
Abstract
Background:
Clinical thyroid disease is associated with changes in the cardiovascular system, including changes in heart rate during exercise. However, data on the relation between subclinical thyroid disease (SCTD) and heart rate during exercise are limited.
Methods:
We investigated 3799 apparently healthy subjects who were evaluated in the Institute for Preventive Medicine at the Sheba Medical Center. All subjects answered standard health questionnaires; were examined by a physician; completed routine blood tests including thyrotropin, free triiodothyronine, and free thyroxine levels; and underwent a treadmill exercise according to the Bruce protocol. Subjects with known thyroid disease or those who were taking thyroid-related drugs were excluded from the analysis. Heart rate profile was compared between patients with subclinical hypothyroidism (SCHypoT), patients with normal thyroid function, and patients with subclinical hyperthyroidism (SCHyperT) using propensity score matching.
Results:
Seventy patients had SCHyperT and 273 had SCHypoT. Compared with age- and sex-matched normal subjects, SCHyperT subjects had a higher resting heart rate (83±17 vs. 76±12 beats per minute [bpm], p=0.006), a significantly higher recovery heart rate (94±12 vs. 90±12 bpm, p=0.045), and a significantly lower heart rate reserve (80±20 vs. 87±18 bpm, p=0.006). Subjects with SCHypoT showed a trend toward a lower resting heart rate (75±13 vs. 77±15 bpm, p=0.09) and had a significantly lower recovery heart rate (88±12 vs. 90±13 bpm, p=0.035). There was no significant difference in exercise duration or blood pressure between subjects with SCTD and their matched normal controls.
Conclusions:
Subjects with SCTD have a significantly different heart rate profile during rest, exercise, and recovery.
Introduction
The cardiovascular system is a major target for thyroid hormone action (4,5). Heart rate, cardiac output, and systemic vascular resistance are closely linked to the function of the thyroid gland (6). Previous reports on subjects with subclinical hyperthyroidism (SCHyperT) have shown an increased resting heart rate and left ventricular mass, an increased risk for the development of atrial fibrillation, and an increase in cardiovascular mortality (6 –9). Subclinical hypothyroidism (SCHypoT) was shown to be associated with reduced diastolic function and reduced ejection fraction during exercise (3). However, previous reports have failed to show decreased resting heart rate among SCHypoT subjects.
Data on the correlation between endogenous SCTD and heart rate profile during rest exercise are lacking. We hypothesized that heart rate profile at rest, exercise, and recovery will be correlated with subclinical thyroid abnormalities. Therefore, the aim of the present study was to evaluate heart rate and blood pressure behavior during exercise and recovery among asymptomatic and apparently healthy subjects with SCTD during routine exercise stress tests.
Methods
Study population
The Institute for Preventive Medicine of the Chaim Sheba Medical Center performs approximately 9000 annual examinations. The center population consists mainly of apparently healthy men and women who undergo annual examinations for health screening. The study population was described previously (10,11). In brief, all participants are interviewed at the time of each annual examination using standard questionnaires that gather information regarding demographic characteristics, medical history, and health-related habits (including dichotomous questions concerning current smoking status, and regular physical activity). Thereafter, blood samples are drawn after a 12-hour fast and analyzed immediately. A physician at the center performs a complete physical examination, including blood pressure measurement. All patients undergo a standard exercise stress test each year. A computerized database of all the annual visits in this center was established in the year 2000 and is the source of data for this study.
The Institutional Review Board of the Sheba Medical Center approved this study on the basis of strict maintenance of participants' anonymity during database analyses. Data from patients were recorded anonymously. No individual consent was obtained.
Inclusion and exclusion criteria
The study population comprised men and women who visited the Institute for Preventive Medicine during the years 2000–2011. A total of 4816 unselected patients completed a treadmill exercise test and had complete thyroid function tests (TSH, FT4, and FT3) taken during their first visit to the center at the discretion of the examining physician. Exclusion criteria included: known or suspected thyroid disease, extreme TSH levels (above 10 or below 0.03 mIU/L), the use of thyroid-related drugs, and incomplete exercise stress test data. The final study sample included 3799 patients.
