
Abstract
Background:
Levothyroxine has been shown to enhance pregnancy outcomes in women with hypothyroidism requiring in vitro fertilization (IVF). However, the precise magnitude of these benefits remains to be determined. In particular, it has yet to be clarified whether levothyroxine may fully overcome the detrimental effects of hypothyroidism or, conversely, whether affected women remain at reduced prognosis for pregnancy outcomes.
Methods:
Patients who underwent IVF–intracytoplasmic sperm injection (ICSI) over a 3-year period were reviewed. Cases were deemed eligible if they were diagnosed with clinical or subclinical hypothyroidism and were receiving levothyroxine. Controls were two subsequently age-matched euthyroid women for every case. Both cases and controls were selected only if serum thyrotropin was ≤2.5 mIU/L.
Results:
In total, 137 women with treated hypothyroidism and 274 controls were included. Baseline characteristics of the two study groups were similar with the exception of body mass index, which was slightly higher among the cases (22.9±3.9 vs. 21.9±3.3 kg/m2, p=0.013). Most IVF-ICSI cycle outcome variables were also similar, with the exception of a higher rate of cancellation for poor response (3.6% vs. 0.7%, p=0.04), a longer duration of stimulation (10.9±2.2 vs. 10.1±2.0 days, p=0.001), a higher proportion of women failing to obtain viable embryos (17% vs. 7%, p=0.006), and a lower fertilization rate (75% vs. 86%, p=0.017) among cases. Conversely, the clinical pregnancy rate per started cycle, the implantation rate, and the live birth rate per started cycle did not differ; they were 36% and 34% (p=0.93), 28% and 22% (p=0.11), and 30% and 27% (p=0.50) in cases and controls, respectively. Subgroup analyses comparing women with (n=79) and without (n=58) thyroid autoimmunity and comparing women who were diagnosed with overt hypothyroidism (n=70) or subclinical hypothyroidism (n=67) failed to identify relevant differences.
Conclusions:
In our population, IVF-ICSI outcome was not significantly hampered in women with adequately treated hypothyroidism. The magnitude of the detected differences in cycle outcome was mild, and we failed to document any differences for the most relevant outcomes, i.e., pregnancy rate, implantation rate, and delivery rate. In conclusion, adequate levothyroxine treatment maintaining thyrotropin serum levels below 2.5 mIU/L may overcome the detrimental effects of hypothyroidism.
Introduction
A large body of literature has demonstrated the wide benefits of levothyroxine in the treatment of hypothyroidism-associated symptoms. Considering specifically reproductive health, levothyroxine has been shown to restore a normal menstrual pattern and to normalize luteinizing hormone pulsatility and prolactin levels (1). Moreover, this treatment has recently been documented to lower the risk of miscarriage and preterm birth (3). Overall, there is a general consensus that levothyroxine should be offered to women with clinical hypothyroidism (1,3). Conversely, even if it is plausible that levothyroxine may also be of benefit in women with subclinical hypothyroidism or thyroid autoimmunity, the data available are presently insufficient to definitely recommend its use in these conditions (3).
The impact of hypothyroidism in the context of the in vitro fertilization–intracytoplasmic sperm injection (IVF-ICSI) cycle has received less attention, but, not surprisingly, available evidence generally supports the view that an optimal thyroid function is required to optimize the rate of success. A recent randomized controlled trial demonstrated that levothyroxine may enhance pregnancy and implantation rates in women with subclinical hypothyroidism (4). On the other hand, the magnitude of these benefits has been questioned by Kilic et al. (5) and Scoccia et al. (6), who documented a worse IVF outcome in women with treated hypothyroidism, suggesting that levothyroxine is unable to fully overcome the detrimental effects of this condition. These studies, however, had some important methodological limitations and the question remains open (7).
In this study, we deemed it of interest to further investigate the chances of success in women with adequately treated hypothyroidism undergoing IVF. Clarifying this aspect is of the utmost relevance for better counseling affected women and for guiding further research in this area. Notably, if a detrimental effect emerged, researchers would be called to ideate and investigate new therapeutic approaches for this condition.
