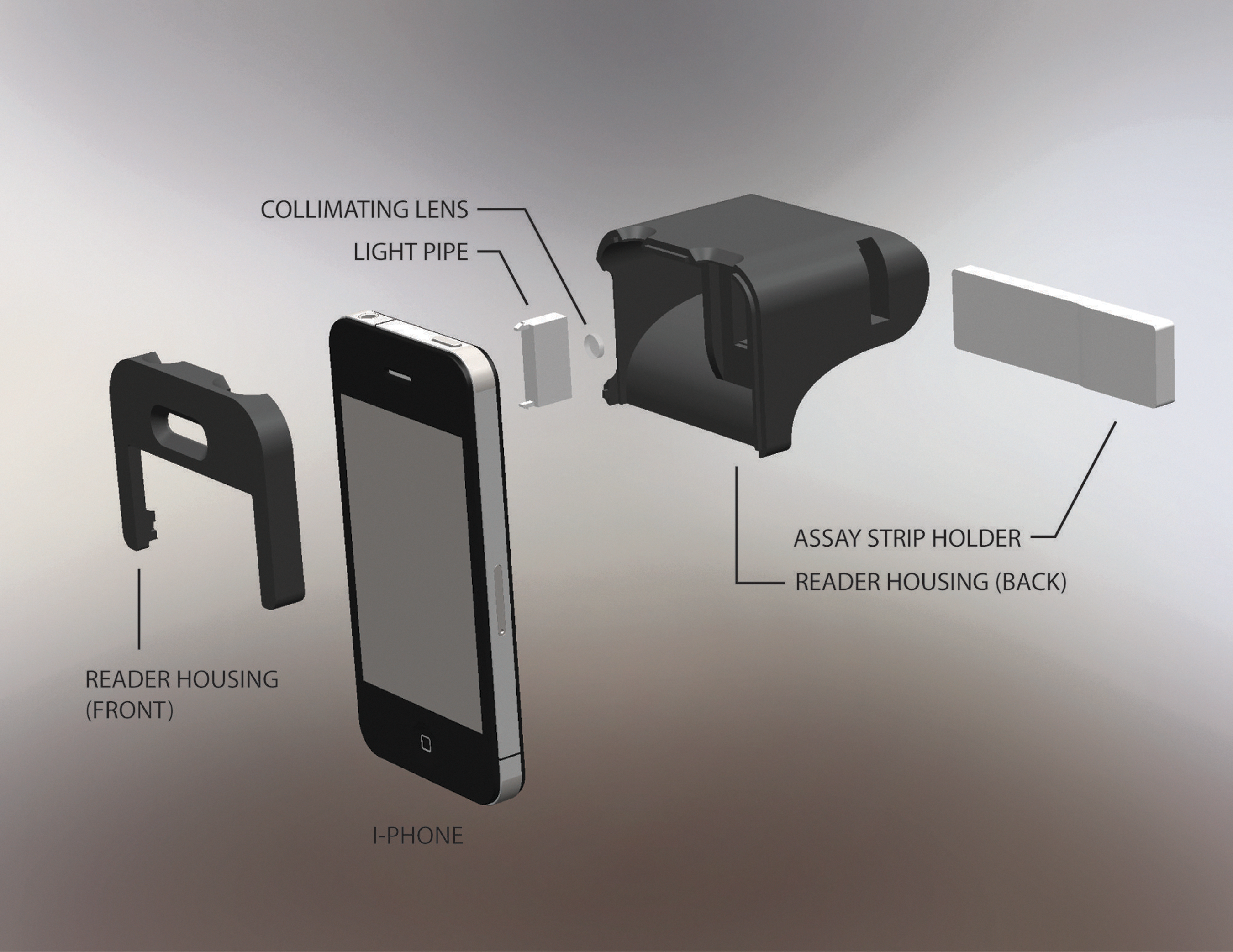
Smartphone TSH Measurement Device.
Disorders of Thyroid Function Saturday Poster Clinical
Resistance to thyroid hormone (RTH) is a disorder associated with decreased end-organ responsiveness to thyroid hormone. Typically, patients with RTH have increased levels of thyroxine (T4) and triiodothyronine (T3) with a normal or increased serum level of thyroid-stimulating hormone (TSH). Clinical features of this disorder are variable, and no guidelines about treatment are available. We report a novel mutation in the thyroid hormone receptor β (TRβ) gene that causes RTH.
We analyzed the clinical presentations and changes in thyroid function tests (TFTs), including magnetic resonance imaging (MRI) of the pituitary gland and results of other laboratory tests. We performed direct DNA sequencing of the TRβ gene.
A 44-year-old Japanese man had goiter, palpitation, and poor concentration. His TFTs showed high levels of circulating free thyroid hormones (T3 and T4) and normal TSH concentrations, which indicated inappropriate secretion of TSH. The patient was negative for thyroid antibodies, including thyroid peroxidase antibody, thyroglobulin antibody, and TSH receptor antibody. MRI of the pituitary gland revealed no pituitary tumor. Thyrotropin-releasing hormone test showed normal levels of TSH and prolactin. The concentration of the α-subunit of the pituitary glycoprotein hormone was in the normal range. Thus, on the basis of clinical results, we concluded that the patient had RTH, and direct sequence analysis showed that a mutation of the TRβ gene caused replacement of a tyrosine (Y) with cytosine (C) at codon 321 (Y321C). BLAST search using the NCBI database of humans and recent studies confirmed that the sequence variant, Y321C, was a de novo mutation in exon 9 of the TRβ gene.
Our patient showed features consistent with those of RTH. A novel mutation, Y321C, was found in exon 9 of TRβ of our patient.
THE PATTERN OF TEMPORAL CHANGES IN SERUM FREE-THYROXINE LEVELS AFTER RADIOACTIVE IODINE THERAPY AND THE FACTORS INFLUENCING THE THERAPEUTIC RESPONSE TO RADIOACTIVE IODINE THERAPY IN HYPERTHYROIDISM IN A GROUP OF CHINESE PATIENTS
Disorders of Thyroid Function Saturday Poster Clinical
Radioactive iodine therapy (RAI) is a common modality of treatment for hyperthyroidism. To definite the temporal course of change in serum free-T4 (fT4) level, we prospectively monitored clinical and biochemical features in 56 thyrotoxic patients who received RAI for the first time between 1st July 2009 to 31st March 2010.
After RAI, clinical follow-ups were arranged at week 4, 8, and 12, and then 3 monthly up to the 12th month. fT4 was monitored before RAI and at week 1, 2, 3, 4, 5, 10, 14, 18, 24, 36, and 48 after RAI. A successful outcome was defined as achievement of hypo- or euthyroidism at week 24 and week 48. The relationship of baseline clinical parameters and outcome was studied by Spearman's rank-order correlation. Multivariate analysis was performed using logistic regression. The degree of fluctuation in fT4 within different time periods was assessed by analysis of variance (ANOVA).
A successful outcome was obtained in 67.9% and 69.2% of patients at week 24 and week 48, respectively. Factors associated with successful outcome were female sex (p=0.028) and shorter duration of antithyroid drug used before RAI (p=0.054). fT4 in week 4 to week 12 showed a good positive predictive value to the outcomes. Mean fT4 dropped from baseline (25.06±11.4 pmol/L) to a nadir at around week 4 by 23% (19.24±9.06 pmol/L) and rose to a peak at around week 10. The degree of fluctuation in fT4 within a time interval at different periods after RAI, as reflected by the coefficient of variation (CV), is shown in the Table. The highest CV occurred between week 6 to week 12, suggesting that fluctuation in fT4 level was greatest within this time frame.
Two-thirds of patients could achieve a long-standing remission with RAI. A successful outcome was difficult to be predicted form basic clinical variables. Wide fluctuations in fT4 levels occurred after RAI, and close monitoring, especially between 6 to 12 weeks, is warranted.
Coefficient of Variation (CV) of Serum fT4, at 2 Weekly Intervals, at Different Periods After RAI
Disorders of Thyroid Function Saturday Poster Clinical
Congenital hypothyroidism (CH) is an important cause of mental retardation, which can be avoidable by neonatal screening. To date the optimal cutoff level of bloodspot TSH (TSHneo) used in neonatal screening programs for CH remains controversial. While some programs use values of 5 mIU/L, others adopt cutoffs of 20–25 mIU/L. Objective: To evaluate the potential diagnosis impact of different TSHneo cutoffs for the detection of CH in children born in 1997–2008 in Sao Paulo State-Brazil.
All infants with a TSHneo value≥5 mIU/L (AutoDELFIA) were re-evaluated by a second sample of TSHneo. If confirmatory serum TSH≥10 mIU/L, 99mTc thyroid scintigraphy was performed, and treatment with thyroxine was started. After 3 years of age, children with topic thyroid were reevaluated with 131I thyroid scintigraphy and TRH test after withdraw thyroxine for 4–6 weeks. ROC curves were constructed using different cutoffs of TSHneo (5, 6, 7, 8, and 9 mIU/L).
Between 1997 and 2008, 275,665 newborns were screened. Seventy-one presented confirmatory TSH≥5 mIU/L. After reevaluation, 6 (8.5%) had the diagnosis of definitive CH confirmed; 13 patient (18%) had basal TSH between 5 and 10 mIU/L and exaggerated response to TRH (TSH peak≥35 mIU/L); 35 (49%) normalized thyroid function; 7 newborns died, and 8 children lost follow-up. Two patients (3%) remained with basal serum TSH between 5 and 10 mIU/L and had normal response to TRH test (hyperthyrotropinemia). Considering the cutoffs of 5, 6, 7, 8, and 9 mIU/L, the recall rate and the number of children with confirmed diagnosis of CH would be 0.9% and 19; 0.4% and 13; 0.2% and 9; 0.09% and 6; and 0.04% and 5, respectively.
The cutoff of 6 mIU/L had the better sensitivity (73%) and specificity (68%) values for TSHneo in detecting all cases of CH. However, the lack of information on the potential improvement of the neurological outcome generated by the early treatment of children with mild dysfunction and the additional costs does not allow the adoption of this cutoff at this moment.
Department of Internal Medicine, Division of Endocrinology and Metabolism, Medical School of Ribeirão Preto, University of São Paulo, Ribeirão Preto, Brazil
Thyroid Cancer Saturday Poster Clinical
Human leukocyte antigen G (HLA-G) is a nonclassical major histocompatibility complex molecule with multiple immunomodulatory properties. Several studies have demonstrated the involvement of HLA-G in tumorogenesis by promoting immunosuppression in tumor microenvironment. Objectives: To verify the expression of HLA-G in normal thyroid tissue, goiter, benign, and malignant thyroid gland neoplasms. To evaluate the different expression among groups and its association with clinical parameters.
Immunohistochemistry for HLA-G was performed on 72 papillary carcinomas (PTC), 19 follicular carcinomas (FTC), 8 medullar carcinomas (MTC), 22 follicular adenomas (FA), 22 goiters (G), and 14 normal thyroids (N). The percentage of cell staining was documented, and the staining intensity was graded as 0, 1+, 2+, and 3+. Clinical data were obtained through medical records. Statistical analysis was performed, using mean±standard deviation (SD) and median, Chi-square test, and Mann–Whitney test.
The staining intensity classified as 0, 1+, 2+, and 3+ were, respectively, PTC=0%, 44,4%, 40,3%, and 15,3%; FTC=0%, 53%, 47%, and 0%; MTC=0%, 75%, 25%, and 0%; FA=0%, 64%, 27%, and 9%; G=62,8%, 27,3%, 4,5%, and 0%; n=86%, 14%, 0%, and 0%. The mean±SD (median) of the percentage of cell staining were PTC=69,3±23,1%(75%); FTC=83,7±24,5%(90%); MTC=78,7±26,9%(90%); FA=62,73±26%(70%); G=6,1±11,9%(0%); n=3,9±10%(0%). In PTC, FTC, MTC, and FA, the staining intensity and the percentage of cell staining were significantly higher than in normal thyroid tissue (p<0.001). The tumor area with HLA-G expression was greater in FTC compared to FA (p=0.002). We found an association between clinical parameters and the intensity of expression of HLA-G in the PTC group (age, histological subtype, and recurrence rate).
This study demonstrated for the first time the expression of HLA-G in thyroid neoplasm, with slight expression in hyperplasic areas of goiter and normal tissue. The percentage of cell staining in FTC was higher than in FA. It was found an association between some prognostic factors and gene expression in PTC. The present study suggests that the role of HLA-G in oncogenesis should be further investigated, since it can be a potential tumor marker.
FOUR (4) CASES OF FETAL HYPERTHYROIDISM IN EUTHYROID WOMEN WITH HISTORY OF SURGERY FOR GRAVES' DISEASE: GESTATIONAL TIME-SPECIFIC FETAL HEART RATE (FHR) USEFUL FOR MONITORING FETAL THYROID STATUS DURING TREATMENT
Disorders of Thyroid Function Saturday Poster Clinical
Pregnant women in remission status after ablative therapy for Graves' disease occasionally have high levels of TRAb, which may lead to fetal hyperthyroidism (FH). In this setting, maternal free-T4 levels are ineffective as an indicator of fetal thyroid status. Sampling of fetal blood by cordocentesis is discouraged, since it may lead to serious complications. Fetal bone maturation or goiter determined by ultrasound would be an useful indicator. However, it requires technical experience. FHR is considered a less-accurate indicator of fetal thyroid status. Although FHR decreases as pregnancy progresses, it has been evaluated without allowance for gestational time in previous studies. We report four cases of FH effectively treated by monitoring FHR. FHR was evaluated taking gestational weeks into account.
FH was highly suspected in 4 cases on the bases of fairly high TBII (66–90%; normal<10%) and TSAb (1930–4076%; normal<180%) values and high FHR. Iodine administration to mothers was initiated between 20–27 weeks of gestation. Thionamides were added when FHR did not sufficiently decrease or increased after a transient fall. FHR was evaluated taking into account the gestational-related range.
The babies were born in 34–38 weeks of gestation. FT4 and TSH concentrations at birth determined by using cord blood were 0.9–2.0 ng/dL (normal 0.9–1.7 ng/dL) and <0.05–9.7 μU/mL (normal 2.9–12.4 μU/mL), respectively. The development of FH at the initiation of therapy was confirmed by the occurrence of hyperthyroidism after birth in all four cases.
Measurement of FHR may represent a practical and reliable tool for determining fetal thyroid status during the treatment of FH developed in euthyroid pregnant women with a history of ablative therapy for Graves' disease. Taking gestational weeks into account is essential in the evaluation of FH. Further studies are necessary to confirm these findings.
Pediatrics, Pontificia Universidad Catolica de Chile, Santiago, Chile
Disorders of Thyroid Function Saturday Poster Clinical
Graves' disease (GD) is rare in children, being diagnosed more frequently in adolescents. It has been suggested that the clinical presentation in prepubertal children would be more severe than the pubertal with regard to the presenting symptomatology. Our objective was to determine whether differences exist in the presentation of Graves' disease between these two age groups.
The diagnosis of GD in 27 prepubertal children (median, Q1–Q3) (7; 5.7–9.3) was compared with that in 31 pubertal patients (12.7; 10.9–14). The medical records of the patients (46 girls) diagnosed between years 1992 and 2011 at Pontificia Universidad Católica de Chile were retrospectively investigated.
At diagnosis, 46.5% of patients were prepubertal with ages between 2.9 and 17.1 years (10.35 years; 6.92–13 years; p<0.0001), female-to-male ratio 4/1. Height-SDS (median, Q1– Q3) [(0.67;−0.52–1.86) vs. (0.32;−0.12–0.87); p=NS] and BMI-SDS [(0.18;−0.97–0.75) vs. (0.18;−0.82–0.62; p=NS] did not differ between prepubertal and pubertal. The most common clinical presentations between both groups were diffuse goiter (96.3 vs. 96.6%; p=NS), hyperactivity (63 vs. 41.9%; p=NS), frequent bowel movements (48.1 vs. 51.6%; p=NS), sleep disturbances (44.4 vs. 54.6%; p=NS), and palpitations (37 vs. 48.4%; p=NS). The most frequent ocular manifestation were exophthalmus (48.1 vs. 58.1%; p=NS) and eyelid retraction (14.8 vs. 16.1; p=NS). Values of TSH (μIU/mL) [(0.01; 0.01–0.03) vs. (0.01; 0.01–0.02); p=NS], free T4 (ng/dL) [(2.44; 1.61–5.43) vs. (3.42; 2.18–6.35); p=NS], and T3 (ng/dL) [(401.9; 258.5–644.8) vs. (410; 223–572); p=NS].
We did not find any differences at presentation of GD among prepubertal and pubertal patients. Neuropsychiatric symptoms such as hyperactivity and sleep disturbances, together with exophthalmus, are common features in children with GD.
Endocrinology, Amrita Institute of Medical Sciences, Cochin, India
Disorders of Thyroid Function Saturday Poster Clinical
Hypothyroidism is generally believed to be as common in India, as it is worldwide. However, there is a paucity of data on the prevalence of hypothyroidism in India.
An epidemiological, cross-sectional, multicenter study was conducted in eight major cities (Bangalore, Chennai, Delhi, Goa, Mumbai, Hyderabad, Ahmedabad, and Kolkata) of India to study the prevalence of hypothyroidism among adult population, through 94 general health camps organized over five months. Thyroid abnormalities were diagnosed on the basis of laboratory results (serum free-T3, free-T4, and thyroid-stimulating hormone [TSH]). Subjects with history of hypothyroidism and on levothyroxine therapy and those with serum free-T4 level <0.89 ng/dL and TSH>5.50μIU/mL were categorized as hypothyroid. The prevalence of self-reported and undetected hypothyroidism and antithyroid peroxidase (anti-TPO) antibodies was also assessed in the study population.
A total of 5376 adult male or female patients aged more than 18 years (mean age 46 years, equally distributed in both gender groups) were enrolled in the study, of which the data of 5360 patients were analyzed. The overall prevalence of hypothyroidism was 10.95% (n=587) of which 7.48% (n=401) patients self-reported the condition, whereas hypothyroidism was undetected in 3.47% (n=186) patients. Additionally, 8.02% (n=430) patients were found to have subclinical hypothyroidism (normal serum free-T4 and TSH>5.50μIU/mL). Anti-TPO antibodies for autoimmunity were detected in 21.85% (n=1171) patients.
The prevalence of hypothyroidism, including self-reported hypothyroidism, was high in the overall study population (approximately 1 in 10). The prevalence of subclinical hypothyroidism was also substantial (8%) in the overall population, indicating the extent of this problem. Twenty-one percent of the study population showed anti-TPO antibodies, suggesting that thyroid autoimmunity is common.
THE STUDY OF APUD SYSTEM IN PATIENTS WITH HYPOTHYROIDISM OF DIFFERENT AGES
Disorders of Thyroid Function Saturday Poster Clinical
The aim of the study was to examine the content of the gastric mucosa of gastrointestinal hormones in patients with hypothyroidism.
We investigated 37 patient gastrobiopsy hypothyroidism from 23 to 65 years. The diagnosis of hypothyroidism was confirmed by measurement of thyroid hormones and thyroid-stimulating hormone (TSH) in serum. Immunohistochemistry in gastrobiopsies of the antrum of patients studied gastrin, serotonin, and melatonin. The primary antibodies used commercial antibodies to serotonin, gastrin, and melatonin (Dako, Glostrup, Denmark; titer 1:50). Measurements were carried out in five fields of view (with an increase in lens 40) in three slices of the examined organ.
As a result of it was found that in patients in whom no biopsy serotonin and melatonin in the blood TSH level was 19.9±3.8 mIU/L, the level of free T4 7.8±2.4 pmol/L, total T4 46±3.8 ng/mL. In the group of patients whose biopsy visually determined serotonin in the blood TSH level was 14.38±2.4 mIU/L, the level of free T4 8.1±2.3 pmol/L, and total T4 47±4.9 ng/mL. Only in biopsies of patients with hypothyroidism were detected all young APUD hormones: gastrin-secreting cells (G-cells) 5.6±3.7%, serotonin-secreting cells (EC-cells) 3.7±1.3%, and the melatonin-producing cells 1.3±0.6%. In adulthood and old age, there is a mosaic of APUD cells.
Thus, the results indicate a possible violation of local gastrointestinal hormonal regulation in patients with hypothyroidism middle-aged and elderly.
STUDY OF LEVELS ERYTHROPOIETIN AND PROINFLAMMATORY CYTOKINES IN PATIENTS WITH HYPOTHYROIDISM BLOOD WITH ANEMIA
Disorders of Thyroid Function Saturday Poster Clinical
The aim of the study was to examine the levels of proinflammatory cytokines and erythropoietin in hypothyroidism with anemic syndrome.
We have examined 50 patients with hypothyroidism with iron-deficiency anemia normochromic and hypochromic in age from 17 to 62 years. Among them were 36 women and 14 men. Examination included the definition in the blood levels of thyroid hormones, serum iron, erythropoietin, ferritin, and total blood by standard methods.
The study revealed that 72% of patients with hypothyroidism with anemia HB blood level was below 90 g/L, and in 28% of patients with Hb levels of the blood was below 70 g/L. The level of erythropoietin in the blood plasma in 73% of the patients was below 5 ng/mL. In 40% of the patients, revealed serum ferritin levels were below 20 ng/mL, which proves depletion of iron levels. In the study of interleukins, blood of patients with hypothyroidism showed an increase in proinflammatory cytokines IFN-γ up to 7.15±2.3 pg/mL and IL 1β 11.4±5.2 pg/mL, indicating a possible suppression of the level of erythropoietin interleukins. In the analysis of thyroid function in patients with hypothyroidism with anemia it was found that the level of thyroid-stimulating hormone was within 23.7±2.8 mIU/mL, free T4 7.9±1.3 pg/mL, antibodies to thyroid peroxidase 527.5±62.7 IU/mL.
Thus, in hypothyroidism with anemia, a change of proinflammatory cytokines and decreased levels of erythropoietin and ferritin levels.
CORRELATION OF TSH VALUES IN CHEMICALLY EUTHYROID PEDIATRIC HYPOTHYROID PATIENTS WITH BMI PERCENTILES ADJUSTED FOR GENDER AND AGE
Disorders of Thyroid Function Saturday Poster Clinical
The objective of this study was to determine if there is a significant correlation of TSH values in chemically euthyroid pediatric hypothyroid patients with BMI percentiles.
Retrospective chart review of 71 hypothyroid pediatric patients ages 7 months–19 years who were seen in the pediatric endocrinology clinic at the Loyola University Medical Center in 2011. Inclusion criteria were a TSH within the normal range (0.5–4.3 mU/L) and being on replacement treatment with levothyroxine for more than 6 months. Exclusion criteria were the presence of other endocrinopathies. TSH and free-T4 values were divided into quartiles and compared with BMI percentiles normalized for gender and age.
There was no correlation between BMI percentile (classified as normal weight <85th percentile, overweight 85th–95th percentile, or obese >95th percentile) and TSH quartile (p-value 0.456). Correlation was also not present when looking at TSH values divided into thirds or halves, or when comparing subgroups of patients based on gender, age, ethnicity, or type of hypothyroidism. There was also no correlation between BMI percentile and free-T4 values divided into quartiles. Secondary findings showed a trend for children over age 11 to be more likely to have lower TSH values (p-value 0.051) and females to have lower TSH values (p-value 0.12); however, neither was significant, and neither group showed a correlation to BMI percentile.
In pediatric hypothyroid patients on replacement with levothyroxine that are chemically euthyroid, there is no correlation with BMI percentiles and TSH values. Further adjustments of levothyroxine dose to lower TSH within the normal range do not provide additional benefit in terms of weight control.
Pulmonary Medicine, VA Medical Center, Omaha, NE
Disorders of Thyroid Function Saturday Poster Clinical
Obstructive sleep apnea (OSA) and hypothyroidism share many features, including obesity, fatigue, decreased libido, depressed mood, impaired concentration, and snoring. Periorbital and peripheral edema are usually associated with hypothyroidism, but are also seen in OSA. Given this clinical overlap, TSH screening is a prerequisite before polysomnography (PSG) in some centers. However, economic justification of this biochemical screening is not established. This study aimed to (1) describe the prevalence of diagnosed hypothyroidism and (2) assess the prevalence of undiagnosed hypothyroidism in patients with OSA confirmed by PSG.
We retrospectively reviewed the records of all patients with PSG-confirmed OSA between October, 2010, and September, 2011. Abstracted data included age, gender, body–mass index (BMI), respiratory disturbance index (RDI), apnea–hypopnea index (AHI), TSH levels in the two years preceding PSG, pre-existing diagnosis of hypothyroidism, and patients with newly diagnosed hypothyroidism (based on TSH value at the time of PSG).
Four hundred eighteen patients were diagnosed with OSA during the study period. Average age was 58 years (range 22–90), and 394 (94.3%) were men. Mean BMI was 34.5 kg/m2 (range 18.4–68.8). Mean RDI and AHI values were 45.9 (range 1.6–180.) and 31.2 (range 0–149.4), respectively. TSH levels were done within two years of PSG in 385 patients (92.1%). While 48 patients (11.5%) had diagnosed hypothyroidism and were on thyroxine before PSG, only 2 patients (0.5%) were diagnosed with hypothyroidism based on their TSH level at the time of PSG.
