
Abstract
Background:
Brain metastases (BM) from differentiated thyroid carcinoma (DTC) are uncommon, and many questions about their management remain unsolved. The objective of this retrospective study was to analyze the characteristics, treatments, and outcomes of patients with BM from DTC.
Methods:
Among the 1523 patients with a DTC prospectively recorded in institutional databases between 1989 and 2012, 21 patients (1.4%) with BM were retrospectively retrieved. Patient characteristics, histological findings on initial thyroidectomy specimen, treatments, and time to death were reviewed. Overall survival (OS) was calculated using the Kaplan–Meier method. Survival curves for various subgroups of patients according to baseline characteristics and treatment received were compared.
Results:
The mean age at initial and BM diagnosis was, respectively, 52.7 and 63.2 years. World Health Organization performance status (PS) at BM diagnosis was good (<2) for 12 patients and poor (≥2) for 9. The initial carcinoma was papillary for 12 patients, follicular for 5, and poorly differentiated for 4. Eighteen patients had other previous and/or synchronous distant metastases: lung (11), bone (10), and others (2 peritoneum, 1 liver, 1 adrenal gland, and 1 uterine cervix). The average interval between the first metastasis and the BM was 3 years (range 0–35.6 years). The mean number and the mean size of BM were, respectively, 2.8 (range 1–10) and 22.5 mm (range 3–44 mm). Surgery was performed for 10 patients and radiotherapy (RT) for 18, with 2 stereotactic radiosurgery (SRS), 2 conformal RT limited to the metastasis, and 15 whole-brain RT. The median OS after BM was 7.1 months. OS at 1 and 2 years were 41.6% and 35.6%. PS and realization of surgery or SRS had an impact on survival, with OS of 27 months when PS <2 versus 3 months when PS ≥2 (p=0.0009), and OS of 11.9 months after surgery or SRS versus 3.6 months in their absence (p=0.04).
Conclusions:
BM from thyroid cancer may have an indolent evolution with survival of one to two years or longer for specific groups of patients. Therefore, aggressive treatment options such as neurosurgery and RT should be strongly considered in patients with good PS.
Introduction
B
Materials and Methods
The prospectively maintained institutional database at Institut Bergonié was retrospectively searched for patients with DTC and BM for the period 1989–2012. Patients with other primary neoplasms were excluded. Among 1523 patients with DTC (operated between 1 January 1989 and 31 December 2011 and follow-up until 31 December 2012), 136 patients developed distant metastases. Twenty-one patients with BM were identified, representing 1.4% of all patients and 15.4% of metastatic patients. A histological confirmation of the thyroid origin of BM was present for 11 patients. Medical records were reviewed and the following data are reported: patient sex and age (at the DTC diagnosis and at the BM diagnosis), pathology, mode of presentation and radiologic features of BM, patient performance status (PS) according the World Health Organization (WHO) classification at BM diagnosis, treatment modalities (surgery, SRS, WBRT with or without boost), and patient outcomes. Indications for treatment have evolved at our institution over the study years. Surgery was indicated if there were few BM (one or two) or for patients with multiple BM but with good PS and one BM responsible for neurologic symptoms (most frequently intracranial hypertension). SRS was not available at our institution before 2000. Currently, surgery is favored over SRS for patients with a single BM and good PS. SRS is indicated for frail patients with a single BM, for a single BM located in inoperable areas, and for patients with few cerebral lesions (≤3). WBRT was frequently performed in our study because it was systematically used until 2000. Nowadays, WBRT is only used in the case of multiple BM (>3).
All pathologic specimens were reviewed by a single thyroid expert pathologist using current WHO criteria and the Union for International Cancer Control classification. Follow-up occurred until December 2012. Informed patient consent was not necessary for this retrospective study; internal review board approval was obtained.
Overall survival (OS) after BM was calculated using the Kaplan–Meier method, and survival time was measured from the diagnosis of BM to the date of death or last follow-up. All causes of death are taken into account. Survival curves for various subgroups of patients according to baseline characteristics (PS >2 or PS ≤2, number of BM, or presence of neurologic symptoms at BM diagnosis) and treatment received (WBRT, SRS, and/or surgery) were compared using a two-sided log-rank test (p-value <0.05 was considered significant).
