
Abstract
Background:
Controlled ovarian hyperstimulation (COH) is a crucial step of assisted reproductive technology (ART). Thyroid dysfunction and autoimmune thyroid disease (ATD) may negatively affect the outcome of ART, but the underlying mechanisms are still poorly understood. Our aim was to evaluate the respective role of ATD and thyroid function, as assessed by serum thyrotropin (TSH), on the early outcome of COH.
Methods:
In total, 262 (202 ATD-negative and 60 ATD-positive) euthyroid subfertile women underwent ART. Before COH, serum follicle-stimulating hormone (FSH), luteinizing hormone, and estradiol (E2) were measured at cycle day 3, and progesterone at cycle day 21. At oocyte pickup and at embryo transfer, we evaluated the performance of recombinant FSH (r-FSH), as assessed by serum E2 concentration/total administered r-FSH units (E2/r-FSH) ratio and by oocyte quality.
Results:
At both oocyte pickup and embryo transfer, the performance of r-FSH was significantly poorer in ATD-positive than in ATD-negative women. In the ATD-positive group, women with a TSH <2.5 mIU/L displayed a higher serum E2 concentration at oocyte pickup, a higher E2/r-FSH ratio, and a greater number of mature metaphase II oocytes than women with a TSH >2.5 mIU/L. When ATD-positive women were divided into quartiles according to their serum TSH level, both the ovarian response to r-FSH and the number of mature metaphase II oocytes significantly increased from the lowest to the highest quartiles of serum TSH concentration.
Conclusions:
ATD has a negative effect on the early outcome of COH, but this negative influence may be avoided with adequate levothyroxine therapy aimed at keeping TSH <2.5 mU/L. Thyroid antibodies and serum TSH should be checked in any woman undergoing ART
Introduction
Because of the high prevalence of ATD in the female sex on one hand, and the association between ATD and reduced fertility on the other hand, it is not surprising that a consistent number of subfertile women with ATD undergo assisted reproductive technology (ART). A crucial step of ART is controlled ovarian hyperstimulation (COH), in which a regimen of fertility medications is used to stimulate the development of multiple ovarian follicles in a single cycle. Compared with a natural menstrual cycle, this procedure allows to retrieve more than one fertilizable oocyte (7) and to select embryos for transfer and for cryopreservation (8). Many efforts have been made to optimize COH by designing treatment schedules tailored to individual responses, which depend on an array of factors, including maternal age, ovarian reserve, and genetic predictors (9,10).
The mechanisms responsible for the association between ATD and poor ART outcomes are still under debate. Besides the potential negative impact of thyroid autoimmunity per se on the outcome of ART in terms of pregnancy rate (11) and risk of miscarriage (12 –16), strong evidence suggests that inappropriately low levels of thyroid hormones, being caused by ATD, play an important role (17,18). Cramer et al. (19) reported that a raised serum TSH, suggesting subclinical hypothyroidism, significantly predicted failure of in vitro fertilization. Furthermore, LT4 treatment in female patients with subclinical hypothyroidism was proven to have beneficial effects on embryo quality and implantation, and reduced the miscarriage rate (20,21). In this regard, it is still unclear whether thyroid autoimmunity per se exerts such a negative effect or if it just represents a marker of a more generalized immune imbalance. Moreover, there are no conclusive data to determine which is the main factor in pregnancy outcome after ART, that is, either thyroid autoimmunity or impaired thyroid function. By reviewing available data, Krassas et al. (4) concluded that an association does exist between ATD and pregnancy outcome, but this link is far from unequivocal, leaving many questions unanswered. Differences in the methodological approach, timing of observation, and age of patients may partially explain why clear evidence is still lacking. It is likely that multiple mechanisms contribute to the success or the failure of both natural and medically assisted pregnancy. These factors include oocyte biology, embryonic development, endometrial receptivity, and coexistent morbidities, such as obesity, polycystic ovary syndrome, and endometriosis (22).