The absolute prevalence of hypothyroidism in this cohort of patients with PSG-confirmed OSA was 12.0%. This included 11.5% with pre-existing disease and 0.5% with incident disease based on the TSH done at the time of PSG. Accordingly, it would appear that routine screening for hypothyroidism as a prerequisite to PSG is not cost effective.
Medical School, SUNY Upstate Medical University, Syracuse, NY
Disorders of Thyroid Function Saturday Poster Clinical
The clinical presentation of recurrent hyperthyroidism after treatment for Graves' disease is reasonably assumed to appear as progressive hyperthyroidism with diminishing LT4 replacement requirements. We present two patients with well-established hypothyroidism following 131I ablation. Variable replacement needs led to the recognition of a functioning thyroid remnant while still hypothyroid on LT4 replacement.
Case 1: A 55-y.o. man, 108 kg, was euthyroid for 8 years following 131I treatment for Graves' disease, when he presented with a TSH of 11.7 and symptoms of hypothyroidism. Thyroid replacement needs never stabilized. A thyroid-bed ultrasound showed a normal-sized thyroid with normal Doppler blood flow. Following pretreatment with thyrotropin-alpha, he underwent repeat ablation with 30 mCi 131I. Case 2: A 29-year-old man, 81 kg, with Graves' disease became hypothyroid following treatment with 20.1 mCi 131I. His replacement needs never stabilized. Thirty-two months following initial treatment, a technetium scan while on LT4 showed a functioning remnant, and the residual gland was surgically removed.
The persistence of concurrent hypothyroidism obscures the presence of a functioning remnant. Presumably, the variability of T4 release by the remnant results in the inability to establish a clinically appropriate and stable replacement LT4 dose. A functioning remnant is also suggested by a relatively low, weight-based replacement dose.
In hypothyroid patients following 131I ablation for treatment of Graves' disease, variable LT4 replacement requirements may reflect the presence of a functioning thyroid remnant and the need for repeat ablation.
Serial Thyroid Studies and Replacement Doses
Iodine Uptake & Metabolism Saturday Poster Basic
Soy consumption is associated with thyroid disorders such as hypothyroidism, goiter, and autoimmune thyroid disease, as well as increased iodine requirement in certain cases. However, the antithyroid components in soy are yet to be identified, and the molecular mechanisms involved remain unclear. This study examined if soy isoflavones affect iodine uptake and expression of genes involved in the biosynthesis of thyroid hormones in the Fischer rat thyroid cell line (FRTL-5).
FRTL-5 cells were treated with Novasoy, a soy alcohol extract containing 30% isoflavones, or major isoflavone aglycones (genistein, daidzein, and glycitein) or glycosides (genistin, daidzin, and glycitin) for 24 hrs. Iodide uptake was measured by a colorimetric assay. The protein content of thyroglobulin (Tg), sodium/iodide symporter (NIS), and thyroid-stimulating hormone receptor (TSHR) was measured by Western blotting. Cytotoxicity of tested compounds was determined by the MTT cell proliferation assay.
Iodide uptake in FRTL-5 cells was dose-dependently suppressed by Novasoy (50, 100, or 200 μg/mL) added into the assay or to the cell culture (10, 25, or 50 μg/mL) (p<0.05). However, neither the major isoflavone aglycones nor glycosides alone or in combination had similar effects. Novasoy (up to 200 μg/mL) had no cytotoxic effect. Novasoy (1, 10, and 50 μg/mL) and genistein (1 and 10 μM) markedly increased the protein content of a 40-kDa Tg fragment (P40), a well-known autoimmunogen, nonglycosylated NIS, and TSHR in the FRTL-5 cells (p<0.05).
The alcohol soluble components other than the major isoflavones in soy remarkably inhibited iodide uptake in the FRTL-5 cells. Soy isoflavones, particularly genistein, induced the production of P40, an autoimmunogen, which might be responsible for the high incidence of autoimmune thyroid disease reported in the soy infant formula-fed children.
Department of Internal Medicine, University of Pisa, Pisa, Italy
Thyroid Cancer Saturday Poster Basic
We have studied the antitumor activity of the new pyrazolo[3,4-d]pyrimidine compound (CLM29) in primary medullary thyroid cancer (P-MTC) cells and in the TT cell line.
The antiproliferative and proapoptotic effects were tested in P-MTC cells obtained at surgery from patients, in TT cells harboring (C634W) RET mutation and in human dermal microvascular endothelial cells (HMVEC-d). The concentrations of CLM29 used in the in vitro experiments were 1, 5, 10, 30, and 50 μM.
CLM29 proved to inhibit in vitro tyrosine kinase activity of recombinant human RET, vascular endothelial growth factor receptor-2, and epidermal growth factor receptor. Proliferation assays in TT and P-MTC cells showed a significant reduction of proliferation by CLM29 (p<0.001, ANOVA). CLM29 increased the percentage of apoptotic cells both in TT and in P-MTC cells dose dependently (p<0.001, ANOVA), while had no effect on migration and invasion in both cell types. CLM29 determined a significant inhibition of HMVEC-d proliferation, blocking extracellular-signal-regulated kinases 1/2 phosphorylation, and induced, significantly, the apoptotic process in these cells. RET mutations were observed in 2 P-MTCs, the inhibition of proliferation by CLM29, obtained in P-MTC from tumors with RET mutation, were similar to those from tumors without. TT cells were injected s.c. in CD nu/nu mice, and tumor masses became detectable between 20 and 30 days after xenotransplantation. CLM29 (50 mg/kg/day) inhibited significantly tumor growth and weight, and the therapeutic effect was significant starting on the 48th day after cell implantation (18 days after the beginning of treatment). The CLM29-treated group of animals showed a slight, but not significant, weight loss if compared to the control one. A significant reduction of Ki-67 immunostaining and of microvessel density was observed in the CLM29-treated tumors.
The antitumor activity of a new pyrazolo[3,4-d]pyrimidine compound (CLM29) in vitro, and in vivo, in MTC, has been shown, opening the way to a future clinical evaluation.
Department of Internal Medicine, University of Pisa, Pisa, Italy
Autoimmunity Saturday Poster Translational
Chemokines are secreted under the influence of cytokines in thyrocytes, fibroblasts, preadipocytes, and myoblasts from orbital cells in Graves' ophthalmopathy (GO).
To our knowledge, we are the first to evaluate the effects of increasing concentrations of corticosteroids or rapamycin on the secretion of Th1 [chemokine (C-X-C motif) ligand 10 (CXCL10)] and Th2 [chemokine (C-C motif) ligand 2 (CCL2)] in primary cultures of thyrocytes, fibroblasts, preadipocytes, and myoblast obtained from the orbits of GO patients.
In primary cultures of thyrocytes, fibroblasts, preadipocytes, and myoblasts from GO patients, CXCL10 is undetectable in the supernatant. Interferon (IFN)-gamma dose dependently induced CXCL10 release, whereas tumor necrosis factor (TNF)-alpha alone had no effect, and their combination had a significant synergistic effect on CXCL10 secretion. GO thyrocytes, fibroblasts, preadipocytes, and myoblasts produced in basal-condition low amounts of CCL2. TNF-alpha dose dependently induced CCL2 release, whereas IFN-gamma alone had no effect. However, the combination of TNF-alpha and IFN-gamma had a significant synergistic effect on CCL2 secretion. Treatment of GO thyrocytes, fibroblasts, preadipocytes, and myoblasts with increasing concentrations of corticosteroids or rapamycin (in a pharmacological range), added at the time of IFN-gamma and TNF-alpha stimulation, dose dependently inhibited CXCL10 and CCL2 release.
Corticosteroids or rapamycin, in a pharmacological range, plays an inhibitory role both on Th1 (CXCL10) and Th2 (CCL2) chemokines, in thyrocytes and in GO orbital cells, suggesting that the therapeutic effect of these drugs could be exerted, at least in part, through this mechanism.
Department of Internal Medicine II, University Hospital of Munich, Munich, Germany
Thyroid Cancer Saturday Poster Basic
The tumor-homing property of mesenchymal stem cells (MSCs) has lead to their use as delivery vehicles for therapeutic genes. The application of the sodium–iodide symporter (NIS) as therapy gene allows noninvasive imaging of MSC biodistribution and functional transgene expression by 123I-scintigraphy or PET-imaging, as well as therapeutic application of 131I or 188Re. Based on the critical role of the chemokine RANTES/CCL5 secreted by MSCs in the course of tumor stroma recruitment and differentiation into cancer associated fibroblasts, the use of the RANTES/CCL5 promoter should allow tumor stroma-targeted expression of NIS after MSC-mediated delivery.
In the current study, we stably transfected human MSCs with NIS driven by the CCL5 promoter (RANTES-NIS-MSC). Human colon carcinoma cells LS174t were injected into the spleen of nude mice, which resulted in induction of multifocal liver metastases. We investigated distribution and recruitment of RANTES-NIS-MSCs in liver metastases by 123I-scintigraphy and 124I-PET imaging, ex vivo gamma counting, and immunofluorescence analysis after systemic tail-vein injections of RANTES-NIS-MSCs.
Five days after intrasplenic tumor cell injection, 5×105 RANTES-NIS-MSCs were injected via the tail vein three times in four-day intervals followed by radionuclide application 48h later. 123I-scintigraphy and 124I-PET imaging revealed active MSC recruitment and CCL5 promoter activation in the multifocal liver lesions in 70% of mice as shown by tumor-selective iodide accumulation. After i.v. injection of wild-type MSCs, no significant iodide accumulation in liver metastases was observed. Immunofluorescence analysis revealed strong accumulation of MSCs in liver metastases in contrast to the surrounding normal liver tissue and nontarget organs.
Taken together, our results convincingly demonstrate selective recruitment of NIS-expressing MSCs driven by the RANTES promoter into liver metastases of colon cancer, resulting in induction of tumor-specific iodide accumulation. This novel gene therapy approach opens the prospect of NIS-mediated radionuclide therapy of metastatic cancer after MSC-mediated gene delivery.
Department of Internal Medicine II, University Hospital of Munich, Munich, Germany
Thyroid Cancer Saturday Poster Basic
The tumor-homing property of mesenchymal stem cells (MSCs) has lead to their use as delivery vehicles for therapeutic genes. The application of the sodium-iodide symporter (NIS) as therapy gene allows noninvasive imaging of functional transgene expression by 123I-scintigraphy or PET-imaging, as well as therapeutic application of 131I or 188Re. Based on the critical role of the chemokine RANTES/CCL5 secreted by MSCs in the course of tumor stroma recruitment, use of the RANTES/CCL5 promoter should allow tumor stroma-targeted expression of NIS after MSC-mediated delivery.
In the current study, we stably transfected human MSCs with NIS driven by the CCL5 promoter (RANTES-NIS-MSC). Using a human hepatocellular cancer (HCC) xenograft mouse model (Huh7), we investigated distribution and tumor recruitment of RANTES-NIS-engineered MSCs after systemic injection by gamma camera imaging.
123I-scintigraphy revealed active MSC recruitment and CCL5 promoter activation in the tumor stroma of Huh7 xenografts (6.5% ID/g 123I, biological half-life: 3.7 h, tumor-absorbed dose: 44.3 mGy/MBq). In comparison, 7% ID/g 188Re was accumulated in tumors with a biological half-life of 4.1 h (tumor-absorbed dose: 128.7 mGy/MBq). Immunofluorescence analysis and measurement of ex vivo 123I biodistribution verified active recruitment of RANTES-NIS-MSCs in the tumor stroma, whereas nontarget organs showed no significant MSC recruitment/transgene expression. Administration of a therapeutic dose of 131I or 188Re (55.5 MBq) in RANTES-NIS-MSC-treated mice resulted in a significant delay in tumor growth and improved survival without significant differences between 131I and 188Re.
These data demonstrate successful stromal targeting of NIS in HCC tumors by selective recruitment of NIS-expressing MSCs and by use of the RANTES/CCL5 promoter. The resulting tumor-selective radionuclide accumulation was high enough for a therapeutic effect of 131I and 188Re opening the exciting prospect of NIS-mediated radionuclide therapy of metastatic cancer using genetically engineered MSCs as gene delivery vehicles.
Endocrinology, Diabetes, & Metabolism, University of Colorado, Aurora, CO
Thyroid Cancer Saturday Poster Basic
Thyroid cancer causes >1700 deaths/year in the United States, and metastatic differentiated thyroid cancer (DTC), poorly-differentiated thyroid cancer (PDTC), and anaplastic thyroid cancer (ATC) cause a majority of these deaths. Our group recently reported the novel findings that peroxisome proliferator-activated receptor gamma (PPARγ) is highly expressed in ATC compared to DTC and promotes tumor growth and invasion.
shRNA-mediated PPARγ silencing, microarrays, Western blot (WB) analysis, immunohistochemistry (IHC), genetic TXNIP overexpression, proliferation assays, and pharmacologic treatment of ATC cells
Using microarray analysis, we show that TXNIP is upregulated 11.2-fold when PPARγ is knocked down with shRNA in HTh74 ATC cells. TXNIP regulates cellular redox status, inhibits glucose uptake and cell cycle progression, and is a tumor suppressor in different types of cancer. The role of TXNIP in thyroid cancer has not been evaluated. WB and IHC analysis of multiple thyroid cancer cell lines as well as primary thyroid cancer cell culture and tissue specimens reveal high TXNIP levels in DTC cells (TPC-1, BCPAP, and MDAT41) and normal thyroid in contrast to low or undetectable TXNIP levels in ATC cells (HTH74, C643, TJH11T, T238, and 8505C). Genetic overexpression of TXNIP in HTh74 cells produces a 53% inhibition of proliferation compared to vector controls (p=0.0244). To determine if TXNIP can be upregulated by pharmacologic agents, HTh74 cells were treated with D-allose (positive control) and pathway-specific targeted therapies. Only the PI3K inhibitor LY294002 and the mTOR inhibitor rapamycin increased TXNIP protein levels in these ATC cells, suggesting that the PI3K-mTOR pathway may be involved in TXNIP suppression in ATC. LY294002-mediated TXNIP upregulation was also observed in other ATC cells (T238 and C643).
The tumor suppressor TXNIP is expressed in normal thyroid tissue and DTC with a loss of expression in ATC, and inhibitors of PI3K and mTOR can reinduce expression of TXNIP in ATC cells. TXNIP regulation appears to be an important step in thyroid cancer progression to PDTC and ATC, and these data highlight the potential of TXNIP as a biomarker and therapeutic target in the treatment of advanced thyroid cancer.
Nuclear Medicine and Endocrine Oncology, Institut Gustave Roussy, Villejuif, France
Thyroid Cancer Saturday Poster Basic
Radioactive iodine (RAI) ablation for low-risk differentiated thyroid cancer (DTC) is still a matter of debate. In the absence of RAI, data regarding serum thyroglobulin (Tg) levels measured with a sensitive method during levothyroxine treatment (Tg/LT4) are missing.
This single-center retrospective study assessed serum Tg/LT4, using the Tg assay Access® kit with functional sensitivity of 0.1 ng/mL, in 88 consecutive patients treated by total thyroidectomy without RAI ablation for low-risk DTC and tumors of uncertain malignant potential (TUMP).
Eighty-eight patients (68 F, 20 M; mean age 50 yr), with DTC (80) and TUMP (8), were included. DTCs were classified as pT1, pT2, and pT3 in 76, 1, and 1 case, respectively, and pN0, pNx, and pN1 in 41, 31, and 6 cases, respectively. Following surgery, 10 patients had Tg antibody (TgAb). Among those without TgAb, Tg/LT4 was ≤2 ng/mL in 97%, ≤1 ng/mL in 97%, and ≤0.1 ng/mL in 50% of patients. From 12 to 24 months after surgery, the Tg/LT4 level measured in 48 patients was ≤2 ng/mL in 96%, ≤1 ng/mL in 90%, and ≤0.1 ng/mL in 50% of patients. After a median follow-up of 2.5 years (range: 0.6–7.2 yr), two cases had persistent or suspicious disease, one patient with a Tg/LT4 at 11 ng/mL and an abnormal neck ultrasonography and one patient with an increasing Tg/LT4 at 2 ng/mL and with a normal neck ultrasonography.
Within the first two years following total thyroidectomy without RAI ablation, Tg/LT4 level is ≤2 ng/mL in 96 to 97% of low-risk DTC patients and can be considered as a reliable marker of the absence of disease.
Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN
Thyroid Cancer Saturday Poster Basic
The PAX8/PPARγ fusion protein (PPFP) is associated with less-aggressive disease in follicular thyroid carcinomas (FTCs) (Sahin et al. J Clin Endocrinol Metab 90:463, 2005), suggesting that PPFP may favorably impact FTC outcomes. We have demonstrated that PPFP inhibits tumorigenesis in vivo by decreasing neovascularization in human thyroid and mouse xenograft tumors while upregulating expression of multiple tumor suppressor microRNAs, including miR-122, and miR-375 in FTC (Reddi et al. Genes Cancer 1:480, 2010, Reddi et al. Genes Cancer 2:46, 2011).
To identify PPFP-mediated pathways, we constitutively expressed PPFP in FTC-derived WRO-82-1 (PTEN-intact) and FTC-133 (PTEN-null) cell lines.
WRO-PPFP cells showed 9-fold (p<0.0001) reduced tumor progression, while FTC-133-PPFP cells showed only modest 1.5-fold (p<0.0079) inhibition of xenograft tumor progression. Restoration of PTEN expression to wild-type FTC-133 cells completely (100%) inhibited tumor progression, while FTC-PPFP-PTEN cells showed only a 72% inhibition of tumor progression, suggesting that PPFP may be inhibiting PTEN function. However, absence of AKT (Thr308) phosphorylation in FTC-PPFP-PTEN cells indicated that PTEN was likely functional. We observed that PTEN expression was upregulated in WRO-PPFP cells and correlated with reduced levels of pPDK1 and reduced AKT(T308) phosphorylation. Immunohistochemistry confirmed that PTEN expression was increased in human tumors expressing PPFP, while PPFP-negative FTC had weak or no PTEN expression. Furthermore, in vitro studies demonstrate that upregulation of PTEN by PPFP involves transcriptional (increased PTEN promoter activity) and post-translational (increased PTEN half-life and decreased proteosomal degradation) mechanisms. Cellular fractionation and in situ fluorescence staining studies demonstrate nuclear localization of PTEN in the presence of PPFP, suggesting that tumor suppression is mediated by nuclear PTEN events, including control of cell growth, cell cycling, and chromosomal stability.
We conclude that PPFP independently functions as a tumor suppressor in FTC, mediated in part by modulating PTEN expression.
Laboratory Medicine and Pathology, Mayo Clinic, Rochester, MN
Thyroid Cancer Saturday Poster Translational
Anaplastic thyroid cancer (ATC) accounts for <5% of all thyroid cancer cases. Most ATC are inoperable at the time of diagnosis and fatal within a few months. ATC is largely unresponsive to traditional therapies, including radioactive iodine, external beam radiation, or chemotherapy. Given the aggressive nature of this cancer and lack of effective treatment options, there is a pressing need to develop novel therapeutic strategies. The rearranged PAX8/PPARγ fusion gene occurs frequently in follicular thyroid cancer (FTC). We recently discovered that the PAX8/PPARγ fusion protein (PPFP) exhibits a distinct tumor suppressor function. Three lines of evidence support this conclusion. PPFP expression is associated with favorable prognosis in FTC (Sahin et al. JCEM 90:463, 2005); PPFP inhibits aggressive tumorigenesis in vivo by decreasing neovascularization in human thyroid and mouse xenograft tumors; and PPFP upregulates expression of multiple tumor suppressors, including PTEN, miR-122, and miR-375, in FTC (Reddi et al. Genes Cancer 1:480, 2010, Reddi et al. Genes Cancer 2:46, 2011). We therefore evaluated the therapeutic potential of PPFP in ATC.
We constitutively expressed PPFP in five ATC-derived cell lines (BHT-101, KTC-2, KTC-3, FRO, and C-643) and evaluated them for cell growth in vitro using MTT assay and xenograft tumor growth in vivo. Thyroid expression markers (NIS, Tg, TPO, and PAX8) were evaluated using RT-PCR, and transcriptional activation was confirmed by reporter analysis. NIS function was evaluated by radioactive iodine-uptake studies.
Ectopic expression of PPFP in five ATC-derived cell lines significantly inhibits cell growth in vitro in all 5 cell lines (1.5- to 2-fold, p<0.05) and xenograft tumor growth in vivo in 3 cell lines (5- to 15-fold, p<0.005). PPFP increases expression of NIS, PAX8, and/or TPO transcripts, suggesting that PPFP may affect redifferentiation. Increased expression of these transcripts is associated with increased promoter activity. Moderate increase in iodine uptake was observed in both FRO-PPFP and KTC-3-PPFP cells that had upregulated NIS expression.
Overexpression of PPFP may offer a novel therapeutic strategy for treatment of anaplastic thyroid cancer.
Surgery, Boston University, Boston, MA
Thyroid Cancer Saturday Poster Translational
Thyroid cancer is the most common endocrine malignancy. The current gold standard, fine-needle aspiration biopsy (FNAB), yields 10–10% indeterminate results necessitating thyroidectomy for diagnosis. Elastic scattering spectroscopy (ESS) is a new, minimally invasive optical biopsy technique, mediated by a fiber-optic probe sensitive to cellular and subcellular features. We assessed the potential to incorporate an ESS probe into preoperative transcutaneous aspiration biopsy to differentiate benign from malignant thyroid nodules.
We built a miniaturized ESS probe to fit through a 23-gauge biopsy needle and tested it with IRB approval on 64 patients undergoing ultrasound-guided FNAB of thyroid nodules. ESS data were collected from three distinct locations within the thyroid nodule. Cytology was our gold standard and postsurgical pathology for indeterminate cytology.
All patients tolerated the procedure well; additional time required was less than 30 seconds. Spectral appearance differed between solid and liquid portions of the thyroid nodule. Only one patient had an insufficient biopsy (1.5%); spectra could be collected on all patients. Cytology obtained with the integrated ESS-FNA device compared to standard FNAB showed similar numbers and types of cells. A waveform signature could discriminate benign from malignant disease.
It is feasible to collect cytologic material and ESS data in the clinic during ultrasound-guided FNAB using a miniaturized combined ESS-biopsy needle probe. Cytology is comparable to conventional FNA biopsy; ESS data from this miniaturized optical probe are comparable to the standard ESS probe used in the diagnosis of other malignancies. Preliminary analysis reveals a unique waveform signature that can differentiate benign from malignant thyroid nodules and improve targeting of biopsies. With the collection of further data, an algorithm using cytology and ESS data could potentially be used as an in-situ real-time minimally invasive adjunct to conventional FNA cytology to improve diagnosis and prevent unnecessary surgery.
Internal Medicine, Medical School of Ribeirao Preto, University of Sao Paulo, Brazil, Ribeirao Preto, Brazil
Thyroid Cancer Saturday Poster Translational
Fine-needle aspiration biopsy (FNAB) represents at present the most sensitive and specific method for the identification of malignant thyroid nodules (TN); however, it has substantial limitations. About 20%-30% of all FNABs are diagnosed as indeterminate for malignancy, often prompting diagnostic thyroidectomy. Among them, 8%-56% are found to be malignant. Such a high number of noncancer thyroid surgeries results in additional morbidity and higher healthcare costs. Objectives: To evaluate the contribution of testing the V600E BRAF in improving the FNAB diagnosis of TN.
This prospective study included 230 samples of TN from 192 patients. After the cytological smears, the puncture needle was washed with saline. After extraction and amplification, the DNA was subjected to digestion with the enzyme XbaI. In the presence of the mutation V600E BRAF, a fragment of 166 pb is displayed in a 10% polyacrylamide gel. The mutations status was correlated with cytology and surgical pathology diagnosis.
In accordance with the results of the cytological examination, patient samples were subdivided as Bethesda I (n=32, 13.9%), II (n=72, 31.3%), III (n=52, 22. 6%), IV (n=30, 13.0%), V (n=23, 10.0%), and VI (n=21, 9.2%). The search for BRAF mutation was positive in 37 samples (16.1%): Bethesda I=3, 9.4%: II=2, 2.8%; III=3, 5.8%, IV=4, 13.3%, V=8, 34.8%; VI=17, 81%. So far were operated 68/159 patients negative for BRAF mutation and 24/33 patients positive for mutation. Twenty-nine out of 68 patients negative for the mutation were diagnosed with papillary thyroid carcinoma (PTC), and 24/24 patients positive for the mutation were confirmed to PTC. The prevalence of BRAF mutation was 45% in patients diagnosed with PTC. The sensitivity and accuracy of cytological results were 45% and 65.2%, respectively, and increased to 62.3% and 75% when cytological results were associated with BRAF V600E mutation research.
A combination of cytology and molecular test for only one mutation in FNAB samples, such as V600E BRAF, enhances the sensibility and accuracy of FNAB cytology for the diagnosis of PTC and allows the identification of PTC in samples classified as Bethesda I, II, III, and IV.