Materials and Methods
Patients who were selected for IVF-ICSI between January 2009 and December 2011 at the Infertility Unit of the Fondazione Ca’ Granda Ospedale Maggiore Policlinico were reviewed. Women were deemed eligible as cases if they were diagnosed with clinical or subclinical hypothyroidism and were receiving levothyroxine. Controls were subsequently age-matched (±1 year) euthyroid women who had never been on therapy with levothyroxine. They were matched to cases in a 2:1 ratio. Additional eligibility criteria for both groups included (a) age <40 years, (b) no previous IVF-ICSI cycles, (c) serum free triiodothyronine and free thyroxine values within the normal range, and (d) serum thyrotropin (TSH) tested the month preceding the IVF cycle ≤2.5 mIU/L (1). Patients who underwent either classical IVF or IVF-ICSI were included. This analysis exclusively refers to the first treatment cycle. The local Institutional Review Board approved the study. All women undergoing IVF in our unit are informed about the necessity to contact the unit after the scheduled time of delivery to obtain data on pregnancy course (according to Italian legislation) and they routinely sign an informed consent for the use of their data for research purposes.
All patients underwent transvaginal ultrasound between day 1 and day 8 of the cycle during the month preceding the beginning of hyperstimulation. Data on the history of thyroid disorders were collected at this time. Women who were already on levothyroxine therapy at the time of assessment for study entry could be included. Serum TSH was systematically tested at this time, and if it was found higher than the threshold value of 2.5 mIU/L, it was measured again. If the value was confirmed above the threshold, the patient was referred to an endocrinologist who set or adjusted the appropriate levothyroxine treatment. After a period established by the endocrinologist on the basis of the underlying condition, a control assessment of serum TSH, free triiodothyronine, and free thyroxine was performed. If all three analyses were within the normal range, the patient could start with controlled ovarian hyperstimulation. During the IVF cycle, serum TSH was not assessed and the levothyroxine dose was not adjusted.
Patients were monitored and managed according to a standardized clinical protocol as reported in detail elsewhere (8). Briefly, the protocol of stimulation and the dose of recombinant follicle-stimulating hormone (Gonal-F; Merck Serono) were determined on an individual basis according to characteristics of the patients such as age, serum hormonal levels, and antral follicle count. Patients underwent serial transvaginal ultrasonography and hormonal monitoring during hyperstimulation. When three or more leading follicles with a mean diameter >18 mm were observed, 250 μg of recombinant human chorionic gonadotropin (hCG) (Ovitrelle; Merck Serono) was administered subcutaneously. Oocyte retrieval was performed transvaginally 36 hours after hCG injection. Embryo transfer was performed 48–72 hours after oocyte collection. Cycles were canceled if there was a poor or hyper-response. We defined hyper-response as a serum estradiol level >4000 pg/mL and/or more than 20 follicles identified on ultrasonography scan before hCG administration. Poor response was defined by echographic evidence of fewer than three follicles during ovarian hyperstimulation. Serum hCG assessment to ascertain the development of pregnancy was performed at +16 days from hCG administration. Clinical pregnancy was defined as ultrasonographic demonstration of a vital embryo within an intrauterine gestational sack 4–5 weeks after embryo transfer. The implantation rate was calculated as the ratio between the number of gestational sacks identified at this time and the number of embryos transferred. Women were diagnosed with overt hypothyroidism if serum TSH was >2.5 mIU/L and serum concentrations of free thyroxine or triiodothyronine were outside of their reference ranges. Subclinical hypothyroidism was defined as serum TSH >2.5 mIU/L and free thyroid hormones within the normal range (9). All pregnant women were contacted by phone after the scheduled time of delivery to obtain data on the outcome of the pregnancy.
Serum TSH was measured with the Immulite analyzer, a fully automated solid-phase third-generation immunoassay analyzer with a chemiluminescent detection system (Diagnostic Products Corp.). Both the intra- and interassay coefficients of variation were <10%. Thyroid peroxidase and/or thyroglobulin antibodies were measured by diagnostic commercial kits using an immunofluorescence assay (Phadia; Thermo Scientific), with normal values set at <40 IU/L (antithyroglobulin) and <35 IU/L (antithyroperoxidase).
Analysis of the data was carried out with the Statistics Package for Social Sciences (SPSS 18.0). Statistically significant differences were determined using unpaired Student's t-test, nonparametric Wilcoxon unpaired test, or Fisher's exact test, as appropriate. A p-value ≤0.05 was considered statistically significant. The main outcome chosen was the live birth rate per started cycle. The sample size was calculated based on an expected delivery rate of 20% per started cycle among controls and stating as clinically relevant a twofold lower chance of delivery in women with treated hypothyroidism. On these bases and setting type I and II errors at 0.05 and 0.20, respectively, the required sample size consisted of about 400 women (135 cases and 270 controls). A three-year period of recruitment was decided based on preliminary data on the incidence of eligible cases obtained over a one-year period.