The aim of the present study was to evaluate the respective role of thyroid autoimmunity and thyroid function, as assessed by serum TSH level, on the ovarian response to a standard protocol of controlled hyperstimulation. We decided to focus on this short-term outcome in order to selectively study the influence of thyroid diseases on the ovarian sensitivity to gonadotropin stimulation. Using this design, we avoided the confounding effect of the many other factors, which contribute to the final outcome of ART (endometrial microenvironment, male factor, anatomical abnormalities). To this purpose, we evaluated two parameters of the COH procedure: (a) the ovarian response to recombinant follicle-stimulating hormone (r-FSH), as assessed by the ratio of serum estradiol (E2) concentration over the total number of administered r-FSH units (E2/r-FSH ratio); (b) the number of retrieved mature metaphase II (MII) oocytes. These short-term outcomes were compared in two groups of euthyroid subfertile women subdivided according to the presence or absence of ATD. Women with and without ATD shared the same age range. All women were candidates for in vitro fertilization with intracytosplasmic sperm injection.
Subjects and Methods
We performed a retrospective, cohort, single-center study, which was approved by our Institutional Review Board. The study group included 262 euthyroid subfertile women undergoing their first ART procedure, who were recruited from January 2006 to January 2012. All subjects resided in a northern Italy area, which is characterized by mild iodine deficiency. Inclusion criteria were as follows: (a) subfertility of various causes; (b) indication for one ART cycle through a long gonadotropin-releasing hormone-α protocol with r-FSH; (c) a euthyroid state at the time of COH (either spontaneous or resulting from LT4 substitution treatment); (d) availability of information about thyroid autoimmunity tests. All patients gave their written informed consent for the future use of clinical and hormone data for research purposes according to the local Ethics Committee and the guidelines of the Declaration of Helsinki. In the study group, 202 women had no biochemical or clinical evidence of thyroid autoimmune disease (ATD-negative) and 60 had evidence of thyroid autoimmunity (ATD-positive), as assessed by positive results (at least two times higher than the reference range) in the tests for antithyroglobulin and/or antithyroid peroxidase antibodies. ATD-negative and ATD-positive women shared the same age range. In the ATD-positive group, the majority of women (87%) were untreated, whereas 13% were treated with LT4 for a previous diagnosis of hypothyroidism. Demographic data were collected and body mass index (BMI) was calculated in each subject. Before the COH procedure, we measured serum FSH, luteinizing hormone (LH), E2, and prolactin (PRL) at cycle day 3, and serum progesterone at cycle day 21.
COH protocol
The stimulation protocol was performed as follows: on day 21 of the previous cycle, a baseline ultrasonography scan was performed and leuprorelin acetate (Enantone; Takeda Italia Farmaceutici S.p.A) was administered subcutaneously at a daily dosage of 1.0 mg for at least 14 days. After having confirmed ovarian suppression by both ultrasonography scan (absence of ovarian activity, ovarian cyst formation, and endometrial proliferation) and serum E2 levels ≤40 pg/mL, exogenous gonadotropin administration was started. COH was performed with r-FSH (Gonal-F; Merck-Serono) at a fixed daily dosage of 150 IU for 5 days. Serum E2 levels were measured five days after starting r-FSH, when the first scan was performed and the dose of r-FSH was adjusted according to the ovarian response. Starting from day 9, women were observed daily until the criteria were fulfilled for discontinuing the gonadotropin-releasing hormone analog and for administering human chorionic gonadotropin (hCG) at a dose of 10,000 IU intramuscularly. hCG treatment was aimed at triggering ovulation, as assessed by the appearance of at least two leading follicles, with a mean diameter >18 mm, and by the rise of serum E2 concentration. No longer than 24 hours elapsed from the last injection of r-FSH and the administration of hCG. Thirty-five to 36 hours after hCG administration, ovum pickup was performed by trans-vaginal ultrasound-guided ovarian puncture. After stripping, oocytes were assessed for their maturation; only oocytes having resumed their first meiotic division and reaching metaphase II were used for in vitro fertilization. On the day of transfer, embryos were graded according to their morphologic appearance under a light microscope, and transferred.
