
Abstract
Background:
The effects of moderate variations in dietary iodine intake on maternal and fetal thyroid function are poorly understood. Recent studies question the usefulness of neonatal screening of congenital hypothyroidism as a tool for monitoring iodine deficiency. We proposed to test the hypothesis of an association between iodine intake during the last trimester of pregnancy and fetal thyroid function at the time of birth.
Methods:
The study was undertaken at term in 233 healthy pregnant women (29.7±5.6 years) and in their newborn. Inclusion of women in the study was done within the 24 hours before delivery.
Results:
The median maternal urinary iodine concentration was 126.5 μg/L. The maternal free triiodothyronine (FT3), although not thyrotropin (TSH) and free thyroxine (FT4), correlated significantly with the urinary iodine concentration (r=0.17, p=0.013). The cord blood TSH, FT4, and FT3 correlated positively with the maternal urinary iodine concentration at the time of delivery (r=0.24, p=0.001; r=0.16, p=0.032; and r=0.24, p=0.003, respectively). The cord blood and heel blood TSH correlated positively with the amniotic fluid iodine concentration (r=0.21, p=0.015 and r=0.15, p=0.036). The cord blood TSH correlated positively with the cord blood FT4 (r=0.21, p=0.022) and FT3 (r=0.32, p=0.017). The maternal TSH correlated significantly with the cord blood TSH (r=0.22, p=0.014) and with the heel blood TSH (r=0.13, p=0.050).
Conclusions:
The results of this study show the presence of a positive association of TSH-FT4 at the time of delivery, which may be modulated by the amount of iodine consumed by the mother during pregnancy.
Introduction
A
In 2007, the WHO established a series of recommendations to improve the intake of iodine in pregnant women (6). These WHO recommendations have stimulated the implantation of policies concerning iodine prophylaxis and/or the incorporation into clinical practice of the administration of iodine supplements for pregnant women. However, the clinical experience with iodine supplementation has produced inconsistent results (7 –10), such that the amount of dietary iodine to be consumed during pregnancy is still being determined.
One of the commonly used biochemical indicators to determine the magnitude of iodine deficiency in the population is the neonatal thyrotropin (TSH), mean values of which are raised in populations with iodine deficiency, thus reflecting a deficit in fetal thyroid function. Recent studies, though, have questioned the usefulness of neonatal screening of congenital hypothyroidism as a tool for monitoring iodine deficiency (11). Indeed, some studies have found that children of mothers who received iodine supplements in populations with mild to moderate iodine deficiency have higher cord blood TSH values (8,10,12), an observation not concordant with the expected direct relation between iodine deficiency and neonatal TSH values. Likewise, another controversial effect seen in some studies concerns the elevation of maternal TSH in women who received iodine-enriched multivitamin complexes (9,13).
Up to now most attention has been placed on the study of thyroid function and its relation with iodine intake during the early months of pregnancy, with just a few studies examining thyroid function in humans at the end of pregnancy. However, this is a particularly important time as it is immediately before the biological disconnection between the mother and the fetus. Various bodies of evidence suggest that the maternal thyroid hormones play an important role in fetal development toward the end of pregnancy. This hypothesis is supported by different studies highlighting the passage of significant amounts of thyroxine (T4) and triiodothyronine (T3) from the mother to the fetus (14), as demonstrated by the fact that infants with congenital athyreosis treated soon after birth do not have the neuropsychomotor complications associated with severe thyroid hormone deficiency (15).
Given this background, we proposed to test the hypothesis of an association between iodine intake during the last trimester of pregnancy and fetal thyroid function at the time of birth.