Results
Patient characteristics
Of the 21 patients, 12 were female and 9 male (female/male ratio=1.33:1) (Table 1). The mean patient age was 52.7 years (range 13.3–72.7 years) at initial diagnosis, and 63.2 years (range 43.1–76.9 years) at BM diagnosis. Eighteen patients presented other previous and/or synchronous distant metastases: lung (11), bone (10), peritoneum (2), liver (1), adrenal gland (1), and uterine cervix (1). A histological confirmation was obtained for the two unexpected localizations in the uterine cervix and the adrenal gland. The mean interval between the diagnosis of the first metastasis and BM was 3 years (range 0–35.6 years) for these patients.
BM, brain metastases; BSC, best supportive care; CRT, conformal radiation therapy; PS, performance status; TC, thyroid cancer; WBRT, whole-brain radiation therapy.
Histological findings of the primary tumor
Twelve patients had papillary carcinoma (six typical, four with follicular variant, and two with encapsulated form of classical papillary thyroid cancer [TC]), five had follicular carcinoma (four classical and one oncocytic), and four had poorly differentiated carcinoma. Stages were pT0-2 for nine patients, pT3-4 stage for eight, and unknown for four. Nodal involvement was present for five patients, absent for eight, and unknown for eight. The thyroid origin of the BM was histologically confirmed for 11 patients after biopsy or resection of the BM (with immunohistochemical analyses showing TTF1 positivity and thyroglobulin positivity).
Clinical and radiologic features of BM
The mean number of BM was 2.8 (range 1–10) with a mean size of 22.5 mm (range 3–44 mm). Seventeen patients had few BM (≤3), including 12 patients with a single BM. For 12 patients, BM were revealed by neurologic symptoms, including headaches, nausea, motor or sensory deficits, ataxia, aphasia, confusion, and epileptic seizures. For the other nine patients, the BM were diagnosed by chance. The diagnosis was made on systematic cerebral imaging before TKI prescription for four, on iodine scans for two, on PET scans for two, and on magnetic resonance imaging of the spine for one patient with a cerebellar lesion. WHO PS at BM diagnosis was good (<2) for 12 patients and poor (≥2) for 9. For 11 patients, computed tomography images or magnetic resonance imaging were available and reviewed. Three patients had dural metastases mimicking a meningioma with dural tails and occasionally bony invasion (Fig. 1). All other patients had brain parenchymal lesions with frequent ring enhancement and variable edema or hemorrhagic character (Fig. 2).

Three examples of dural metastases with intense enhancement on T1-Gd magnetic resonance imaging:
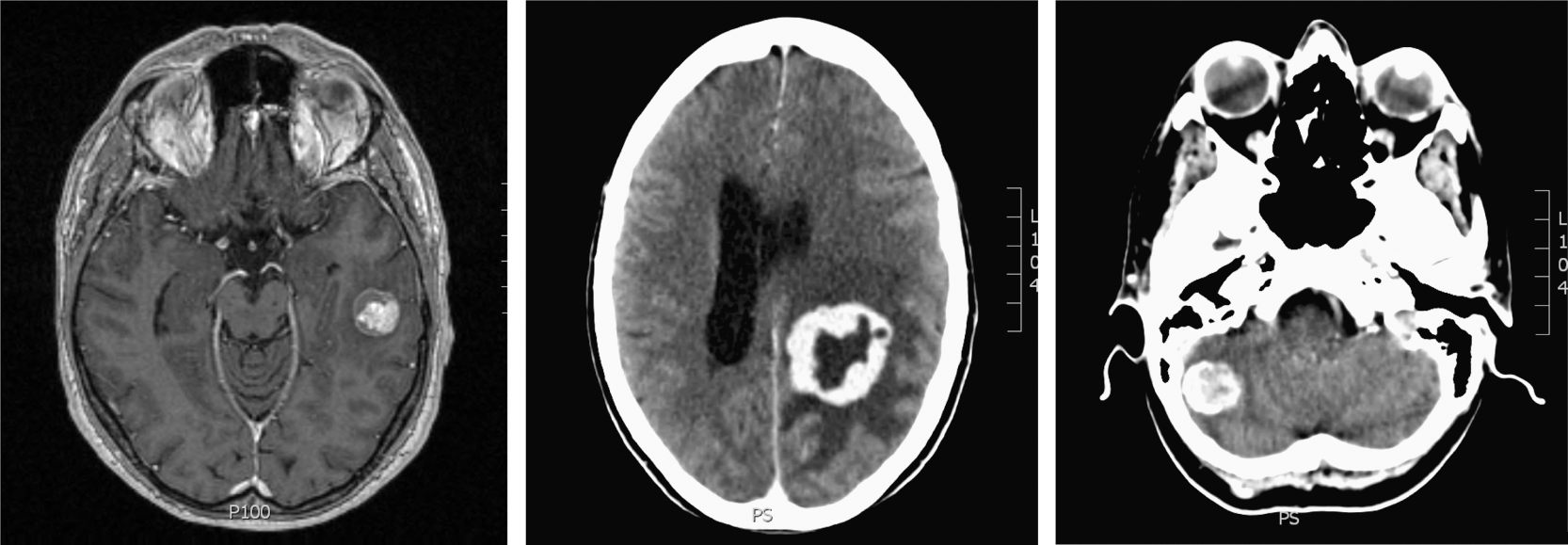
Three examples of brain parenchymal lesions with variable ring enhancement and edema.