On both the day of pickup and the day of embryo transfer, the ratio between serum E2 concentration and the total number r-FSH IU administered during the CHO procedure (E2/r-FSH ratio) was calculated. This allowed measuring the performance of r-FSH in producing an adequate ovarian stimulation in ATD-positive as opposed to ATD-negative women.
Serum assays
The serum concentrations of TSH (third-generation TSH assay; normal range 0.4–4 mIU/L) were measured using an immunochemiluminescent assay by an automated analyzer (Immulite 2000; DPC Cirrus) employing commercial kits (Diagnostic Products Corporation). The sensitivity of the assay was 0.004 mIU/L and the intra- and interassay coefficients of variation were 3.5% and 5.4%, respectively. Serum concentrations of antithyroglobulin antibody (Tg-Ab; normal range <60 U/mL) and anti–thyroid peroxidase antibody (TPO-Ab; normal range <60 U/mL) were measured using immunochemiluminescent assays employing commercial kits (Brahams). The sensitivity of the assay was 33 U/mL for TG-Ab and <50 U/mL for TPO-Ab. The intra- and interassay coefficients of variation were 2.6% and 13%, respectively, for TG-Ab and 3.9% and 8%, respectively, for TPO-Ab.
Serum E2 and progesterone levels were measured using a commercial RIA kit (Diagnostic Systems Laboratories). The sensitivity of the assay was 2.2 pg/mL and 0.12 ng/mL, respectively; the intra- and interassay coefficients of variation were 7.5% and 9.3%, respectively, for serum E2 and 6.8% and 8.8%, respectively, for progesterone. Serum FSH and LH levels, as well as PRL, were measured by immunoenzymatic assays (FSH and PRL [Abbott Laboratories]; LH [Dade Behring]). The sensitivity of the assay was 0.2 U/L for FSH and LH; the intra- and interassay coefficients of variation were as follows: FSH, 4.7% and 8.9%, respectively; LH, 3.1% and 4.0%, respectively. The sensitivity of the assay was 0.6 ng/mL for PRL; the intra- and interassay coefficients of variation were 5.3% and 7.1%, respectively.
Statistical analysis
A preliminary power analysis was performed, which confirmed a good statistical power (alpha=0.02, power [1 − beta error prob]=0.90) with our number of patients, means, and standard deviations.
Quantitative values were expressed as mean±SD or as median and interquartile range, as appropriate. Between-group comparisons were performed by Student's t-test for unpaired data and by the Mann–Whitney U-test according to a normal or nonparametric distribution of data and variable tested. A p-value <0.05 was considered statistically significant. When more than two groups were compared, the analysis of variance was performed.
Results
The clinical and hormone features of subfertile women, subdivided according to their ATD status, are summarized in Table 1. Age, BMI, causes of infertility, and prevalence of male factor infertility were equally distributed in the two groups of women. Similarly, no significant difference between ATD-positive and ATD-negative women was found for their serum level of TSH; for the early follicular phase concentration of FSH, LH, E2, and PRL; and for the serum concentrations of progesterone during the luteal phase before undergoing ART.
Data arepresented as mean±SD or percent of the corresponding group.
On cycle day 3.
On cycle day 21.
ATD, autoimmune thyroid disease; BMI, body mass index; FSH, follicle-stimulating hormone; LH, luteinizing hormone; n.s., not significant; PCOS, polycystic ovary syndrome; r-FSH, recombinant-FSH; TSH, thyrotropin.
