
Abstract

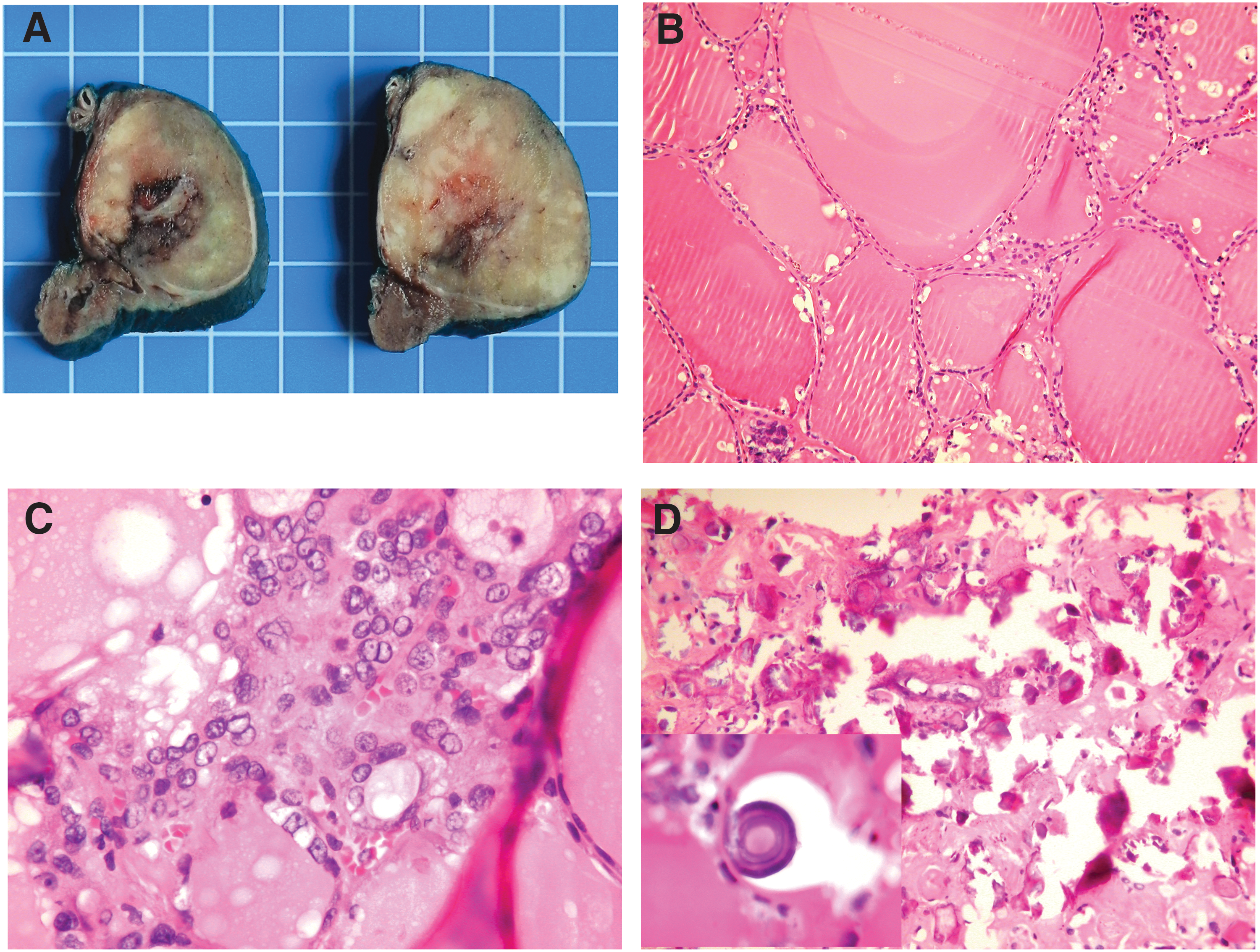
The follicular variant of papillary thyroid carcinoma (FV-PTC) without vascular or capsular invasion is considered to have virtually no metastatic potential or recurrence risk (1). The macrofollicular variant of papillary thyroid carcinoma (MFV-PTC) is a very rare variant of FV-PTC the behavior of which appears to be similar to FV-PTC (2). However, more recently, this phenomenon has been challenged by reports of systemic metastases and recurrent and fatal cases (3). We report a case of encapsulated noninvasive MFV-PTC that presented with gross lymph node metastases, and briefly review the literature. A right thyroid nodule was incidentally found by a computed tomography scan in an 80-year-old male. Subsequently, a 3.7 cm×3.6 cm×3.3 cm heterogeneous iso- to hyperechogenic thyroid nodule in the right lobe and a 2.2 cm×2 cm×1.3 cm right jugular lymph node, both with calcifications, were detected by ultrasonography. Fine-needle aspiration biopsy of both lesions was performed under ultrasonography guidance and showed malignant cells consistent with PTC. The patient underwent a total thyroidectomy with central and right (levels 3–4) lymph node dissection. The thyroidectomy specimen revealed a 3.7 cm×3.2 cm×2.9 cm encapsulated white solid nodule in the right lobe (Fig. 1), which was entirely submitted for histological evaluation. On histology, the nodule was completely surrounded by a thick and focally calcified capsule, without evidence of vascular or capsular invasion. The nodule was predominantly macrofollicular, with minor areas composed of smaller follicles. The cells lining the macrofollicles were often attenuated without significant nuclear atypia (Fig. 1). In contrast, the cells lining the smaller follicles were more cuboidal and had the typical nuclear features of PTC (Fig. 1). Numerous intratumoral calcifications and psammoma bodies were observed (Fig. 1). Insular/solid growth, necrosis, or mitotic activity was not observed. Two lymph node metastases were found. The largest one (2.4 cm) was composed predominantly of macrofollicles, akin to the primary tumor (Fig. 1). Immunohistochemistry was supportive of malignancy, with the tumor cells being diffusely positive for galectin-3, and focally positive for HBME-1 (Hector Battifora mesothelin-1) in the non-macrofollicular areas only. The proliferative index (Ki-67) in the primary tumor and in the larger metastasis was very low (<1% overall). However, small micro/normofollicular foci were present, where the proliferative index was higher (10% of cells). The result of the B-RAF mutation analysis (exons 11 and 15) in the primary tumor was negative.