Materials and Methods
Study subjects
The study was undertaken in 233 consecutive healthy pregnant women at the Carlos Haya Regional University Hospital, Malaga (Spain), at term, after verifying that the inclusion criteria for the study were met. Inclusion in the study was done within the 24 hours before delivery. All the women underwent an obstetric examination and fetal ultrasonography to confirm the absence of any disorders, either maternal or fetal. Criteria for exclusion included the presence of maternal and/or fetal disorders that might represent an obstetric or perinatal risk and elective cesarean deliveries. Pregnant women with a known history of thyroid dysfunction or taking thyroid hormone or antithyroid drugs were also excluded. The women were specifically asked about their intake of iodized salt or supplements containing iodine during the pregnancy. No iodinated skin cleansers were used in the vagina or during cesarean deliveries. During the active phase of the delivery, all the women provided samples of blood and urine, and 193 women provided a sample of amniotic fluid at the time of amniorrhexis.
During delivery, a sample of cord blood was obtained from 161 of the newborns. Measurements were made of cord blood pH. The usual immediate postpartum neonatal variables (Apgar and somatometry) were determined. A heel blood sample was taken from 227 of the newborns during the first 48 hours after delivery and dried on filter paper. All the samples (except for the heel blood samples) were stored at −80°C until the analysis.
The study was approved by the Ethics and Clinical Investigation Committee of Carlos Haya Hospital and written informed consent was obtained from all the participants. This work complies with the principles laid down in the Declaration of Helsinki. As the study included taking samples from minors, the parents also provided signed informed consent.
Laboratory procedures
The TSH, free T3 (FT3), and free T4 (FT4) in the blood of the mother and the cord of the newborn were measured by chemiluminescence (Roche Diagnostics, Basel, Switzerland). For TSH, the low, medium, and high coefficient of variation (CV) value was 7.2%, 4.5%, and 4.1%. For FT4, the low, medium, and high CV value was 8.0%, 7.5%, and 8.0%. For FT3, the low, medium, and high CV value was 10.0%, 5.0%, and 1.9%. Anti-thyroid peroxidase (anti-TPO) antibodies were measured by a radioimmunometric assay (Biocode S.A., Liege, Belgium). Anti-TPO were considered positive if the titer was >50 IU/mL. Heel human TSH was measured by a solid-phase, two-site fluoroimmunometric assay (AutoDELFIA Neonatal hTSH; Perkin-Elmer, Zaventem, Belgium) using the 1235 AutoDELFIA (Perkin-Elmer). The intra-assay CV was 6.1% (low value) and 5.2% (high value), and the interassay CV was 9.0% (low value) and 6.7% (high value). The iodine concentration in urine and amniotic fluid samples was measured by the modified Benotti and Benotti technique (16,17).
Statistical analysis
The quantitative variables were measured as the mean±standard deviation and the qualitative variables as percentages. The contrast hypothesis for two samples was evaluated with the Student's t-test. The contrast hypothesis for more than two samples was determined with an analysis of variance (ANOVA) test. In the event that the variables did not adjust to normality, a Kruskall–Wallis test was done. For adjustment of the model for other variables, two- or multi-way ANOVAs were designed, introducing the continuous variables as covariables. The correlation between variables was determined using the Spearman test, designing multiple linear regression models in those cases where it was desired to predict the variance adjusted for other variables, besides the main variable. In all cases the rejection level for a null hypothesis was α<0.05.
Results
Clinical and anthropometric variables of the mother and the newborn
The mean age of the 233 women was 29.7±5.6 years. Tables 1 and 2 show the other maternal and newborn variables. All the newborns weighed >2000 g at birth. Of the 233 newborns, 47.1% were girls.
FT3, free triiodothyronine; FT4, free thyroxine; TPO, thyroid peroxidase; TSH, thyrotropin.
Iodine intake
The mean urinary iodine concentration (UIC) is shown in Table 1, and the median was 126.5 μg/L (95% confidence interval [133.9–160.4 μg/L]). Of all the mothers, 42.2% reported having consumed iodized salt during the pregnancy; 72.6% took KI supplements daily throughout gestation, and 20.2% took multivitamin supplements containing KI daily throughout gestation. Only 5.3% of the women (n=10) had taken neither iodized salt nor iodine-containing supplements. About 37.1% of pregnant women had a UIC <100 μg/L, 23.1% had a UIC between 100 and <150 μg/L, 26.4% had a UIC between 150 and <250 μg/L, 11.1% had a UIC between 250 and <400 μg/L, and 2.3% had a UIC ≥400 μg/L.