Short-term outcome of COH in ATD-positive and ATD-negative women
The mean (±SD) total dose of administered r-FSH was 2207.4±1117.6 IU and 2283.1±990.1 IU in ATD-negative and ATD-positive women, respectively. While the mean serum level of E2 measured at oocyte pickup did not significantly differ in ATD-positive as compared with ATD-negative women (939.6±615.5 pg/mL vs. 1187.4±847.0 pg/mL, respectively), at the day of embryo transfer the mean serum concentration of E2 was significantly lower in ATD-positive as compared with ATD-negative women (803.2±528.0 vs. 1091.2±692.5, respectively, p=0.018). The E2/r-FSH ratio at the time of pickup (left panel) and embryo transfer (right panel) and the total number of administered r-FSH IU during the COH procedure are shown in Figure 1. These data indicate that the performance of r-FSH in producing an adequate ovarian stimulation was significantly poorer at both oocyte pickup and embryo transfer in ATD-positive compared with ATD-negative women.
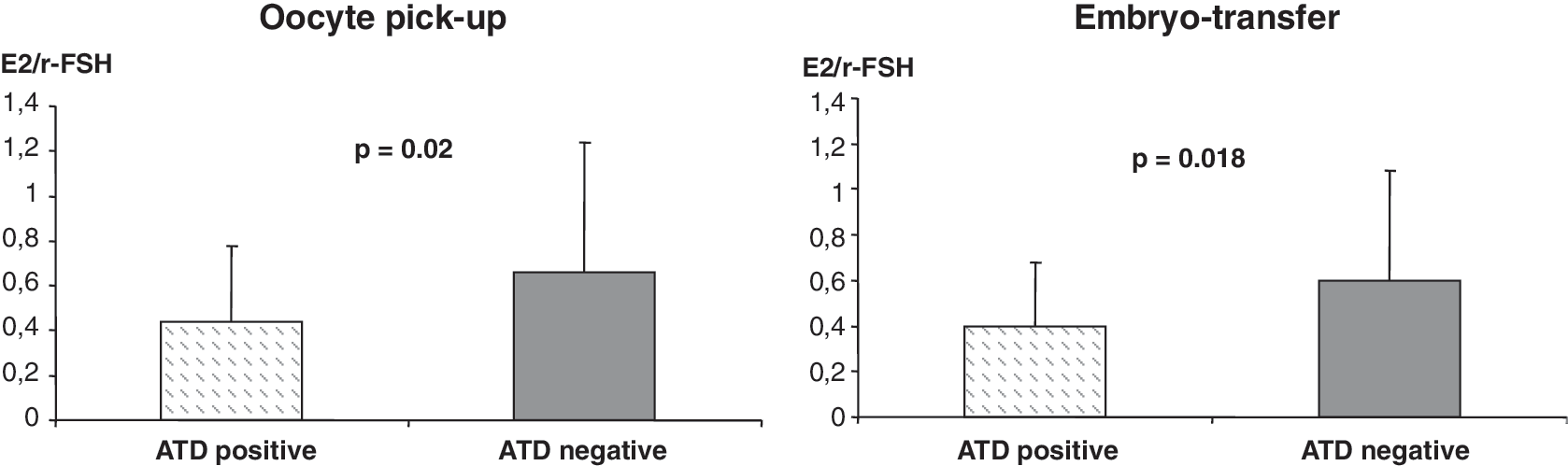
Ratio between estradiol (E2) plasma levels at the time of oocyte pickup (left panel) and embryo-transfer (right panel) and the total number of recombinant follicle-stimulating hormone (r-FSH) units administered during the controlled ovarian hyperstimulation procedure. Subfertile women are subdivided according to their autoimmune thyroid disease (ATD) status (ATD positive and ATD negative). Data are expressed as mean±SD.
