
Abstract
Background:
Thyroid hormones are important for the adult brain, particularly regions of the hippocampus including the dentate gyrus and CA1 and CA3 regions. The hippocampus is a thyroid hormone receptor–rich region of the brain involved in learning and memory. Consequently, alterations in thyroid hormone levels have been reported to impair hippocampal-associated learning and memory, synaptic plasticity, and neurogenesis. While these effects have been shown primarily in developing rats, as well as in adult rats, little is known about the effects in adult humans. There are currently no data regarding structural changes in the hippocampus as a result of adult-onset hypothyroidism. We aimed to establish whether hippocampal volume was reduced in patients with untreated adult-onset hypothyroidism compared to age-matched healthy controls.
Methods:
High-resolution magnetization-prepared rapid acquisition with gradient echo (MPRAGE) scans were performed on 11 untreated hypothyroid adults and 9 age-matched control subjects. Hypothyroidism was diagnosed based on increased levels of thyrotropin (TSH) and reduced levels of free thyroxine (fT4).
Results:
Volumetric analysis of the right and left hippocampal regions, using functional magnetic resonance imaging of the brain (FMRIB) integrated registration and segmentation tool (FIRST), demonstrated significant volume reduction in the right hippocampus in the hypothyroid patients relative to the control group.
Conclusions:
These findings provide preliminary evidence that hypothyroidism results in structural deficits in the adult human brain. Decreases in volume in the right hippocampus were evident in patients with adult-onset overt hypothyroidism, supporting some of the findings in animal models.
Introduction
H
We have recently reported cognitive abnormalities in a longitudinal study of adults with overt hypothyroidism before and following
According to Gilbert et al. (12), different brain regions require thyroid hormones at different stages of development; the basal ganglia before the hippocampus, and the posterior before the anterior regions of the cortex. This suggests that the point at which thyroid hormone abnormalities begin during development and across the lifespan may have a greater impact on one region compared with another (13 –15). Studies in neonatal, perinatal, postnatal, and adult rats have reported neuronal alterations that have been attributed to hypothyroidism, including changes in brain structure and function, short- and long-term memory, gene expression, cell signaling, and migration (9,11,12,16 –19). Early studies investigating the effects of hypothyroidism on the CA1, CA3, and dentate gyrus region of the hippocampus demonstrated a reduction in the volume, weight, and numerical density of cells within the dentate gyrus and CA1 regions of the hippocampus with a corresponding decrease in volume, but an increase in numerical density of cells within the CA3 region (18,20). A number of these differences were evident in both developing and adult hypothyroid rats, suggesting that regardless of the time of onset and duration of hypothyroidism, the hippocampus is vulnerable to this condition. Further evidence of this is found in Gilbert's investigation of the effect of developmental hypothyroidism on euthyroid adult animals (19); she reported that adult rats had reduced population spike amplitude and short-term plasticity, along with amplified long-term synaptic plasticity in the CA1 area, despite the fact that their thyroid hormones were within the normal range. These findings support the idea that alterations in thyroid status at a young age can permanently alter hippocampal function, even with a return to euthyroid status.
In the adult brain, DeSouza et al. (10) suggest that thyroid hormones are implicated in the regulation of hippocampal neurogenesis. They found an influence of thyroid hormones on the survival of adult hippocampal progenitors. Furthermore, they suggest that the level of thyroid hormones may be crucial for this relationship; they found that the decline in hippocampal neurogenesis could be attenuated by thyroid hormone replacement. Findings from Ambrogini et al. (13) are consistent with the view that by preventing apoptosis, thyroid hormones promote cell survival. Hypothyroidism resulted in a reduction in the number of cells and volume of the dentate gyrus; this may reflect some of the cognitive impairments reported in hypothyroidism. Importantly though, regardless of the time at which hypothyroidism begins, these morphological changes and learning and memory deficits have been reported in both the animal and human literature during developmental and adult stages (1,2,9,11,21).