Definition of SCTD
SCHyperT and SCHypoT were defined biochemically. SCHyperT was defined as TSH levels below 0.4 and above 0.03 mIU/L, with normal levels of FT4 and FT3. SCHypoT was defined as TSH levels above 4 and below 10 mIU/L. Laboratory data of all patients with suspected SCHypoT or SCHyperT were reviewed by the last author who confirmed the diagnosis.
Exercise stress test protocol
All patients in the study completed a maximal treadmill exercise test according to the Bruce protocol under the supervision of a board-certified cardiologist. Heart rate was measured and documented before the beginning of the test, at the end of the test, and during recovery (4–5 minutes after the end of the test). Heart rate response was defined as the maximum heart rate divided by the age-predicted maximal heart rate (percentage), and heart rate reserve was defined as the difference between heart rate at rest and during maximal exercise. Additional documented variables included exercise duration (in minutes) and metabolic equivalents (METS), systolic and diastolic blood pressure at rest, at the end of the test and during recovery, and the presence of atrial or ventricular arrhythmias during the exercise.
Statistical analysis
Baseline clinical characteristics and heart rate profile during the exercise stress test were compared between the three study groups (SCHypoT, Normal, SCHyperT) by using either T-test for continuous variables or chi-square test for categorical variables. In order to balance covariates among the three study groups, propensity score matching was used, as previously described by Thoemmes (12). For patients with SCHyperT, a 1:2 nearest neighbor method was used. For patients with SCHypoT, a 1:1 nearest neighbor matching was used. To ensure good matching, a caliper of 0.2 was defined as the maximum allowed difference between two matched participants. The propensity score analysis included the following covariates: age, sex, low-density lipoprotein cholesterol, systolic blood pressure, body–mass index, current smoking status (yes or no), physical activity (yes or no), and recovery time during the end of the exercise. All statistical analyses were performed with SPSS (ver. 20.0) statistical software.
Results
Total study population
Among the study subjects, 3456 (91%) patients had normal thyroid function tests, 70 (1.8%) patients had SCHyperT, and 273 (7.2%) patients had SCHypoT. Baseline characteristics of the three study groups are summarized in Table 1. Age, sex, systolic blood pressure, creatinine and hemoglobin levels, total cholesterol and high-density lipoprotein cholesterol, and personal history of ischemic heart disease were all significantly different among the three study groups. The frequency of women was higher in the SCTD groups than in the normal thyroid group. Mean age was 48±10 years in the normal thyroid group, compared with 49±10 in the SCHyperT group and 52±12 in the SCHypoT group. There were no significant differences among groups with respect to diastolic blood pressure, triglyceride levels, low-density lipoprotein cholesterol levels, the use of beta blockers, smoking status, or physical activity.
BMI, body–mass index; BP, blood pressure; HDL-C, high-density lipoprotein cholesterol; IHD, ischemic heart disease; LDL-C, low-density lipoprotein cholesterol; SCHyperT, subclinical hyperthyroidism; SCHypoT, subclinical hypothyroidism; TSH, thyrotropin.