Treatment
For two patients with poor overall condition, no surgery or RT was performed, and treatment was limited to best supportive care. Surgery was performed for 10 patients. Eighteen patients underwent external beam RT: 2 SRS, 2 conformal RT limited to the tumor or tumor bed, and 15 WBRT (8 with boost to the tumor). The median RT dose was 45 Gy (range 26–54 Gy). Most frequently, the dose per fraction was 3 Gy (range 1.8–4 Gy). Associations with the different treatment modalities are summarized in Table 2.
DTC, differentiated thyroid carcinoma; OS, overall survival; SRS, stereotactic radiosurgery.
Survival
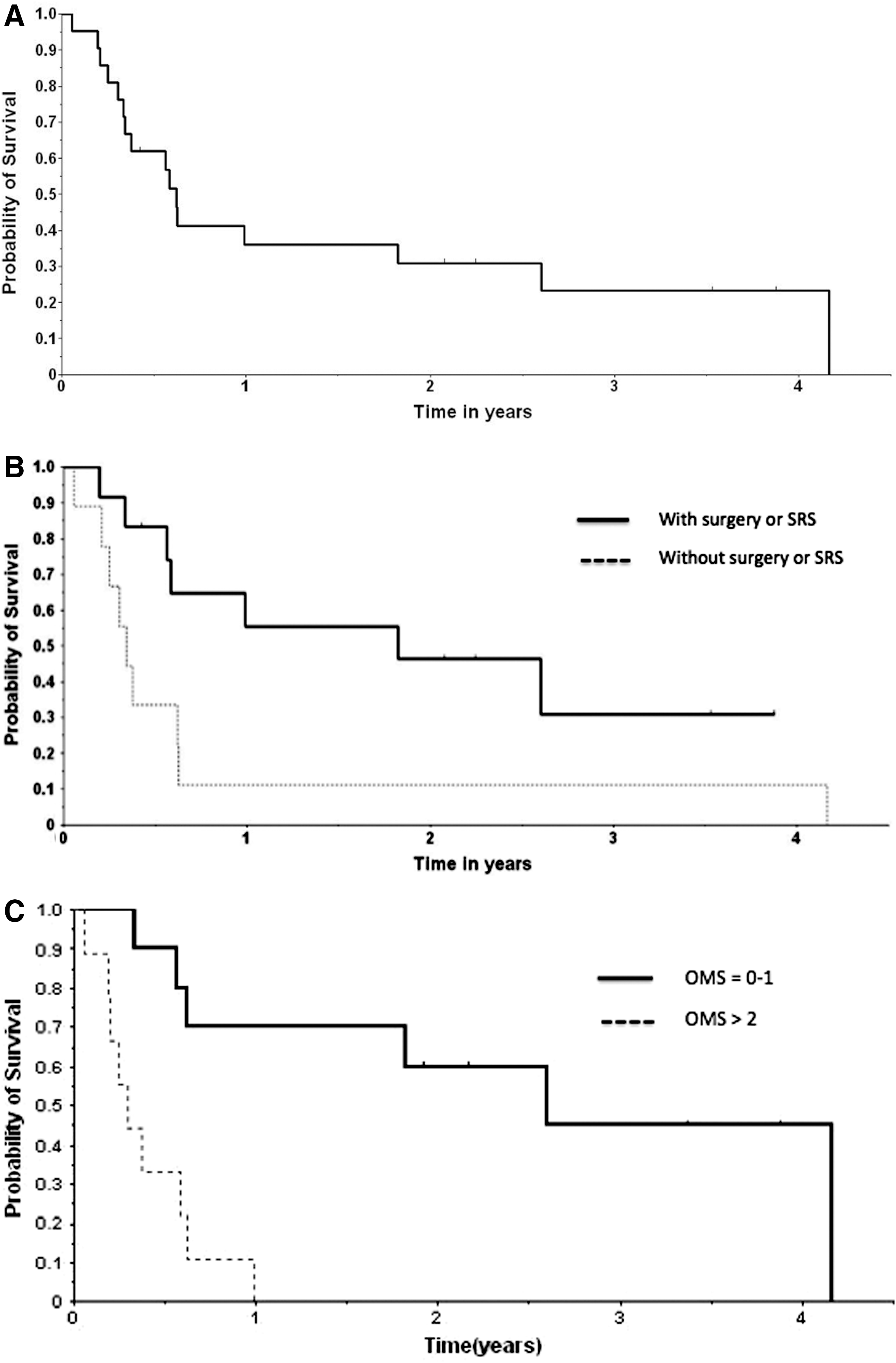
At the time of the last follow-up, six patients were still alive, with follow-up ranging from 2 to 45 months (Fig. 3). Among the 15 patients who died, death was due to progression of the brain lesion(s) in eight patients and to progression of other metastatic sites in four (two patients with a pulmonary evolution, one patient with a hepatic progression, and one with complications of bone metastases with a medullary compression). For three patients, treated between 1989 and 1994, the cause of death was unknown, with missing data in their files.