While there are currently no data available regarding hippocampal volume in human subjects with adult-onset hypothyroidism, Oatridge et al. (22) demonstrated increased whole-brain volume and reduced ventricle size compared to baseline values in three adult-onset hypothyroid subjects following
More recently, using voxel-based morphometry (VBM), Singh et al. (25) reported reduced white- and gray-matter volumes in a small number of young adults with untreated hypothyroidism (mean age=31.1 years). Gray matter decreases were found in the bilateral cerebellum and left postcentral gyrus, while white matter decreases were found in the bilateral cerebellum, the right precentral gyrus, right inferior and middle frontal gyrus, right inferior occipital gyrus, and right inferior temporal gyrus. While there was no attempt to relate this decreased volume to measures of cognitive function, the authors point out that these regions are involved in a number of functions that have been shown to be impaired in hypothyroidism, such as attention, visuospatial processing, and memory. Focusing specifically on the hippocampus, Wheeler et al. (21) demonstrated for the first time that children and adolescents with congenital hypothyroidism had smaller hippocampi, particularly on the left side, in comparison to control children. They proposed that these hippocampal volume reductions contribute to the reduced performance evident on a number of memory tasks. This is in line with findings from the animal literature, where changes to the structure of the hippocampus are evident in both congenital and adult-onset hypothyroidism. While these recent studies suggest that hypothyroidism does influence cortical and subcortical volume, no studies to date have examined these effects in the hippocampus in adult-onset hypothyroidism. The aim of the present study was to determine for the first time the effects of adult-onset hypothyroidism on hippocampal volume.
Materials and Methods
Participants
Hypothyroidism was diagnosed based on free thyroxine (fT4) levels below the lower limit of the normal range (11 pmol/L) and thyrotropin (TSH) levels above the upper limit of the normal range (10 mU/L). Eleven patients (two male) with hypothyroidism aged 27–55 years participated in this study. The majority of patients were recruited from general practitioner referrals to the endocrinology outpatient service, the remainder being direct referrals to the endocrinology department from other specialist teams within the hospital. All patients reported classical symptoms of hypothyroidism; these symptoms ranged from 4 to 12 months. All reported normal growth and puberty and no childhood developmental problems or illness that might have reflected earlier development of hypothyroidism. All patients were scanned within one to two weeks of diagnosis and before treatment began. Nine healthy control subjects (one male) aged 26–54 years and of similar education were recruited from the local community via fliers in the hospital and word of mouth. All participants were native English speakers, with normal or corrected to normal vision, and were right-handed. Exclusion criteria included a previous history of ischemic heart disease, stroke, diabetes, head injury, epilepsy, psychiatric illness, significant visual impairment, or pregnancy. Furthermore, no participants had taken part in previous published studies from our laboratory (1). All study subjects gave their written signed consent to the study, which was approved by the Research Ethics Committee of the Psychology Department, Trinity College Dublin, and the Adelaide and Meath Hospital and St. James's Hospital, Dublin, Ireland. One control participant and one hypothyroid participant were excluded from the analysis due to excessive motion. Blood was drawn from each participant before scanning for analysis of thyroid hormone levels.
Structural MRI data acquisition
Scanning was conducted on an Intera Achieva 3.0 Tesla MR system (Philips, Andover, MA). First, a reference scan was acquired to resolve sensitivity variations. Then 180 high-resolution T1-weighted anatomic magnetization-prepared rapid acquisition with gradient echo (MPRAGE) axial images were acquired (FOV 230 mm, thickness 0.09 mm, voxel size 0.9 mm×0.9 mm×0.9 mm, total duration 325 sec).