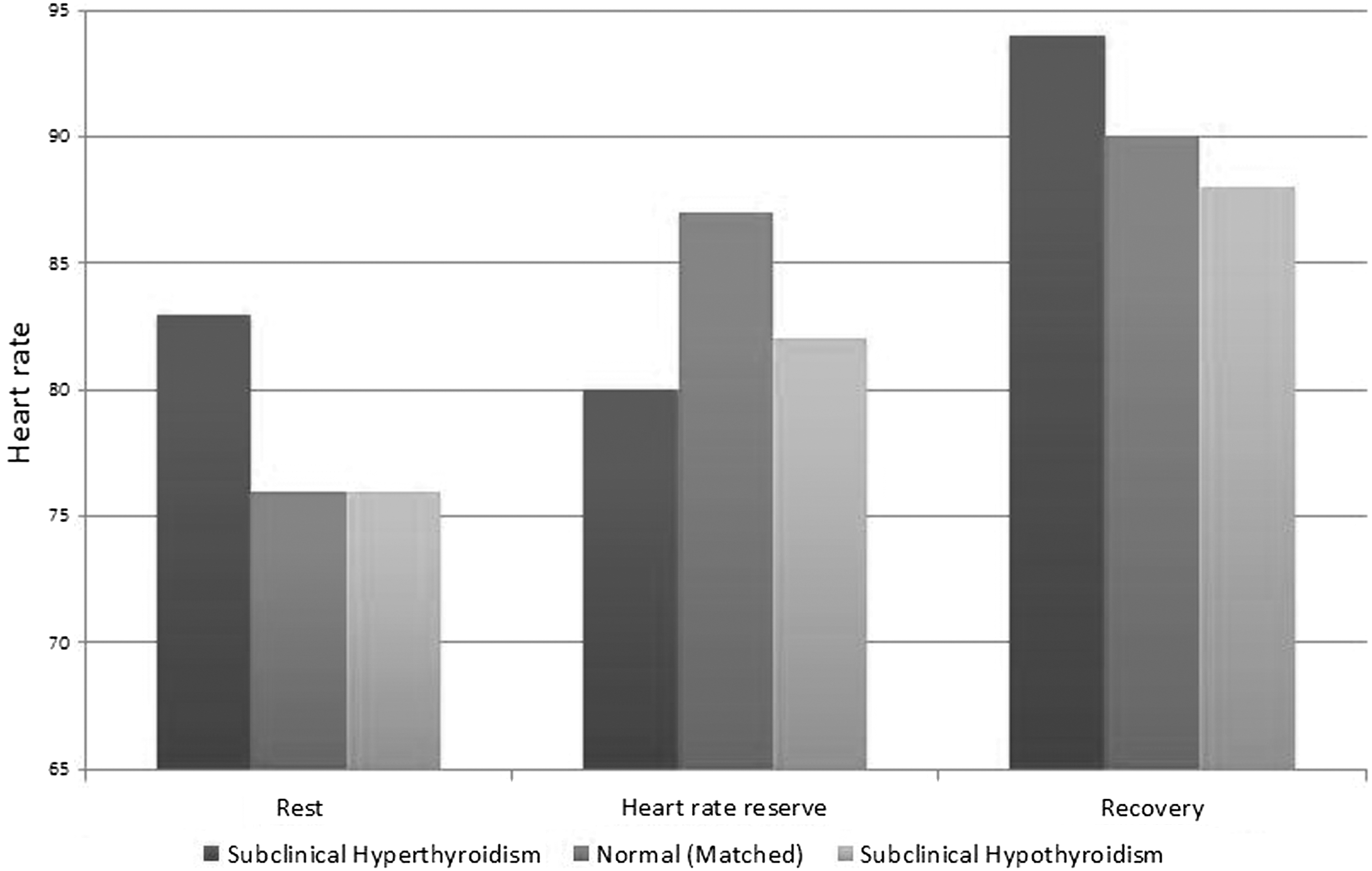
Heart rate profile and the exercise test results of the three study groups are summarized in Table 2. Heart rate at rest, at maximal exercise, and during recovery, as well as heart rate reserve, were all significantly different among the three study groups (Fig. 1). Resting heart rate was 78±14 beats per minute (bpm) in normal subjects, compared with 83±17 and 76±13 bpm in SCHyperT and SCHypoT patients, respectively (p<0.001 for the overall difference among the three groups). Exercise duration, METS, and heart rate response were also significantly different among the three groups. While normal subjects had a mean exercise duration of 588±162 seconds, patients with SCHyperT and SCHypoT completed the exercise after 537±126 and 549±169 seconds, respectively (p<0.001 for the overall difference among the three groups).