The iodine concentration was also measured in the amniotic fluid from 193 women. The iodine concentration in the amniotic fluid was 14 times lower than that in the urine, showing a significant positive correlation (r=0.24, p=0.003). ANOVA analysis for UIC groups (<100, 100–149, 150–249, 250–499, and >500 μg/L) showed significant differences in iodine concentration in amniotic fluid (12.12±8.33, 11.55±4.90, 13.52±6.01, 16.98±6.13, and 17.52±5.64 μg/L, respectively) (p=0.018). Also, significant differences were found for UIC between low (≤12 μg/L) and high (>12 μg/L) iodine concentrations in the amniotic fluid (UIC=126.2 μg/L vs. 165.3 μg/L, respectively) (p=0.006). However, the number of hours fasting before delivery and the collection of the biological samples correlated negatively with the UIC (r=−0.17, p=0.013). The iodine concentrations in the urine and in the amniotic fluid did not differ significantly according to the intake of iodized salt or iodine-containing supplements, even after correcting for the number of hours fasting (data not shown).
Maternal thyroid function
The maternal values of TSH, FT4, and FT3 are summarized in Table 1. Of the study sample, 30 (15%) of the women had a TSH >5 μIU/mL. No significant differences were found in the maternal FT4 and FT3 between women with TSH ≤5 and women with TSH >5 μIU/L (data not shown). As expected, the FT3 and FT4 values correlated positively (r=0.41, p<0.0001). However, the maternal TSH values did not correlate significantly with the FT3 (r=0.02, p=0.809) or the FT4 (r=0.09, p=0.209). Five women had positive anti-TPO antibodies (>50 IU/mL). The maternal thyroid function at the time of delivery did not differ significantly in the anti-TPO antibody-positive cases (data not shown). The maternal thyroid function at the time of delivery did not correlate significantly with the number of hours fasting before delivery (Table 3).
UIC, urinary iodine concentration.
Neonatal thyroid function
The cord blood concentrations of TSH, FT4, FT3, and anti-TPO antibodies are shown in Table 2. The cord blood TSH and FT4 correlated with the cord blood pH (r=−0.19, p=0.032; and r=0.18, p=0.041, respectively).
The cord blood TSH correlated positively and significantly with the cord blood FT4 (r=0.21, p=0.022) (R 2=0.14, after adjusting for the cord blood pH, maternal UIC, and gestational age). Likewise, the cord blood TSH correlated positively with the cord blood FT3 (r=0.32, p=0.017) (R 2=0.27, after adjusting for the cord blood pH, amniotic fluid iodine concentration and gestational age). The cord blood FT3 and FT4 correlated significantly (r=0.23, p=0.001).
The cord blood TSH concentrations were significantly higher (p<0.0001) than the TSH concentrations obtained in the heel blood at 48 hours of life (Table 2). In no case was the heel blood TSH above 9 μU/mL. On the other hand, 21 of the newborns had a cord blood TSH above 20 μIU/mL, of whom 7 were above 40 μIU/mL. The correlation between the cord blood TSH and the heel blood TSH was significant (r=0.36, p<0.0001). The degree of contribution to the variance in the heel blood TSH increased slightly when the regression model included the amniotic fluid iodine concentration as well as the cord blood TSH (R 2=0.22). The TSH concentrations in the cord blood and the heel blood were significantly higher in the male newborns (p<0.05 and p<0.0001, respectively).
Correlation between maternal and fetal thyroid function
The maternal TSH concentration in serum was significantly lower than the cord blood TSH concentration (p<0.0001), but significantly higher than the heel blood TSH concentration (p<0.0001) (Tables 1 and 2). The maternal TSH correlated significantly with the cord blood TSH (r=0.22, p=0.014) and with the heel blood TSH (r=0.13, p=0.050).