Image processing
Segmentation and volumetric analysis of the left and right hippocampus was performed using the functional magnetic resonance imaging of the brain (FMRIB) integrated registration and segmentation tool (FIRST) from FMRIB's Software Library (FSL) v4.1.8 (26,27). This is a semi-automated model-based subcortical tool that uses a Bayesian probabilistic approach from shape and appearance models derived from a library of 317 manually segmented images (obtained from the Center for Morphometric Analysis, Massachusetts General Hospital, Boston). In the first step, a two-stage affine registration to a T1 standard space template (MNI 152 at 1 mm resolution) was performed on each subject's MPRAGE, using 12 degrees of freedom and a subcortical mask to exclude voxels outside the hippocampus. Next, the left and right hippocampus were segmented with 30 modes of variation. These increase the robustness and reliability of the results by optimizing them based on the leave-one-out cross-validation of the training set. Following this, boundary correction of these regions included determining whether the boundary voxels were part of the left or right hippocampus. Papers comparing manual and automated segmentation of the hippocampus frequently state that automated methods produce larger left and right hippocampi (28 –30). One of the complaints about FSL's FIRST is that the boundary correction is too liberal. Normally voxels are included if they passed the probability threshold of z>3 (p<0.001) (30). However, several papers have successfully used these methods in the past to identify differences in hippocampal volume between groups (31 –33). In order to generate regions that were more comparable to those reported in manual tracing studies, we used both a z>3 boundary threshold (typical in FSLs FIRST scripts) and a more conservative z>2 boundary threshold for the hippocampal regions, ensuring in this second analysis that fewer nonhippocampal voxels were included. The segmented left and right hippocampus of each participant was overlaid onto their brain to ensure correct registration and segmentation. The volume of each region was measured (mm3), along with the intracranial volume (ICV). ICV is calculated as the sum of the gray matter, white matter, and cerebrospinal fluid, and can be used to adjust regional volumes for sex and height differences across subjects (34 –36). Subjects who have larger ICV typically have larger subcortical regions; for this reason, it is important to correct for ICV (28). The volume of the hippocampus was adjusted for ICV, according to a method developed by Free et al. (37), using an analysis of covariance approach as detailed by Erickson et al. (32). Briefly, the adjusted volume=raw volume – b×(ICV – mean ICV), where b is the slope of a regression of a region of interest volume on ICV. These methods have been used extensively in previous studies (31,34,38 –42). This adjusted volume was then used for all analyses.
Analytic measurement
Using the DPC Immulite 2000 analyzer (Diagnostic Products Corp., Los Angeles, CA), serum TSH concentrations were measured using a third-generation chemiluminescent immunometric assay, and fT4 was measured using a competitive analog immunoassay (coefficient of variation <5% for all).
Statistical analyses
All statistical analysis was conducted using SPSS v19 (IBM). Analysis of variance (ANOVA) was used to investigate differences between the groups. Mean values (standard error of the mean; SEM) were reported throughout. Where a covariate was included, the adjusted means and SEM are reported. We conducted a post hoc power analysis using G*Power (v3.1.3), with an alpha level of 0.05, one tailed using the means (adjusted for the effect of age) and SEM of the hippocampal volumes.
Results
Participant demographics
Hypothyroid (mean [±SEM] age 42.3±3.5 years) and control subjects (mean age 38.6±4.0 years) did not differ in age (p=0.50). Mean TSH and fT4 levels in hypothyroid subjects were 61.85±8.54 mU/L and 5.19±0.70 pmol/L, respectively. Mean TSH and fT4 levels in normal subjects were 1.61±0.21 mU/L and 16.39±0.93 pmol/L, respectively (Table 1).
Values are presented as mean±SEM. There were no significant differences between the groups on age or sex.