Cancer Biology and Angiogenesis, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA
Thyroid Cancer Saturday Poster Translational
Myopericytoma is a mesenchymal tumor characterized by perivascular proliferation of oval to spindled cells with myoid and pericytic features. BRAFV600E mutation can occur in epithelial or mesenchymal cancers with a crucial role in tumor cell-matrix adhesion (microenvironment).
We report the first case (45-yo woman) of myopericytoma arising in the thyroid and harboring BRAFV600E. Thyroid imaging and 18FDG PET/CT were performed to assess disease stage. DNA large-scale genotyping and immunohistochemistry were performed on excised thyroid myopericytoma (TM) tissue and tissue-derived primary TM cell cultures. Mutant BRAFV600E mRNA was knocked down in TM cells by specific short-hairpin (sh) RNA with cell adhesion/migration, and senescence assays performed. Extracellular matrix (ECM) genes were assesses by qPCR/multiprofiling gene expression, and anchorage (Matrigel) assays were developed. TM cell viability was determined with vemurafenib (a selective inhibitor of BRAFV600E).
Thyroid imaging revealed a goiter associated with an irregular/hypoechoic/hypervascularized/hypofunctional mass in the left thyroid lobe with mediastinal extension and high 18FDG uptake. The mass was diagnosed as TM. It harbored the heterozygous BRAFWT/V600E mutation and showed extension to the perithyroidal fibroconnective tissue, but no neck lymph nodes/distant metastases were detected. Both TM tissue and established primary TM cells harbored BRAFV600E and were positive for smooth muscle actin, phosphor-ERK1/2, Ki67, and stem cell markers. A higher vascular density (CD31+) was also found in the TM vs. normal thyroid. PTH and thyroid-specific markers were negative. Sh-control TM cells expressed high levels of ECM molecules (mRNA and protein); as a result, they grew as cell aggregates in Matrigel. Sh-BRAFV600E TM cells showed a significant reduction of cell adhesion/migration and increased senescence vs. controls. Vemurafenib significantly reduced viability of TM cells vs. controls.
We report the first TM and primary TM cell culture with heterozygous BRAFV600E. We demonstrate BRAFV600E-dependent cell adhesion/migration. These results also suggest that vemurafenib might have a potential therapeutic efficacy in patients with BRAFWT/V600E-TM.
Internal Medicine, Endocrinology, University of Patras Medical School, Patras, Greece
Thyroid Cancer Saturday Poster Translational
It has been known for decades that oxidation of iodide and oxidation of thyroglobulin are central steps in thyroid hormone synthesis, yet the importance of oxidative stress in thyroid gland pathologies was recognized only recently. Compared to other tissues, the thyroid has high antioxidant capacity, but the precise molecular nature of its antioxidant defenses is poorly known. NQO1 [NAD(P)H:quinone oxidoreductase 1] is an important antioxidant and detoxification protein, with multiple roles in restoring redox balance and preserving homeostasis; its expression in human thyroid has been previously reported. Increased levels of oxidized lipids and DNA have been found in thyroid cancer, but it remains unknown whether these result from reduced antioxidant defenses in the cancer tissue. To address whether the increased oxidative damage seen in thyroid cancer results from reduction of antioxidant defenses, we assessed NQO1 protein abundance in a panel of papillary thyroid cancer samples.
We analyzed a total of 26 anonymized formalin-fixed paraffin-embedded papillary thyroid cancer samples. A previously characterized mouse monoclonal anti-human NQO1 antibody (A180, sc-32793; Santa Cruz) was used in a standard immunohistochemistry protocol to detect NQO1 in the cancer tissue and in healthy thyroid tissue from each patient. The University of Patras Ethics Committee approved the study.
NQO1 protein was undetectable in healthy thyroid tissue. All (26/26) papillary thyroid cancer samples showed cytoplasmic NQO1 staining, ranging from strong (n=9) to moderate (n=9) to weak (n=8).
(i) Specific upregulation of the antioxidant and cell-protective protein NQO1 is ubiquitous in papillary thyroid cancer, and may therefore be considered a new hallmark. (ii) The finding of NQO1 induction suggests that the increased oxidative damage seen in papillary thyroid cancer is unlikely to result from general suppression of antioxidant defenses. (iii) The molecular mechanisms leading to increased NQO1 abundance and the biological consequences of antioxidant defense induction in papillary thyroid cancer warrant further investigation.
Withdrawn
Head and Neck Surgery, Memorial Sloan Kettering Cancer Center, New York, NY
Thyroid Cancer Saturday Poster Clinical
Well-differentiated thyroid cancer (WDTC) is rising in incidence in the United States and across the world. We present the changing trends in the incidence, presentation management, and outcomes of WDTC within our institution over 8 decades.
Retrospective case note review of 2797 patients who had thyroid surgery in the Memorial Sloan Kettering Cancer Center between 1932 and 2005. Data collected included demographics, treatment, histopathology, and outcomes. Variables were compared using Chi-squared test. Oncological outcomes were calculated using the Kaplan-Meier method. Univariate analysis was performed using the log-rank test, and multivariate analysis using Cox regression analysis.
The median follow-up for the group was 90 months. There has been an increase in number of patients managed per decade. The median age of the whole group was 45 years. Patients managed after 1985 were more likely to be over the age of 45 years (53% versus 44%, p<0.001). The percentage of women increased from 68% to 72% (p=0.026), and the percentage papillary carcinomas increased from 78% to 92%, p<0.001. pT1 lesions increased from 19% to 48% in the latter cohort. There was no increase in incidence of pT4 tumors. The percentage of pN+ cases fell from 48% to 33% (p<0.001). The incidence of patients with distant metastasis at presentation was similar. Patients in the later cohort were less likely to have thyroid lobectomy (29% versus 72%, p<0.001). There was a change in the use of RAI, with 8% versus 44% of the latter group receiving postoperative RAI (p<0.001) (see Table). Analysis of factors predictive of poor outcome confirmed non-papillary histology, age over 45 years, M1 or gross extrathyroid extension, and size over 4cm as independent predictors on multivariate analysis of DSS.
Descriptive Statistics of Whole Group And Stratification By Pre/Post-1985
RAI: Postoperative radioactive iodine therapy.
Older patients with earlier-stage disease present an increasing workload for our department. Future efforts must include attempts to identify those patients who will benefit from less-invasive treatment, while focusing of resources on those patients most likely to benefit.
Thyroid Cancer Saturday Poster Clinical
Age and extrathyroidal extension are the 2 most important predictors of outcome in patients with papillary thyroid cancer. Nodal metastases are generally agreed to be less predictive of outcome. This is reflected in the current AJCC staging system for thyroid cancer. Patients <45 yrs are staged as stage I regardless of primary tumor size, ETE, and nodal status and are only classified as stage II if distant disease is present. In contrast, patients >45 yrs are classified into stage I-IV depending on T, N, and M factors. The objective of our study was to determine if the AJCC system accurately predicts disease specific survival in patients>45 yrs with and without nodal metastases.
The records of 792 patients over 45-years old with PTC and without distant metastases treated at MSKCC between 1985–1985 were analyzed. Five hundred fifty-six were women (70%); 399 were pT1 (50%), 102 pT2 (13%), 220 pT3 (28%), and 71 (9%) were pT4; 583 (73%) were N0, and 209 (27%) were N1. Disease-specific survival (DSS) were then determined for patients with and without nodal disease, stratified by AJCC stage, using the Kaplan-Meier method.
For patients with N0 disease, 347 (60%) were stage I, 86 (16%) stage II, 129 (22%) stage III, and 21 (4%) stage IV according to AJCC criteria. With a median follow-up of 51 months, the 5-year DSS was 100% for all patients regardless of stage. For patients with N1 disease, 69 (33%) stage III and 140 (67%) stage IV according to AJCC criteria. With a median follow-up of 62 months, the 5-year DSS was 100% for stage III and 93% for stage IV, p=0.045 (see Figure).
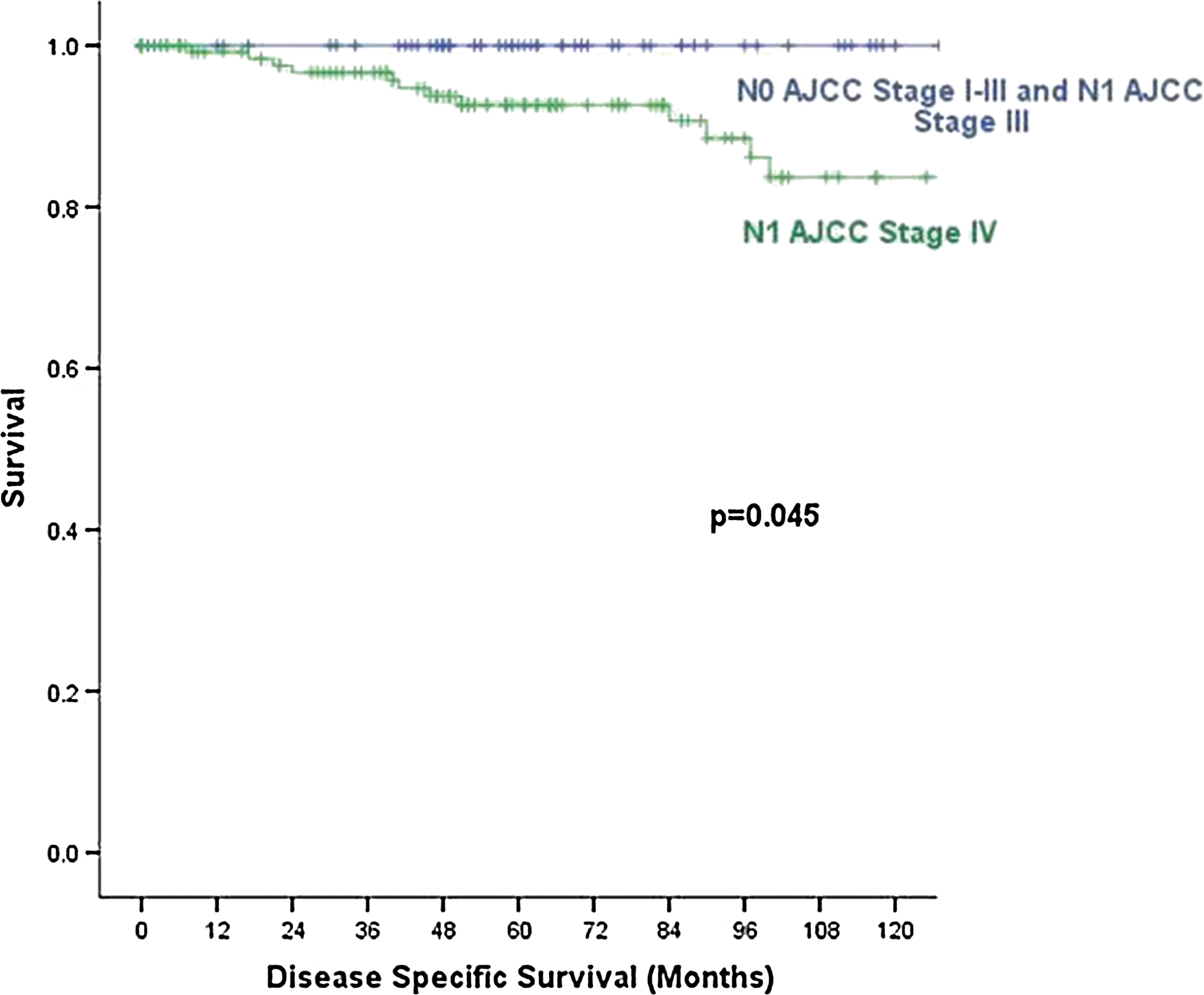
Disease-specific survival of 792 patients treated at Memorial Sloan-Kettering Cancer Center, 1985–1985.
In patients over 45 yrs of age with PTC, the AJCC staging system accurately predicts outcome in patients with N1 disease, but does not predict outcome in patients with N0 disease, all of whom survived in this study. With an increasing number of patients >45 yrs being diagnosed with T3T4N0 disease, the AJCC staging system requires modification to take this into account.
Thyroid Cancer Saturday Poster Clinical
Medullary thyroid cancer (MTC) is one of the most aggressive thyroid tumors. Its prognosis is dependent from the stage at diagnosis. Since MTCs<1 cm (mMTCs) are present in 0.2 to 8% at autopsies, they are considered clinically irrelevant.
A total of 84 sporadic mMTCs (up to 1.5 cm) were selected from a series of 610 MTCs (13.7%). They were 30 men and 54 women. The mean age at the diagnosis was 51.4 yrs. Thirty-four out of 84 (40.5%) had lymph node metastases, and 3/84(3.5%) had liver metastases. Fifty-eight out of 84 (69%) were diagnosed by routine serum calcitonin (Ct); the other 26/84 (31%) were incidental findings (n=10) or diagnosed with cytology (n=16). After a mean follow-up of 7 years (range 2–2 yrs), 48/84 (57%) patients were cured (i.e., 2 negative stimulation tests); 17/84 (20%) were biochemically affected; and 19/84 (22.6%) had metastases. No patients died for the disease.
According to the diameter of the mMTC, we distinguished 12/84 (14.3%) mMTC<0.5 cm [group-A]; 52/84 (61.9%)>0.5, and <1 cm [group-B] and 20/84 (23.8%)>1 cm [group-C]. The extension of the disease was significantly correlated with the diameter of the mMTC, and none (0/12) of the group-A showed metastatic lesions (p=0.0033). However, 20/52 (38.5%) of group-B and 12/20 (60%) of group-C showed lymph node and/or distant metastases. The 3 cases with liver metastases belonged to group-C. Nine out of12 (75%) of group-A were cured, while 3 remained biochemically affected; 30/52 (57.7%) of group-B were cured, while 22 were affected (n=13 biochemically, n=9 with evident metastases); 9/20 (45%) of group-C were cured, while 11 were affected (n=1 biochemically, n=10 with evident metastases). Eleven out of 12 (91.7%) of group-A, 39/52 (75%) of group-B, 8/20 (40%) of group-C were diagnosed with Ct.
From this study, it appears that the definitive cure is correlated with the diameter: in mMTCs<0.5 cm, we can expect a definitive cure in 75% of cases and a biochemical persistence in 25% of cases, and it decreases to 57.7% and 45% in mMTCs>0.5 and <1 cm and >1 cm and <1.5 cm, respectively, and a higher prevalence of metastatic affected patients are present in these groups. The question of whether the mMTCs<0.5 cm could be innocuous tumors never developing into bigger tumors remains to be answered.
Medicine, University of Southern California, Los Angeles, CA
Thyroid Cancer Saturday Poster Clinical
TgAb methods vary widely in specificity, and the cut-off values used to define TgAb positivity*. Both false-negative and false-positive serum TgAb classifications can mask persistent/recurrent DTC. False-negative TgAb prompts the use of Tg IMA methodology (TgIMA) that underestimates Tg when TgAb is present, whereas false-positive TgAb classifications prompt the use of TgAb-resistant Tg methodologies [radioimmunoassay (RIA) or tandem mass spectrometry (TMS)] that have inferior functional sensitivities (FS=20% between-run imprecision over 6–6 months) as compared with second-generation TgIMAs [FS=∼0.5 or ∼2.6 versus ≤0.10 μg/L(ng/mL)], for TgRIA or TgTMS versus TgIMA, respectively.
This study compared the frequencies of false-positive and false-negative serum TgAb classifications for the Kronus (FS=0.4 kIU/L) versus Roche (FS=?15 kIU/L, still being determined) TgAb methods using different cut-off values, and TgIMA/TgRIA ratios of <75% as an independent indicator for the presence of interfering TgAb*.
Thirty-eight out of 84 (38%) of consecutive Tg+TgAb requests had TgAb detected (≥0.4 kIU/L) using Kronus, versus 100, 77, 48, and 35 percent using Roche cut-offs of <10, 15, 20, and 25 kIU/L, respectively. Twenty-seven percent of specimens that were undetectable by Kronus (<0.4 kIU/L) had Roche values>20 kIU/L. Tabulated are TgAb false-positive and false-negative frequencies at different cut-off values applied to a cohort of 841 DTC sera with unequivocally detectable TgRIA [≥1.0 μg/L(ng/mL)] values. In 503/841 (59.8%), TgIMA/TgRIA ratios were <75%, suggesting the presence of interfering TgAb. Severe interference [TgIMA=≤0.10 μg/L(ng/mL)] that has the potential to influence clinical decision making was evident in 190/503 (37.8%) of these sera.
False-positive and false-negative TgAb classifications were seen for both methods at all cut-off values. Using Kronus-versus-Roche cut-offs of <0.4 versus 20 kIU/L, respectively, the frequency of false-negative classifications appeared comparable (5.4 versus 4.9 percent). However, false-positive classifications were higher for the Roche method at the lower cut-off values, possibly reflecting sensitivity limitations for measuring values <20 kIU/L. *Spencer et al. JCEM 96:1283, 2011
Influence of Cut-off Value on TgAb Classifications
# 2nd-generation Tg IMA μg/L (ng/mL).
Thyroid Cancer Saturday Poster Clinical
Hürthle cell carcinoma (HCC) is rare and considered as an aggressive variant of follicular carcinoma due to their ability to develop metastases. Many questions are unsolved. The objective of this study was to assess the outcome of patients with HCC.
One hundred thirty patients with HCC were identified from 3 comprehensive cancer center databases and treated between 1968 and 2010. Patient's characteristics, histological findings, treatments, and follow-up data were reviewed. Disease-specific survival (DSS) was calculated by Kaplan-Meier method.
Eighty-three out of 130 were women (sex ratio 1.8). Median age at diagnosis was 58.6 yrs (range 16–16). Median tumor size was 35 mm. Nodal involvement was rare (6.3%). Six patients had metastases at presentation, and 40.8% had local advanced stage (pT3 or pT4a). Diagnosis was initially missed in 10 cases and corrected at relapse and/or after review by a thyroid expert pathologist. Thirty-five patients had initially or developed metastases, generally radioiodine refractory and some rare metastasis localizations (pleura, endobronchic, liver, skin, stomach, muscle, or kidney) were observed. FDG Pet-scan SUVmax was high (median 13.5, range 3.7–48.7). Ten-year DSS was 84.4% IC 95[76.8–91.8%] and, respectively, 95.7% for minimally invasive and 75.6% for widely invasive (p=0.005). Median DSS after metastasis was 6.2 yrs. Local treatments (surgery, radiofrequency, cementoplasty, and/or external radiotherapy) permit prolonged survival with good quality of life for slowly progressive patients.
Our study confirms that diagnosis of HCC is difficult and often occurred for elderly patients at advanced stage. Prognosis is good for minimally invasive HCC, but even in this case metastases could occur. In widely invasive HCC, prognosis is worse, because generally, iodine refractory. Some metastases grow slowly, and local treatments should be then discussed. Specific biological studies are required for a better understanding of this rare disease and to help diagnosis.
IMPACT OF DEGREE OF EXTRATHYROIDAL EXTENSION OF DISEASE ON PTC OUTCOME
Thyroid Cancer Saturday Poster Clinical
The clinical importance of extrathyroidal extension (ETE) on outcome of papillary thyroid cancer (PTC), particularly with respect to disease extending to the surgical margin is not well established. This study assesses the importance of surgical margin and extrathyroidal invasion relative to local control of disease and oncological outcome.
A retrospective analysis of a prospective institutional endocrine database was conducted on 276 patients with PTC treated between 1955 and 2004 according to impact of margin-negative resection (n=199, 72%), disease up to surgical margin (n=19, 7%), microscopic (n=39, 14%), and gross (n=19, 7%) ETE. Data were compared with Fisher's exact test or ANOVA.
Median follow-up was 3.1–6.8 years per study group (disease-free survival, range 1–1 years). The proportion of those with age>45 years, prior radiation exposure, distant metastasis at presentation, and those undergoing total thyroidectomy was not significantly different between groups (see Table). Tumor size and multifocality correlated with extent of local disease, which in turn was significantly associated with regional nodal disease at time of primary operation and incidence of persistence of disease after multimodality therapy. Extent of local disease correlated significantly with subsequent clinical recurrence after a disease-free period; however, it was not significantly different between negative and close margin resection.
Analysis of 276 Patients with PTC Treated Between 1955 and 2004
Control of disease correlates with extent of extrathyroidal invasion; outcome is significantly worse in patients with gross extrathyroidal disease extension than in those with microscopic local invasion apparent on histopathological assessment. However, risk of clinical recurrence appears similar between patients undergoing margin-negative and close-margin resection.
Thyroid Cancer Saturday Poster Clinical
Worldwide, the increase in thyroid cancer incidence is paralleled by the increasing power of detection owing thyroid-imaging modalities and FNAC. Besides this temporal variation, large geographical variations exist and might be similarly associated with increased detection. Here we studied variations in use of screening exams leading to detect functional or structural thyroid abnormalities in Belgium, a western European country (11,000,000 inhabitants) with mild iodine deficiency. The Belgian Cancer Registry (BCR) reported marked geographical variations in thyroid cancer incidence, with a European Standardized Incidence Rate (ESR) of 3.3 and 6.7 per 100,000 person years (py) in the North (Flanders) and the South (Wallonia), respectively, further designated as low- and high- incidence regions (LIR and HIR). This geographical difference was mainly explained by an increased proportion of small (T1) papillary thyroid cancers [ESR of T1 PTC of 1.4 and 4.1 per 100,000 py in the LIR and HIR, respectively (BCR 2004–2004)].
A representative sample of the Belgian health insurance database (2003–2008) was used to calculate the age-standardized rate of tests potentially leading to the discovery of thyroid disease (serum TSH, neck ultrasound, carotid duplex, CT, or MRI, or PET), both in the global population residing in the LIR and HIR, and in a restricted population (excluding individuals with a history of thyroid disease).
In the global population, the TSH testing rate was lower in the LIR compared to the HIR. However, the difference was not statistically significant in the restricted population [338.3 (95%CI 337.2–339.4) vs. 350.1 (95%CI 348.6–351.7) per 1,000 py, p=0.3]. The rate of imaging procedures potentially unmasking an occult thyroid tumor was significantly lower in the LIR compared to the HIR, both in the global population as well as in the restricted population (p<0.0001) (see Table for the restricted population).
Geographical thyroid cancer incidence variations parallel substantial variations in the use of a panel of diagnostic imaging tests, potentially leading to incidental detection of thyroid cancer.
PROSPECTIVE EVALUATION OF THE MCGILL THYROID NODULE SCORE. IS IT A VALID TOOL?
Thyroid Cancer Saturday Poster Clinical
Despite the rise in incidence of thyroid cancer, no tool exists to help predict which thyroid nodules harbor malignancy. Our group recently developed the McGill Thyroid Nodule Score (MTNS), which can help predict the risk of malignancy. This study aims to prospectively validate it.
Two hundred forty-five consecutive patients were enrolled between July 2009 and March 2011. MTNS scores, age, gender, and extent of surgery were recorded at their first visit. Final pathology was recorded postoperatively. The percentage of malignancy was calculated for each MTNS score. Using Fisher's exact test, the risk of malignancy for each group was compared to that anticipated based on the MTNS. We then used linear regression to plot a best-fit curve for both the retrospective and prospective data and compared the two.
We found no statistically significant difference when comparing the risk of malignancy between the retrospective group originally used to create the MTNS and the prospective group used to validate this tool with p>0.05 for all groups. Regression analysis revealed linear curves with no significant difference between them (p=0.35).
Therefore, we can conclude that the MTNS system is in fact a valid tool and can assist clinicians with multiple aspects of the management of patients with thyroid nodules. These aspects include the prediction of which nodules harbor malignancy, the facilitation of surgical decision making, interprofessional communication, as well as patient discussion.
McGill Thyroid Nodule Score
Thyroid Cancer Saturday Poster Clinical
BRAF mutations are the most common genetic abnormality in PTC. Mutations in PI3K have been identified in thyroid cancers and, although relatively common in anaplastic, are rare in PTC. Mutations involving one of these genes rarely overlap in the same tumor.
We describe 3 cases of aggressive PTC with dual somatic mutations in BRAF and PI3K
Case #1 is a 65-year-old (yo) man with PTC who underwent total thyroidectomy (TT), neck dissection, and radioactive iodine (RAI), with negative post-treatment scan. CT chest was negative at diagnosis. Four months later, he was noted to have rapid progressive disease (PD) with neck, lung, and bone metastases. Patient underwent a CT-guided biopsy of the lung, which confirmed poorly differentiated PTC. He was not eligible for clinical trial due to congestive heart failure history. Treatment with carboplatin and docetaxel was initiated, but was discontinued due to PD. He was then started on sorafenib, but expired 4 weeks later due to PD. Case #2 is a 57-yo woman with PTC diagnosed at 46 yo. She underwent TT, and received 616 mCi of RAI over 6 years. Due to progressive peritoneal, liver, and lung metastases, she was referred to our institution. After molecular analysis was performed, patient started on a selective BRAF inhibitor and had a response of stable disease with regression. She was taken off study 8 weeks later due to PD. Subsequently, she received a PI3K+MEK inhibitor. Restaging showed a response to therapy (see Figure). She had significant skin toxicity, progressed during drug hold, and died 6 months later. Case #3 is a 49-yo man with widely metastatic poorly differentiated PTC treated with partial lobectomy (due to unresectability), and chemoradiation. He was noted to have rapid PD with lung, bone, and brain involvement 4 months later. The patient was offered a clinical trial, but instead opted to start sunitinb outside a trial. First restaging is not yet available. Table 1 summarizes mutations identified in each case.