Heart rate and blood pressure profiles of the study population. Heart rate profile and blood pressure of the three groups of subjects: Compared with unmatched normal subjects, heart rate (in beats per minute) during rest and recovery was higher and lower in SCHyperT and SCHypoT patients, respectively (top chart). Heart rate reserve was reduced in both SCHyperT and SCHypoT subjects. All differences reached statistical significance (p<0.001 for between study groups). However, there were no differences in systolic or diastolic blood pressures between the three groups of subjects. SCHyperT, subclinical hyperthyroidism; SCHypoT, subclinical hypothyroidism.
bpm, beats per minute; METS, metabolic equivalents.
In contrast, systolic and diastolic blood pressure during exercise and recovery were not significantly different between the study groups.
Propensity score matching
Subclinical hyperthyroidism
Subjects with SCHyperT were well matched with 140 propensity-score-matched subjects with normal thyroid function as shown in Table 3 and Supplementary Figure S1 (Supplementary Data are available online at
Heart rate profile after propensity score matching. Compared with propensity score matched normal subjects, heart rate (in beats per minute) during rest and recovery was higher and lower in SCHyperT and SCHypoT patients, respectively. Heart rate reserve was reduced in both SCHyperT and SCHypoT subjects. All differences between SCHyperT subjects and their matched controls reached statistical significance. Heart rate recovery was significantly different between SCHypoT subjects and their matched controls.
The table shows the baseline characteristics of subjects with subclinical thyroid disease compared with their matched controls. The two left columns show subclinical hyperthyroid subjects compared with their matched normal controls (1:2 matching). The two right columns show subclinical hypothyroid subjects compared with their matched normal controls (1:1 matching). There were no statistically significant differences in baseline characteristics between subclinical hyperthyroid subjects and their matched controls after propensity score matching.
Thyroid function tests were significantly different between SCHypoT and their matched controls and between SCHyperT and their matched controls (p<0.001 for all comparisons).
The only difference between subclinical hypothyroid disease subjects and their matched controls was a slightly lower creatinine level in the matched control population (p=0.014).
The table shows the cardiovascular characteristics of subjects with subclinical thyroid disease compared with their matched controls. The three left columns show subclinical hyperthyroid subjects compared with their matched normal controls (1:2 matching). The three right columns show subclinical hypothyroid subjects compared with their matched normal controls (1:1 matching).
Subclinical hypothyroidism
Subjects with SCHypoT were also well matched with 273 propensity-score-matched subjects with normal thyroid function (Table 3 and Supplementary Fig. S1). Similar to subjects with SCHyperT, subjects with SCHypoT also showed differences from propensity-score-matched normal group, including a trend toward a lower resting heart rate (75±13 vs. 77±15 bpm, p=0.09) and a significantly lower recovery heart rate (88±12 vs. 90±13 bpm, p=0.035). There was no statistically significant difference in heart rate response (94%±7% vs. 95%±6%, p=0.38), heart rate reserve (83±20 vs. 82±20 bpm, p=0.64), exercise duration (549±169 vs. 546±156 seconds, p=0.79), and blood pressure values between the SCHypoT patients and their matched normal controls (Table 4 and Fig. 2).
Discussion
The main finding of the present study is that SCTD is correlated with changes in heart rate profile during rest exercise and recovery. Our results include one of the largest cohorts of patients with endogenous SCHyperT, and it shows that heart rate at rest and during recovery is elevated in SCHyperT patients compared with their matched controls. In addition, our study shows lower heart rate during recovery and a trend toward a lower resting heart rate in patients with SCHypoT. Those differences, however, did not translate into a significant change in exercise capacity among patients with SCTD compared with matched controls.