Hippocampal volume
Table 2 provides the hippocampal (adjusted for intracranial volume) and intracranial volume data in mm3. Age at visit was included as a covariate in the ANOVA, as it is known to influence hippocampal volume, and although the groups were closely matched for age and did not differ on this variable, the age range of both groups spanned 28 years. An example of the image created for the left and right hippocampus for both a control and hypothyroid adult is shown in Figure 1. Intracranial volume did not differ between hypothyroid and control subjects (p=0.757). Using a boundary correction of 3, left hippocampal volume was 7.5% lower in hypothyroid subjects, but the difference was not statistically significant (mean left hippocampal volume: controls 4167±133 mm3; patients 3851±118 mm3; p=0.097; Fig. 2A). However, compared to normal subjects, the hypothyroid patient group showed a significant decrease in volume within the right hippocampus amounting to a 12.1% difference between the groups (mean right hippocampal volume: controls 4435±158 mm3; patients 3897±141 mm3; f=6.379; df=1, 15; p<0.05; Fig. 2A). Using a boundary correction of 2, the left hippocampal volume was 5.11% lower in hypothyroid subjects, but the difference was not statistically significant (mean left hippocampal volume: controls 3637±123 mm3; patients 3451±110 mm3; p=0.277; Fig. 2B). Compared to control subjects, the hypothyroid patient group showed a significant decrease in volume within the right hippocampus amounting to a 9.81% difference between the groups (mean right hippocampal volume: controls 3965±134 mm3; patients 3576±120 mm3; f=4.616; df=1, 15; p<0.05; Fig. 2B). Finally, there were no significant differences between the volume of the left and right hippocampus within the groups, again controlling for the effects of age on hippocampal volume (controls: p=0.433; hypothyroid: p=0.057).
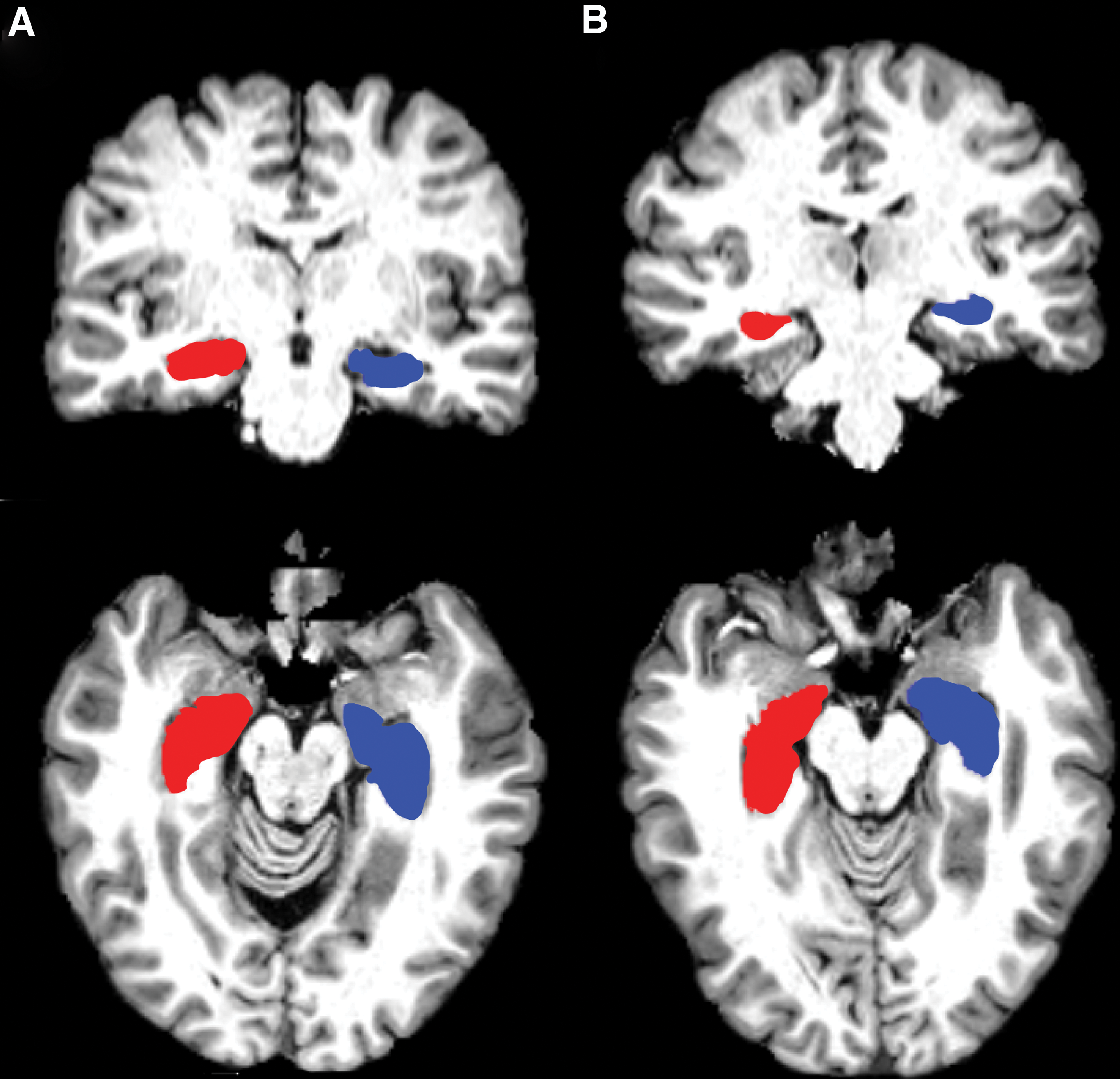
Left (red or dark gray) and right (blue or light gray) hippocampus masks from a control subject

Mean volume of the left and right hippocampus in mm3 in the control and hypothyroid groups, using boundary corrections of 3
Values are presented as mean±SEM. Volumes were adjusted for the effect of age.