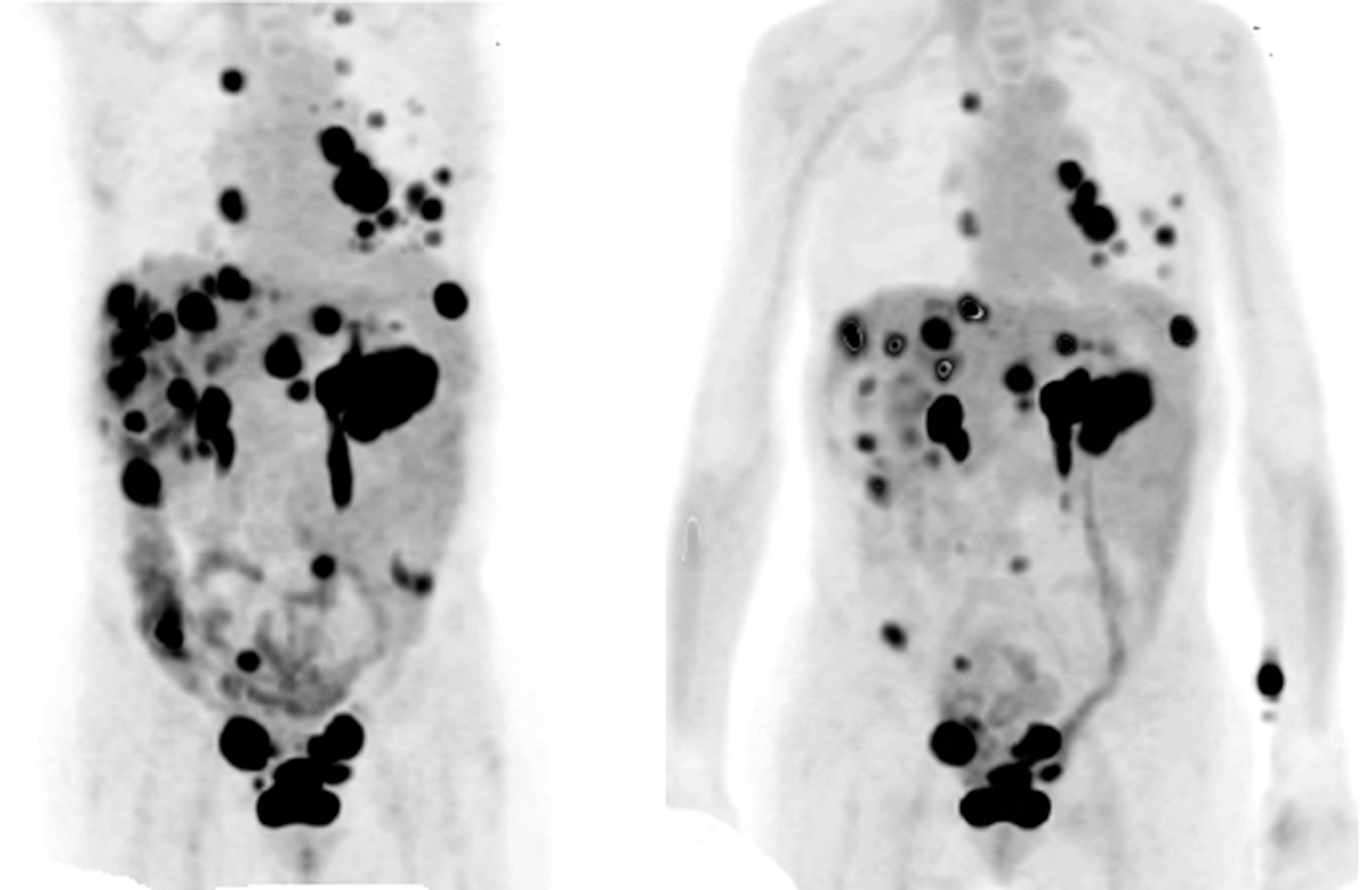
Case # 2: Metabolic response to PI3K+MEK inhibitor
Dual somatic mutations in BRAF and PI3K occur in patients with aggressive PTC, and genetic testing should be offered to these patients. Targeted therapy with selective inhibitors of MAPK and PI3K pathways on a clinical trial may be an effective treatment.
Thyroid Cancer Saturday Poster Clinical
Adequate surgery is the only curative treatment for medullary thyroid cancer (MTC). Reoperation after inappropriate surgery is warranted, but is more challenging due to fibrosis with more recurrences and reoperations. Therefore, we evaluated the clinical outcome in reoperated MTC patients.
We retrospectively reviewed all records of MTC patients (n=156) visiting one of the two major tertiary referral centers between 1980 and 2010. Only patients presenting initially with palpable thyroid nodules and/or suspicious lymph nodes, without distant metastasis (n=85), were included. Adequate surgery was defined as a total thyroidectomy with central compartment dissection and lateral neck dissection if indicated or as biochemical cure after at least a total thyroidectomy. Patients were categorized into two groups: those treated appropriately in one session (n=64) and those who needed two sessions (n=21). These groups were compared with respect to central compartment involvement, disease stage, number of reoperations, and clinical disease-free survival.
Patients treated adequately in one session (n=64) had more often central compartment involvement (62.9% vs. 22.2% p=0.003) and more locally advanced disease (stage 3/4) (75.8% vs. 47.4%; p=0.025) compared to patients who were treated appropriately in two sessions. Patients with nodal involvement or stage 3/4 disease, who needed two sessions for adequate surgery, underwent more reoperations (after the second session) compared to patients treated appropriately in one session (1.00 vs. 0.54, p=0.21; NS and 1.22 vs. 0.51, p=0.006) (see Figure). Patients treated adequately in one session had a longer clinical disease-free survival (60 vs. 36 months, median, p=0.98), but this difference was not statistically significant.
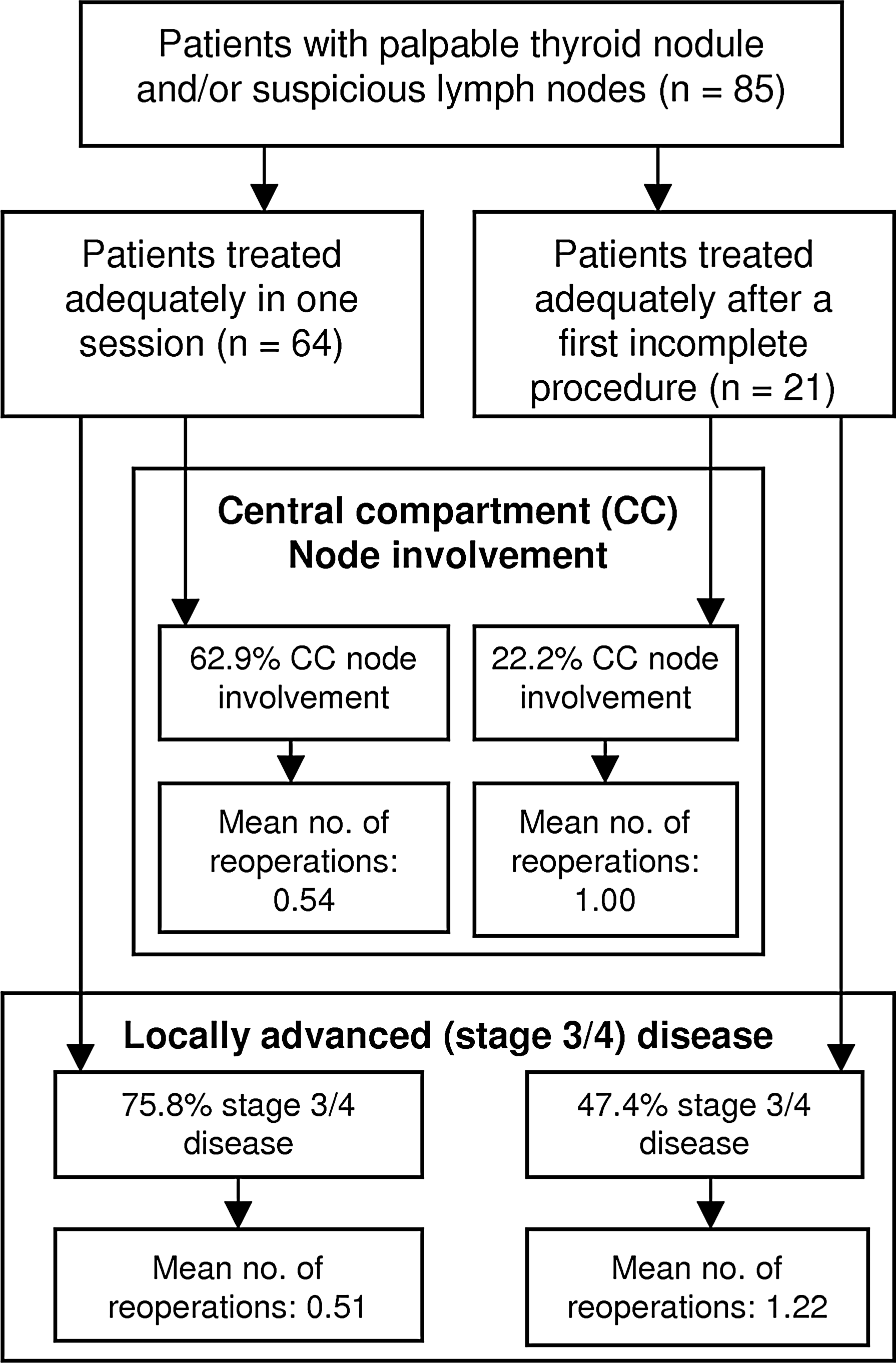
Number of reoperations in patients with nodal involvement or locally advanced disease treated initially in one or two sessions
Patients who needed two procedures for adequate surgery had less locally advanced disease compared with patients treated initially appropriate in one procedure. Furthermore, patients with locally advanced disease required more reoperations (after the second session) when initially treated in two sessions compared to patients treated in one session.
Thyroid Cancer Saturday Poster Clinical
Inter-regional variations in thyroid cancer incidence might be associated with variations in thyroid imaging, FNAC, or thyroid surgery. Here, we studied variations in FNAC and thyroid surgery, as well as diagnostic and therapeutic approaches, for thyrotoxicosis and thyroid nodular disease in Belgium, a western European country (11,000,000 inhabitants) with mild iodine deficiency and marked geographical variations in thyroid cancer incidence. The northern (Flanders) and southern (Walloon) regions were designated as the low- and high-incidence regions in this model (LIR and HIR) with a European Standardized Incidence Rate (ESR) of, respectively, 3.3 and 6.7 per 100,000 person years (py), and an ESR of T1 papillary thyroid cancer of, respectively, 1.4 and 4.1 per 100,000 py [Belgian Cancer Registry (BCR), 2004–2004].
The Belgian health insurance database (2003–2008) and BCR database were used to calculate age-standardized rates and proportions at the level of 1/all patients with thyrotoxic (TOX) or thyroid nodular (ND) disease, 2/all thyroid surgical patients (SURG), and 3/thyroid surgical patients with final diagnosis of thyroid cancer (SURG CA).
The age-standardized rates (ESR, n/100,000 py) of FNAC were similar in the LIR compared to the HIR (49.9[49.2;50.6] vs. 47.6[46.7;48.5]). The ESR of SURG was however significantly lower in the LIR (34.0[33.4;34.6]) compared to the HIR (80.3[79.1;81.5]), with a cumulative risk of SURG of 2.7% in the LIR compared to 6.5% in the HIR before the age of 75y. As summarized in the Table, thyroid surgery as therapy for TOX and ND was studied, and SURG as well as SURG CA patients were studied for diagnostic procedures and/or treatments before the final histological diagnosis [FNAC, lymph node (LN) dissection at first surgery].
Comparison of Treatments, Diagnostic Approaches, and Incidence of Thyroid Diseases in Belgium
Geographical variation in thyroid cancer incidence is paralleled by a more surgical approach in patients with thyrotoxic, and especially nodular disease, potentially leading to the incidental finding of small thyroid cancers. In the HIR proportionally less surgery is preceded by FNAC, and proportionally less histological diagnosis of thyroid cancer is made following total thyroidectomy.
Thyroid Cancer Saturday Poster Clinical
Ultrasound-guided FNA biopsy (USG-FNAB) is a standard approach in the evaluation of thyroid nodules. The 2009 ATA Guidelines recommend the use of molecular markers to guide treatment in patients with indeterminate FNA cytology. BRAF mutation was found in 50%-70% of papillary thyroid carcinomas (PTC). Limited data are available regarding the BRAF mutation with thyroid lymphoma.
A 54-year-old man presented with diffuse lymphadenopathy. Diagnostic tests: PET CT, bone marrow biopsy, and thyroid USG FNAB for following markers: BRAF, KRAS, HRAS, NRAS, RET/PTC1, RET/PTC3, and PAX8/PPARg (Asuragen Clinical Lab, Austin,TX). Surgery and pathology reports were analyzed.
PET-CT showed diffuse uptake in many osseous lesions and thyroid. Bone marrow biopsy diagnosed sarcoidosis. Thyroid ultrasound showed a very heterogeneous, diffusely enlarged thyroid with increased vascularity in the right lobe. The TSH level was elevated, and throxin started. USG-FNAB of the right thyroid lobe was consistent with atypia of undetermined significance (AUS). Follow-up with repeat biopsy in 3 months was initially suggested, but molecular analysis returned positive for BRAF p.V600E mutation. We suspected PTC, and the patient was scheduled for a total thyroidectomy with central neck lymph node dissection. To confirm a diagnosis of PTC, a right thyroid lobectomy was performed with intraoperative frozen-section sent for pathology. This showed a suspected thyroid lymphoma. The procedure was thus restricted to the right lobectomy only. The final pathologic diagnosis was non-Hodgkin's B-cell type marginal zone lymphoma (see Figure). This patient has subsequently undergone chemotherapy

Thyroid lymphoma.
We have described a unique case of thyroid lymphoma, which presented on USG-FNAB as AUS, and BRAF positive. Establishing the diagnosis of thyroid lymphoma is challenging by USG-FNAB alone. The use of molecular marker analysis changed our conservative approach to diagnostic lobectomy that subsequently demonstrated the correct diagnosis and appropriate treatment for this patient. Future research into the correlation between BRAF mutation positivity and thyroid lymphoma may lead to modifications in the interpretation of the mutational analysis as well as the current treatment paradigm.
Thyroid Cancer Saturday Poster Clinical
In a large, urban US public hospital, patients were found to present with more advanced stage differentiated thyroid carcinoma (DTC) than those in an affiliated, adjacent university hospital. Asians comprised the largest ethnic group (45%) in the public hospital. We conducted a qualitative study to understand experiences and challenges contributing to delays in diagnosis among Chinese patients with thyroid cancer.
Five focus groups and 4 key informant interviews led by trained, bilingual Mandarin speakers were conducted. All adult, Mandarin-speaking patients treated for DTC in the public hospital (2000–2011) met inclusion criteria. A phenomenology approach was used to identify common themes.
Seventeen out of 97 eligible patients participated (11 women, 6 men; average age 47). All participants were born in China, had lived in the United States for an average of 14 years (range: 5–5), and a majority reported not seeking regular medical care in China or the United States. Despite a history of an abnormal thyroid exam in over half, presentation to a physician was delayed by an average of 9 years (range: 2–2). Several challenges and barriers to accessing care were identified, with two main themes: misinformation and/or lack of information on thyroid cancer, and socioeconomic/cultural barriers in accessing the US healthcare system. All study participants reported an unawareness of thyroid cancer before diagnosis, and a majority expressed beliefs that such cancer was caused by contaminated seafood, living by the ocean, or consumption of salt. Socioeconomic constraints included language barriers, seeking care from unlicensed health practitioners, and prioritizing establishing a foothold in the United States over health and health-related needs. Nearly all patients denied using traditional Chinese medicine to treat their thyroid condition.
These data underscore the importance of promoting preventative care and the need for targeted education to address significant misinformation on thyroid cancer in this patient population. Future studies are needed to validate these findings and to develop an educational campaign to reduce delays in diagnosis and ensure that timely care and education are received by this vulnerable population.
DETECTION OF RESIDUAL THYROID TISSUE AFTER TOTAL THYROIDECTOMY FOR DIFFERENTIATED THYROID CARCINOMA
Thyroid Cancer Saturday Poster Clinical
Differentiated thyroid carcinomas are among the most curable cancers. However, some patients are at high risk for recurrent disease or even death. Most of these patients can be identified at the time of diagnosis by using well-established prognostic indicators. The aim of this work was to study the validity of Radioactive Iodine Scanning (RAIS) versus Ultrasonography (US) and Computed Tomography (CT) in the detection of residual thyroid tissue after total thyroidectomy for patients with differentiated thyroid carcinoma (DTC).
Thirty patients with DTC were treated by total thyroidectomy and the appropriate type of neck dissection when indicated. One month postoperatively, they were all adjuvantly treated with radioactive iodine. All patients were followed-up postoperatively by the following: 1) RAIS, CT, and US within two weeks. 2) Serum thyroglobulin after radioactive iodine ablation after one month. 3) RAIS, CT, and US within two months.
After two weeks, US was 90% accurate, followed by CT 83.33%, and then RAIS 46.67%. After two months, US accuracy reached 100%, CT 96.6%, and RAIS 90%.
Neck US is highly specific for detection of residual thyroid tumors at the surgical bed compared to RAIS, although it is an operator-dependent technique. CT follows US as regard specificity for detection of residual tumor, but it is less sensitive. Serum thyroglobulin has the highest sensitivity and specificity for detecting recurrent disease after total thyroidectomy and radioactive iodine ablation of any microscopic residual thyroid cells.
Division of Endocrinology & Metabolism, The Johns Hopkins University School of Medicine, Baltimore, MD
Thyroid Cancer Saturday Poster Clinical
Thyrotropin (TSH) level and thyroid autoimmunity may be of prognostic importance in differentiated thyroid cancer (DTC). Preoperative serum TSH level has been associated with higher DTC stage in cross-sectional studies; data are contradictory on the significance of thyroid autoantibodies at the time of diagnosis. We sought to assess the prognostic importance of preoperative serum TSH and perioperative antithyroglobulin antibodies (TgAb) in DTC patients followed by the National Thyroid Cancer Treatment Cooperative Study, a large multicenter thyroid cancer registry.
Patients registered after 1996 with available preoperative serum TSH (n=617) or perioperative TgAb (n=1770) were analyzed for tumor stage, persistent disease, recurrence, and overall survival (OS) (median follow-up 5.5 yr). Parametric tests assessed log-transformed TSH, and categorical variables were tested with χ2. Disease-free survival (DFS) and OS were assessed with Cox models.
Serum TSH level was higher in patients with higher stage disease (geometric mean stage III/IV=1.48 vs. 1.02 mU/L for stages I/II; p=0.006). The relationship persisted in those aged≥45 years after adjusting for gender (p=0.01). Gross extrathyroidal extension (p=0.03) and presence of cervical lymph node metastases (p=0.003) were also significantly associated with higher serum TSH. Disease recurrence and all-cause mortality occurred in 37 and 38 TSH cohort patients respectively, which limited the power for survival analysis (p=0.93). Positive TgAb was associated with lower stage on univariate analysis (positive TgAb in 23.4% vs. 17.8% of stage I/II vs. III/IV patients, respectively; p=0.01), although the relationship lost significance when adjusting for age and gender (p=0.34). Perioperative TgAb was not an independent predictor of DFS (hazard ratio [HR]=1.12 [95%CI=0.74–1.69]) or OS (HR=0.98 [95%CI=0.56–1.72]).
Preoperative serum TSH level is associated with higher DTC stage, mediated by gross extrathyroidal extension and neck node metastases. Perioperative TgAb is not an independent predictor of DTC prognosis. Further research is required to assess whether preoperative serum TSH level predicts recurrence or mortality.
Endocrinology, Southern California Permanente Medical Group, Panorama City, CA
Thyroid Cancer Saturday Poster Clinical
Serial serum Tg+TgAb measurements are considered the cornerstone of postoperative assessment of PTC patients for disease. When present, TgAb interference limits the clinical utility of Tg IMA measurements, prompting the use of less-sensitive Tg methods and/or costlier anatomic imaging to assess disease-status. The objective of this study was to assess TgAb incidence and whether the TgAb concentration and trend relate to postoperative PTC disease status.
A 2-month sample of consecutive Kaiser-Permanente requests sent for Tg+TgAb testing by the USC laboratory was analyzed for TgAb incidence and trends (Kronus TgAb assay, functional sensitivity 0.4 kIU/L). From this cohort, 42 consecutive thyroidectomized (Tx) PTC patients [median age 45, range 18–18 yr; sex: M:F=1:2; TNM: 69% Stage I; 17% Stage III; and 14% Stage IV] without distant metastases and with≥2 years Tg+TgAb tests during LT4 suppression Rx. (TSH<0.4 mIU/L) had disease status analyzed relative to their TgAb trend.
Biochemical histories classified 64.6% patients as never TgAb positive; 22.7% currently TgAb positive and 12.7% TgAb positive at Tx, but currently TgAb negative. The majority (75%) displayed a falling (≥50%) trend (Group 1), 48% of whom became TgAb-negative within 3 years of Tx, especially when the initial TgAb concentration had been low (<10 kIU/L). About 18% maintained detectable, but stable TgAb (Group 2), and 7% displayed a rising (≥50%) TgAb trend (Group 3). Group 1 tended to have pathologic evidence of lymphocytic thyroiditis, and those Group 1 patients that became TgAb-negative had lower initial TgAb levels than those who remained TgAb-positive throughout follow-up (median 1.3 versus 12.3 kIU/L, resp.). Group 1 also had a lower recurrence rate relative to other groups. Group 2 had more persistent disease and higher TNM scores. The cause of the rising TgAb of Group 3 appeared multifactorial: surgery, recurrence of disease, and/or RAI treatment.
Postoperative TgAb trends are reflective of preoperative autoimmune status, therapeutic interventions (surgery or RAI), or recurrence of disease. Serial TgAb measurements have utility as a surrogate tumor marker for assessing disease status and guiding decisions in clinical management.
Cancérologie Cervico-Faciale, Institut Gustave Roussy, Villejuif, France
Thyroid Cancer Saturday Poster Clinical
Invasive thyroid carcinoma is rare, and the extent of surgical management is controversial. The aim of this study was to evaluate the prognostic value of microscopic resection margins.
Retrospective single-center study. Only differentiated thyroid carcinomas invading the larynx, trachea, and/or oesophagus and treated surgically with the goal of macroscopic complete resection were included. Histological subtype, resection margins, postoperative radiation therapy, and preoperative metastases were evaluated with respect to oncologic outcomes.
Forty-six patients (sex ratio 1:1, average age 57 years, range 9–9, average follow-up 4 years) were included. Tumors involved the trachea (70%), cricoid cartilage (40%), thyroid cartilage (22%), and/or oesophagus (46%). Resection was macroscopically complete in all cases, with microscopically free margins (R0) for 22 patients and microscopically close or positive margins (R1) for 24 patients. Adjuvant radiation therapy was administered to 9 R0 patients and 14 R1 patients. Five- and 10-year actuarial local control was 83% (there were no local recurrences after 5 years): 100% for R0 resections and 75% for R1 (p=0.08). Neither radiation therapy nor histopathological subtype significantly affected local control. Five-year local control was lower for patients treated for tumor recurrence (with a prior period of complete remission) versus inaugurally invasive disease (63% vs. 87%, p=0.011). The 5-year actuarial disease-specific survival was 89% (95% for R0 resections and 84% for R1 resections, p=0.5). Five- and 10-year actuarial disease-specific survival was related to preoperative distant metastases (100% and 87%, respectively, for patients M0 versus 68% and 34% for patients M1, p=0.01).
Microscopically negative resection margins (R0) were associated with a trend toward better local control, but adjuvant radiation therapy did not influence outcomes. The presence of distant metastases at the time of surgery carried a lower disease-specific survival. The functional results of extensive surgery should be weighed against the prognosis of metastatic versus nonmetastatic patients, but histopathologically clear margins should remain the goal of surgery for these tumors.
SIALOENDOSCOPY IS A GOOD TREATMENT FOR RADIODINE-INDUCED SIALOADENITIS IN THYROID CANCER PATIENTS
Thyroid Cancer Saturday Poster Clinical
Sialoadenitis is the most common adverse effect of radiodine (RI) ablation for residual thyroid tissue after total thyroidectomy for thyroid cancer. The aim of this study was to evaluate the effect of therapeutic sialoendoscopy for the treatment of radiodine-induced sialoadenitis
Thirteen patients with sialoadenitis symptoms after RI ablation for thyroid cancer were submitted to Diagnostic and Therapeutic Sialoendoscopy. The procedures were performed using a minisialoendoscope 1.1 mm in diameter, under local anesthesia with salivary papilla dilation. Irrigation with saline solution and corticosteroid infusion (hydrocortisone 100 mg) were performed in all patients. The outcomes were evaluated by the patient reports.