The cord blood FT4 was significantly higher than the maternal FT4 (p<0.0001) (Tables 1 and 2), showing a significant relation between the two (r=0.27, p=0.002). The cord blood FT3 was significantly lower than the maternal FT3 (p<0.0001), but with no significant relation between the two. Significant correlations were found between maternal FT4/TSH ratio (mean ratio=5.50±3.76) and cord blood FT4/TSH ratio (mean ratio=1.99±1.09) (r=0.28, p=0.001), but not between maternal or cord blood FT4/TSH ratio and UIC or iodine in amniotic fluid (data not shown). The maternal thyroid function at the time of delivery did not correlate significantly with cord blood pH (Table 3).
In three of the five mothers with anti-TPO antibodies >50 IU/mL, the cord blood anti-TPO antibodies concentration was also >50 IU/mL. In no case did the maternal or newborn thyroid function (TSH, FT4, and FT3) differ significantly in the anti-TPO antibody-positive cases (data not shown).
Maternal thyroid function and iodine intake
The concentration of maternal thyroid hormones or TSH at the time of delivery did not differ significantly according to the consumption of iodized salt or KI during the pregnancy. The maternal TSH, though, correlated positively (but not significantly) with the UIC (r=0.13, p=0.063). The maternal FT3 correlated significantly with the UIC (r=0.17, p=0.018) and showed significant differences between UIC ≤100 μg/L and UIC >100 μg/L groups (4.74±0.58 vs. 4.94±0.67 pg/mL, p=0.035). The FT4 did not correlate significantly with the UIC (r=0.05, p=0.410). No significant differences for maternal TSH and FT4 were found between UIC ≤100 μg/L and UIC >100 μg/L groups (data not shown). Also, no significant differences were found in maternal thyroid function variables in function of iodine concentrations in the amniotic fluid (data not shown).
Newborn thyroid function according to urinary iodine concentration
The cord blood TSH correlated positively with the maternal UIC at the time of delivery (r=0.24, p=0.001) (Fig. 1A) and with the amniotic fluid iodine concentration (r=0.21, p=0.015) (Fig. 1B). The association between the cord blood TSH and the maternal UIC remained significant (p=0.017) (R 2=0.21, after adjusting for the cord blood pH, the weight of the newborn, the maternal TSH, gestational age, and the sex of the newborn). There were significant differences in cord blood TSH between maternal UIC ≤100 μg/L compared to maternal UIC >100 μg/L groups (10.09 μg/L vs. 13.31 μg/L, respectively; p=0.011), and between low (≤12 μg/L) and high iodine concentrations in the amniotic fluid (>12 μg/L) (10.38 μg/L vs. 13.69 μg/L, respectively; p=0.024). No significant differences were found in others newborn thyroid function variables in function of iodine concentrations in urine or amniotic fluid (data not shown). The heel blood TSH correlated significantly with the amniotic fluid iodine concentration (r=0.15, p=0.036). This association remained significant after adjusting for the cord blood TSH and gestational age (p=0.001) (R 2=0.22).