There was a significant (p<0.05) decrease in right hippocampal volume in hypothyroid adults, using a boundary correction of 3 and a more conservative 2. There was no significant difference between control and hypothyroid adults in the left hippocampus or in intracranial volume.
A post hoc power analysis was calculated based on the adjusted means and unadjusted standard deviations (not adjusted for age). With p<0.05, an effect size of 1.087, and a sample of 8 control subjects and 10 hypothyroid subjects, we reached 70% power for differences in the right hippocampus using a boundary correction of 3. When we reduced the boundary correction to 2, using a p<0.05, an effect size of 0.967, and a sample of 8 control subjects and 10 hypothyroid subjects, we reached 62% power for differences in the right hippocampus.
Discussion
Much of the literature has reported significant alterations in the hippocampus as a result of neonatal, perinatal, postnatal, and adult-onset hypothyroidism. The greatest phase of sensitivity to thyroid alterations reportedly occur before and during the postnatal stages. The changes during this period are well characterized in comparison to those during adulthood, many of which are still not well understood (16). These data provide preliminary evidence that patients with untreated adult-onset hypothyroidism have reduced hippocampal volumes in comparison to age-matched healthy subjects. Following adjustment for overall head size and sex differences, we observed a statistically significant 12.1% volume reduction in the right hippocampus and a nonsignificant 7.5% volume reduction in the left hippocampus in patients with hypothyroidism using a hippocampal boundary correction of 3 (Table 2, Fig. 2). Similar findings were still evident with a more conservative boundary correction of 2, though to a smaller degree (there was a significant 9.8% volume reduction in the right hippocampus and a nonsignificant 5.1% volume reduction in the left hippocampus in patients with hypothyroidism). These findings are consistent with the animal literature in which significant effects on the hippocampus as a result of prenatal, postnatal, and adult-onset hypothyroidism have been reported.
Although there is no apparent evidence in the current literature for a hypothyroid-induced vulnerability in one hemisphere versus the other, with much of the animal literature focused on the hippocampus as a whole, Wheeler et al. (21) reported smaller left hippocampi in congenital hypothyroidism in a group of 35 children. They also found a correlation between a larger left hippocampus and visuospatial memory in this group, indicating that children with larger left hippocampi have better visuospatial memory. However, visuospatial memory is typically associated with the right hippocampus. The present study found a significantly smaller right hippocampus in adult-onset hypothyroidism. This is in line with a previous report from our laboratory in which we reported persistent deficits in the Rey–Osterrieth Complex Figure (1), a well-known measure of visuospatial memory. These deficits were evident at baseline before treatment and following six months of thyroid-hormone replacement for adult-onset hypothyroidism, suggesting that hypothyroidism may lead to permanent right hippocampal damage. Our current findings of reduced right hippocampal volume in adult onset hypothyroidism reached a post hoc power level of 70% for the typical boundary correction of 3, and 62% for the more conservative boundary correction of 2. Given the small subject numbers, these power analyses provide considerable strength to the current findings. However, it is important to note that these were one-tailed, as they were calculated post hoc and we knew the direction of the results (decrease in volume). Findings from previous studies, however, would support a directional hypothesis (14 –16,25).