We performed 18 sialoendoscopies in 13 patients. All patients were women, age 20 to 55 (average 38). The most common salivary gland involved was parotid gland 61% (11/18), and submandibular 39% (7/18). In only one patient, we could not realize the examination due to failure in the papilla catheterization. The most common findings of the exam were white and pale ductal mucosa, stenosis, and mucous plug. Eleven out of 13 patients described total relief of symptoms after only one procedure. We had only minor complications after the procedure like salivary gland edema and pain.
Sialoendoscopy with ductal dilation, saline irrigation, and corticosteroid infusion is a very effective treatment for radiodine-induced sialoadenitis.
A SIMPLE METHOD OF SENTINEL LYMPH NODE BIOPSY CAN UPSTAGE 50% OF N0-DIFFERENTIATED THYROID CANCER
Thyroid Cancer Saturday Poster Clinical
The standard method to detect neck metastases for PTC is preoperative ultrasound, but it has low sensitivity for the central neck. Sentinel lymph node (SLN) biopsy is the most used method to stage the lymphatic basin in melanoma and breast cancer, and its interest for clinically N0 Papillary Thyroid Cancer (PTC) is increasing. This study aims to evaluate the effectiveness of a simple technique of SLN biopsy that avoids the use of preoperative lymphoscintigraphy to simplify the procedure, and its efficacy in adequately staging the neck in cases of PTC.
Forty patients N0 PTC were submitted to surgery, intraoperative peritumor injection of radiolabeled colloid (Fitato Tc99), and the procedure was total thyroidectomy to decrease the background radioactivity, SLN localization with gamma probe, and central neck dissection (CND). All specimens were sent to histopathological analysis.
Thirty-seven were women (92.5%), with mean age 43. Tumor size ranged from 0.4 to 3.2 cm (average 1.4). We indentified at least one SLN in 36/40 (90%), average 3/patient. In all patients, at least one SLN was located in the central neck, and 4 had SLN located in lateral neck too. In 18 (50%), SLN was positive at serial sections, and 55% of them had additional metastasis on CND. Two out of lateral SLNs were positive, one of them with no central neck metastases (skip metastases). The presence of a central SLN metastases upstaged the N0 PTC to N1a (Stage III), and a lateral metastases upstaged tumors to N1b (Stage IVA). The SLN biopsy added an average of 14 min to total operative time. The sensitivity of SLN biopsy to diagnose lymph node metastases was 94%, with 100% specificity. Only one false negative occurred (negative SLN with metastases at CND). The negative predictive value (NPV) was 94%.
SLN biopsy for PTC can be done with only intraoperative injections of radiolabeled colloid. SLN Biopsy has a great accuracy to stage the neck in N0 PTC, with 94% Sensitivity and 94% NPV. It is probably the best method to accurately stage the neck in PTC, and has the additional benefit of avoiding unnecessary neck dissections (47% of patients), and to upstage patients with occult lateral neck metastases, who would benefit from further treatment with radioiodine.
Otolaryngology, Emory University, Atlanta, GA
Thyroid Cancer Saturday Poster Clinical
Current ATA guidelines for well-differentiated thyroid cancer (DTC) advocate therapeutic neck dissection for clinically involved or FNA-proven metastatic disease and prophylactic central neck dissection for advanced tumors. Even with established guidelines, the surgical management of cervical nodes remains controversial and heterogeneous. By reviewing data reported to a large national database over a decade, we identified specific tumor characteristics and patient socioeconomic factors, which may underlie existing disparities in the extent of lymph node dissection during thyroidectomy for DTC.
Review of data from the National Cancer Database identified 127,192 patients with DTC (papillary and follicular subtypes) treated surgically from January 1998 to December 2009. The variables examined included patient age, race, gender, insurance status and education level, hospital classification, surgical volume, and size of tumor. Factors predictive of type of thyroidectomy, lymphadenectomy, and number of lymph nodes removed were identified using a multivariate log binomial model.
Thyroidectomy alone was performed in 51.1%, while 48.9% also had lymph nodes dissected. Among those with nodes removed, 55.19% had 1–1 nodes removed, and the remaining 44.81% had>3 nodes removed. Patients with tumors >1 cm were significantly more likely to have nodes removed during surgery (RR 1.2, CI 1.19–1.22) relative to tumors <1 cm. Older patients and African Americans were less likely to have any nodes removed (RR 0.75, CI 0.74–0.77 and RR 0.64, CI 0.62–0.66, respectively). Patients treated at National Cancer Institute Designated Centers were more likely (RR 1.13, CI 1.1–1.15) to have >3 lymph nodes removed, as were patients with tumors >1 cm (RR 1.25, CI 1.21–1.28). However, women (RR 0.87, CI 0.85–0.88) and African Americans (RR 0.89, CI 0.85–0.93) consistently had fewer lymph nodes removed.
The results from this study identify disparities in the surgical management of lymph nodes in DTC among several clinical and demographic factors. In spite of existing guidelines, clinician preferences as well as patient characteristics contribute to the variability in the extent of surgery for DTC.
Pathology, Chung-Ang University Hospital, Seoul, Republic of Korea
Thyroid Cancer Saturday Poster Clinical
Lymph node metastases are frequently detected at the time of diagnosis or during follow-up in cases of papillary thyroid carcinoma (PTC). However, few clinicopathological parameters have been identified as independent predictive factors for lymph node metastasis. This study evaluated the predictive ability of three histological characteristics of PTC in lymph node metastases: hobnail features, loss of cohesiveness/polarity (LOCP), and micropapillary structures. These three characteristics were evaluated in addition to other clinicopathological parameters, which have been studied as predictors for lymph node metastasis.
Tissue specimens from 153 patients with histologically confirmed PTC, including 112 cases of papillary thyroid microcarcinoma (PTMC), were enrolled in this study. Three histological characteristics (hobnail features, LOCP, and micropapillary structures) and several clinicopathological parameters were evaluated for their value in predicting lymph node metastasis.
Hobnail features, LOCP, and micropapillary structures were each significantly associated with and found to be independent predictive factors for lymph node metastasis (p<0.05). These three histological characteristics were closely correlated with one another (p<0.001). Six of the seven possible combinations of these three histological characteristics were independently correlated with lymph node metastasis (p<0.05). Among these combinations, the coincidence of all three histological parameters represented the strongest independent predictive factor for lymph node metastasis (OR: 3.270, p=0.006). Among other clinicopathological parameters, infiltrating tumor growth was also found to be a powerful independent predictive factor for lymph node metastasis.
Our study demonstrates that hobnail features, LOCP, and micropapillary structures, either alone or in combinations, represent strong independent predictive factors for lymph node metastasis in PTC.
Unit of Internal Medicine and Endocrinology, Fondazione S. Maugeri, University of Pavia, Pavia, Italy
Thyroid Cancer Saturday Poster Clinical
Estrogen (ER) and androgen (AR) receptors may be expressed in thyroid tumors. In a recent study (Magri F. et al., Endocrine Related Cancer 2012), we found that ER-alpha positivity, ER-beta negativity, and AR expression are associated with a more aggressive phenotype of T1-differentiated thyroid cancers. The aim was to investigate the relationship between ERs and AR expression and tumor phenotype in T1, T2, T3, and T4 cancers.
One hundred twenty-seven patients (109 females and 18 males) bearing differentiated thyroid cancers (91 T1; 18 T2; 11 T3; 7 T4; 38 of the T1 being incidental). ER-alpha, ER-beta and AR expression in tumors and in correspondent extratumor parenchyma was evaluated by immunohistochemistry.
ER-alpha was expressed mainly in T2 (44.4%), and more rarely in T1 (15.4%), T3 (18.2%) and T4 (28.5%) tumors. AR expression was similar in T1 (20.9%), T2 (27.8%), and T3 (27.2%) tumors, but absent in T4 cancers. ER-beta was the more represented one (52.7% of T1, 64.1% of T2, 54.5% of T3, and 57.1% of T4). Compared with healthy parenchyma, tumors tended to gain ER-alpha and AR expression and to lose ER-beta expression. In T1 tumors, ER-alpha expression was more common in non- cancers (p=0.037); in T2 tumors, ER-alpha expression was associated with capsular invasion (p<0.0001). ER-beta expression was negatively associated with vascular invasion, and AR expression was positively associated with capsular invasion in both T1 and T2 tumors (p=0.005 and 0.014 in T1; p=0.015 and 0.047 in T2, respectively). No significant results emerged in the T3 and T4 subgroups.
ER-alpha positivity, ER-beta negativity, and AR expression are associated with a more aggressive phenotype in T1 and T2 thyroid cancers. This association weakens in T3 an T4 tumors, suggesting a role for ERs and AR in the early stages of tumorigenesis that becomes marginal in the more advanced stages of thyroid cancer.
Service de Médecine Nucléaire, Hôpital Pitié-Salpêtrière, Paris, France
Thyroid Cancer Saturday Poster Clinical
To evaluate the value of postoperative cervical ultrasound (POCUS) for predicting local recurrences (LR) in differentiated thyroid cancer (DTC) patients with initial lymph node metastases (N1).
We retrospectively analysed data of 659 N1-DTC patients treated by surgery and radioiodine therapy in our institution from 1997 to 2010. The survival without LR was estimated with the method of Kaplan-Meier, and the prognostic value of POCUS was studied in univariate and multivariate Cox model-based analyses.
One hundred thirty-six patients presented with an LR (20.6%). Among these patients, LR occurred during the first year and within 3 years in 42% and 83% of cases, respectively. Sensitivity of POCUS in detecting precocious LR occurring during the first year was 86.1%. During the first year of follow-up, 37% of the patients with abnormal POCUS were reoperated. An abnormal POCUS result, an elevation of stimulated thyroglobulin level, and a cervical uptake outside the thyroid bed on postradioiodine therapeutic whole-body scan (WBS) were significantly associated with LR (p<0.0001). In a multivariate analysis, only an abnormal POCUS result and an elevated stimulated thyroglobulin level were predictive of LR (p<0.0001).
The POCUS procedure is useful to detect persistent disease and precocious LR in N1-DTC patients who are classified as moderate- and high-risk DTC groups. It is a strong and independent predictor of the LR risk. POCUS is helpful for individual risk stratification. Prospective randomized studies are needed to confirm the impact of the POCUS procedure on the decision of reintervention.
EXPRESSION OF CYCLIN D1, CYTOKERATIN 7, CYTOKERATIN 20, AND VIMENTIN IN PAPILLARY THYROID CANCER AND RELATIONSHIP WITH PATIENT'S PROGNOSTIC FACTORS
Thyroid Cancer Saturday Poster Clinical
Cyclin D1, cytokeratin (CK)7, CK20, and vimentin play a important role in tumorigenesis and tumor progression. Our aim was to investigate expression of cyclin D1, CK 7, CK 20, and vimentin in 138 papillary thyroid cancer and relationship with clinicobiological factors. Also, we tried to evaluate the value of those as prognostic factors.
We performed immunohistochemical assay for cyclin D1, CK7, CK20, and vimentin in 138 papillary thyroid cancer tissue specimens. The correlation between these factors and the clinicobiological parameters was analyzed.
In 138 papillary thyroid carcinoma specimens, the expression of cyclin D1, CK7, CK20, and vimentin was seen in 118 cases (85.5%), 133 cases (96.4%), 2 cases (1.4%), and 119 cases (86.2%), respectively. In our cases, there was a significant association among the expression of cyclin D1, gender, and lymph node metastasis. However, no obvious correlation was found between those proteins, age, tumor size and number, the lymph node status, and the TNM stage.
Our results suggested increased cyclin D1 expression was seen in female gender, and cyclin D1 may be a useful marker for evaluating lymph node metastasis. However, the clinical utility of cyclin D1, CK7, CK20, and vimentin in thyroid cancer patients has to be further defined by prospective studies with larger sample sizes.
Radiology&nuclear medicine department, King Abdulla Medical City, Mecca, Saudi Arabia
Thyroid Cancer Saturday Poster Clinical
Ablation outcome in patients with papillary thyroid cancer after a single dose of 131I depends on several factors. No single group has achieved a successful complete ablation rate of 100%, and a second ablation dose is needed for patients with residual functioning thyroid tissue. The aim of the current study was to assess successful complete ablation rate after second ablation dose of 30 mCi 131I.
One hundred patients with papillary thyroid cancer (T1 or T2-N0 and M0) candidates for post-total thyroidectomy ablation received first ablation dose of 100 mCi. Six months later, a follow-up 131I whole-body scan (131I WBS) was performed. Patients with residual functioning thyroid tissue in the neck received another ablation dose of 30 mCi 131I on out-patient basis in the same day of scanning. Follow-up 131IWBS was performed 6 months later to assess for ablation outcome whether complete or incomplete.
Ninety-one percent of patients are women with an overall age range of 17–17 years. Successful complete ablation after first 100-mCi 131I ablation dose is 64%. Successful complete ablation rate in the remaining 36 patients after 30 mCi 131I is reported in 26 patients (72%). No significant difference as regard age, gender, and histopathological details (size of primary lesion, capsular or vascular invasion, and histopathology of non-neoplastic thyroid tissue) between patients who achieved complete ablation and those with noncomplete ablation after reablation dose of 30 mCi can be detected. The overall successful complete ablation rate after 2 doses of 131I (overall dose of 130 mCi) is 90%.
The successful complete ablation rate after a second ablation dose of 30-mCi 131I is 72%. No significant difference between completely and noncompletely ablated patients after the second ablation dose as regard age, gender, and histopathological details. The successful complete ablation rate after 30-mCi 131I reablation dose (72%) is higher than the rate of complete ablation after 100-mCi first ablation dose (64%), and the difference is insignificant (p value>0.01). The overall successful complete ablation rate after both ablation doses (130 mCi) is 90%.
Unite Thyroide, CLCC Godinot, Reims, France
Thyroid Cancer Saturday Poster Clinical
Thyroid carcinomas (TC) are rare; the incidence in the French Marne-Ardennnes thyroid registry is 10/100.000 in 2010. The 10-year survival rate is >90%. Nevertheless, some TC are refractory to conventional therapy. The aim of the study was to describe the frequency and clinical features of refractory TC (RTC).
Retrospective study from the cases of the database of the registry diagnosed between 01/01/1983 and 31/12/2005. RTC included metastatic differentiated TC (DTC) refractory to radioiodine therapy, metastatic or locally advanced medullary TC (MTC), anaplastic TC (ATC). We used AJCC, 6th edition. All DTC samples were reviewed by the same pathologist according to the WHO Classification 2004.
Ninety-three cases of RTC/1427 cases of TC (6,5%). 34 DTC: 2.5% of all DTC; 23 women, 11 men, mean age at diagnosis 63.5 years, mean tumor size 52.5 mm, 24/34 (82.3%) stage IV at diagnosis. Refractory characteristics appeared 40.8 months after the DTC diagnosis, and the mean survival was 7.8 years. Approximately 23.5% were papillary (2/18 papillary NOS, 1/18 follicular variant, 4/18 diffuse sclerosing, and 1/18 columnar cell carcinoma); 53% were follicular (1/18 minimally invasive; 5/18 widely invasive; and 12/18 oxyphilic cell type); and 23.5% insular (8/34), 13 MTC: 15.4% of all MTC; 6 women, 7 men, and the mean age at diagnosis was 60.4 years. Eleven out of 19 sporadic and 1 familial case, mean tumor size 34 mm. All were stage IV at diagnosis. Mean survival was 6.2; 46 ATC: 33 women, 13 men, mean age at diagnosis 72.6 years, and the mean tumor size was 73.7 mm, Sixteen out of 46 M1 at diagnosis. Mean survival was 7 months.
In this retrospective study, 6.5% of all patients with TC are refractory: 37% DTC, 14% MTC, and 49% ATC. Most of the DTC and MTC were diagnosed refractory within the first five years following the TC diagnosis, but some after more than 10 years. Most of the patients had aggressive features. Nevertheless, 5 patients with DTC were classified stage I or stage II.
Registre Thyroide, CLCC Institut Jean Godinot, Reims, France
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer (TC) incidence is increasing throughout the world. Some researchers have suggested that this rise is only apparent due to an increase in diagnostic activity. The Marne and Ardennes thyroid cancer registry is the only cancer registry in France, which focuses on thyroid cancer. It has been collecting comprehensive population-based data since 1975. The aim of this study was to describe clinical features and the evolution of the incidence of TC in Marne and Ardennes from 1975 to 2008.
Data on thyroid cancers were provided over a period of 34 years by the Marne and Ardennes TC registry. The period of diagnosis was split into intervals of 5 years, except for the last period (4 years). The incidence rates were standardized to the world population and were given according to sex, period of diagnosis, stage (using AJCC/UICC staging 6th edition), tumor size in mm, and histological subtype.
One thousand nine hundred fifty-two patients were registered in the Marne and Ardennes registry from 1975 to 2008. Among them, 440 were men and 1512 women (sex ratio: 0.29). The mean ages at diagnosis were 49 in women and 51 in men. Less than 2% of cases were children and adolescents. Between the 2 periods 1975–1975 and 2005–2005, the incidence for 100,000 person-year rose as follows: for all TC from 1.0 to 5.9 in men and from 4.2 to 16.2 in women, for pT1 from 0.87 to 7.67, and for small tumors (≤5 mm) from 0.1 to 3.7 and for papillary thyroid cancers (PTC) from 1.2 to 9.4. Between the 2 periods 1975–1975 and 2005–2005, the frequency of TC discovered incidentally by histologic examination rose from 12% to 49%. In the last period 2005–2005, among the TC discovered incidentally, 69% were ≤5 mm, 86% were ≤10 mm, and 93% were PTC.
Our results showed that the rise of the incidence of TC from 1975 to 2008 is in part due to an increase of incidental histologic diagnosis of small PTC.
Surgery, Farwaniya Hospital, Al Ardiya, Kuwait
Thyroid Cancer Saturday Poster Clinical
Thyroid surgery is quite prevalent in Kuwait Hospitals. Despite advances in surgical techniques, this surgery continues to be associated with complications, such as parathyroid resection and recurrent laryngeal nerve injury. This study aimed at (1) determining the incidence of incidental parathyroidectomy during thyroid surgery; and (2) identifying the predictive risk factors for incidental parathyroid resection.
The electronic files of Department of Pathology, Farwaniya Hospital, were screened for thyroidectomy procedures for the last eight years, from 2003 onward to 2011. The pathology reports were reviewed for age, gender, underlying thyroid pathology, and type of thyroid surgery. In addition, the reports were also carefully examined for presence of incidental parathyroid resection, number of parathyroid, and the presence of parathyroid pathology. The statistical analysis was carried out using SPSS V.19.0 computer software; (n=314) thyroidectomy procedures were identified, which included 241 (76.8%) female patients. Of these, 61 (19.4%) procedures were Incidental parathyroid resections cases, with mean age as 38.6 (±10.1 SD) years, and an M:F ratio as 1:6.6. All resection parathyroids were normal, except one case of adenoma. Logistic regression analysis revealed female gender and underlying thyroid malignancy to be the statistically significant risk factors for parathyroidectomy (p=0.017, OR=2.7) and (p=0.001, OR=3.3), respectively. Age and type of thyroid surgery were not the risk factors for incidental parathyroidectomy, though higher proportions of total thyroidectomy were found (55.7% vs. 42.1%) among incidental parathyroid than any other thyroidectomy cases.
Incidental parathyroid resection during thyroid surgery is not uncommon (19.4%) and is comparable to published data in the literature. Female gender and thyroid malignancy were found to be the risk factors associated with unintentional parathyroid resection. Awareness of these factors among surgeons may avoid unnecessary parathyroid resection.
RENAL RETENTION OF RADIOACTIVE IODINE MASQUERADING AS A SOLITARY HEPATIC METASTASIS ON WHOLE-BODY SCAN
Thyroid Cancer Saturday Poster Clinical
Radioactive iodine (RAI) plays a major role in the management of high-risk thyroid cancer. High dose (>100 mCi) post-therapy 131I whole-body scans (WBS) may detect new lesions in up to 50% of cases with a significant proportion of the newly found lesions being unsuspected distant metastases. While postablation 131I WBS may show uptake outside the thyroid bed, interpretive pitfalls may occur due to infrequently encountered physiological variants, which can be confused with metastasis. We present a case of renal retention of RAI mimicking a solitary hepatic metastasis.
Case report: A 76-yo woman with stage III papillary thyroid cancer (T3N0Mx) was found to have multifocal disease with extrathyroidal extension invading skeletal muscle. She received 163 mCu of 131I after thyroid hormone withdrawal (thyroid-stimulating hormone 148 μIU/mL and thyroglobulin level 1.3 ng/mL). Post-RAI WBS showed neck uptake consistent with remnant thyroid and intense uptake over the liver worrisome for solitary hepatic metastasis. Liver function tests and hepatic ultrasound were normal. Ultrasound however suggested dilation of the right renal collecting system and a right extrarenal pelvis. Subsequent PET-CAT scan did not show abnormal FDG-PET accumulation over either the liver or kidney, however, did suggest calyceal dilatation of the right renal pelvis. A second renal ultrasound performed 11 months later documented a stably dilated right renal pelvis.
Correct interpretation of RAI WBS is critical to appropriate thyroid cancer management. In our case, a dilated renal pelvis with delayed retention of RAI led to misinterpretation as a hepatic metastasis. A clinical clue to this was that the thyroglobulin level was lower than usually seen in liver metastasis; also, renal uptake would be more clearly seen on posterior views and should clear on delayed imaging with further hydration. Renal retention causing false-positive WBS imaging in differentiated thyroid cancer is better recognized by the Nuclear medicine than the Endocrine community. Bakheet et al. 1996 noted renal-bed RAI uptake in 2.2% of cases. Appropriate recognition of variants of renal anatomy is crucial to prevent misinterpretation of WBS and inappropriate treatment with RAI.
FOLLICULAR THYROID MICROCARCINOMA PRESENTING AS A THORACIC MASS
Thyroid Cancer Saturday Poster Clinical
Thyroid cancer is the most common endocrine malignancy, and over 90% are well-differentiated papillary and follicular histological subtypes. Although it usually metastasizes to the lung or bone, distant metastasis to muscle and spine are rare.
We describe a patient with an enlarged right thoracic mass as an initial presentation of follicular thyroid microcarcinoma.
A 70-year-old woman was evaluated at an outside hospital for a right thoracic mass. An initial CT thorax revealed a 9.3×4.7×5.4-cm heterogeneous mass extending from the right 8th and 9th thoracic spinal foramen involving the right 9th rib and vertebral body. She declined a biopsy and had carried a presumed diagnosis of schwannoma. Patient returned 1 year later, as the mass had enlarged and caused severe pain. An MRI of thoracic spine demonstrated a similar finding with a soft tissue enhancement surrounding the thoracic spinal cord causing central canal stenosis. No signal abnormality was seen in the thoracic cord. A CT-guided biopsy of the mass revealed metastatic follicular thyroid carcinoma with positive immunostaining for thyroid transcription factor-1 (TTF-1) and negative staining for chromogranin, S-100 protein, and synaptophysin. She underwent a two-stage right thoracotomy and 7th-10th spinal laminectomy with transpedicular resection of vertebral and paravertebral tumor. A preoperative serum thyroglobulin level (Tg) was 24,138 ng/mL with negative thyroglobulin antibodies. The histopathology confirmed metastatic follicular carcinoma of thyroid origin. A total thyroidectomy was performed and revealed a 1.0×0.7×0.7-cm unifocal follicular microcarcinoma with capsular and vascular invasion limited to thyroid gland. One regional lymph node was negative for cancer. Papillary thyroid microcarcinoma 0.3 cm was also found. A postoperative Tg was 1,781 ng/mL. Following administration of 208 mCi of 131I, a metastatic survey showed a large iodine-avid lesion involving multiple levels of mid-thoracic spine, left ileum, and right posterior costophrenic angle.
To our knowledge, this is the first case report of skeletal and spinal metastasis from follicular thyroid microcarcinoma.