Short-term outcome of COH in ATD-positive and ATD-negative women subdivided according to their serum TSH level
We further analyzed the short-term outcomes of COH in ATD-positive women subdivided according to their serum TSH concentration (i.e., greater or less than 2.5 mIU/L). As shown in Figure 2A, ATD-positive women with serum levels of TSH <2.5 mIU/L at starting COH (n=42, median TSH=1.44, range 0.4–2.39 mIU/L) reached a significantly higher concentration of serum E2 at oocyte pickup. They also had a significantly higher E2/r-FSH ratio than ATD-positive women having a serum TSH >2.5 mIU/L (n=18, median TSH=3.51, range 2.66–4.1 mIU/L). The number of M II oocytes was also significantly higher in women with a serum TSH <2.5 mIU/L than in those with a serum TSH >2.5 mIU/L. The mean values of serum E2 at oocyte pickup, the E2/r-FSH ratio, and the number of M II oocytes did not differ in ATD-negative women with a serum TSH greater (n=44) or less than 2.5 mIU/L (n=158; Fig. 2B). A negative correlation was found between the serum TSH levels and both E2/r-FSH ratio and the number of M II oocytes in ATD-positive women (r=−0.336, p=0.02 and r=−0.434, p=0.001, respectively), but not in ATD-negative women.
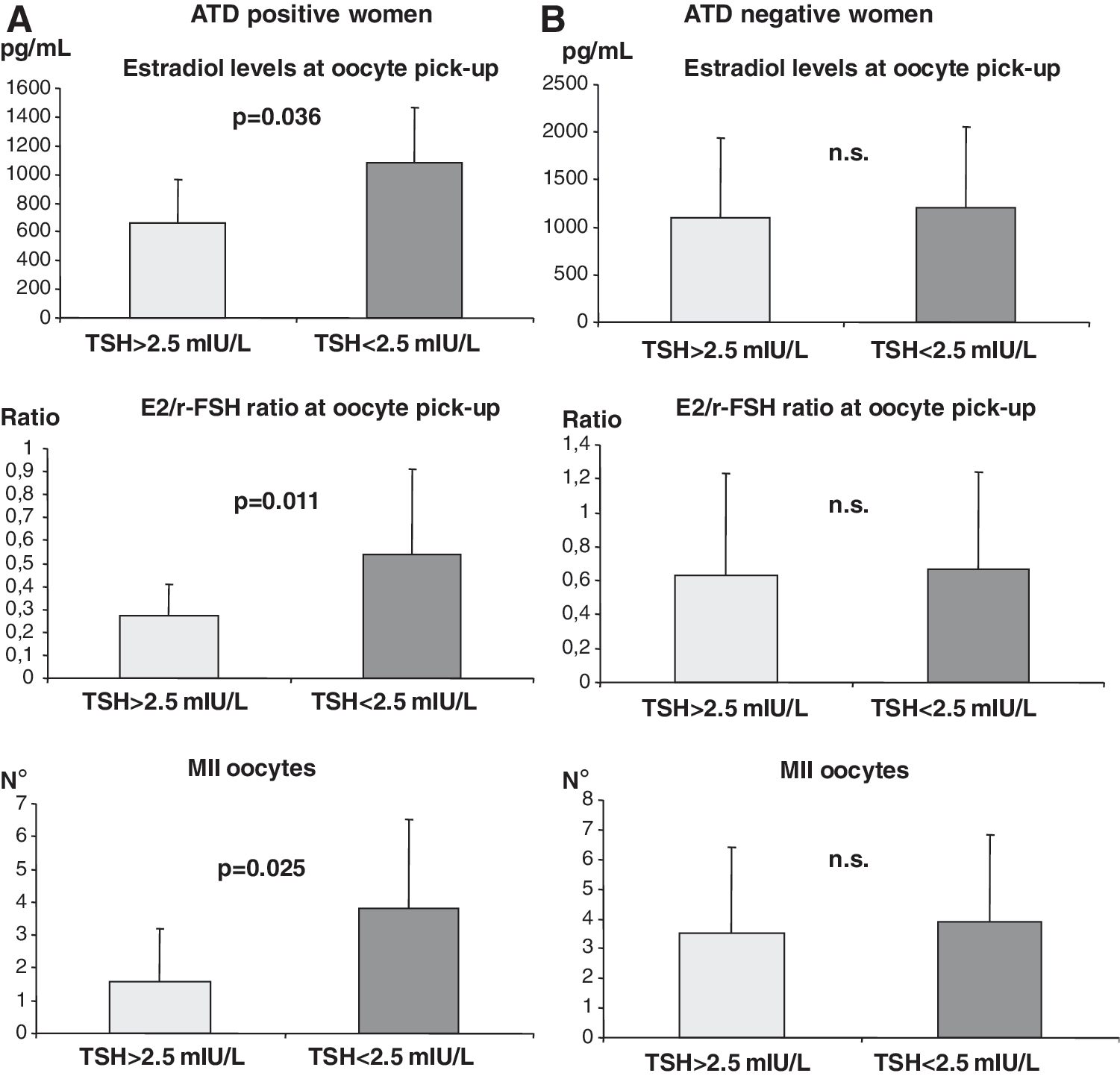
Mean serum levels (±SD) of E2 (top), E2/r-FSH ratio at pickup (middle), and the number of mature metaphase II (MII) oocytes (bottom) in ATD-positive
In a further analysis, ATD-positive women were divided into quartiles according to the distribution of their serum TSH levels. The performance of r-FSH in producing an adequate ovarian stimulation (E2/r-FSH ratio) was progressively and significantly worse when going from the first and second quartiles (corresponding to the lowest serum TSH concentrations) to the third and fourth quartiles (corresponding to the highest serum TSH concentrations; Fig 3, top). A similar trend was found when the number of M II oocytes was considered (Fig 3, bottom).