Although this metastatic MFV-PTC case was encapsulated, without evidence of vascular or capsular invasion, it had two peculiar morphological features that differ from conventional FV-PTC. First, most of the tumor (>50%) was composed of macrofollicles (>250 μm), corresponding to the arbitrary definition of an MFV-PTC (2). Interestingly, that feature was also retained in the larger lymph node metastasis, but not in the smaller one. In the literature, although several cases of MFV-PTC have presented with lymph node metastasis, most of these cases were either infiltrative and/or associated with vascular invasion (2). In the largest series of MFV-PTC of 29 patients, 6 developed lymph node and 2 developed lung metastasis (2). The metastases occurred in older patients who had insular components, extrathyroidal extension, and vascular invasion. In our case, although the patient was elderly, no other risk factors were identified. To the best of our knowledge, there are two other documented cases of encapsulated MFV-PTC without capsular or vascular invasion with lymph node and/or systemic metastasis (3). In comparison, we found no well-documented cases of conventional encapsulated noninvasive FV-PTC with lymph node metastases. In the study by Liu et al. (1), the only encapsulated FV-PTC with lymph node metastasis had several foci of lymphovascular invasion. Moreover, observing that most cases of FV-PTC with metastatic disease had obvious invasion, Lloyd et al. (4) recommend caution in making a diagnosis of FV-PTC in the absence of the major histopathologic features or obvious invasive growth. However, as demonstrated in this case, the application of this recommendation for encapsulated noninvasive MFV-PTC may be questioned.
Second, the primary tumor had numerous psammoma bodies and stromal and capsular calcifications. These features have very rarely been reported in MFV-PTC (2). Very few studies related psammoma bodies and calcifications to frequencies of metastases and survival in patients. Moreover, no data are available on PTC variants such as FV-PTC or MFV-PTC. Bai et al. (5) found that in classical PTC the presence of psammoma bodies and calcifications was significantly correlated with gross lymph node metastasis. Stromal calcification was associated with advanced age (>60 years). Our case of MFV-PTC also exhibits these findings. In conclusion, MFV-PTC is a rare variant of FV-PTC, which may present with gross lymph node metastasis even in the absence of adverse features such as capsular or vascular invasion. Further studies are required to determine whether MFV-PTC behaves differently from FV-PTC.