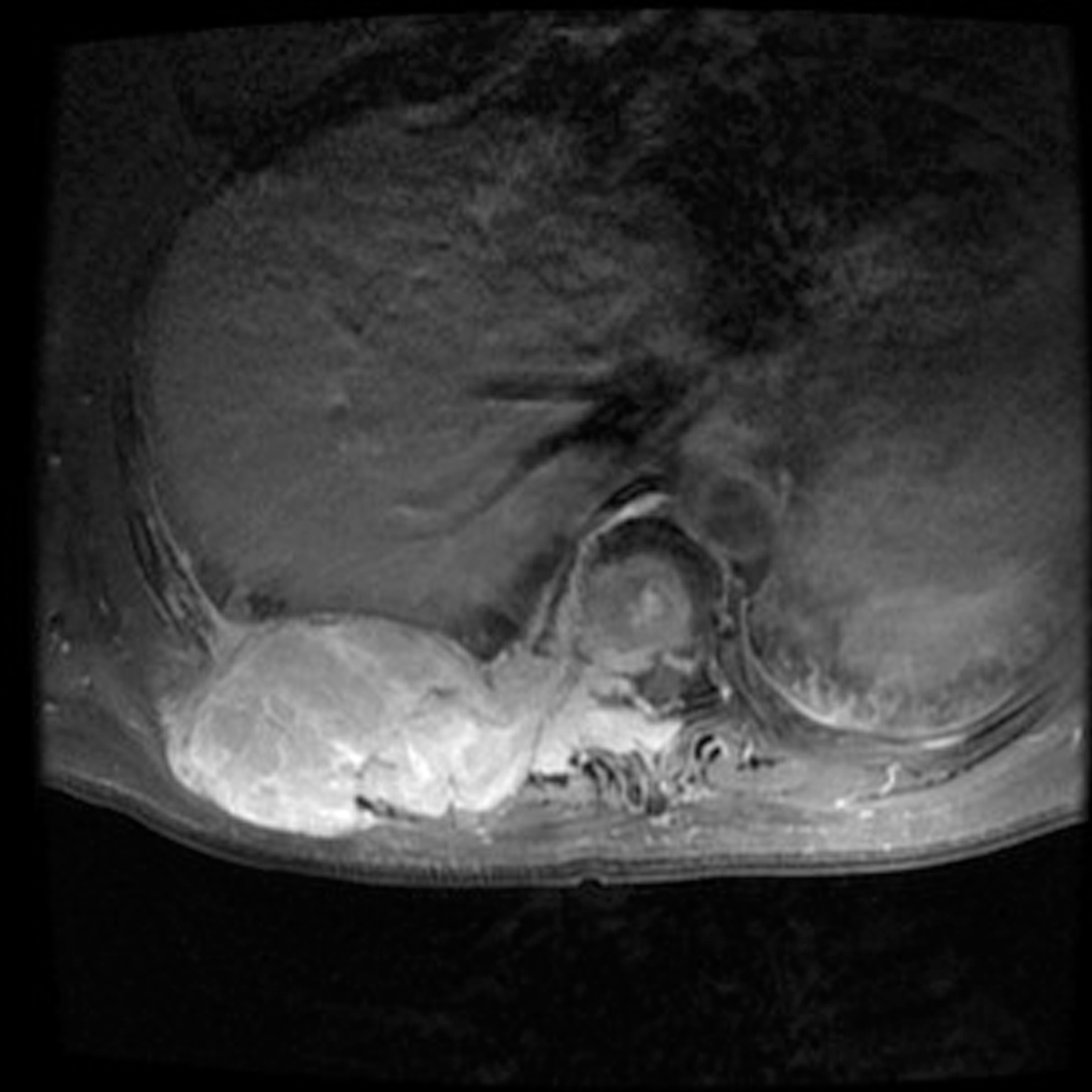
An MRI demonstrates a heterogeneous soft tissue enhancement extending from the 8th and 9th thoracic spine invading the 9th rib and surrounding the thoracic spinal cord at the same level.
Thyroid Cancer Saturday Poster Clinical
A very rare case of papillary thyroid carcinoma is presented who is suffering from unilateral Graves' ophthalmopathy after treatments with total thyroidectomy and after radioiodine-131 (131I) administration.
A 26-year-old woman underwent total thyroidectomy with neck dissection for papillary carcinoma of pT3, pEx1, and pN1a (according to UICC classification) in October 2010. She clinically had no distant metastases, and has been treated with TSH suppression dose of levothyroxine. In June 2011, she received an ablative dose of 131I (3.7 GBq) after levothyroxine withdrawal, and subsequent whole-body images revealed tracer uptake in the thyroid bed and near the trachea. At initial visit in July 2010, she was in euthyroid state with suppression of TSH, and had negative autoantibodies for thyroglobulin, thyroperoxidase, and thyrotropin (TSH) receptor. Re-evaluation of TSH concentration showed normal value.
She complained of eye discomfort, and presented the left upper eyelid retraction in November 2011. Her eyes measured 18 mm with a Hertel exophthalmometer. Orbital magnetic resonance imaging was normal; however, TSH receptor antibody (TRAb) appeared as 1.2 IU/L (reference range, < 1.0 IU/L), and thyroid-stimulating antibody (TSAb) increased to 326% (reference range, <180%).
In patients with thyroid cancer, Graves' ophthalmopathy may develop from radiation-induced thyroid injury with appearance of thyroid-stimulating immunoglobulin in the serum.
Laboratory of Comparative Endocrinology, KU Leuven, Leuven, Belgium
Thyroid Development Saturday Poster Basic
It is known that antithyroid drugs such as methimazole (MMI) and propylthiouracil cross the mammalian placenta and may have adverse effects on fetal development. A similar problem occurs in birds where MMI is deposited into the egg and taken up by the developing embryo.
Laying hens were treated with MMI (0.03% in the drinking water). We measured total and reduced MMI content as well as thyroxine (T4) and 3,5,3′-triiodothyronine (T3) availability in hens, eggs, and embryos at different stages of development, before and after the start of embryonic thyroid gland activity.
Following 16 weeks of treatment, circulating MMI levels in hens were on average 7 μg/mL. MMI levels in thyroid (μg/g) were more than 3-fold, as high while levels in the liver and brain were lower and, respectively, 50% and 25% of the level in plasma. MMI levels in eggs collected from 8–8 weeks of treatment were double in egg white and yolk compared to maternal plasma, while levels in head and trunk of 6-day-old embryos were slightly higher (8–8 μg/g). In 14- and 18-day-old embryos, MMI levels in brain and liver were lower (4–4 μg/g), slightly above levels in the adult liver. Maternal treatment reduced T4 content in egg yolk to 30% and T3 content to 50% of control values. In 6-day-old embryos, T3 and T4 levels in the trunk were not affected, but the T3 level in the head was strongly decreased. In 14- and 18-day-old embryos, plasma T4 and T3 were decreased, while hormone content in most tissues was not affected. However, T3 availability was clearly decreased in the brain at both stages.
We conclude that the brain of early embryos is exposed to relatively high doses of MMI compared to older embryonic stages and certainly compared to the adult brain. The effect of maternal MMI treatment on embryonic thyroid hormone availability is most pronounced for brain T3, which is reduced throughout embryonic development.
USING A MOUSE MODEL OF LOCAL HYPERTHYROIDISM TO DISSECT THE ROLE OF THYROID HORMONE IN THE REGULATION OF ENERGY EXPENDITURE
Thyroid Hormone Action Saturday Poster Basic
Thyroid hormone (TH) regulates basal metabolic rate and adaptive thermogenesis in mammals. Nuclear receptor corepressor NCoR is essential for TH signaling as one of the key cofactors for thyroid hormone receptors (TRs). By generating a mouse line that can conditionally express a modified NCoR protein (NCoRΔID) that is unable to interact with TRs, we have demonstrated that NCoR attenuates activation of positive TR target genes. Thus, animals that express NCoRΔID in a certain tissue may serve as a model of tissue-specific hyperthyroidism. Mice that express NCoRΔID globally demonstrate elevated energy expenditure (EE) due to enhanced peripheral TH signaling. The goal of our study was to identify the mechanisms of increased EE in NCoRΔID mice with a potential to use tissue-specific NCoRΔID models to further elucidate the role of TH in control of energy metabolism.
Male NCoRΔID mice and their wild-type (WT) littermates were studied at 14–14 weeks of age (n=–8). RNA isolation and quantification of expression by qPCR were performed using standard techniques.
Adaptive thermogenesis in NCoRΔID was assessed by cold exposure (4°C) for 72 h. NCoRΔID animals demonstrated improved ability to defend their body temperature accompanied by significant weight loss and no change in food intake compared to the WT, suggesting increased EE. Analysis of mRNA expression in brown adipose tissue (BAT) at the end of the 72-h period showed no significant differences in the expression of thermogenic markers such as Ucp-1, Pgc-1α, Dio2, Gmpr, and lipogenic enzymes between the genotypes. These results suggest that NCoRΔID mice have normal BAT-mediated thermogenesis. When housed at thermoneutrality (30°C) to block adaptive thermogenesis NCoRΔID animals showed increased food intake and body temperature with no changes in body weight compared to WT indicative of increased EE. No increase in expression of thermogenic markers in BAT was detected, suggesting that activation of BAT was not responsible for the changes in EE.
Disruption of NCoR-TR interactions leads to elevated EE due to an increase in basal metabolic rate. Further studies using tissue-specific NCoRΔID mutants will identify the specific tissues/pathways responsible for this phenotype.
THE EFFECTS OF THYROID HORMONES ON PROSTATE PHYSIOPATHOLOGY
Thyroid Hormone Action Saturday Poster Basic
Triiodothyronine (T3) and the sympathetic input play crucial roles in normal and tumoral development of tissues. The prostate of pubescent and sexually active adult rats expresses high activity of type 1 deiodinase (D1). This enzyme is stimulated by the sympathetic input, and its activity is involved in local generation of T3 (Biol Reprod 84: 118, 2011). In prostate cancer, D1 expression is low in human cells (unpublished data), and it is known that β-adrenergic hyperactivity promotes invasion and metastasis (neuroendocrine [NE] phenotype). Type 3 deiodinase or D3 (inactivating pathway of thyronines) is present in different types of neoplasia, but its expression has not been analyzed in prostate cancer. We propose that progression of prostate cancer will be accompanied by inverse changes of deiodinase expression (D1 decrease and D3 increase), and T3 supplementation could prevent tumor progression. The aims of this study were 1) to analyze D1 and D3 expression in cancerous prostate of TRAMP mice, and 2) to evaluate the effects of T3 (2.5 μg/day) alone or in addition to the β-adrenergic agonist isoproterenol (ISO, 200 μg/pellet) on athymic mice inoculated with human prostate cancer cells (LNCaP).
Gene expression was analyzed by qRT-PCR.
TRAMP mice expressed high levels of D1 and prostatic T3 at 8 weeks of age, but both declined at 13 (intraepithelial neoplasia) and 30 weeks of age (cancer). In contrast, the highest levels of prostate D3 expression were found in 30-week-old TRAMP mice. In athymic mice, T3 administration did not modify tumor growth, but it prevented the increase of gene expression induced by ISO (VEGF, uPA, MMP-9, and cromogranin A). Moreover, 10 nM T3 reduced the acquisition of the NE phenotype by LNCaP cells treated with 50 μM ISO.
These data suggest that local T3 generation could prevent the invasive potential associated with β-adrenergic hyperactivity. We thank Guadalupe Delgado, Martνn Garcνa, and Felipe Ortiz for their technical assistance. Supported by CONACYT (127368 and 78955), PAPIIT (IN201210).
Endocrinology, Cesar Milstein Hospital, Buenos Aires, Argentina
Thyroid Hormone Action Saturday Poster Clinical
A worse lipid profile in relation to lower thyroid function and insulin resistance has been previously reported both in diabetics and nondiabetics. However, this interaction has never been yet explored in the elderly, in whom both thyroid dysfunction and metabolic disturbances are quite prevalent. Our aim was to study the impact of thyroid function on lipid metabolism in elderly patients with MS.
Seventy-seven patients above 65 years with MS were recruited in our Endocrine Unit. TSH and free-T4 serum levels were determined together with several metabolic and anthropometric parameters. Only those patients with TSH levels 0.3–3 mU/L and normal free-T4 levels (0.7–1.8 ng/dL) were included. A cutoff level above 3.5 of the TG/HDL-c ratio was used as a predictor of insulin resistance. Lineal correlation, Student t-test and ANOVA were used for statistical analysis.
Spearman correlation between TSH and total-chol and LDL-chol was significant (r=0.375, p=0.001 and r: 0.372, p=0.001 respectively). When TSH levels were divided into > or <2.5 mU/L, total-chol and LDL-chol values were found significantly higher in the elevated TSH group (209±48 vs. 177±46 mg/dL, p=0.003 and 134±40 vs. 108±35 mg/dL, p=0.003, respectively). The interaction term between TSH>2.5 and TG/HDL-c ratio>3.5 was also significantly associated with higher total-chol and LDL-cholesterol levels (p=0.008 and 0.026). Moreover, when TG/HDL-c ratio >3.5 was present, the difference between total-chol in patients with TSH> or <2.5 mU/L was further increased (212±52 vs. 158±32 mg/dL, respectively, p<0.001).
In elderly patients with MS, lower thyroid function is associated with higher cholesterol levels. This relationship is amplified by high TG/HDL-c ratio, a parameter related to insulin resistance.
DIFFERENT STIMULI INCREASE DEIODINASE TYPE 2 MRNA EXPRESSION IN A MURINE MACROPHAGE CELL LINE
Thyroid Hormone Metabolism & Regulation Saturday Poster Basic
Previously we showed that type 2 deiodinase (D2) is upregulated in the liver during chronic and acute illness in association with the inflammatory response. Preliminary data suggested liver macrophages to be the source of D2. The aim of this study was to evaluate the mechanisms involved in the illness-induced D2 increase using a murine macrophage cell line. To this end, we also studied the effect of pioglitazone, a PPARγ agonist involved in bacterial clearance.
RAW264.7 cells were stimulated with LPS (1–1 ng/mL), cycloheximide (10 μg/mL) (to inhibit protein synthesis), or pioglitazone (5 μM and 10 μM). Specific inhibition of inflammatory pathways was attempted using siRNAs transfected with lipofectamine or electroporation. IFNβ, as a marker of cellular activation, and D2 mRNA were measured using qPCR and corrected to an appropriate housekeeping gene.
D2 mRNA was upregulated in RAW cells after 3h of stimulation with LPS in a dose dependent manner. Surprisingly, cycloheximide treatment of the cells without LPS also increased D2 mRNA expression. Furthermore, transfection of control siRNA using lipofectamine as a transfection agent increased D2 expression, but electroporation of control siRNA did not induce D2 mRNA expression. Pioglitazone (10 μM) also increased D2 mRNA expression after 4 and 8 h. Increased D2 expression was consistently accompanied by an increase of IFNβ mRNA expression.
A variety of stimuli, leading to an increase of IFNβ mRNA, are able to increase D2 mRNA in macrophages. Our results suggest that D2 expression in macrophages is associated with the innate immune response. It may modulate T3-regulated gene expression during the cellular response to inflammation or stress. Further experiments are needed to determine the signal transduction pathways involved in D2 induction as a result of cellular stress.
Institut für Experimentelle Endokrinologie, Charité-Universitätsmedizin Berlin, Berlin, Germany
Thyroid Hormone Metabolism & Regulation Saturday Poster Basic
An atypical form of resistance to thyroid hormone (RTH) leads to a rare human disease, characterized by retarded growth and bone age. Aberrant thyroid hormone levels (high T4, low T3, elevated rT3, and high-to-normal TSH) indicate a defect in deiodinase-dependent thyroid hormone metabolism. Findings of reduced concentrations of plasma selenoproteins suggested a generalized defect of selenoprotein biosynthesis and led to the identification of mutations in the SECISBP2 gene. SECISBP2 is thought to play an essential role for selenoprotein biosynthesis. Mutations in the SECISBP2 gene lead to reduced expression of selenoproteins and cause a syndrome with relatively mild to more severe phenotypes.
Our group set out to create mouse models to test whether Secisbp2 is essential for selenoprotein biosynthesis and to study the consequences of Secisbp2 deletion in tissues and the whole organism.
First results showed the essentiality of Secisbp2: a constitutional knockout leads to early embryonic lethality. Nevertheless, Secisbp2 heterozygotes have no obvious phenotype. They are fertile, and their thyroid function tests are normal. Biochemical analysis revealed only minimal changes in selenoprotein expression. Hepatocyte-specific Secisbp2 knockout mice appear normal too, but show a dramatic reduction of hepatic selenoprotein expression. Neuron-specific Secisbp2 knockout mice have a more severe phenotype and survive for approximately three weeks. They are smaller and weigh less than their wild-type littermates. They exhibited a marked movement phenotype with an awkward, broad based, and dystonic gait. Immunohistochemical stainings demonstrated a specific loss of parvalbumin-positive interneurons in somatosensory cortex and hippocampus.
We compared our Secisbp2 mice with similar mouse models lacking tRNA[Ser]Sec. Interestingly, the phenotypes, as well as the consequences on selenoprotein level, of our Secisbp2 mice are milder than in tRNA[Ser]Sec knockout mice. We will therefore also explore alternative factors that could compensate for Secisbp2 function.
Scienze Chirurgiche, Sapienza Università di Roma, Roma, Italy
Thyroid Hormone Metabolism & Regulation Saturday Poster Clinical
The literature shows that hypothyroidism can induce carpal tunnel disease by edema of peritendinous tissue. Other epidemiological studies confirmed the high incidence of hand musculoskeletal disease among people affected by thyroid disease without identifying a possible pathogenesis of the phenomena. In a previously study on a population of 7963 patients undergoing total thyroidectomy in our Department, we observed that 4.8% of patients affected by DTC referred a past surgical decompression of carpal tunnel.
In this prospective study, we evaluated the prevalence of Dupuytren's contracture, trigger finger, and carpal tunnel in a large series of patients referred to our thyroid service, with various thyroid disease and different levels of functions. We enrolled patients with euthyroid nodular diseases, toxic adenoma, Basedow disease, total thyroidectomy, hypothyroidism, and thyroiditis, and we divided this population in two groups: patients treated with L4 or L4-L3 and patient not treated. We evaluated the presence of hand musculoskeletal disease by a neurological and musculoskeletal examination after a standardized symptom questionnaire. The prevalence of hand musculoskeletal problems was analyzed with respect to thyroid function, thyroid autoantibody status, and thyroid hormonal therapy.
The aim of this preliminary study was demonstrate that the high prevalence of hand disease in patients with thyroid disease not only is related to hypothyroidism but it significantly increases also in euthyroid patients treated with thyroid hormones.
Our goal for the future is the genetic and molecular analysis of the specific cellular signaling response of peritendinous fat and peritendinous guaina to the exogenous and endogenous thyroid hormone, to identify this unknown pathogenetic mechanism.
MULTIMODALITY IMAGING IN STAGING OF THYROID CANCER
Thyroid Imaging Saturday Poster Basic
The biology and evolution of thyroid cancer are variable depending on the histology and grade of the tumor. Distant metastasis from differentiated thyroid carcinoma decreases the 10-year survival of patients by nearly 50%. We explore the advantages and limitations of several modalities used in the initial staging of a patient with metastatic thyroid cancer, including CT, MRI, iodine scans, bone scan, and 18F FDG PET scans.
A 57-year-old woman with no significant medical history presented with a vague history of left hip fullness for 4 months and a 20-lb weight loss. The PCP noted a large left gluteal mass on physical exam. The patient was also noted to have thyroid enlargement, and was subsequently diagnosed with hyperthyroidism and started on methimazole.
MRI of pelvis confirmed a 10×7-cm mass involving the left iliac bone extending into the left sacrum and involving iliacus, gluteus, and paraspinal muscles. Other bony pelvis lesions were also noted. An osteosarcoma was contemplated, and a bone scan was ordered that was negative —frequently the case in thyroid cancers. This prompted a biopsy of the gluteal mass, revealing metastatic follicular thyroid cancer (FTC). The patient had a total thyroidectomy, and a whole-body 123I scan following surgery revealed multiple skeletal lesions in the humerus, shoulders, bony pelvis, and left tibia. The patient was treated with RAI 131I therapy. A one-year follow-up 131I scan showed progression of skeletal metastases. An 18F-FDG-PET scan at the same time showed more skeletal lesions not detected on the 131I scan and vice versa. Following multiple doses of radioactive iodine treatment the patient continued to progress. Further follow-up with 18F-FDG-PET scans revealed central necrosis following treatment not easily appreciated on an MRI and iodine scan (lower contrast resolution).
The biological behavior of various clones of thyroid cancer cells was evaluated by different functional and anatomical modalities. MRI, iodine scans, and PET scans gave additive information about the patient's initial lesions and response to treatment. Thus, we conclude that multimodality imaging is of additional value in the work-up of advanced stages of thyroid cancer.
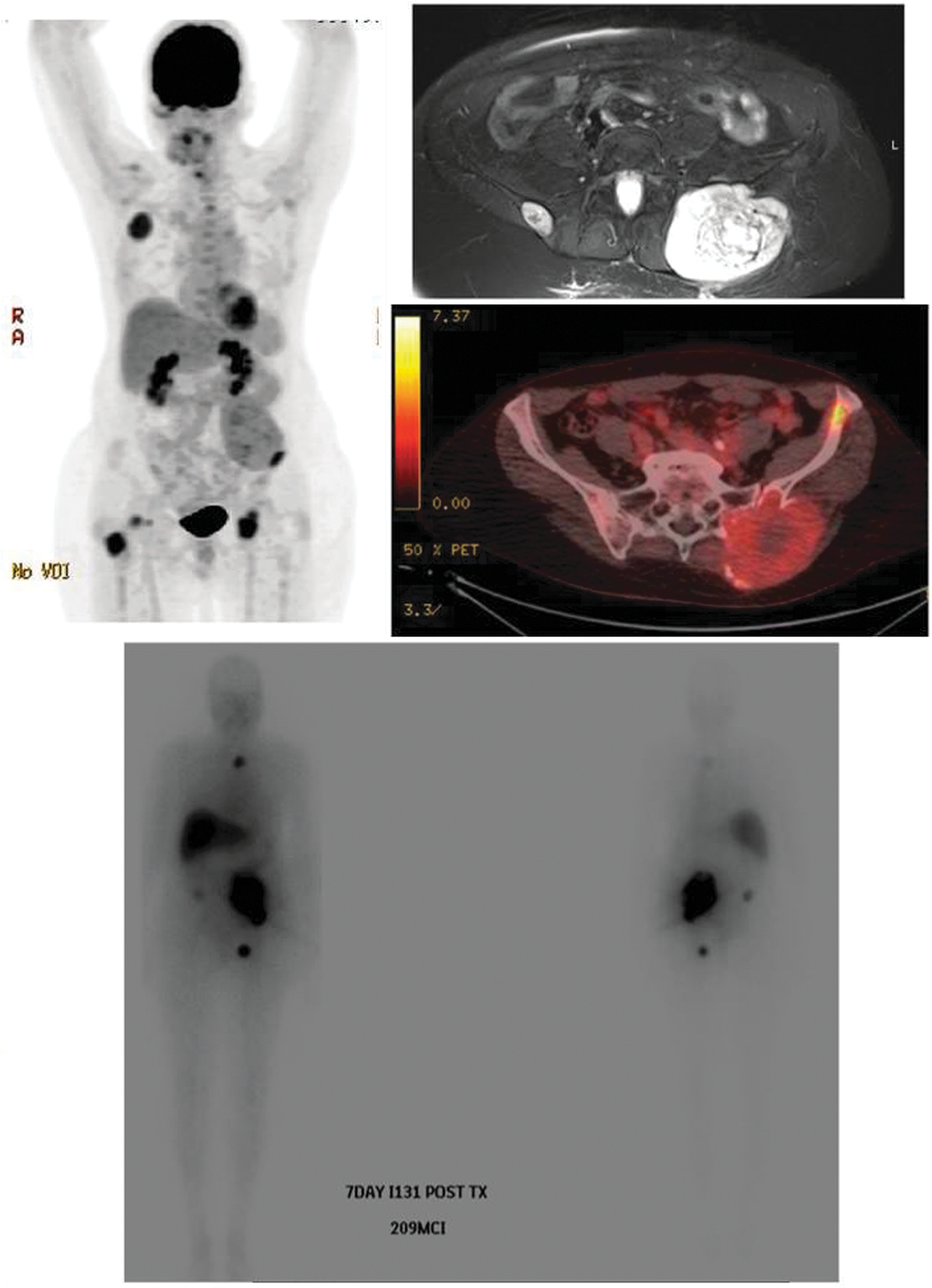
MIP images from a whole body PET scan, Cross-sectional fused FDG-PET image at the level of pelvis, pelvis MRI, and whole-body 131I scan 7 days after therapy with 209 mCi of 131I. PET images show an FDG avid mass at the left iliac bone. The iodine scan also shows a left iliac mass with iodine uptake. MRI shows a soft tissue mass at the left iliac bone involving a left iliacus, gluteus, and paraspinal muscles.
Thyroid Imaging Saturday Poster Translational
18F FDG PET is currently the preferred modality for staging and restaging of multiple cancers. It is also being extensively investigated in the assessment of response to therapy and treatment modulation. However, no reports document the utility of FDG PET in patient management modulation. Tumor grade has been correlated to Ki67 (a proliferation marker) and 18F FDG uptake. More aggressive, higher-grade tumors tend to have a higher metabolic rate—FDG uptake. In daily clinical practice, this characteristic is not routinely used, as data supporting its use have not been reported. Frequently, patients present with more than one lesion/tumoral mass and may have two and occasionally three synchronous cancers.