Results
During the study period, 137 out of 1053 women (13%) fulfilled our selection criteria for cases. The median (interquartile range, IQR) serum TSH before initiating treatment was 4.8 (4.1–6.1) mIU/L. The median (IQR) daily dose of levothyroxine used to normalize serum TSH was 75 (50–89) μg. The presence of thyroid antibodies was documented in 79 cases (58%). Among them, the numbers with exclusively thyroid peroxidase antibodies, with exclusively thyroglobulin antibodies, and with both antibodies were 18 (23%), 3 (4%), and 58 (73%), respectively. The number of women treated because of overt hypothyroidism and subclinical hypothyroidism was 70 (51%) and 67 (49%), respectively.
These 137 cases were matched to 274 controls. Baseline characteristics of the two study groups are shown in Table 1. No statistically significant difference emerged, with the exception of body mass index, which was higher among cases. The characteristics of the IVF-ICSI cycles are summarized in Table 2. The rate of canceled cycles for poor response was higher, the duration of stimulation was longer, and the total number of women not performing embryo transfer (i.e., the sum of those who were canceled for poor response, those who failed to obtain oocytes, and those who obtained oocytes but failed to obtain viable embryos) was higher in women with treated hypothyroidism. No statistically significant differences emerged for the other variables. The median (IQR) fertilization rate in cases and controls was 75% (60–100%) and 86% (67–100%), respectively (p=0.017). The median (IQR) rate of top-quality embryos per oocyte used was 33% (25–50%) and 33% (25–67%), respectively (p=0.45).
Only one woman (among controls) was receiving cabergoline because of hyperprolactinemia.
AFC, antral follicle count; AMH, anti-Müllerian hormone; FSH, follicle-stimulating hormone; IVF-ICSI, in vitro fertilization–intracytoplasmic sperm injection; PRL, prolactin; TSH, thyrotropin.
Data are reported as n (%), mean±SD, or median (interquartile range) as appropriate.
Refers to women undergoing oocytes retrieval (131 cases and 271 controls).
Refers to women retrieving suitable oocytes (125 cases and 265 controls).
The number of suitable oocytes and the number of used oocytes differ because of the Italian legislation banning the systematic use of all the available oocytes.
Refers to all women.
Refers to women performing embryo transfer (114 cases and 254 controls).
ART, assisted reproductive technology; ET, embryo transfer; GnRH, gonadotropin releasing hormone; hCG, human chorionic gonadotropin; rFSH, recombinamt FSH.
Clinical pregnancies were documented in 49 cases and 94 controls. The number of twin pregnancies in the two groups was 13 and 17, respectively. The implantation rate in cases and controls was 28% (62 of 224) and 22% (111 of 507), respectively (p=0.11). The clinical pregnancy rates per started cycle, per oocytes retrieval, and per embryo transfer in the two groups were 36% and 34% (p=0.93), 37% and 35% (p=0.66), and 43% and 37% (p=0.30), respectively (Fig. 1). Abortions occurred in 8 of 49 women among cases (16%), and in 21 of 94 women among controls (22%) (p=0.51). No intrauterine demise occurred. Live births were documented in 41 cases and 73 controls. The live birth rates per started cycle, per oocyte retrieval, and per embryo transfer in cases and controls were 30% and 27% (p=0.50), 31% and 27% (p=0.41), and 36% and 29% (p=0.18), respectively (Fig. 1).