Subclinical hyperthyroidism and the heart
Data on SCHyperT include studies on exogenous and endogenous states of hyperthyroidism. Data on endogenous SCHyperT are limited and include few studies with a small number of patients in each study (13 –15). In contrast to endogenous SCHyperT, there is more available information on cardiovascular changes in patients with exogenous SCHyperT. In patients treated with TSH-suppressive doses of L-thyroxine, changes in the cardiovascular system include increased heart rate, shorter isovolumetric relaxation time, and higher left ventricular mass (16 –18). In addition, Sawin et al. (19) clearly demonstrated that there is an increased risk for atrial fibrillation in older patients with SCHyperT. Our study is consistent with these previous reports and shows that SCHyperT is not only a biochemically defined state. The SCHyperT group had a higher resting heart rate, a higher heart rate during recovery, and a trend toward a lower heart rate reserve. All these parameters were correlated in the past with poor cardiovascular outcomes (20 –22). This observation is consistent with the work of Parle et al. (7), who showed a higher rate of death from all causes (but especially from cardiovascular disease) among patients older than 60 years with subclinical hyperthyroidism. The American Thyroid Association and American Association of Clinical Endocrinologists Taskforce on Hyperthyroidism therefore recommend the treatment of any individual with SCHyperT older than 65 years if the TSH is <0.1 mIU/L and to consider treatment if the TSH is between 0.1 and 4 mIU/L (23).
Subclinical hypothyroidism and the heart
SCHypoT is relatively common compared with SCHyperT, especially among older women (24). While most studies did not find any correlation between SCHypoT and heart rate or systolic cardiac function at rest, there are data regarding changes in the cardiovascular system associated with SCHypoT, including shortened pre-ejection period, reduced diastolic function, and reduced ejection fraction during exercise (25 –27). Cardiovascular changes in patients with SCHypoT are reversible and tend to disappear with treatment with L-thyroxine (28). Brenta et al. (29) used exercise ventriculography to demonstrate that diastolic dysfunction among subclinical hypothyroid subjects can be reversed by the use of exogenous L-thyroxine.
Our analysis showed significant differences between patients with SCHypoT and their unmatched normal counterparts, including changes in exercise tolerance and heart rate profile during exercise and recovery. However, after using propensity score matching to adjust for all significant covariates (including age and sex), only heart rate during rest and recovery remained different between SCHypoT and normal subjects. Our results are consistent with previous reports showing changes in the cardiovascular physiology of SCHypoT patients. However, to our knowledge the present study is the first to show significant changes in heart rate recovery among subjects with SCHypoT. Biondi et al. (25), in a comprehensive review of the literature of SCTD, showed that although studies focusing on SCHypoT did find changes in cardiovascular physiology of SCHypoT patients, none found changes in resting heart rate among these patients. The differences between prior reports and the present study may be due to less rigorous selection of patients (we excluded patients with known thyroid disease), or to the use of different diagnostic criteria (different range of TSH values).
Another surprising finding in our analysis was the lack of difference in the exercise capacity among patients with SCHypoT compared with normal subjects. Previous studies have clearly shown impaired diastolic and systolic function among patients with SCHypoT, which should have resulted in poor exercise tolerance. In our analysis, SCHypoT subjects had a shorter exercise duration time (588 vs. 547 seconds) and lower METS compared with normal patients, but the difference did not remain significant after propensity score matching, suggesting that SCHypoT per se did not affect exercise capacity among study subjects.
Study limitations
Despite being one of the largest studies focusing on heart rate profile of subjects with endogenous SCTD, the analysis is still underpowered with respect to minor changes in heart rate profile and exercise capacity. In addition, our study has several other limitations. First, this is a retrospective observational study and therefore there are risks of selection bias and residual confounding despite validation analyses using propensity-score matching. Second, the study consisted of mainly Jewish, relatively young and healthy individuals from a high-socioeconomic-background population. This might limit the validity of our conclusions to other populations. Third, the cause and duration of the thyroid disease were not evaluated in this study. Lastly, this study is based on the analysis of heart rate profile and did not include evaluation of subjects' physical fitness. Therefore, our results might be affected by the functional capacity and physical fitness of this relatively healthy population, although we did adjust for regular physical activity, resting heart rate, and METS during maximal exercise in the multivariate model.
Conclusions and clinical implications
We have shown that healthy subjects with SCTD have a significantly different heart rate profile during rest and recovery. Both parameters were previously shown to be associated with adverse long-term cardiovascular outcomes, suggesting that careful observation is warranted in this population.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.