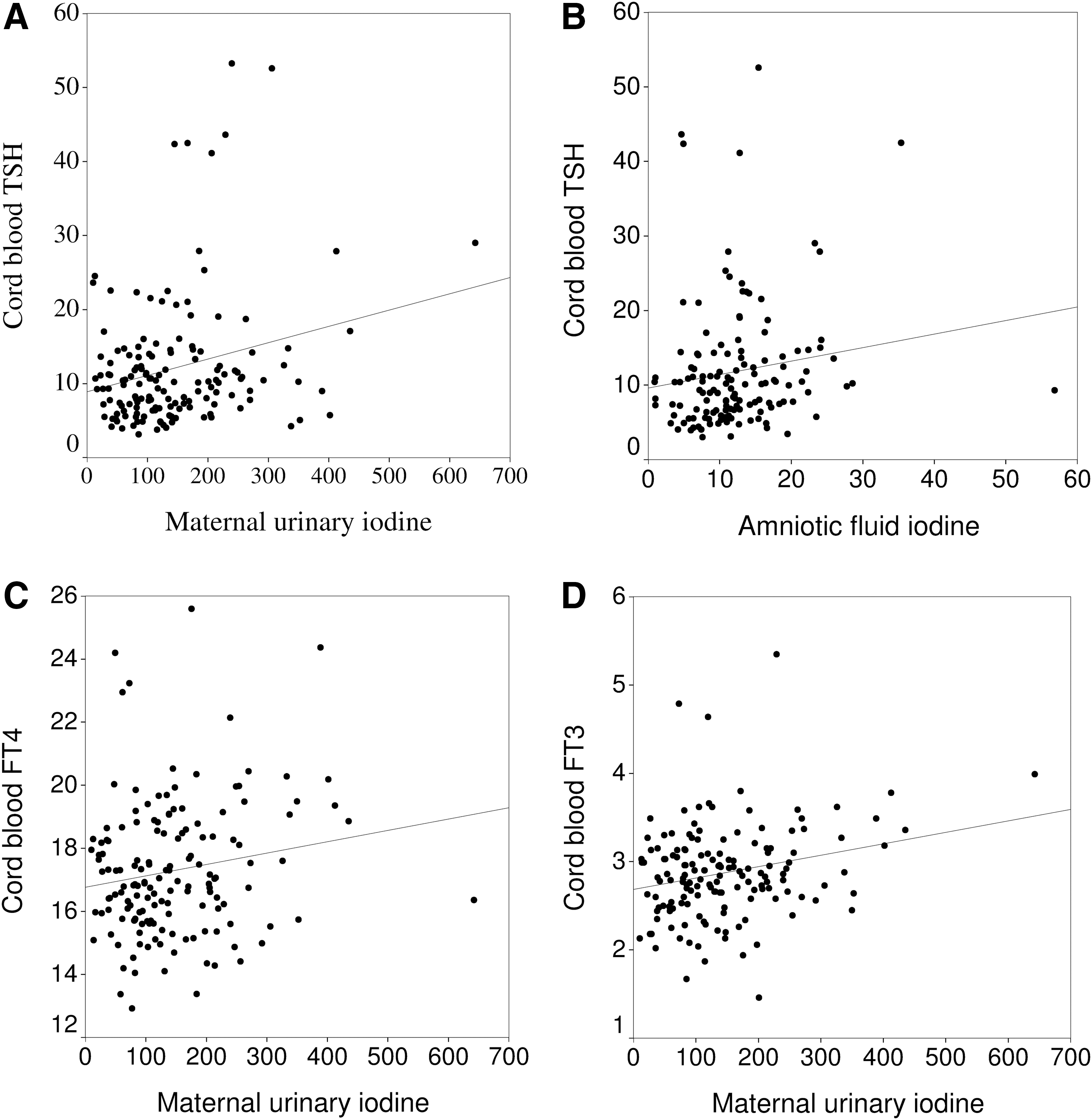
Correlations between the maternal iodine concentration (μg/L) and the cord blood thyroid hormones at the time of delivery.
The cord blood FT4 correlated significantly with the maternal UIC (r=0.16, p=0.032) (Fig. 1C). The correlation remained significant after adjusting for the maternal TSH, cord blood pH, and gestational age (R 2=0.12) (p=0.041), or for the maternal FT4, cord blood pH, and gestational age (R 2=0.16) (p=0.043). Maternal TSH–urinary iodine interaction significantly contributed to the variance of the cord blood FT4 (p=0.004) (Fig. 2), after adjusting for the cord blood pH and gestational age.