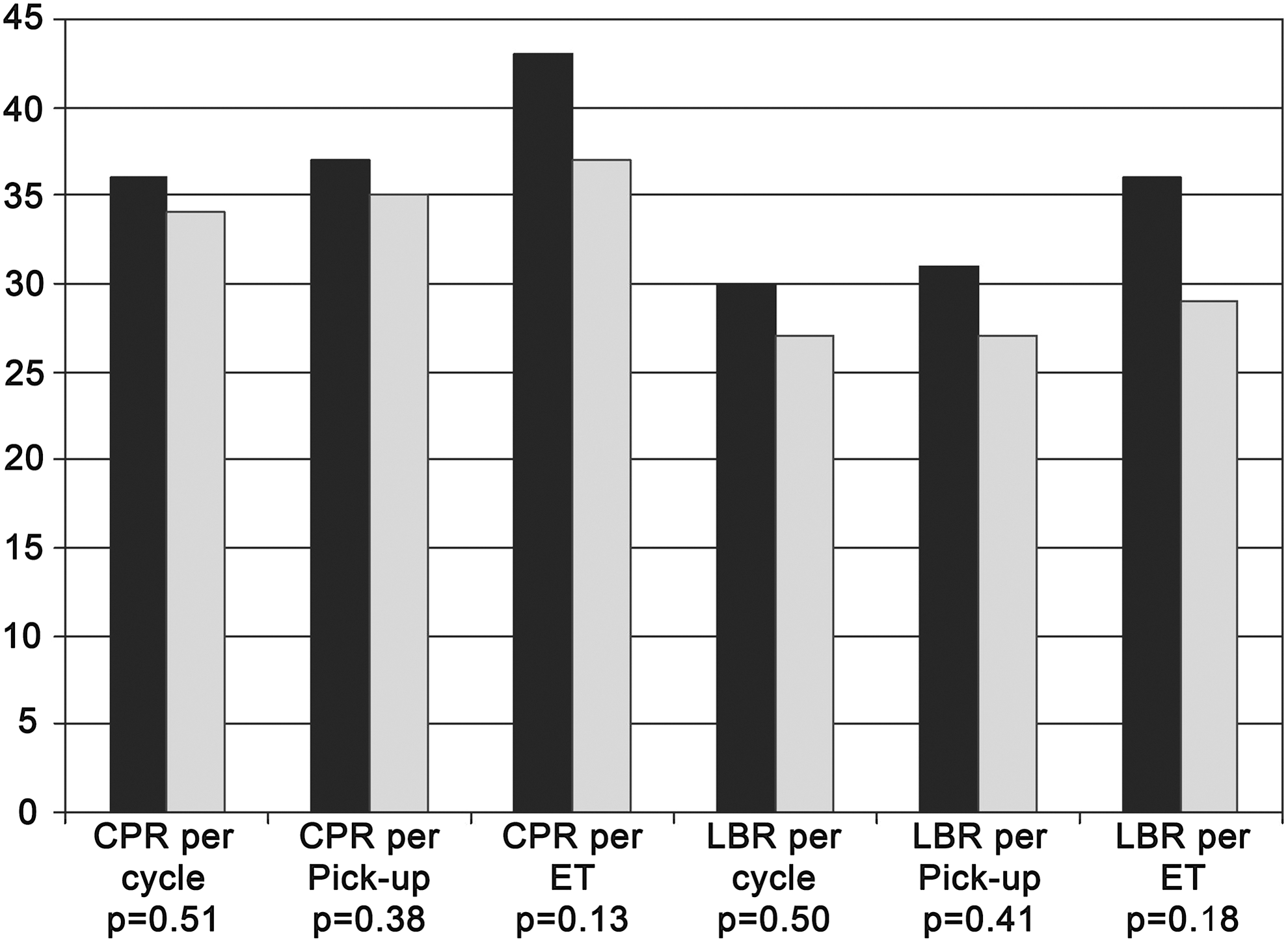
Chances of success in women with treated hypothyroidism (cases, black bars) and in controls (controls, gray bars). The figure refers to the chances of live birth (primary outcome of the study). Data are presented separately as live births per started cycle, per oocyte retrieval, and per embryo transfer. p-Values are reported below. No statistically significant differences emerged. CPR, clinical pregnancy rate; ET, embryo transfer; LBR, live birth rate; Pick-up, oocytes retrieval.
Subgroup analyses were performed within the group of women with treated hypothyroidism. First, we compared women with (n=79) and without (n=58) thyroid autoimmunity. Baseline characteristics of the two groups did not differ (data not shown). The median (IQR) serum TSH before initiating treatment was 5.3 (4.5–7.0) and 4.4 (3.8–5.2) mIU/L, respectively (p=0.004). The median (IQR) daily doses of levothyroxine used to normalize serum TSH were 75 (50–82) and 75 (50–100) μg, respectively (p=0.95). The main findings of the IVF outcomes are summarized in Table 3. No statistically significant differences emerged. An intragroup analysis according to the specific autoantibodies detected also failed to document any significant result (data not shown).