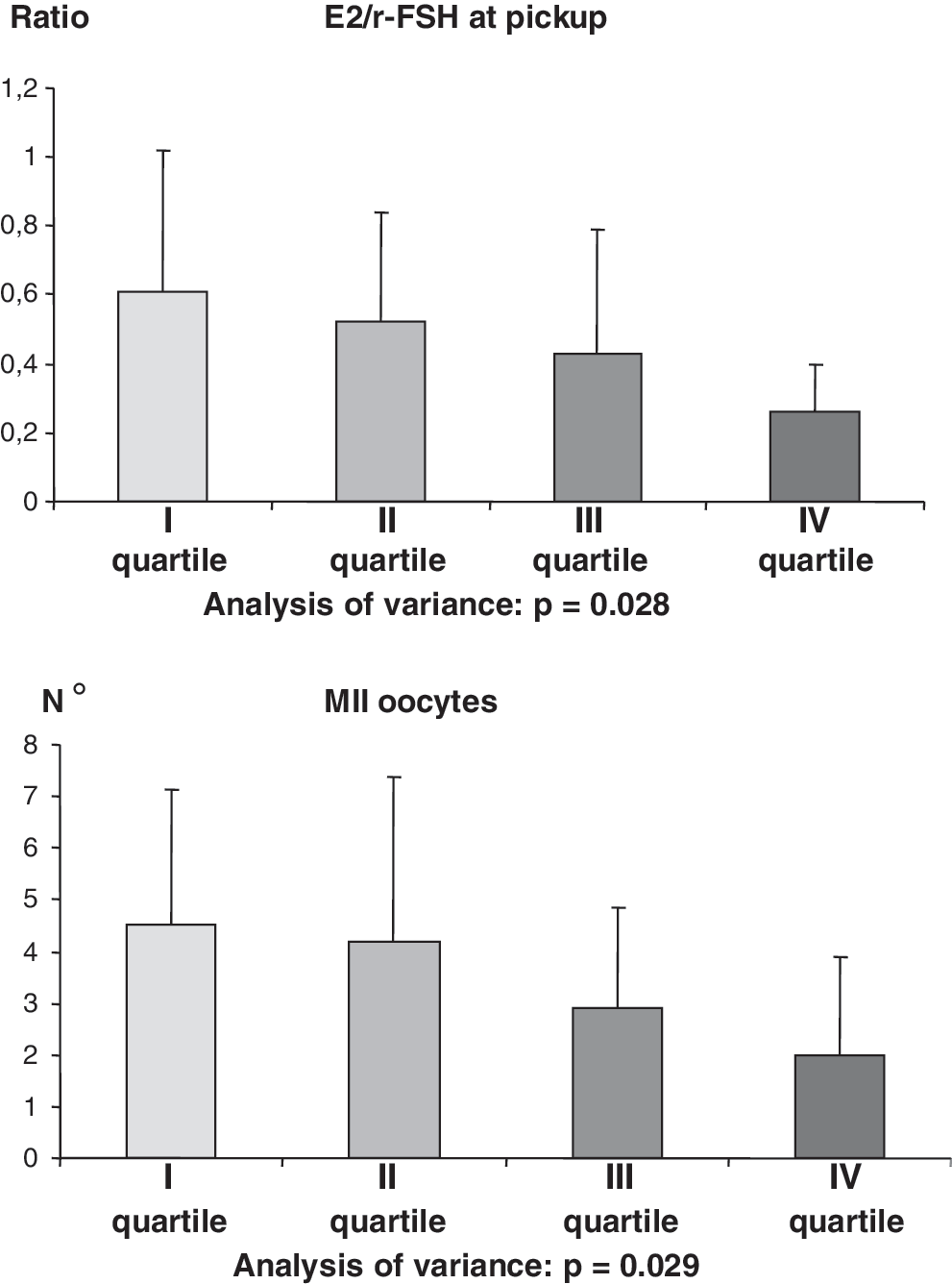
E2/r-FSH ratio (top) and number of MII oocytes (bottom) in ATD-positive women subdivided according to quartiles of distribution of their serum TSH (15 women in each quartile). E2/r-FSH ratio expressed as mean±SD.
There was no difference in the pregnancy rate between ATD-negative (35%) and ATD-positive (28%) women.
Discussion
Currently available data in the literature support the concept that hypothyroidism, even when subclinical, can impair fertility and increase pregnancy-related morbidities (6,23 –26). Overt hypothyroidism and subclinical hypothyroidism occur in 0.5% and in 2–3% of pregnancies, respectively (1,27). Thyroid autoimmunity, as assessed by circulating thyroid antibodies, is the main cause of thyroid failure, and is found in 5–15% of women in their childbearing age (5). It follows that a consistent number of women with ATD may undergo ART in order to conceive. Conversely, the presence of ATD may negatively affect the outcome of ART. Even in the absence of a definitive consensus, probably because of different experimental conditions, timing of observations, and heterogeneity of studied subjects, several studies indicate that the rates of miscarriage and poor pregnancy outcome are increased in women with ATD (16,28,29).
The thyroid autoimmune status and/or thyroid dysfunction may exert a negative impact on ART in different phases (ovarian response to gonadotropin stimulation, oocyte fertilization, embryo development, and implantation), all being crucial for the final outcome. Apart