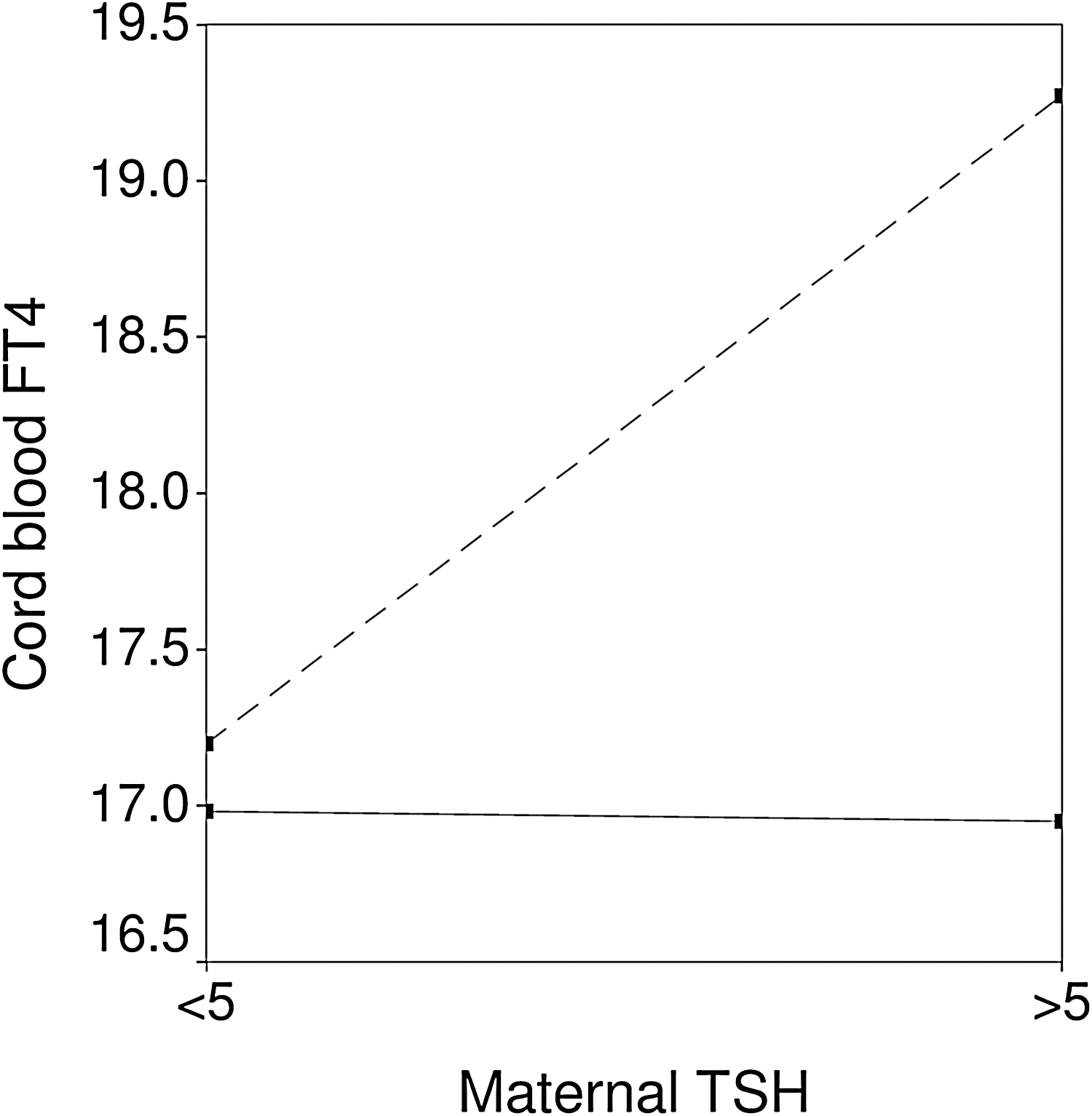
Maternal TSH–urinary iodine interaction significantly contributes to the variance of the cord blood FT4 (pmol/L) (p=0.004): (—) women with urinary iodine concentration ≤100 μg/L; (---) women with urinary iodine concentration >100 μg/L.
The cord blood FT3 correlated significantly with the maternal UIC (r=0.24, p=0.003) (Fig. 1D). This correlation remained significant after adjusting for the maternal or cord blood TSH, for the maternal FT3 or FT4, and for the cord blood pH (p<0.01 in all cases).
Discussion
The most relevant results of this study are as follows: (a) the TSH, FT4, and FT3 in cord blood from newborns correlate positively with the UIC of the mothers, and (b) the TSH, FT4, and FT3 in the cord blood from newborns are positively correlated at the time of delivery, which may be modulated by the amount of iodine consumed by the mother during pregnancy in a moderate-iodine-deficient area (18).