Data are reported as n (%), mean±SD, or median (interquartile range) as appropriate.
Refers to women undergoing oocytes retrieval (78 AB POS women and 53 AB NEG women).
Refers to women retrieving suitable oocytes (73 AB POS women and 52 AB NEG women).
The number of suitable oocytes and the number of used oocytes differ because of the Italian legislation banning the systematic used of all the available oocytes.
Refers to all women.
Refers to women performing embryo transfer (64 AB POS women and 50 AB NEG women).
Refers to total number of embryos transferred (124 in AB POS women and 100 in AB NEG women).
Refers to pregnant women (27 in AB POS women and 22 in AB NEG women).
AB NEG, women with treated hypothyroidism and negative thyroid antobodies; AB POS, women with treated hypothyroidism and positive thyroid antobodies; DR, delivery rate; IR, implantation rate; PR, pregnancy rate.
Second, we compared women who were diagnosed with overt hypothyroidism (n=70) with those who were diagnosed with subclinical hypothyroidism (n=67). Similarly, baseline characteristics of the two groups did not differ (data not shown). The median (IQR) serum TSH before initiating treatment was 6.2 (5.6–7.6) and 4.3 (3.7–4.6) mIU/L, respectively (p<0.001). The median (IQR) daily doses of levothyroxine used to normalize serum TSH were 75 (50–100) and 50 (25–75) μg, respectively (p<0.001). The main findings of the IVF outcomes are summarized in Table 4. The outcomes of the two groups were similar with the exception of the number of embryos transferred, which was higher in women with overt hypothyroidism.
Refers to women undergoing oocytes retrieval (67 women with treated OH and 64 women with treated SH).
Refers to women retrieving suitable oocytes (63 women with treated OH and 62 women with treated SH).
The number of suitable oocytes and the number of used oocytes differ because of the Italian legislation banning the systematic used of all the available oocytes.
Refers to all women.
Refers to women performing embryo transfer (56 women with treated OH and 58 women with treated SH).
Refers to total number of embryos transferred (116 in women with treated OH and 108 in women with treated SH).
Refers to pregnant women (28 in women with treated OH and 21 in women with treated SH).
OH, women with treated overt hypothyroidism; SH, women with treated subclinical hypothyroidism.
Discussion
In this study, we document that IVF-ICSI outcome is not hampered in women with adequately treated hypothyroidism. Affected women were at higher risk for cycle cancelation because of poor response, the duration of stimulation was longer, the fertilization rate was lower, and their overall chances of reaching the stage of embryo transfer were lower. However, the magnitude of these differences was mild and we failed to document any difference between the study groups for the most relevant outcomes, i.e., pregnancy rate, implantation rate, and live birth rate. Moreover, we also failed to detect an independent detrimental effect of thyroid autoimmunity. Finally, considering the comparison between women treated for overt and subclinical hypothyroidism, a statistically significant difference emerged only for the number of embryos transferred. However, the relevance of this finding is doubtful considering that the magnitude of the difference is small (the mean number of embryos transferred was 2.1 and 1.9, respectively) and the number of embryos obtained was identical (2.9 and 2.9, respectively).
Our findings are in contrast with those of two recent similar studies on IVF-ICSI outcome in women with treated hypothyroidism. Kilic et al. (5) compared 15 women with treated hypothyroidism to 31 euthyroid controls and observed a lower clinical pregnancy rate (13% vs. 42%, p=0.021). Scoccia et al. (6) compared 21 women with treated hypothyroidism and 219 euthyroid controls and documented a significantly reduced implantation rate (8% vs. 33%, p=0.001), clinical pregnancy rate (14% vs. 47%, p=0.004), and delivery rate (14% vs. 47%, p=0.035) (6). The significance of these studies has, however, been questioned because the authors did not use today's stringent criteria for levothyroxine treatment, i.e., serum TSH levels below 2.5 mIU/L (10). The mean±SD serum TSH of the treated women in the two studies was 2.2±1.2 and 2.5±1.3 mIU/L, respectively. Thus, a consistent proportion of the affected women were actually undertreated (7). Notably, these conflicting observations may also be explained by other differences in the population studied, in particular the etiology or severity of the hypothyroidism itself. To our knowledge, these are the sole previous available contributions comparing IVF-ICSI outcome in women with treated hypothyroidism to a group of euthyroid women. There is, thus, a need for further evidence on this issue.