We describe a 41-year-old man with a history of left femoral osteosarcoma resection presenting 10 years later with a mesenteric mass, bilateral neck lymph nodes, and a multinodular goiter. A total thyroidectomy, bilateral neck dissections, and the mesenteric mass biopsy revealed a tall-cell variant left thyroid lobe nodule and left-neck lymph nodes; a classic papillary thyroid cancer in the right thyroid lobe and in right neck lymph nodes; and a spindle cell mesenteric tumor. A surveillance FDG PET scan performed before the resections were able to discriminate and predict preoperatively the different histologies and grade of tumors quantitatively.
FDG uptake was not appreciated in the right neck/right thyroid lobe. Mild uptake was noted in the mesenteric lesion. Intense uptake was noted in the tall-cell variant left thyroid lobe thyroid cancer and left neck lymph nodes with an SUVmax (standardized uptake value) of 10.8. These data were helpful in stratifying and modulating patient's management of his 3 synchronous tumors. FDG PET data drove the aggressive bilateral neck dissections. The lower grade of FDG uptake of the patient's spindle cell tumor allowed it to be followed-up conservatively, excluding an aggressive sarcomatous lesion.
Semiquantitative parameters can be helpful in modulating patient management.
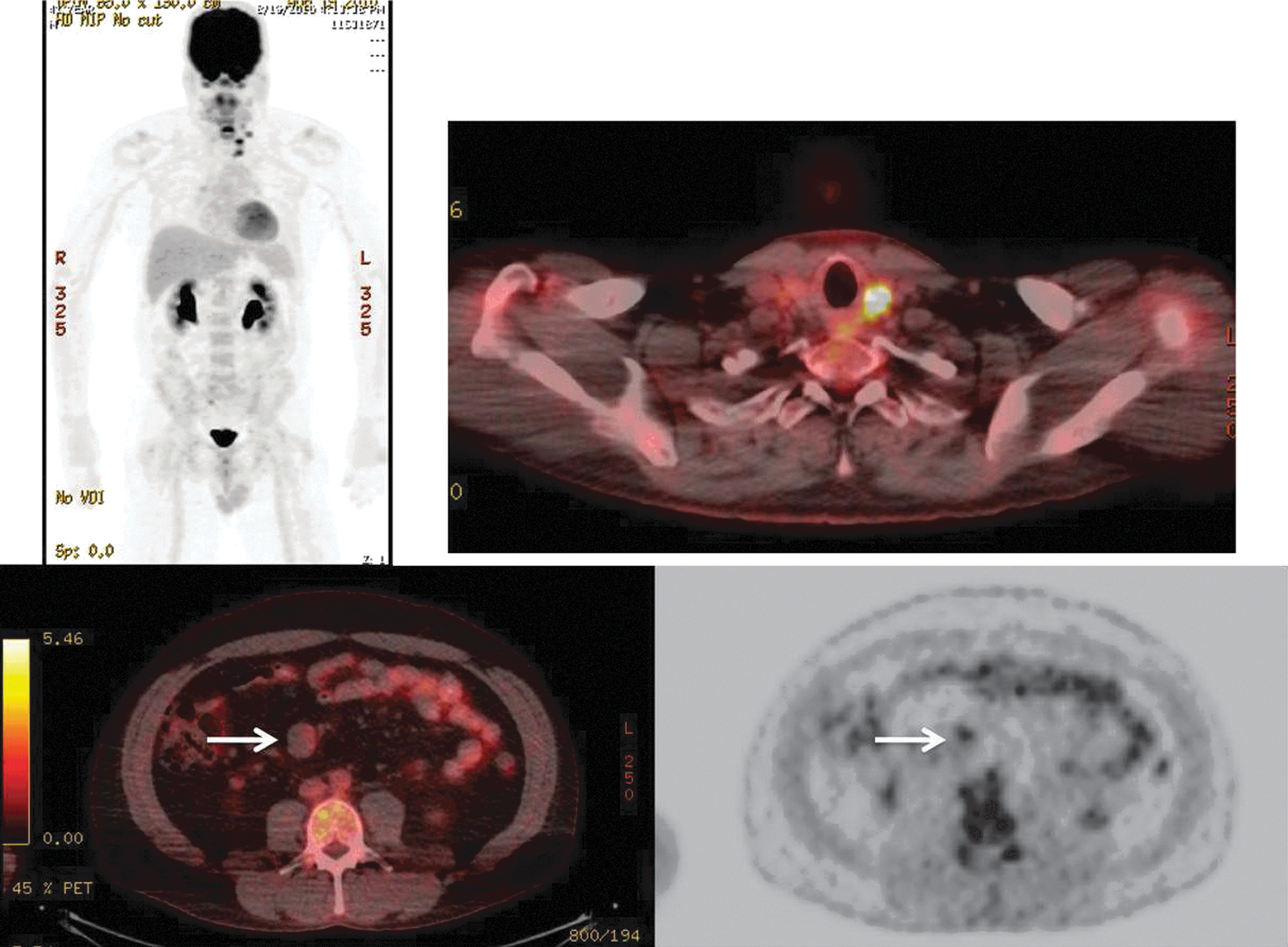
MIP image shows intensely FDG-avid left thyroid lobe and neck lymph nodes. Fused axial at level of thyroid: intensely FDG-avid left thyroid lobe. Fused axial of abdomen and PET-only images of abdomen: Mild FDG uptake in mesenteric mass (white arrow).
Thyroid Nodules & Goiter Saturday Poster Clinical
Outside of Asia, transaxillary robotic thyroidectomy is not widely conducted, partly due to apprehension in applying the technique to an obese patient population. In a large single-surgeon series of robotic thyroidectomy in the United States, we investigated its application in patients with high body-mass index (BMI).
From November 2010 to April 2012, 94 consecutive robotic transaxillary thyroidectomies were performed. Total thyroidectomy was approached from a single axillary incision; lobectomy was approached from ipsilateral incision. After IRB approval, a prospective database was retrospectively queried for data, including diagnosis, complications, and operative time. Overweight was defined as BMI>25 and obese as BMI>30. Statistical analysis was performed using ANOVA, Fisher's exact test, and Student's t-test.
The study group comprised 44/94 cases of robotic total thyroidectomy and 50/94 of robotic lobectomy. Preoperatively, 50% had normal BMI<25, 35% had BMI>25, and 15% had BMI>30 (range 17.2–40.3). There were no conversions to conventional neck incision. The major complication rate was 0% with no cases of hematoma, permanent vocal cord paresis, brachial plexopathy, or permanent hypoparathyroidism. Six out of 94 patients (6%) had temporary dysphonia, and 2/94 (2%) patients required treatment with calcitriol for postoperative hypocalcemia, but all patients had complete resolution within 6 months after surgery. Rates of temporary dysphonia and temporary hypocalcemia did not differ significantly across BMI groups (p=0.148 and 0.162, respectively). Patients with BMI<25 undergoing lobectomy had a shorter mean operative time than BMI>25 and BMI>30, but this was not statistically significant (68 vs. 74 vs. 75 min, p=0.37). Operative time for total thyroidectomy was similar across BMI cohorts (97 vs. 118 vs. 99 min).
For patients with higher BMI, robotic transaxillary thyroidectomy is a safe, feasible alternative with a low complication rate and negligible difference in operative time.
Endocrinology, University of Vermont, South Burlington, VT
Thyroid Nodules & Goiter Saturday Poster Clinical
Approximately 2% of thyroid nodules are due to metastatic disease, most often caused by renal, breast, lung, or uterine carcinomas. We report a novel case of metastatic bronchial carcinoid to the thyroid gland. Case: A 56-year-old woman with a history of metastatic bronchial carcinoid presented to the Endocrine clinic for management of new-onset diabetes mellitus. An abnormal CXR in 2005 led to resection of a 5-cm carcinoid tumor in the left lung. Regional LNs were free of disease. In 2006, CT showed new lesions in the liver and pancreas, and at her present visit in 2011, metastatic disease was noted in the liver, pancreas, bone, and retina. She had no symptoms of carcinoid syndrome.
Patient underwent a physical examination. Ultrasound, CT, and octreotide scintigraphy confirmed the presence of tumor in the thyroid.
Physical examination detected a solitary left thyroid nodule. Ultrasonography confirmed that this nodule was in the left lobe and measured 22×14×14 mm. A CT showed the new thyroid nodule, and octreotide scintigraphy showed uptake at the site of the nodule in the left lobe.
We present a novel case of bronchial carcinoma metastatic to the thyroid gland. Reviewing the literature, only 1% of carcinoids spread to endocrine organs, with the most frequent site being the pancreas. There were 3 accounts or a total of 8 cases of carcinoid tumor that metastasized to the thyroid gland. While most thyroid nodules are benign, the possibility of metastatic disease must be considered in patients no matter how remote the history of cancer.
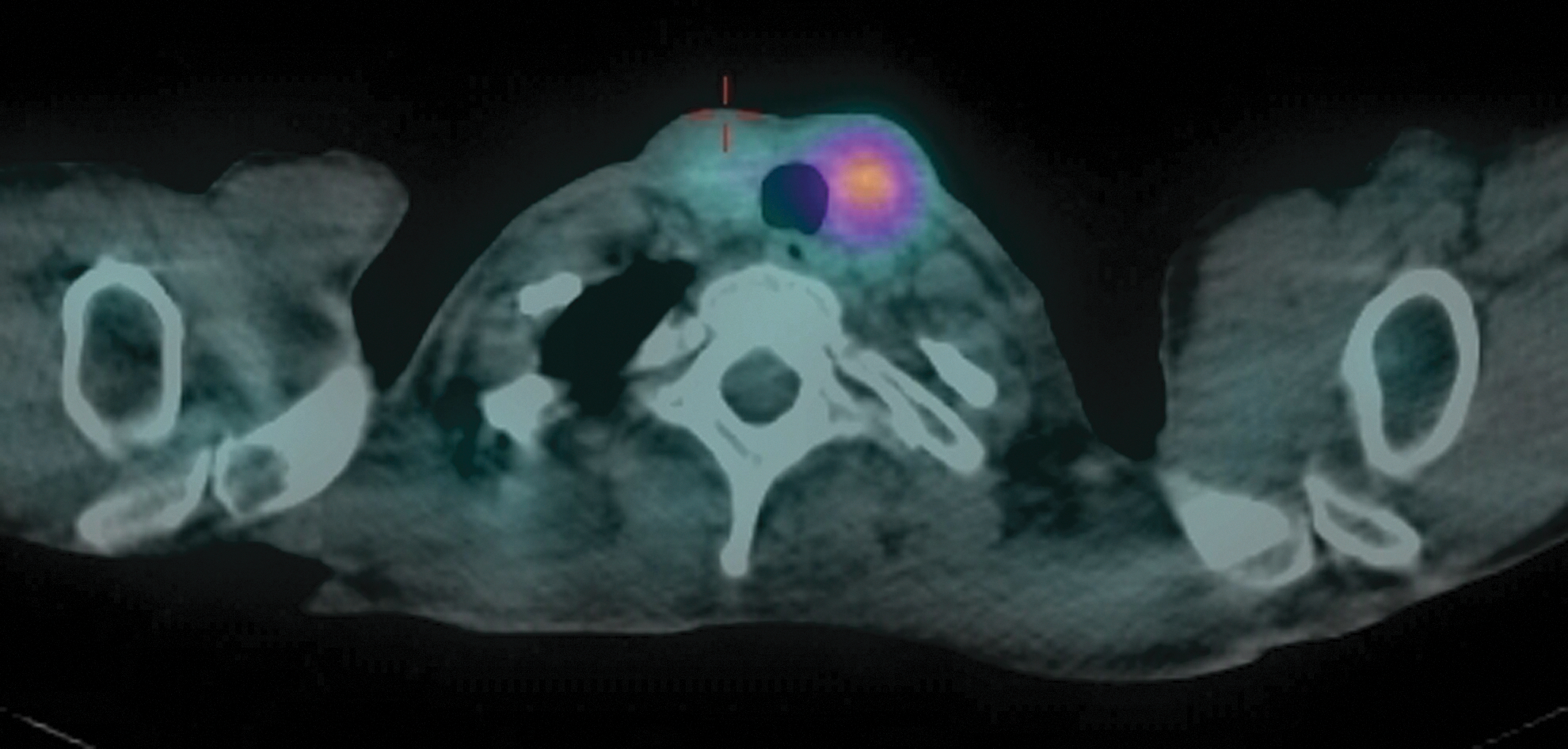
Fused image of 111In-Octreotide scan SPECT CT of neck with uptake in left thyroid lobe performed at 24 hrs.
Abstract Author Index
A'amar, O. P-230
Abaylai-uly, J.A. P-217, P-218
Abd-El Kareem, M. P-261
Abd-El Razek, S. P-261
Abdelmalek, M. P-55
Acca, M. P-168
Aceves, C. P-208, P-270
Adam, M. P-242, P-247
Adzick, N. P-150
Agah, R. P-120
Agate, L. P-63
Agcaoglu, O. P-79
Ahmadi, S. P-207
Ahmadzadehfar, H. P-164
Ahmed, I. P-186
Ahmed, R. P-275, P-276
Ain, K.B. P-251
Akpeng, B. P-62
Aksoy, E. P-79
Al Ajmi, S. P-264
AlbornozBalmaceda, E. P-43
Al-Brahim, N. P-264
Aldawish, M.A. O-29
Algeciras-Schimnich, A. O-28
Al Ghuzlan, A. O-9, P-227, P-253
Ali, H. O-17
Ali, S. P-42
Aliyev, S. P-79
Al-Johani, A. O-19
Alkazaz, N. P-176
Almeida, J.S. P-131
Al-Munshy, T. P-261
Al-Rijjal, R.A. P-151
Al-Salman, K. P-261
Alva-Sánchez, C. P-128, P-208
Al-Wagih, H. P-250
Alzahrani, A.S. P-151
Al-Zubeidi, H. P-127
Ammendola, M. P-167
Amouzgar, A. O-26
Ancelle, D. P-262
Anderson, G.W. O-14
Anderson, J.C. P-80
Andruss, B. P-152
Anguiano, B. P-208, P-270
Angulo-Barbosa, S. P-270
Antonelli, A. P-222, P-223
Antoun, S. P-88, P-89
Aoki, K. P-134
Appelman-Dijkstra, N. O-1
Araujo, P. P-112
Araya, A. P-215
Argirò, G. P-167
Armstrong, M. P-65, P-277
Arnesen, T. P-54
Arnold, A.M. O-7
Aroeira-Neves, M.G. P-131
Arrojo e Drigo, R. O-11
Asa, S.L. P-144
Ashur-Fabian, O. P-190
Asnani, S. P-80
Aso, S. P-91
Assumpção, L.M. P-112
Astapova, I. P-269
Atassi, T. P-273
Attaee, M. O-26
Attard, M. P-168
Au Yeung, Y. P-211
Aurengo, A. P-259
Austin, D. P-70
Ayers, S. O-13
Azizi, F. O-26
Babli, S. P-86
Badreddine, M. P-90
Bae, J. P-170, P-171
Bae, S. P-84
Bahn, R. P-205, P-206
Baitei, E.Y. P-151
Bak, B. O-1
Bald, E. P-268
Ball, D. O-17, O-25
Ban, Y. P-202, P-210
Banach, R. P-177
Bandai, S. P-50
Bandeira, F. P-97, P-98
Banerjee, M. P-74
Bansal, S. P-102
Baracos, V.E. P-88, P-89
Barbacioru, C. O-10
Barbaro, D. P-167
Bardet, S. P-153
Barnidge, D.R. O-28
Barreto, A. P-271
Barrett, P. O-23
Bartlett, D.L. P-277
Bassett, J. P-106
Bastian, T.W. O-14
Bastie, D. P-153
Baudin, E. O-9, P-173, P-227
Bauer, A. P-150
Bauer, R. O-2
Beaudenon-Huibregtse, S.L. P-152
Beck-Peccoz, P. O-1
Bellantone, R. P-232
Bender, J.L. P-176
Benhamou, E. P-153
Benisvy, D. P-153
Benvenga, S. P-118, P-119, P-120
Berber, E. P-79
Berman, J.W. P-43
Bernard, A. P-169
Bernard, D. O-1
Bernet, V. O-30
Bhatia, N.D. P-249
Bianco, A.C. O-11
Bienvenu-Perrard, M. O-20
Biermann, K. P-164
Biermasz, N. O-1
Biersack, H. P-164
Bigio, I. P-230
Bigorgne, C. O-20
Bigos, S.T. P-251
Bilezikian, J. P-48
Bischof, K. P-203
Bischoff, L.A. P-185, P-186
Bishop, J. P-62
Bocci, G. P-222
Boelaert, K. P-143, P-196
Boelen, A. O-23, P-272
Bohinc, B.N. P-55, P-56
Bonastre, J. P-153
Bonichon, F. O-9, P-87, O-21, P-153, P-169, P-240
Böning, G. P-224
Bonington, S. P-78
Bonomi, M. O-1
Boparai, J. P-207
Borget, I. O-9, P-88, P-89, O-21, P-153, P-173, P-227
Bosch, C. O-1
Bossowska, A. P-122
Bossowski, A. P-122
Bottici, V. P-238
Bournaud, C. P-153, P-169
Bowzyk Al-Naeeb AB, A. P-81
Bradley, N.L. P-69
Brandt, S.F. P-100, P-101
Brassard, M. O-21
Braun, D. P-192, P-273
Braverman, L.E. O-6
Brenta, G. P-271
Bresner, L. P-177
Breuning, M. O-1
Bridji, B. P-153
Brierley, J.D. P-176, P-251
BritoCampana, J. P-205, P-206
Brodschi, D. P-271
Brooks-Wilson, A. O-26
Broome, J.T. P-72, P-129
Brose, M.S. O-17, O-25
Broutin, S. P-88
Brouwers, A.H. P-195
Brunner, D. P-122
Bruno, R. P-168
Buell, J. P-138
Bueno, S.M. P-43
Bullock, M. O-27
Burch, H.B. O-34, P-241
Burnett, M. P-278
Burshell, A. P-94
Cabanillas, M. P-245
Caglar, D. P-59, P-68, P-161
Caicedo, D. O-11
Caldas, G. P-97
Caldwell, K.L. P-141
Caldwell, M. P-220
Calixto, A. P-112
Cambridge, E. O-1
Cambuli, F. P-103
Campi, I. O-1
Campos, M. O-11
Campos-Martin, Y. P-91
Cantara, S. P-61
Canterino, J. P-198
Capelli, V. P-258
Cappagli, V. P-238
Cappola, A.R. O-7
Capuano, S. P-61
Capula, C. P-168
Cardoso, L.F. P-191
Carlson, B.A. P-273
Carlson, D.L. P-155
Carrat, X. P-87, P-240
Carreño, L.J. P-43
Carrillo, D. P-215
Carty, S.E. P-65, P-147, P-277
Castagna, M. P-61
Castelo-Branco, M. P-165
Catargi, B. P-153
Cattani, A. P-215
Cazeau, A. P-87, P-240
Chae, B. P-170, P-171
Chaker, S. P-174
Chang, E. P-170, P-171
Channabasappa, S. P-40
Charboneau, W. O-8, P-73
Chatterjee, V. O-1, O-19
Chee, R. P-120
Chen, A. P-100, P-101, P-256
Chen, C. P-37
Chen, H. P-72
Chen, L. P-62
Chen, N.H. P-277
Chen, X. P-72
Chen, Z. P-100, P-101
Chiarini, S. P-274
Chiovato, L. P-258
Cho, M. P-145, P-146
Chockalingam, V. P-93, P-94
Choe, J. P-62
Choi, C. P-211
Choi, H. P-64
Choi, J. P-52, P-53, P-85
Chongkrairatanakul, N. P-266
Chougnet, C.N. O-9, P-71, O-21, P-173, P-227
Chowdry, R.P. P-101
Chudova, D. O-10
Chung, J. P-52, P-53, P-85
Chung, K. P-175
Chung, W. P-66, P-67
Chung, Y. P-257
Chwatko, G. P-268
Ciampi, R. P-238
Cisternas, P.A. P-43
Clairman, H. P-45, O-31
Clarke, B. P-48
Clary, D.O. O-25
Claude-Desroches, M. O-21
Clifton-Bligh, R.J. O-27
Cohen, E.E. O-17
Conte, F.F. P-149
Cooper, D.S. P-251
Copland, J.A. P-148, P-228
Corrado, A. P-223
Corsten, M. P-90
Cortes, C. P-43
Cosci, B. P-63
Costa Azevedo, M. P-98
Costa-e-Sousa, R.H. P-269
Costante, G. P-167, P-168
Costi, B. P-98
Cote, G. P-245
Coucoravas, C. P-103
Crocetti, U. P-168
Cunha, L.L. P-149
Curry, J. P-186
Curti, S. P-258
D'Aloiso, L. P-168
D'Angeli, F. P-61
D'Ercole, C. P-274
Da Settimo, F. P-222
Dadu, R. P-245
Dai, Q. P-154
Dalac, A. P-262, P-263
Dalal, S. P-113
Damante, G. P-166
Danesi, R. P-222
Dao, P. O-16
Darras, V.M. O-2, O-35, P-268
Dattani, M. O-1
Davicioni, E. O-16
Davidge Pitts, C. O-8, P-73
Davidov, T. P-108, P-109, P-110
Davies, T.F. P-60, P-201
Davis, T. O-1
Deandreis, D. O-9, P-153, P-173, P-227
Decallonne, B. P-242, P-247
de la Fouchardiere, C. O-21
de Leu, A.S. P-131
Dejax, C. P-153
Delezie, E. P-268
Delgado-Gonzalez, E. P-270
den Dunnen, J. O-1
De Nicola, P. P-99
de Paula, F.A. P-191
DePouli, L.C. P-278
De Remigis, A. P-99
De Remigis, P. P-99
De Schutter, H. P-242, P-247
Deshmukh, V.C. P-124, P-125
Dettmer, M.S. P-58
De Vis, K. P-157, P-158
de Vries, E.M. O-23, P-272
Dhindsa, S. P-135
Dhir, G. P-38
Diana, T. P-122, P-123, P-203
Di Domenicantonio, A. P-222
Diehl, A. P-55, P-56
Diggans, J. O-10
Dima, M. P-166
Dina, M. P-259
Ding, H. P-154
Djekidel, M. P-275, P-276
Do Cao, C. O-21
Dolev, Y. P-244
Dolp, P. P-224, P-225
Donadi, E.A. P-213
Dornelles, A. P-93
Driscoll, C. P-229
Driscoll, D.M. P-273
Dubois, C. P-242, P-247
Ducharme, M.P. P-118
Dugas, L. P-219
Durante, C. P-166, P-167, P-168
Durso, M. O-33
Earp, M. O-26
Eberhardt, J. O-34
Eberhardt, N. P-148, P-228, P-229
Eggels, L. O-23
Egri, P. P-107
Ehrenkranz, J. P-209
Eid, M. P-51
Elaraj, D. P-113
Elisei, R. P-63, O-17, O-25, P-238
El-Refaei, S. P-261
Elsawaf, M. P-248
El Serfay, M. P-250
Elson, D.F. P-266
Endo, K. P-204
Eric, B. P-88, P-89, O-21, P-253
Espiritu, T. P-209
Eugenin, E.A. P-43
Evjenth, R. P-54
Ezzat, S. P-144
Ezziddin, S. P-164
Fadda, G. P-232
Faingold, M. P-271
Fallahi, P. P-222, P-223
Fam, B. O-26
Fang, C. P-249
Farsetti, A. P-232
Fatemi, S. P-239, P-252
Faugeron, I. P-169
Federici, S. P-274
Fedewa, S. P-256
Feig, D. O-6
Fein, H.G. P-251
Feinglos, M. P-55
Feitosa, N.L. P-213
Fekete, C. O-11
Feliciello, A. P-61
Ferrannini, E. P-223
Ferrari, S. P-222, P-223
Fieffe, S. P-262, P-263
Filetti, S. P-166, P-167, P-168
Filippini, A. P-99
Fischetti-Galvin, J. P-198
Fisher, J. P-42
Fliers, E. O-23, P-272
Fong, J. P-196
Fonseca, C.P. P-165
Fonseca, T. O-11
Fortinsky, P. O-7
Fossati, M. P-271
Foyn, H. P-54
Frachetti, K. P-135
Francart, J. P-242, P-247
Franklin, J. P-90
Franklyn, J.A. P-143, P-196
Fratianni, C.M. P-265
Freitas, M. P-165
Friesema, E.C. O-35
Frigerio, C. P-271
Fujikawa, M. P-50
Fukata, S. P-132
Fuziwara, C. P-231
Gaba, A. P-172
Gaiti, M. P-258
Galton, V.A. P-106
Ganapathi, B. P-216
Gandhi, A. P-76
Ganly, I. O-4, P-155, P-162, P-236, P-237
Gannon, A. P-150
Garcia, E.S. P-213, P-231
García, H. P-215
García-Miñaur, S. P-182
Garfield, D. P-190
Geloneze, B. P-112
Georgieff, M. O-14
Gereben, B. O-11, P-107
Geske, J. O-8
Geysens, S. P-268
Gharavy, N. O-1
Ghossein, R. P-155, P-236
Giani, C. P-63
Giannella, A. P-274
Gilbert, M.E. P-189
Giorgenon, T. P-231
Giraudet, A. O-21
Giuffrida, D. P-167
Godbert, Y. P-87, P-240
Godoy, C. P-215
Göke, B. P-224, P-225
Gong, G. P-84
Gonzalez, P.A. P-43
Goranova, R. P-82
Goukassian, I. P-230
Govil, S.C. P-248
Grebe, S. P-228
Grebe, S.K. O-28, P-148
Grewal, R. O-4
Grilli, P. P-274
Grist, W. P-100
Grob, F. P-215
Gross, N. P-70
Grzegorzewski, K.F. P-100
Gu, Z. P-121
Guarneri, F. P-120
Gupta, V. P-172
Guy, C.D. P-55
Habeb, A. O-19
Habeos, I. P-233
Hacker, M. P-224, P-225
Haddad, Z. O-16
Haissaguerre, M. O-9
Halsall, D. O-19
Hambleton, C. P-138, P-139
Hammuda, M. P-221
Han, J. P-64, P-84
Hanaoka, N. P-254, P-255
Hara, T. P-184
Hartl, D.M. O-9, P-173, P-227, P-253
Hasham, A. O-15
Hatfield, D.L. P-273
Haugen, B.R. P-226, P-251
Hay, I. O-8, P-73
Hayes, K. P-256
Haymart, M.R. P-74
He, X. O-6
Heller, K.S. P-249
Hennekam, R. O-1
Henriques de Figueiredo, B. P-87, P-240
Henske, E. P-232
Hercbergs, A. P-190
Heuer, H. O-2, O-35
Heydarian, P. O-26
Hier, M.P. P-59, P-68, P-161, P-244
Hirano, T. P-202, P-210