Most studies evaluating the relation between iodine intake during pregnancy and fetal thyroid function have been undertaken in populations with very low or very high levels of iodine intake (2,5). However, the effects of moderate variations in the amount of dietary iodine on maternal and fetal thyroid function in a population with moderate iodine deficiency (19) are less well known (20).
To date, screening programs for congenital hypothyroidism using the measurement of neonatal TSH have suggested that the increase in the number of neonates with moderately elevated TSH concentrations (>5 mU/L in whole blood) is proportional to the degree of iodine deficiency during pregnancy (21). An increase in iodine concentration in iodized table salt markedly improved iodine status of pregnant women in Switzerland (1999–2004), and this improvement was reflected in the reduced frequency of newborn TSH concentration >5 mU/L (22). More recent studies, though, have shown an association between mothers with a greater iodine intake and newborns with higher TSH concentration at the time of birth (8,10,12). Even so, the results are still far from being conclusive. In some cases the neonatal TSH was measured in cord blood and in others in heel blood during the first days of life.
The present study was undertaken in a sample of pregnant women with a median urinary iodine at the time of delivery of 126 μg/L, even though most of the women consumed iodized salt or iodine-containing supplements. This sample of pregnant women was taken from the general Spanish population, who has a median urinary iodine of 117.2 μg/L (urinary iodine/urinary creatinine ratio: 104.2 μg/g) (23). In our study, simultaneous measurements were made not only of the maternal urinary iodine and the iodine in the amniotic fluid at the time of birth, but also of the maternal thyroid function and that of the newborn in cord blood, as well as the heel blood TSH within the first 48 hours of life. In addition, the cord blood thyroid hormone and the heel blood TSH were adjusted for other possible perinatal and intrapartum variables that might interfere with the thyroid function.
In our study, the UIC at the time of delivery was not associated with the form of iodine intake during pregnancy. Most studies, including those by our group undertaken in the same population of pregnant women, have found a clear association between the intake of iodized salt or iodine-containing supplements and the UIC (8) during the three trimesters of pregnancy. Several explanations may exist for the lack of correlation between iodine intake and the UIC in the period immediately before delivery. Only very few women in our study did not consume iodized salt or took iodine-containing supplements. Another factor may be the variable period of fasting before delivery, as shown by the negative correlation between the UIC and the number of hours fasting before delivery.
Only a few studies have examined the iodine concentration in human amniotic fluid in relation to the usual dietary intake of iodine (17). The results of our study show that the amniotic fluid iodine concentration at the end of pregnancy correlates with the maternal UIC. The amniotic fluid iodine concentration is independent of the gestational age (17,24), but is related to UIC (17). Our results of amniotic fluid iodine concentration at the end of pregnancy are similar to the data reported by Rayburn et al. (24), and similar to that found during the second trimester of pregnancy (17), confirming the selective transplacental iodine uptake already established early in pregnancy that persists until delivery.
In our study, the TSH in cord blood correlated with the heel blood TSH, which is well known (25,26). In addition, the cord blood TSH concentration correlated with the cord blood pH, which is a marker of stress during delivery (27). Although the associations reported are significant, the variation in the different thyroid parameters explained by the variation of pH is small. The effects of the different perinatal factors such as gestational age, asphyxia, or difficulty during delivery (28), and even the sex of the newborn (29), cannot be ignored in the investigation of neonatal TSH concentration and may partly account for the discrepancies in the literature concerning the association between iodine intake and TSH concentration in the newborn. The correlations found between the cord blood pH and the cord blood FT4 (positive) and FT3 (negative) suggest that situations of perinatal stress conditioning a decrease in cord blood pH reduce the availability of FT4 and favor a preferential secretion of FT3 in neonatal blood during the early moments of life.