Median OS.
Median OS after BM was 7.1 months. Survival for seven patients was over 1 year. OS at 1 and 2 years were, respectively, 41.6% and 35.6%.
Survival comparisons were performed between subgroups of patients according to baseline characteristics and treatment received. Two factors (PS and realization of surgery and/or SRS) had a huge impact on survival. Indeed, median OS was 27 months if PS was <2 and only 3 months if PS was ≥2 (p=0.0009). Similarly, median OS was 11.9 months if surgery and/or SRS were performed and 3.6 months in absence of surgery and/or SRS (p=0.04). No impact of WBRT, number of BM, or presence of neurologic symptoms at BM diagnosis was found.
Discussion
The prevalence of BM among patients with metastatic thyroid cancer is estimated to be 4.5–18% (1,2). However, this number is probably an underestimate because, nowadays, systematic cerebral imaging before TKI treatment allows the detection of more asymptomatic BM. Management of these patients remains difficult because available data are based on old series with frequently symptomatic patients with potentially worse prognosis. Unfortunately, in the absence of recent data, our management is inevitably based on data from these old series, and overtreatment of asymptomatic BM is a possibility, given that data on the treatment of asymptomatic patients are not available.
In our series, with a median OS after BM of 7.1 months, outcomes of brain metastatic patients from DTC appear poor. However, outcomes of patients treated with surgery and/or SRS were better with a median OS of 11.9 months. In comparison, OS was only 3.6 months without surgery and/or SRS. Few data are available in the literature and most of the publications are case reports. Table 2 summarizes data of the nine studies containing more than five patients (2 –10). All are retrospective studies with inherent bias. Most patients had DTC, but medullary or anaplastic carcinomas were present too. Median and mean OS after BM ranged from 4 to 33 months with better survivals after surgery or SRS. Chiu et al. (3) and McWilliams et al. (8) reported a survival of 16.7 and 20.8 months after surgery versus 3.4 and 2.7 months without surgery. In the study by Salvati et al. (7), in which all patients underwent surgery and WBRT for a single BM, OS was 26 months for DTC. Patients with a single BM seem to have a better outcome than patients with multiple metastases (OS of 12 vs. 3.7 months in the study by Chiu et al. (3)).
Several studies have investigated SRS treatment for BM from lung, breast, colorectal, renal cancers, or melanomas and guidelines are now available (11,12). Typically, SRS is considered for patients with good prognosis, presenting 1–3 lesions less than 3–4 cm, but only two series have studied SRS for BM from TC. In the series by Kim et al. (9), nine patients underwent SRS with a median marginal dose of 18 Gy. In the study by Bernad et al. (10), 15 patients were treated with SRS. The OS for these two series were the highest published, with 33 and 37.4 months, respectively; the median numbers of lesions treated with SRS were 1 (range 1–6) and 1.5 (range 1–9).
In terms of prognostic factors, due to the limited number of patients, it was impossible to individualize prognostic factors among initial histological findings on the thyroidectomy specimen. McWilliams et al. (8) reported better outcomes for papillary carcinoma (OS=23.6 months) than for follicular carcinoma (OS=8.3 months), but only two patients had follicular carcinomas in their series.