Even if our study suggests that adequate levothyroxine treatment of hypothyroidism can normalize IVF-ICSI outcomes, it does not paradoxically provide definitive evidence as to the need for this kind of treatment. Since the study was not randomized, we cannot rule out the possibility that the chances of success would have been similar even without levothyroxine administration. In fact, although surprising, available evidence on the detrimental impact of hypothyroidism on IVF-ICSI success is so far limited. In a recent meta-analysis, Van den Boogaard et al. (2) reported that, in contrast to spontaneous pregnancies, there is no definite evidence for a lower pregnancy rate and an increased risk of miscarriage in women with thyroid dysfunction and autoimmunity undergoing IVF. The common odds ratios were 0.67 [95% confidence interval 0.36–1.4] and 1.6 [95% confidence interval 0.76–3.5], respectively (2). We herein speculate that this result may be the consequence of a type II error caused by insufficient evidence. In fact, the lack of a statistically significant clinical impact contrasts with the results of a recent randomized controlled trial in women with subclinical hypothyroidism undergoing IVF (4). In this study, levothyroxine administration was associated with a higher implantation rate (27% vs. 15%, p=0.04) and a higher live birth rate (53% vs. 25%, p=0.04) (4).
Notably, our study indirectly also sheds some light on the pathogenetic mechanisms linking thyroid autoimmunity and miscarriage. Two main hypotheses have been proposed for this association (11,12). On the one hand, the autoimmune process leading to the development of thyroid antibodies may be deleterious on its own. Circulating thyroid antibodies per se or the autoimmune-related process may interfere with pregnancy development. Alternatively, thyroid antibodies may reflect a subtle decrease in the capacity of the thyroid function to adapt adequately to the changes associated with the pregnant state because of a reduced functional reserve. Our observation that the presence of antithyroid antibodies did not impact on IVF-ICSI outcomes tends to favor this second explanation. Women with thyroid antibodies who are adequately treated did not seem to face an increased rate of abortion.
Some limitations of the study should be recognized. In particular, the choice of the control group may be a matter of concern. Controls were matched by age and study period, but we cannot exclude some confounders. On the other hand, the baseline characteristics of the two groups were highly similar. Body mass index was the unique variable that differed, but the magnitude of the difference was mild and of doubtful clinical relevance (22.9 and 21.9 kg/m2 in cases and controls, respectively). The risk of misdiagnosis is also unlikely because controls systematically underwent a serum TSH assessment the month preceding the attempt and those with a history of thyroid disorders were excluded. On the other hand, it has to be recognized that controls were not screened for thyroid peroxidase and/or thyroglobulin antibodies, and hence we cannot exclude that a proportion of controls may actually have thyroid autoimmunity. This may have diluted the potential detrimental effects of thyroid autoimmunity. In this regard, this possibility is uncommon in women with serum TSH ≤2.5 mIU/L. Two independent groups recently showed that, in women aged 20–40 years, the prevalence of thyroid peroxidase and/or thyroglobulin antibodies is below 10% (13,14). Finally, in both study groups, thyroid function was not monitored during the ovarian hyperstimulation. This may be a limitation given that serum TSH has been shown to increase during IVF cycles (15). It may be speculated that, at least among cases, a strict monitoring of serum TSH during hyperstimulation would have allowed to promptly adapt levothyroxine dosage and thus optimizing the benefits of this treatment. On the other hand, the lack of major differences in the study outcomes argues against the relevance of this limitation. An alternative explanation may be that a single fixed dose of levothyroxine may be sufficient in studied cases because the severity of the disease was low in most of them.
In conclusion, women scheduled for IVF-ICSI with adequately treated hypothyroidism can be reassured regarding the success of the procedure. Ovarian responsiveness and fertilization rate are reduced and the chance of reaching the stage of embryo transfer is lower, but the pregnancy and live birth rates are not affected. In fact, adequate levothyroxine treatment maintaining TSH serum levels below 2.5 mIU/L may overcome the detrimental effects of hypothyroidism. Finally, our study also tends to rule out an independent harmful effect of autoimmunity per se. Further evidence is needed, however, to resolve the discrepancies with the two previous studies on this issue and determine whether our conclusion may be valid in all subgroups of affected women.
Footnotes
Author Disclosure Statement.
No competing financial interests exist for any of the authors