from thyroid diseases, several other biochemical and anatomical factors (altered anatomy of tubes and uterus, endometrial receptivity, thrombophilic status, male factor, and others) may interfere with the success of ART. In order to avoid these possible confounders, we focused our attention on the narrow temporal window starting from ovarian stimulation to oocyte transfer. This allowed us to selectively study the “ovary factor” and, in particular, the ovarian response to r-FSH. We compared two groups of subfertile women with or without ATD, who did not differ for the clinical features (age, BMI, comorbidities) that are recognized as independent risk factors for both naturally occurring and ART-induced pregnancies. The high prevalence of ATD-positive women (22.9%) was considered as a bias related to the high prevalence of ATD-positive women with reduced fertility who undergo ART.
We found that in subfertile women undergoing a standard ART procedure, the presence of ATD is associated with a worse performance of r-FSH, as assessed by the ratio between serum E2 levels and the total number of administered r-FSH units during the COH procedure. This finding suggests that the presence of ATD, even in the absence of overt or subclinical hypothyroidism, may exert a negative influence on the outcome of COH. Our findings agree with previous data linking ATD to a significantly increased risk of reproductive failure after ART (11), and are in line with the notion that patients with recurrent ART failure have a higher incidence of ATD even in the presence of euthyroidism (30,31). Other authors, however, challenged this association and failed to find a difference in ART outcome between ATD-negative or ATD-positive women undergoing ART (28,32).