Maternal thyroid function tests in pregnant women require the use of gestational age-specific reference intervals (30). Several studies have shown that an iodine supply during pregnancy is usually associated with a moderate reduction in TSH and a mild increase in FT4 in pregnant women (7,12). Other studies, though, have detected a mild increase in maternal TSH in pregnant women who consume iodine supplements, with no significant changes in FT4 concentration (9) or with a reduction in the percentage of pregnant women who have hypothyroxinemia (13). In our study, the maternal concentrations of TSH, FT4, and FT3 measured at the time of delivery were not significantly different according to the consumption of iodized salt or KI during the pregnancy.
Surprisingly, the cord blood concentrations of TSH, FT4, and FT3, and to a lesser extent the heel blood TSH, correlated positively with the maternal urinary iodine and with the amniotic fluid iodine concentration, although the variation in the different thyroid parameters explained by the variation in iodine levels is small. These associations were independent of other factors that could induce a rise in TSH concentrations during delivery, as the associations remained after including these factors in the regression models. In addition, an association was also found between the heel blood TSH concentration and the iodine concentration in the amniotic fluid. This paradoxical association between a greater iodine intake during pregnancy and a greater increase in the neonatal TSH has also been found by others (12), as well as in prior studies by our group in pregnant women treated with different doses of KI (8,10).
The intake of iodine in amounts above physiological quantities has an inhibitory effect on both maternal (31) and fetal (32) thyroid function, such that the increase in cord blood TSH found in women who take iodine supplements during pregnancy has been interpreted by some as the consequence of this inhibitory effect (12). Nonetheless, this positive association between the intake of iodine supplements and cord blood TSH concentrations is accompanied by significantly higher cord blood FT4 concentrations, which tends to contradict the above interpretation. In our study, the cord blood concentrations of FT3 and FT4 also correlated positively with iodine intake, an observation also noted in a study in China where the children with a higher water-derived iodine intake had a lower mean serum triiodothyronine and higher serum free thyroxine and serum TSH concentrations (33).
In healthy adults, as a consequence of the negative T4-TSH feedback, both hormones are correlated negatively. However, the TSH regulation mechanisms at the time of delivery are not well known (8,12). The interpretation in most studies is that the increased TSH in women who take more iodine during pregnancy is probably the undesired consequence of the inhibitory effect of iodine on thyroid function (9,13). Other interpretations, though, are also possible. In our study we noted a positive correlation between the maternal and the cord blood TSH and in the cord blood between the TSH and the FT4 and FT3. This positive TSH-FT4 correlation in the cord blood has been reported before (12,34); it is maximal at the time of term delivery, is lower when the prematurity of the newborn is greater (34), and becomes negative as the days pass after the delivery (35). Our result probably just reflects the greater positive effect of TSH on FT4 secretion than the negative effect of FT4 on TSH secretion at this stage, probably as a result of the postnatal TSH surge. This increase in the TSH at the end of delivery may contribute to stimulate the thyroid function of the newborn, which would explain the recently published results finding that the highest maternal TSH concentrations in the second half of pregnancy are associated with better scores on the development test of the children (36).
In summary, the results of this study suggest that the mild increase in TSH in women at the final moment of delivery and in the newborns may be the physiological response of the fetal–maternal unit to guarantee adequate thyroid hormone concentrations, vital for the adequate neurocognitive development of the newborn, rather than the consequence of an inhibitory effect of iodine on the hypothalamic–hypophysary axis. Nevertheless, further studies are needed about the iodine supplement required during pregnancy and its effects on the newborn according to the iodine intake status of pregnant women.
Footnotes
Acknowledgments
We thank Trinidad Ramos-Rodríguez and Cristina Cabo-Simó, midwives of the Gynecology Service, Hospital Regional Universitario Carlos Haya (Malaga), for the technical assistance. This study was undertaken with the aid of a grant from the Consejería de Salud of the Junta de Andalucía (PI-0501/2009 and PI-0373/2012). CIBER de Diabetes y Enfermedades Metabólicas asociadas and CIBER de Fisiopatología de la Obesidad y Nutrición are Instituto de Salud Carlos III (ISCIII) initiatives.
Author Disclosure Statement
No competing financial interests exist.