Comparisons with percentage volume reductions in the animal literature are difficult. Reported alterations in animals include a reduction in the weight of the hippocampus, a reduction in the number of cells found, damaged growth of axons and dendrites, and a reduction in the volume of the hippocampus (16). However, it is important to note that some of these differences did not remain following correction for overall brain volume (23,24). Rabie et al. (43) demonstrated a difference of up to 30% in hippocampal volume between 35-day-old (propylthiouracil (PTU)-induced) hypothyroid rats and control rats. They provided evidence that these effects were permanent. Even after a return to a euthyroid state, there was still a significant reduction in the volume of the hippocampus in a separate group of PTU-treated rats 160 days after birth (43). While the presence of altered hippocampal volume in adult rats is in agreement with the present findings of decreased hippocampal volume in adult-onset hypothyroidism, the methods that we used are considerably different to those used by Rabie et al., and our findings were considerably smaller (7–12%). On the other hand, more recently Powell et al. (24) reported that hippocampal volumes were significantly lower in hypothyroid rats. However, they also noted that when they looked at hippocampal volume as a percentage of total volume, differences were no longer evident. This suggests that hypothyroid rats had smaller head sizes than control rats, which was also supported by Hasegawa et al. (23). In contrast, the results of the current study provide evidence that patients with untreated adult-onset hypothyroidism have reduced hippocampal volumes, and that these differences remain following correction for intracranial volume due to head size and sex differences, in comparison to age-matched controls. But the findings from these previous studies highlight the importance of establishing whether there is a history of developmental thyroid disease in studies of adult-onset hypothyroidism.
The long-term impact of hypothyroidism remains unclear. Some studies have reported that alterations are irreversible. For example, Madeira et al. (18) reported that there was an irreversible reduction in the number of cells in the CA1 region of the hippocampus, which did not recover with a return to a euthyroid status, while impaired growth of axons and dendrites within the CA3 region of the hippocampus was preserved following a return to a euthyroid status (16). Using positron emission tomography (PET), Bauer et al. (44) found significant reductions in cerebral blood flow in adult onset hypothyroidism across a number of regions, including the hippocampus. Following three months of thyroid hormone replacement therapy, these reductions normalized. While no follow-up scans were carried out in the current study, behavioral evidence indicates that even with a return to a euthyroid status, patients with adult-onset hypothyroidism still display significant impairments in hippocampal-associated memory tasks (1). We have previously reported that relational memory learning and recall, both immediate and delayed, were significantly lower in those with adult-onset hypothyroidism (1). Furthermore, they had difficulty encoding a complex figure and a verbally presented story. A return to a euthyroid status following six months of treatment did not ameliorate these deficits. Hypothyroid patients still experienced difficulty with some measures of spatial and relational memory, both of which are known to rely on the hippocampus. Overall, these findings indicate that memory deficits are associated with hypothyroidism. However, in the future, there is a need to determine whether the structural alterations in the hippocampus found in the present study mediate these cognitive deficits.
While it is difficult to determine what the decrease in hippocampal volume reflects in the present study, Madeira et al. (18) suggest that the reduced volume in the CA3 region of the adult rat hippocampus reflects increased neuronal packing—that is, the space between the neurons decreased causing an overall reduction in hippocampal volume. While such a conclusion cannot be made here, it is noteworthy that a similar reduction in the volume of the right hippocampus was found in adult-onset hypothyroidism. These results provide a foundation for determining the impact that this reduced volume has on hippocampal functioning, and on the subsequent relationship between the hippocampus and the other regions of the brain. Examining the interaction between these regions during cognition may bridge the gap between behavioral and MRI studies.