Many hypotheses have been put forward to explain the link between ATD, infertility, and pregnancy-related morbidities. Both a direct role of anti–thyroid peroxidase antibodies (33) and an indirect role of ATD as a marker of generalized immune imbalance (34) were proposed. ATD may also jeopardize the functional reserve of the thyroid, thus resulting in subclinical hypothyroidism, an established risk factor for maternal and fetal outcomes. For this reason, the recently published Guidelines for Thyroid Dysfunction in pregnancy (6) emphasize the crucial role of preconception serum TSH, and recommend LT4 therapy in women with ATD and associated subclinical hypothyroidism in order to maintain a serum TSH concentration <2.5 mIU/L.
To further investigate this issue, our subfertile women with or without ATD were stratified according to a prestimulation serum TSH concentration higher or lower than 2.5 mIU/L. ATD-positive women with a serum TSH <2.5 mIU/L showed both a better ovarian response to r-FSH and a better oocyte quality (i.e., a higher number of M II fertilizable oocytes) compared with ATD-positive women with a serum TSH >2.5 mIU/L. On the other hand, ATD-positive women with a serum TSH <2.5 mIU/L did not differ for any investigated parameter when compared with the corresponding TSH subgroup of ATD-negative women. These findings underline the crucial role played by thyroid function for the achievement of an adequate oocyte maturation, which is an essential step in physiological conception and becomes even more relevant during a COH procedure (1).
In agreement with our findings, Kim et al. (20), by investigating the outcome of ART-induced pregnancy in patients with subclinical hypothyroidism, found that embryo quality, implantation rate, and live birth were significantly impaired and were ameliorated by LT4 treatment.
In our study, the pivotal role of the prestimulation serum level of TSH was further highlighted when the outcome of COH was compared in ATD-positive women subdivided in quartiles of their serum TSH. We found a significant trend toward a better ovarian response to r-FSH stimulation and a better oocyte quality (i.e., greater production of M II fertilizable oocytes) in ATD-positive women having a serum TSH in the lower quartiles. No such a trend was observed in ATD-negative women.
With the limitation of the retrospective design, our study provides strong evidence supporting the concept that in women with ATD, a pre-COH TSH concentration >2.5 mIU/L can negatively affect the short-term outcome of the procedure. In our study group, only 13% of patients were being treated with LT4. If our results are confirmed in future studies, LT4 substitution may be recommended, according to the ATA guidelines and Endocrine Society and ATA guidelines (5,6), in any woman with circulating thyroid antibodies and a >2.5 mU/L serum TSH who is scheduled for an ART procedure. Another limitation of our study that should be taken into account is the relatively small number of patients included in the subgroups evaluated, emphasizing the need of further studies to confirm our findings.
In conclusion, our findings indicate that the coexistence of thyroid autoimmunity and insufficient thyroid function has a negative effect on the early phase of COH, as assessed by the amount of E2 produced during r-FSH administration and by oocyte quality. This negative effect is no longer evident in ATD-positive women with a serum TSH level corresponding to the lowest quartile of distribution. Our findings strongly support the concept that the negative influence of ATD on the ovarian response during ART may be overcome by administering LT4 substitution treatment to women with a serum TSH >2.5 mU/L. It follows that women undergoing medically assisted reproductive technology should be screened for circulating thyroid antibodies and serum TSH level before undergoing ovarian hyperstimulation.
Footnotes
Acknowledgment
We would like to thank Dr. Alberto Malovini (Lab. Informatica e Sistemistica per la Ricerca Clinica, IRCCS Fond. S. Maugeri, Pavia), for his statistical assistance.
Author Disclosure Statement
The authors have nothing to disclose.