In terms of WBRT after surgery or SRS, in our series, as in series reported by McWilliams et al. (8) and Chiu et al. (3), no difference in OS was found after WBRT. Previously published data showed that WBRT is able to destroy microscopic disease after surgery or SRS with a reduction of intracranial relapses and neurologic deaths (13 –15). However, these results must be balanced with the risk of long-term neurotoxicity (16,17) and indeed, despite reduction of intracranial relapses, trials have failed to show improvement in OS or for the duration of functional independence. For patients with BM from TC, very long survival has been reported (>10 years) (18,19) and recent therapeutic advances such as TKI may help to prolong survival (20). Therefore, it is difficult to propose systematic adjuvant WBRT after surgery or SRS for these patients. Repeat surgery and SRS, or salvage WBRT can be proposed in the case of relapse depending on the type of relapse. Systematic adjuvant WBRT should be reserved for patients with more than three BM. In the future, perhaps, RT advances with hippocampal sparing will enable the reduction of neurologic radiation-induced damages. Although adjuvant WBRT for patients with few BM treated by surgery is subject to controversy, SRS of the resection cavity appears to be an interesting therapeutic approach with a reduction in the risk of local recurrence without increasing neurological toxicity (21 –23).
The question of how to select patients for aggressive treatments is essential. In our series, most patients (70%) had other distant metastases but with frequent indolent evolution. In addition, extracranial disease was not an argument against invasive management. The most discriminating prognostic factor seems simply to be the PS at diagnosis of BM. In our series, OS was 27 months with PS <2 versus 3 months with PS ≥2. Different RT studies have investigated prognostic indices to help in selecting patients for aggressive treatments: the Radiation Therapy Oncology Group recursive partitioning analysis, and the Radiation Therapy Oncology Group–graded prognostic assessment (24 –26). However, none of these indices included thyroid cancer for their development. As an indication, OS is not statistically different according to the presence or absence of neurologic symptoms at the moment of BM diagnosis, indicating that the detection and treatment of asymptomatic cerebral lesions does not lead to overtreatment.
Concerning systemic treatment, few data have shown efficacy of radioactive iodine (131I) treatment for BM. Some reports have noted benefit of 131I when uptake in the BM are present. However, most brain lesions are 131I-refractory lesions and this treatment is usually not very effective. If 131I is planned, caution should be taken to prevent rapid worsening of tumor growth during withdrawal from thyroid hormone and to minimize any edema (27,28). In our study, most patients (13 of 21) were 131I-refractory at the moment of BM diagnosis. For four other patients, the diagnosis of the TC and BM were concurrent. These patients had very poor outcomes with no time for 131I treatment. Four patients had uptake in cerebral metastases, but only one (who underwent surgery and WBRT) had a good evolution with three additional 131I treatments that were effective on bone metastases. Recent advances with targeted agents such as TKI offer great hope for the management of metastatic refractory thyroid cancer. However, these novel drugs are associated with an increased risk of hemorrhage and their use for BM is not recommended. Similarly, the role of chemotherapy remains very limited and no recommendation for its use can be made at this time.
Our results have to be interpreted with caution due to their retrospective character, the low number of patients, and the long period of study with inherent changes of practices. However, this study remains interesting because, with 21 patients, it is one of the three biggest found in the literature (3,8). Moreover, nine patients (43%) had an incidental diagnosis of BM after systematic brain imaging; among these, eight were diagnosed within the last five years, that is, in the era of modern treatments (surgery, SRS, targeted agents). Further, when interpreting the better outcomes after surgery and/or SRS rather than after WBRT, it must be kept in mind that local treatments were delivered to healthy patients with a probably better prognosis irrespective of the performed treatment.
Conclusions
Patients with BM from thyroid carcinoma have a relatively short survival. However, indolent evolution and one- to two-year or longer survivals are possible, providing support to treat these patients with combined and repeated aggressive treatments, including neurosurgery and RT. In guidelines published in 2009, the American Thyroid Association recommends that “surgical therapy in selected incurable patient is important to prevent complications in targeted areas, such as the central nervous system” (29). The most important prognostic factor to select patients for these aggressive treatments seems to be a good PS (<2). Although systematic searching for BM is not indicated for patients with lymph node metastases in the neck, it appears essential for patients with distant metastases because the presence of BM in these cases is probably more frequent than commonly thought, and because these patients are candidates for TKI treatments (with a potential risk of hemorrhage and potential improvement of survival). Reviewing outcomes of these mainly asymptomatic patients should enable us to better define their prognosis in the era of modern treatments.
Footnotes
Acknowledgment
The authors thank Pippa McKelvie-Sebileau of Institut Bergonié for medical editorial assistance with the English.
Author Disclosure Statement
The authors have no disclosures to declare.