Amelioration of hypothyroidism-induced changes in the brain depends upon the period during which hypothyroidism begins, and at least in animal models the region of the hippocampus in question, with the greatest sensitivity to hypothyroidism evident in early development. The prevalence of hypothyroidism is known to increase with age (45), but little is known about the effects of hypothyroidism on the adult brain and the age at which it will have the most impact on cognitive functioning (46). There is evidence that thyroid function is particularly important in cognitive function during aging when the brain is more reliant upon hormonal levels (47,48). Furthermore, hypothyroidism has been deemed “reversible dementia” (49,50), and for this reason plays a large part in dementia research (51,52). It is possible that hypothyroidism induces an age- and task-dependent impairment of memory. Some studies looking at normal elderly adults found that hypothyroidism was not associated with cognitive impairment (53,54), while others found that older adults were more vulnerable to the hypothyroid state than younger adults (3). In contrast, Tong et al. found that the deficits in odor memory and spatial consolidation were more impaired in young hypothyroid mice (two months) than older hypothyroid mice (15 months) (46). In the present study, age did not differ between the groups. However, as it is known to influence hippocampal functioning, and as the prevalence of hypothyroidism increases with age, we included age as a covariate in the analysis. Taking all of this into account, there is a need to examine the interaction between age, thyroid-induced cognitive impairments, and structural changes to regions of the brain associated with cognition, such as the hippocampus.
While the reductions in hippocampal volume in hypothyroidism reported here support those found in several previous studies (11,17,18,21,43), the current study has some limitations. Advances in automated segmentation methods such as FSL's FIRST and Freesurfer have resulted in some concern within the field about the differences in volume calculations using automated methods versus manual hippocampal tracing. While several groups suggest that automated methods inflate hippocampal volume (28,30), including voxels on the boundary that are not part of the hippocampus, the need for the use of automated methods becomes apparent in large-scale, multicenter studies. As a precaution, and to reflect manual estimations more closely, we ran a second set of analyses using a more conservative boundary correction value. We still found significantly smaller hippocampal volumes in hypothyroid patients using this more stringent automated method. These values were similar to or smaller than other previously published studies using the same methods (28,30), suggesting that we can optimize automated methods to better reflect manual tracing, allowing for significantly faster and more reliable testing across experimenters and centers. Although the number of patients who successfully completed this study is low, we still found a significant reduction in the volume of the right hippocampus (meeting a power level of between 62% and 70%). The nonsignificant difference in the left hippocampal size may have been related to limited statistical power due to low patient numbers. The lack of follow-up scans reduces our ability to interpret the permanent effects of adult-onset hypothyroidism on the hippocampus. Given that much of the animal literature reports some regrowth of the hippocampus, although at a lower level than control animals, and that the human behavioral literature indicates at least some improvement in performance on a range of memory tasks, we would expect to see alterations to the hippocampal volume with treatment. Furthermore, studies have shown that regions of the hippocampus in London taxi drivers are plastic (55,56)—that they change with spatial navigation experience, suggesting that the decrease in hippocampal volume seen in the current study may change with treatment. Lastly, as the adult-onset hypothyroidism literature consistently relies upon self-reported medical histories in addition to a valid diagnosis of adult-onset hypothyroidism, the subjects were interviewed upon admission to the study, and none of the included subjects reported previous experiences of hypothyroidism. However, we cannot rule out the possibility that some may have experienced hypothyroidism in early life.
Overall, our previous behavioral studies (1), along with the present findings, enhance our understanding of hippocampal changes associated with hypothyroidism. Although the numbers in the present study were small, the findings support previous studies that have reported neuronal alterations in hypothyroidism (21,22). Untreated adult-onset hypothyroidism leads to a reduction in volume of the right hippocampus. This has implications for our understanding of the role of thyroid hormones in cognition.
Footnotes
Acknowledgments
Many thanks to Dr. Joanne Feeney (Trinity College Institute of Neuroscience) for her assistance with MRI data collection and to Dr. Jim Monti (Department of Psychology, Beckman Institute) for his assistance with the volumetric analysis.
Author Disclosure Statement
No competing financial interests exist.