Hiromura, M. P-210
Hoang, C. P-259
Hodak, S.P. P-65, P-147
Hollenberg, A.N. P-269
Holt, J.H. P-219
Homer, J. P-76
Hong, S. P-84
Hoofnagle, A.N. O-18
How, J. P-51
Howard, R. P-241
Howell, G. P-65
Howland, T. P-137
Hsu, H. P-102
Hull, B. P-49
Humaid, F.B. P-151
Ibrahim, B. P-68
Ibrahimpasic, T. P-155
Ikwuezunma, G.B. P-49
Imagawa, J. P-39
Italiano, A. P-87, P-240
Ito, K. P-47
Iwahara, K. P-133
Iwaku, K. P-47
Iwama, S. P-214
Izuora, K.E. P-142
Jacobs, S. P-101
Jain, K.S. O-5
Jang, H. P-85
Jansen, L. P-195
Jarjoura, D. O-12
Jarzab, B. O-17
Jayakumar, L. P-248
Jean-Louis, G. P-259
Jeon, E. P-179
Jeon, M. P-64
Jha, N. O-29
Jiang, X. P-81
Jiang, Y. P-154
Jing, F. P-75
Joe, A. P-164
John, M. P-216
Johnsen, L. P-44
Johnson, S. P-81
Johnston, J. P-172
Jones, A.D. O-30
Jones, R.L. P-141
Jonklaas, J. P-251
Joshi, M. P-38
Jozaghi, Y. P-59
Jung, E. P-179
Jung, S. P-170, P-171
Jung, Y. P-175
Kabaker, A. P-277
Kahaly, G.J. P-122, P-123, P-203
Kalergis, A.M. P-43
Kaleta, E.J. O-28
Kaliebe, O. P-93
Kalimani, E. O-22
Kalra, S. P-216
Kamel-Reid, S. P-144
Kandil, E. P-138, P-139, P-197
Kang, B. P-145, P-146
Kant, S. O-1
Kantor, G. P-87
Karawagh, A. P-130
Karreth, F.A. P-232
Katz, P.M. O-6
Keddache, M. O-3
Kelly, A. P-169
Kelly, L.M. P-147, O-33
Kempers, M. O-1
Kemppainen, J. P-152
Kennedy, G. P-148
Kennedy, G.C. O-10
Kennedy, S. P-78
Khan, A.N. P-42
Khan, M. P-207
Khuri, F.R. P-100, P-101
Kievit, J. P-246
Kikut, J. P-278
Kim, B.W. O-24
Kim, E. P-170, P-171
Kim, H. P-52, P-53, P-84, P-85, P-260
Kim, J. P-123, P-145
Kim, K. P-145, P-146, P-260
Kim, N. P-52, P-53, P-85
Kim, S. P-52, P-53, P-85, P-101, P-170, P-171, P-175
Kim, T. P-64, P-84, P-175
Kim, W. P-64, P-84
Kim, Y. P-180, P-181, P-260
Kimura, E.T. P-231
Kinuya, S. P-267
Kirschner, L. O-12
Kita, H. P-267
Kitazono, T. P-50
Klein, M. P-273
Kloos, R.T. O-10
Knoop, K. P-224, P-225
Koenig, R.J. P-74
Köhrle, J. P-192
Komminoth, P. P-58
Kongsted, A.H. P-44
Kono, S. P-100
Kosok, L.L. O-30
Kramp, K.H. P-246
Kreissl, M.C. O-17
Kriek, M. O-1
Krishnasamy, S. P-187
Kulcsar, M.A. P-255
Kumar K M, P. P-40
Kunii, Y. P-47
Kunwar, S. P-92
Kuo, Y. P-80
Kushnir, M.M. O-18
Kwak, H. P-170, P-171
Kwakkel, J. O-23, P-272
Kwan, P. P-143, P-196
Kwon, S.C. P-249
Kyriazopoulou, V. P-233
Labourier, E. P-152
Ladenson, P.W. P-251
Lagarde, P. P-87, P-240
Lagast, H. P-48
La Manna, L. P-258
La Motta, C. P-222
Langfield, L. P-152
Lanman, R. O-10
Lann, D.E. P-80, P-198, P-248
Lapenta, L. P-274
La Perle, K.M. O-12
Lapunzina, P. P-182
Laros, J. O-1
Larson, S. O-4
Latif, R. P-60, P-201
Lau, V. O-24
Lawler, J. P-232
Leadbeater, W.E. P-196
Leboulleux, S. O-9, P-88, P-89, O-21, P-153, P-169, P-173, P-227, P-253
Lechan, R. O-11
Lecumberri, B. P-182
Lee, A.A. O-12
Lee, C. P-67, P-175
Lee, D. P-178
Lee, E. P-175
Lee, J. P-66, P-67, P-179, P-209
Lee, K. P-178
Lee, R. O-8, P-73
Lee, S. P-230
Lee, Y. P-175
Leenhardt, L. P-153, P-259
Lennerz, B. P-122
Lepoutre-Lussey, C. P-259
Lessig, M.K. P-150
le Tissier, P. O-1
Letizia, C. P-166
Leung, A.M. O-6
Lewy, G.D. P-196
Li, Y. P-123
Liang, J. P-75, P-163, O-32
Liang, Z. P-163
Licitra, L. O-17
Lilis, I. P-233
Lim, I.P. P-249
Lima, L. P-98
Lin, Y. P-46, P-75, P-163, O-32, O-36
Linek, M. P-254, P-255
Lischinsky, J. P-45, O-31
Liu, W. P-121
Llamazares, O. P-91
Lobo, M.A. P-131
Loiseau, H. P-87
Lombardi, C.P. P-232
Long, W. P-46, O-36
López, J. P-91
Lorusso, L. P-63
Lotay, V. O-15
Loughran, S. P-76
Lu, C. P-245
Lu, S. P-109, P-110
Lukacova-Zib, I. P-96
Lumbroso, J. P-227
Luo, B. P-154
Luque, A. P-91
Lv, M. P-154
Lyford-Pike, S. P-62
Ma, R. P-60, P-201
MacConaill, L. P-232
Macias, C.A. P-108
Maciel, L.M. P-191, P-212, P-213, P-231
MacMillan, C. P-174
Madde, P. P-228, P-229
Magalhaes, P.K. P-212, P-213, P-231
Magner, J. P-251
Magri, F. P-258
Mahdi, Y. P-273
Maia, J. P-97
Majeed, M. P-130
Majumder, A. P-117
Makambi, K.H. P-193
Makhmudov, A.A. P-141
Mallick, U. P-81, P-82, P-83
Mamelle, E. P-173
Manchanda, P.K. O-12
Mancusi, C. P-223
Mangeshkar, M. O-17
Maniakas, A. P-161
Mannstadt, M. P-48
Manolakou, S. P-111, P-233
Marcello, M.A. P-112, P-149
Marchese, C. P-274
Marconcini, G. P-238
Mariotta, L. O-35
Marlow, L.A. P-148, P-228
Marti, J.L. O-5
Martínez-Aguayo, A. P-215
Martinez-Barbera, J. O-1
Massicotte, M. P-88, P-89, O-21
Matsubayashi, S. P-41, P-184
Matsumoto, M. P-47
Matsumoto, S. P-41
Matsushita, A. P-134
Maxon, H.R. P-251
Mayerl, S. O-2
Mayor, M. P-182
McCabe, C.J. P-143, P-196
McCoy, K.L. P-65, P-277
McDonald, T. P-90
McEwan, A.J. O-29
McIver, B. O-28, P-148, O-30, P-228, P-229
McLachlan, S. P-37
McLeod, D.S. P-251
McNicol, A. P-81
Medina, M. O-11
Medvedev, V. O-17
Meijer, J.A. P-246
Meikle, A. O-18
Memeo, L. P-167
Mencel, P. P-248
Ménégaux, F. P-259
Meng, C. P-163, O-36
Merad, M. P-88, P-89
Meringolo, D. P-168
Mesquita, P. P-97
Mete, O. P-144
Meyer, B.F. P-151
Miccoli, P. P-222
Michigishi, T. P-267
Miles, D. O-25
Milham, D. P-209
Miller, B.T. O-24
Miller, J.L. P-185, P-186
Milosevic, D. P-148
Minagawa, A. P-47
Miniard, A.C. P-273
Minutti, C. P-219
Mirghani, H. O-9, P-173, P-227
Mitchell, M. P-102
Mitmaker, E.J. P-86
Miyauchi, A. P-39
Miyawaki, N. P-39
Mizukami, Y. P-267
Mlynarek, A. P-59, P-68, P-161
Moch, H. P-58
Mochizuki, T. P-134
Molinaro, E. P-63
Momotani, N. P-132, P-214
Montesano, T. P-167
Monzani, F. P-167
Mora-Garzon, M. O-11
Moraitis, D. O-22
Moran, C. O-19
Morari, E. P-149
Morel, O. P-153
Mori, M. P-70
Morioka, T. P-134
Morita, H. P-134
Morlan, M. P-91
Morris, L.G. O-5
Morrish, D.W. O-29
Morrison, D. P-90
Morrison, J.A. P-226
Morrow, L. P-220
Morshed, S.A. P-201
Mostoufi-Moab, S. P-150
Mott, J. P-82
Muckle, M. P-164
Mueller, J. O-35
Mukasa, K. P-47
Müller, S. O-17, O-25
Muller-Kobold, A.C. P-195
Murad, M.H. P-205
Murby, B. P-76
Musso, C. P-271
Nabawi, A. P-250
Nakamura, H. P-39, P-133
Nakatake, N. P-132
Nallala, D. P-265
Nanni, S. P-232
Narawane, R. P-54
Nascimento, C. P-227
Nassif, J. P-105
Nathan, M.H. P-278
Navarrete, P. P-104
Nayar, R. P-113
Nelkin, B. O-17, O-25
Nelson, P.J. P-224, P-225
Nepote, A. P-271
Netzel, B.C. O-28
Newfield, R. P-127
Ng, C. P-211
Ng, Y. P-211
Niederle, B. O-17
Niel, S. P-203
Nielsen, M.O. P-44
Nikiforov, Y.E. P-58, P-65, P-147, O-33
Nikiforova, M.N. P-58, P-65, P-147, O-33
Nikolopoulos, S.N. O-22
Nistal, M. P-182
Nixon, I.J. O-4, P-155, P-162, P-236, P-237
Nk, T. P-130
Noh, J.Y. P-47
Nookala, R. P-129
Noureldine, S.I. P-139, P-197
Nucera, C. P-232
Nudischer, R. O-26
O'Donnell, A. P-136
Ogilvie, J.B P-249
Ohba, K. P-133, P-134
Ohye, H. P-47
Ojomo, K.A. P-243
Okamura, K. P-50
Oki, Y. P-134
Oliveira, J.C. P-213
Olivo, P.D. P-122, P-123, P-203
O'Mara, D. P-193
Onjaro, G.A. P-111
Oostdijk, W. O-1
Opazo, M.C. P-43
Orellana, P. P-215
Orlandi, F. P-167
Orozco, A. P-104
Orradre, J. P-91
Otsuka, F. P-204
Owonikoko, T.K. P-100, P-101
Pacheco-Rosado, J. P-189, P-208
Paciaroni, A. P-168
Pacini, F. P-61
Pai, S.I. P-62
Paixão, C.M. P-131
Pallardo, L. P-182
Palmer, F.L. O-4, P-155, P-162, P-236, P-237
Palussière, J. P-240
Pan, C. P-121
Pandolfi, P. P-232
Pang, H. P-55
Panunti, B. P-93
Papachristou, D. P-233
Papaleontiou, M. P-74
Papneja, N. P-95
Paramesh, A. P-42
Pardoll, D. P-62
Park, H. P-257
Park, J. P-67
Park, K. P-145, P-146
Park, R. P-70
Park, S. P-257
Parlow, A.F. O-12
Parrott, N. P-76
Pasternak, J.D. P-199, P-200
Patel, K. P-249
Patel, S.G. O-4, P-155, P-162, P-236, P-237
Patey, M. P-262
Paul, T. P-90
Payne, R.J. P-59, P-68, P-86, P-161, P-244
Pearce, E.N. O-6
Pelegrina, B. P-182
Peng, S. P-62
Peoples, G. O-34
Pereira, A. O-1
Pérez, L. P-182
Perren, A. P-58
Persani, L. O-1
Petrovic, I. P-239
Phan, H.T. P-195
Piercy, D. P-55
Pieruzzi, L. P-63
Piha-Paul, S. P-245
Pilli, T. P-61
Pinchera, A. P-238
Pitelka-Zengou, L. P-113
Plateroti, M. P-103
Plukker, J.T. P-195, P-246
Pochart, J. P-262, P-263
Polson, R. P-209
Ponce, C. P-271
Pontecorvi, A. P-167, P-232
Potdevin, L. P-108, P-109, P-110
Prasad, M. P-276
Prazeres, P. P-98
Prebtani, A. P-95
Pribitkin, E. P-186
Pringle, D.R. O-12
Priolo, C. P-232
Prohaska, J. O-14
Prokop, L. P-205
Psaty, B.M. O-7
Puxeddu, E. P-168
Qian, L. P-154
Qiu, L. O-36
Rachinsky, I. P-90
Radowsky, J. O-34, P-241
Rahmani, M. O-26
Rajab, H. P-49
Rajanayagam, O. O-19
Rajaraman, M. P-90
Ralhan, R. P-174
Ramalingam, S.S. P-100, P-101
Ramírez-San Juan, E. P-128
Rangasami, J. O-1
Rao, A.D. P-117
Rapoport, B. P-37
Read, M.L. P-143, P-196
Reading, C. O-8, P-73
Reddi, H.V. O-28, P-148, O-30, P-228, P-229
Reix, N. P-273
Reynolds, J. O-10
Ricard, M. P-153
Richardson, K. P-59
Riedel, C.A. P-43
Rivera, J. P-86
Roberts, W.L. O-18
Rockwood, A.L. O-18
Rodin, G. P-177
Rodriguez, A. P-208
Rodriguez-Diaz, E. P-230
Rogerio, J. P-100
Rohl, S. P-148
Romei, C. P-63, P-238
Ronga, G. P-167
Rosai, J. P-99
Rosen, J.E. P-230
Ross, D.S. P-251
Rouxel, A. O-20
Rovet, J.F. P-45, O-31
Royer, B. O-20
Ruffilli, I. P-222
Ruivenkamp, C. O-1
Russ, G. O-20
Russo, D. P-166, P-167
Ryan, G. P-143, P-196
Ryu, H. P-257
Ryu, J. P-175
Ryu, Y. P-175
Saba, N.F. P-100
Sabet, A. P-164
Sadeghi-Nejad, A. P-102
Sadow, P.M. P-232
Sahay, R.K. P-216
Saiprasad, S. P-220
Salama, M. P-137
Salazar, L. P-37
Saliba, J. P-161
Sams, S.B. P-226
Sanchez-Huerta, K. P-189
Sandison, A. P-106
Santos, J. P-165
Saraceno, G. P-119
Sarantopoulou, C. O-22
Sasaki, S. P-134
Sastre, J. P-91
Sato, K. P-50
Satoh, T. P-133
Savagner, F. P-240
Sawicki, M.P. P-183
Sawka, A. P-176, P-177
Schlumberger, M. O-9, P-71, P-88, P-89, O-17, O-21, O-25, P-153, P-173, P-227, P-253
Schneider, D.F. P-72, P-243
Schnitman, M. P-271
Schoenmakers, N. O-1
Schöffski, P. O-17, O-25
Schomburg, L. P-273
Schvartz, C. P-153, P-240, P-262, P-263
Schweizer, U. P-192, P-273
Schwenk, N. P-224, P-225
Scopa, C. P-233
Sedlinsky, C. P-271
Seed, R.I. P-143, P-196
Seeher, S. P-273
Sekhon, S. P-95
Sekiya, K. P-47
Sela, E. P-59
SellariFranceschini, S. P-223
Severin, D. O-29
Shah, J.P. O-4, P-155, P-162, P-236, P-237
Shah, M. O-17, O-25
Shaha, A.R. O-4, P-155, P-162, P-236, P-237
Sharma, J. P-100, P-101
Sharma, N. P-143, P-196
Sharma, P. P-220, P-264
Sharma, V. P-226
Sherman, S. O-17, O-25, P-251
Shi, Y. P-151
Shifrin, A.L. P-80, P-198, P-248
Shin, D.M. P-100
Shinall, J.B. P-129
Shinall, M.C. P-129
Shinde, R. P-152
Shindo, M. P-70
Shoback, D. P-48
Shon, H. P-179
Shong, Y. P-64, P-84
Silva, S.O. P-131
Sim, J. P-145, P-146
Singaporewalla, R.M. P-117
Singh, R.J. O-28
Siperstein, A. P-79
Sippel, R.S. P-72, P-243
Sisson, J. P-74
Skarulis, M.C. P-251
Skocic, J. P-45, O-31
Skugor, M. P-92
Sluiter, W. P-195
Smallridge, R. P-148, O-30
Smit, J.W. P-246
Smith, J. P-72
Smith, V.E. P-143, P-196
Soares, F.A. P-149
SoaresFilho, M.A. P-97, P-98
Soldin, O.P. P-193
Solorzano, C.C. P-72, P-129
Song, B. P-170, P-171
Song, H. P-121
Soubeyran, I. P-87, P-240
Spaulding, S. P-135, P-136
Spencer, C. P-239, P-252
Spitzweg, C. P-224, P-225
Sponziello, M. P-166
Srivatsa, S. P-100, P-101
Stan, M.N. P-205, P-206
Stang, M.T. P-65, P-277
Stannek, S. P-203
St. Clair-Rein, L. P-207
Steck, J.H. P-254, P-255
Stefan, M. O-3
Steward, D.L. P-251
St. Germain, D.L. P-106
Stojadinovic, A. O-34, P-241
Stokvis-Brantsma, W. O-1
Stordeur, S. P-242, P-247
Sturgeon, C. P-113
Sugisawa, C. P-204
Suh, H. P-230
Sun, S. P-100
Sun, Y. O-1
Sundaresh, V. P-205, P-206
Surovtseva, O. P-272
Suzuki, A. P-55
Suzuki, M. P-47
Swamy, N. P-220
Swindell, R. P-76, P-78
Sykiotis, G. P-233
Tabah, R. P-51
Tacito, A. P-63
Tajiri, J. P-132
Takahashi, G. P-134
Takahashi, Y. P-204
Takeda, H. P-267
Takizawa, N. P-41
Tamburrano, G. P-166
Tamilia, M. P-59, P-161, P-244
Taniyama, M. P-202, P-204
Taskin, H.E. P-79
Taylor, B. P-78
Teixeira, P.S. P-131
Thabane, L. P-177
Thapa, P. P-206
Thethi, T.K. P-42
Thien, C.I. P-131
Thompson, P.R. P-54
Thuret, A. P-263
Tincani, A.J. P-112
Tiu, S. P-211
Tohidi, M. O-26
Tom, E. O-10
Tomer, Y. O-3, O-15
Tonda, M. O-17
Toor, A. P-172
Torlontano, M. P-167, P-168
Torregosa, H. P-187
Toti, P. P-61
Toubeau, M. P-240
Toubert, M. P-153, P-169
Tozaki, T. P-202, P-210
Trahan, M.A. P-197
Tran, L. P-221
Travagli, J. P-253
Treml, M. O-26
Trésallet, C. P-259
Triche, T. O-16
Trimarchi, F. P-119
Troalen, F. P-227
Trooskin, S.Z. P-108, P-109, P-110
Tsoumalis, G. O-22
Tsuji, S. P-267
Tsukatani, T. P-267
Tuluc, M. P-185
Tumino, S. P-167, P-168
Turbeville, P. P-209
Turnell, A. P-143
Tuttle, R.M. O-4, P-155, P-162, P-236, P-237
Uchida, H. P-134
Ueta, C. O-11, O-24
Unnikrishnan, A.G. P-216
Unno, T. P-133
Vaisman, M.A. P-131
Valerio, L. P-238
Valverde-R, C. P-104
Van den Bruel, A. P-242, P-247
van der Horst-Schrivers, A.N. P-195
van Dijk, D. P-195, P-246
Van Herck, S.L. P-268
Van Horn, L. P-198
van Trotsenburg, P. O-1
Van Uum, S.H. P-90
Varhaug, J. P-54
Varthakavi, P.K. P-124, P-125
Vasconcelos, E. P-255
Vasko, V. O-12
Vasques, A.J. P-112
Vassallo, J. P-149
Vaz, C. P-135, P-136
Veloski, C. P-38
Vera, P. P-153
Verbeek, H.H. P-246
Véronique, L. P-259
Verrey, F. O-35
Verrienti, A. P-166
Versey, H. P-83
Vicente, A. P-91
Villalobos, P. P-104
Villani, L. P-258
Villanueva, I. P-128, P-208
Villanueva, V. P-271
Viola, D. P-238
Visser, T.J. O-2, O-35
Vita, R. P-119, P-120
Vivaldi, A. P-63
Vlaeminck-Guillem, V. P-103
Vlayen, J. P-242, P-247
Vokes, T. P-48
Volpi, E. P-255
Voshol, P. O-1
Vulsma, T. O-1
Wada, S. P-184
Wagner, E. P-224, P-225
Walfish, P.G. P-174
Walker, B. O-16
Walsh, P.S. O-10
Wang, H. P-121
Wang, M.B. P-183
Wang, S. P-70
Wang, W. P-154
Ward, L.S. P-112, P-149
Warfield, A. P-196
Watanabe, K. P-134
Watanabe, N. P-47
Watkinson, J.C. P-196
Waung, J.A. P-106
Welch, A. P-81
Werneck-de-Castro, J. O-11
Westra, W. P-62
Whitcher, M.M. O-4, P-162, P-236, P-237
White, J. O-1
Wilde, J.I. O-10
Wiljer, D. P-176
Wilkins, F.A. P-42
Willhauck, M.J. P-224, P-225
Williams, G. P-106
Willis, N. P-82, P-83
Winer, D. P-144
Wirth, E.K. P-273
Wirth, L. O-17
Wiseman, S.M. O-16, P-69
Wit, J. O-1
Wittmann, G. O-11
Wnek, A. P-136
Wong, M. O-10
Wood, C. P-221
Wood, W.M. P-226
Wu, J. O-26
Wyllie, D. P-152
Xiao, C. P-221
Xue, L. P-121
Yadav, A. P-142
Yan, K. P-154
Yang, D. P-74
Yang, J. P-145, P-146
Yang, S. P-121
Yao, L. P-139
Yap, B.K. P-76, P-77, P-78
Yassin, S.W. P-261
Ye, F. P-269
Yen, P. P-55
Yip, L. P-65, P-277
Yokoyama, K. P-267
Yoo, J. P-90
Yoo, Y. P-145, P-146
Yoshihara, A. P-47
Yoshino, A. P-134
Young, G. P-62
Young, J. P-199, P-200
Yu, J.Z. P-249
Yu, L. O-12
Yu, S. P-142
Yudd, A. P-109
Zach, C. P-225
Zago, S. P-253
Zakarya, S. P-250
Zandee, W. P-246
Zang, W. O-3
Zankl, H. P-224
Zanocco, K. P-113
Zanolli, M. P-215
Zerdoud, S. P-153
Zhan, M. P-121
Zhang, B. P-154
Zhang, G. P-100
Zhang, W. O-15
Zhao, D. O-32
Zhao, S. P-121
Zheng, R. P-154
Zhou, Q. P-226
Zhu, H. O-1
Ziora, K. P-122
Ziros, P. P-233
Zischek, C. P-224, P-225
Zou, M. P-151